UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d)
of the Securities Exchange Act of 1934
Date of Report (Date of earliest event reported): March 4, 2025
PASSAGE BIO, INC.
(Exact name of registrant as specified in its charter)
Delaware |
001-39231 |
82-2729751 |
(State or other jurisdiction |
(Commission |
(IRS Employer |
One Commerce Square |
19103 |
(Address of principal executive offices) |
(Zip Code) |
(267) 866-0311
(Registrant’s telephone number, including area code)
N/A
(Former name or former address, if changed since last report)
Check the appropriate box below if the Form 8-K filing is intended to simultaneously satisfy the filing obligation of the registrant under any of the following provisions:
☐ |
Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425) |
☐ |
Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12) |
☐ |
Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)) |
☐ |
Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section 12(b) of the Act:
Title of each class |
Trading symbol(s) |
Name of each exchange on which registered |
Common Stock, $0.0001 Par Value Per Share |
PASG |
The Nasdaq Stock Market LLC |
Indicate by check mark whether the registrant is an emerging growth company as defined in Rule 405 of the Securities Act of 1933 (§230.405 of this chapter) or Rule 12b-2 of the Securities Exchange Act of 1934 (§240.12b-2 of this chapter).
Emerging growth company ☒
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Item 2.02 Results of Operations and Financial Condition.
On March 4, 2025, Passage Bio, Inc. (the “Company”) issued a press release announcing its financial results for the year ended December 31, 2024. A copy of the press release is attached as Exhibit 99.1 to this report.
The information in this Item 2.02, including Exhibit 99.1 to this report, shall not be deemed to be “filed” for purposes of Section 18 of the Securities Exchange Act of 1934, as amended (the “Exchange Act”), or otherwise subject to the liabilities of that section or Sections 11 and 12(a)(2) of the Securities Act of 1933, as amended (the “Securities Act”). The information contained in this Item 2.02 and in the accompanying Exhibit 99.1 shall not be incorporated by reference into any other filing under the Exchange Act or under the Securities Act, except as shall be expressly set forth by specific reference in such filing.
Item 7.01 Regulation FD Disclosure.
On March 4, 2025, the Company updated its corporate presentation. A copy of the corporate presentation is attached as Exhibit 99.2 to this Current Report on Form 8-K.
The information in this Item 7.01, including Exhibit 99.2 to this Current Report on Form 8-K, shall not be deemed to be “filed” for purposes of Section 18 of the Exchange Act, or otherwise subject to the liabilities of that section or Sections 11 and 12(a)(2) of the Securities Act. The information contained in this Item 7.01 and in the accompanying Exhibit 99.2 shall not be incorporated by reference into any other filing under the Exchange Act or under the Securities Act, except as shall be expressly set forth by specific reference in such filing.
Item 9.01 Financial Statements and Exhibits.
(d)Exhibits
Exhibit No. |
|
Description |
99.1 |
|
|
99.2 |
|
|
104 |
|
Cover Page Interactive Data File (formatted as Inline XBRL). |
2
SIGNATURE
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
|
PASSAGE BIO, INC. |
|
|
|
|
Date: March 4, 2025 |
By: |
/s/ Kathleen Borthwick |
|
|
Kathleen Borthwick |
|
|
Chief Financial Officer |
3

PASSAGE BIO REPORTS FOURTH QUARTER AND FULL YEAR 2024 FINANCIAL RESULTS AND PROVIDES RECENT BUSINESS HIGHLIGHTS
Interim data from Dose 1 PBFT02 demonstrated durable, elevated CSF PGRN and early evidence of reduction in plasma NfL levels, a disease progression biomarker, as compared to published natural history
Enrolled first FTD-GRN patient to be treated with Dose 2 PBFT02, 50% lower than Dose 1
Expect to report 12-month data from Dose 1 and interim safety and biomarker data from Dose 2 in 2H 2025; plan to seek regulatory feedback on FTD-GRN pivotal trial design in 1H 2026
Extended cash runway into 1Q 2027
PHILADELPHIA – March 4, 2025 – Passage Bio, Inc. (Nasdaq: PASG), a clinical stage genetic medicines company focused on improving the lives of patients with neurodegenerative diseases, today reported financial results for the fourth quarter and year ended December 31, 2024, and provided recent business highlights.
“We are pleased to report strong performance in 2024 as we meaningfully advanced our PBFT02 program, delivering promising data in FTD-GRN patients showing robust, durable progranulin expression and early evidence of improvement in a disease progression biomarker. Furthermore, we completed the process development and scale-up of a high-productivity, suspension-based manufacturing process for PBFT02 and are well-positioned for late-stage development,” said Will Chou, M.D., president and chief executive officer of Passage Bio. “As we enter 2025, we remain focused on execution of our ongoing upliFT-D trial in FTD-GRN and are excited to expand enrollment to include FTD patients with C9orf72 gene mutations. We look forward to building upon the encouraging data generated to date and engaging with health authorities to explore the registrational pathway for this promising, one-time therapy to address a significant unmet patient need.”
Recent Highlights:
| ● | Interim data from FTD-GRN patients in upliFT-D clinical trial demonstrated that Dose 1 PBFT02 consistently increased cerebrospinal fluid (CSF) progranulin (PGRN) and showed early evidence of improvement in a disease progression biomarker: Dose 1 PBFT02 consistently increased CSF PGRN levels in all patients from below 3 ng/mL at baseline to 13 – 27 ng/mL at six months (n=4) and 22 – 34 ng/mL at 12 months (n=2). In addition, plasma neurofilament light chain (NfL) levels, which are associated with disease progression, were 13% lower than baseline on average at 12 months (n=2) post-treatment compared to an expected increase of 29% per year based on published natural history data from untreated symptomatic FTD-GRN patients. |
| ● | Enrolled first FTD-GRN patient to receive Dose 2 PBFT02: Given the robust CSF PGRN levels achieved at Dose 1 and to aid future discussions with health authorities regarding a registrational study design, the company introduced a lower dose level, Dose 2, which is fifty percent of Dose 1. Dose 2 is expected to be administered to the three remaining FTD-GRN patients in Cohort 2 of the upliFT-D study. The first of these three patients has been enrolled, and multiple patients are being evaluated for eligibility across seven active trial sites in Brazil, Canada, Portugal, and the United States. |
| ● | Extended cash runway into 1Q 2027 by moving to outsourced analytical testing model and reducing operating expenses: In January, the company implemented a series of measures in connection with moving to an outsourced analytical testing model and to reduce operating expenses. As a result, the company’s cash runway was extended into the first quarter of 2027 as it continues to focus on the execution of the ongoing upliFT-D clinical trial in FTD-GRN and FTD-C9orf72 and the advancement of its preclinical program in Huntington’s disease. |
Anticipated Upcoming Milestones:
FTD-GRN
| ● | Report 12-month data from Dose 1 and interim safety and biomarker data from Dose 2 in 2H 2025 |
| ● | Seek regulatory feedback on registrational trial design in 1H 2026 |
FTD-C9orf72
| ● | Initiate dosing of FTD-C9orf72 patients in 1H 2025 |
Fourth Quarter and Full-Year 2024 Financial Results
| ● | Cash Position: Cash, cash equivalents and marketable securities were $76.8 million as of December 31, 2024, as compared to $114.3 million as of December 31, 2023. The company expects current cash, cash equivalents and marketable securities to fund operations into 1Q 2027. |
| ● | Research and Development (R&D) Expenses: R&D expenses were $9.6 million for the quarter ended December 31, 2024, and $40.2 million for the year ended December 31, 2024, compared to $12.1 million and $61.4 million for the same quarter and year ended in 2023, respectively. |
| ● | General and Administrative (G&A) Expenses: G&A expenses were $4.7 million for the quarter ended December 31, 2024, and $25.0 million for the year ended December 31, 2024, compared to $6.3 million and $41.6 million for the same quarter and year ended in 2023, respectively. |
| ● | Net Loss: Net loss was $12.7 million, or $0.20 per basic and diluted share, for the quarter ended December 31, 2024 and $64.8 million, or $1.07 per basic and diluted share, for the year ended December 31, 2024, compared to a net loss of $16.8 million, or $0.30 per basic and diluted share, for the quarter ended December 31, 2023 and $102.1 million, or $1.86 per basic and diluted share, for the year ended December 31, 2023. |
About upliFT-D (NCT04747431)
upliFT-D is a Phase 1/2 global, multi-center, open-label clinical trial of PBFT02 administered by single injection into the cisterna magna in patients aged 35 to 75 years with FTD-GRN or FTD-C9orf72. The clinical trial will sequentially enroll three FTD-GRN cohorts and two FTD-C9orf72 cohorts. Enrollment is currently ongoing. The primary endpoint of the clinical trial is to evaluate the safety and tolerability of PBFT02. Secondary endpoints include disease biomarkers and clinical outcome measures. upliFT-D is a two-year clinical trial with a three-year safety extension.
Passage Bio is pursuing several initiatives to support clinical trial recruitment and enrollment, including a collaborative partnership with InformedDNA to provide no-cost genetic counseling and testing for adults who have been diagnosed by their physicians with FTD. More information about upliFT-D can be found here.
About PBFT02
PBFT02 is a gene therapy that utilizes an AAV1 viral vector to deliver, through ICM administration, a functional GRN gene that encodes PGRN. This vector construct and delivery approach aim to elevate PGRN levels in the central nervous system to alter the course of neurodegenerative diseases. Interim clinical data from the Phase 1/2 upliFT-D study in FTD-GRN participants showed that gene replacement by ICM administration of PBFT02 resulted in robust PGRN elevations in the CSF.
The potential clinical benefit of PBFT02 is supported by extensive preclinical studies. In non-human primates, a single ICM administration of PBFT02 led to broad vector distribution throughout the CNS, and robust, dose-dependent elevations in PGRN levels in CSF. An NHP study also demonstrated that AAV1 was particularly proficient at transducing ependymal cells. In a murine FTD model, PBFT02 administration improved lysosomal function and reduced neuroinflammation.
About Passage Bio
Passage Bio (Nasdaq: PASG) is a clinical stage genetic medicines company on a mission to improve the lives of patients with neurodegenerative diseases. Our primary focus is the development and advancement of cutting-edge, one-time therapies designed to target the underlying pathology of these conditions. Passage Bio’s lead product candidate, PBFT02, seeks to treat neurodegenerative conditions, including frontotemporal dementia, by elevating progranulin levels to restore lysosomal function and slow disease progression.
To learn more about Passage Bio and our steadfast commitment to protecting patients and families against loss in neurodegenerative conditions, please visit: passagebio.com.
Forward-Looking Statements
This press release contains “forward-looking statements” within the meaning of, and made pursuant to the safe harbor provisions of, the Private Securities Litigation Reform Act of 1995, including, but not limited to: our expectations about timing and execution of anticipated milestones, including the initiation of dosing of FTD-C9orf72 patients, timing of feedback from regulatory authorities, the progress of clinical studies and the availability of clinical data from such trials; our expectations about our collaborators’ and partners’ ability to execute key initiatives; the financial impact of the restructuring and reduction in workforce and our expectations about cash runway; and the ability of our product candidates to treat their respective target CNS disorders. These forward-looking statements may be accompanied by such words as “aim,” “anticipate,” “believe,” “could,” “estimate,” “expect,” “forecast,” “goal,” “intend,” “may,” “might,” “plan,” “potential,” “possible,” “will,” “would,” and other words and terms of similar meaning. These statements involve risks and uncertainties that could cause actual results to differ materially from those reflected in such statements, including: our ability to develop and obtain regulatory approval for our product candidates; the timing and results of preclinical studies and clinical trials; risks associated with clinical trials, including our ability to adequately manage clinical activities, unexpected concerns that may arise from additional data or analysis obtained during clinical trials, regulatory authorities may require additional information or further studies, or may fail to approve or may delay approval of our drug candidates; the occurrence of adverse safety events; the risk that positive results in a preclinical study or clinical trial may not be replicated in subsequent trials or success in early stage clinical trials may not be predictive of results in later stage clinical trials; failure to protect and enforce our intellectual property, and other proprietary rights; our dependence on collaborators and other third parties for the development and manufacture of product candidates and other aspects of our business, which are outside of our full control; risks associated with current and potential delays, work stoppages, or supply chain disruptions; and the other risks and uncertainties that are described in the Risk Factors section in documents the company files from time to time with the Securities and Exchange Commission (SEC), and other reports as filed with the SEC. Passage Bio undertakes no obligation to publicly update any forward-looking statement, whether written or oral, that may be made from time to time, whether as a result of new information, future developments or otherwise.
Passage Bio, Inc.
Balance Sheets
|
|
December 31, |
||||
(in thousands, except share and per share data) |
|
2024 |
|
2023 |
||
Assets |
|
|
|
|
|
|
Current assets: |
|
|
|
|
|
|
Cash and cash equivalents |
|
$ |
37,573 |
|
$ |
21,709 |
Marketable securities |
|
|
39,183 |
|
|
92,585 |
Prepaid expenses and other current assets |
|
|
838 |
|
|
923 |
Prepaid research and development |
|
|
1,221 |
|
|
2,742 |
Total current assets |
|
|
78,815 |
|
|
117,959 |
Property and equipment, net |
|
|
9,331 |
|
|
15,295 |
Right of use assets - operating leases |
|
|
13,803 |
|
|
16,858 |
Other assets |
|
|
463 |
|
|
433 |
Total assets |
|
$ |
102,412 |
|
$ |
150,545 |
Liabilities and stockholders’ equity |
|
|
|
|
|
|
Current liabilities: |
|
|
|
|
|
|
Accounts payable |
|
$ |
742 |
|
$ |
1,298 |
Accrued expenses and other current liabilities |
|
|
6,707 |
|
|
11,670 |
Non-refundable sublicense and transition services payments received |
|
|
8,226 |
|
|
— |
Operating lease liabilities |
|
|
3,688 |
|
|
3,373 |
Total current liabilities |
|
|
19,363 |
|
|
16,341 |
Operating lease liabilities - noncurrent |
|
|
21,788 |
|
|
22,921 |
Total liabilities |
|
|
41,151 |
|
|
39,262 |
|
|
|
|
|
|
|
Stockholders’ equity: |
|
|
|
|
|
|
Preferred stock, $0.0001 par value: 10,000,000 shares authorized; no shares issued and outstanding at both December 31, 2024 and December 31, 2023 |
|
|
— |
|
|
— |
Common stock, $0.0001 par value: 300,000,000 shares authorized; 62,061,774 shares issued and outstanding at December 31, 2024 and 54,944,130 shares issued and outstanding at December 31, 2023 |
|
|
6 |
|
|
5 |
Additional paid‑in capital |
|
|
720,482 |
|
|
705,789 |
Accumulated other comprehensive income (loss) |
|
|
8 |
|
|
(43) |
Accumulated deficit |
|
|
(659,235) |
|
|
(594,468) |
Total stockholders’ equity |
|
|
61,261 |
|
|
111,283 |
Total liabilities and stockholders’ equity |
|
$ |
102,412 |
|
$ |
150,545 |
Passage Bio, Inc.
Statements of Operations and Comprehensive Loss
|
|
Year Ended December 31, |
||||
(in thousands, except share and per share data) |
|
2024 |
|
2023 |
||
Operating expenses: |
|
|
|
|
|
|
Research and development |
|
$ |
40,179 |
|
$ |
61,419 |
General and administrative |
|
|
24,988 |
|
|
41,580 |
Impairment of long-lived assets |
|
|
5,233 |
|
|
5,390 |
Loss from operations |
|
|
(70,400) |
|
|
(108,389) |
Other income (expense), net |
|
|
5,633 |
|
|
6,327 |
Net loss |
|
$ |
(64,767) |
|
$ |
(102,062) |
Per share information: |
|
|
|
|
|
|
Net loss per share of common stock, basic and diluted |
|
$ |
(1.07) |
|
$ |
(1.86) |
Weighted average common shares outstanding, basic and diluted |
|
|
60,405,036 |
|
|
54,743,490 |
Comprehensive loss: |
|
|
|
|
|
|
Net loss |
|
$ |
(64,767) |
|
$ |
(102,062) |
Unrealized gain (loss) on marketable securities |
|
|
51 |
|
|
923 |
Comprehensive loss |
|
$ |
(64,716) |
|
$ |
(101,139) |
For further information, please contact:
Investors:
Stuart Henderson
Passage Bio
shenderson@passagebio.com
Media:
Mike Beyer
Sam Brown Inc. Healthcare Communications
312.961.2502
MikeBeyer@sambrown.com
|
Nasdaq: PASG © 2025 Passage Bio. All rights reserved. Corporate Presentation March 2025 |
|
2 Forward-Looking Statement This presentation includes “forward-looking statements” within the meaning of, and made pursuant to the safe harbor provisions of, the Private Securities Litigation Reform Act of 1995, including, but not limited to: our expectations about timing and execution of anticipated milestones, including the initiation of dosing of FTD-C9orf72 patients, timing of feedback from regulatory of authorities, the progress of clinical studies and the availability of clinical data from such trials; the potential of our product candidates versus other treatment options and clinical candidates; our expectations about our collaborators’ and partners’ ability to execute key initiatives; the financial impact of the restructuring and reduction in workforce and our expectations about cash runway; and the ability of our product candidates to treat their respective target CNS disorders. These forward-looking statements may be accompanied by such words as “aim,” “anticipate,” “believe,” “could,” “estimate,” “expect,” “forecast,” “goal,” “intend,” “may,” “might,” “plan,” “potential,” “possible,” “will,” “would,” and other words and terms of similar meaning. These statements involve risks and uncertainties that could cause actual results to differ materially from those reflected in such statements, including: our ability to develop and obtain regulatory approval for our product candidates; the timing and results of preclinical studies and clinical trials; risks associated with clinical trials, including our ability to adequately manage clinical activities, unexpected concerns that may arise from additional data or analysis obtained during clinical trials, regulatory authorities may require additional information or further studies, or may fail to approve or may delay approval of our drug candidates; the occurrence of adverse safety events; the risk that positive results in a preclinical study or clinical trial may not be replicated in subsequent trials or success in early stage clinical trials may not be predictive of results in later stage clinical trials; failure to protect and enforce our intellectual property, and other proprietary rights; our dependence on collaborators and other third parties for the development and manufacture of product candidates and other aspects of our business, which are outside of our full control; risks associated with current and potential delays, work stoppages, or supply chain disruptions; and the other risks and uncertainties that are described in the Risk Factors section in documents the company files from time to time with the Securities and Exchange Commission (SEC), and other reports as filed with the SEC. Passage Bio undertakes no obligation to publicly update any forward-looking statement, whether written or oral, that may be made from time to time, whether as a result of new information, future developments or otherwise. |
|
3 REDEFINING THE COURSE OF NEURODEGENERATIVE CONDITIONS Advancing potential best-in-class, one-time progranulin raising FTD-GRN gene therapy Established suspension-based PBFT02 manufacturing process to support late-stage development Strong cash position with runway expected to the end of 1Q 2027* Exploring benefits of elevated progranulin in multiple adult neurodegenerative diseases * Based on cash, cash equivalents and marketable securities as of December 31, 2024. |
|
4 Validating the Therapeutic Potential of PBFT02 Promising data from initial clinical study of PBFT02 in FTD-GRN Genetic form of FTD caused by GRN mutations, which lead to progranulin (PGRN) deficiency No approved disease-modifying therapies One-time, gene replacement therapy Proprietary AAV1 construct Nonsurgical injection directly to cerebrospinal fluid (CSF) Durable, elevated CSF PGRN levels* Urgent Patient Need in FTD-GRN Differentiated, Potential Best-in-Class Profile Fast Track and Orphan Drug Designation * Based on interim data. |
|
5 Significant Market Opportunity for PBFT02 Across Multiple Neurodegenerative Diseases ~18,000 ~21,000 ~72,600 ~3.9M FTD-GRN1–3 FTD-C9orf722–4 AMYOTROPHIC LATERAL SCLEROSIS (ALS) 5–6 ALZHEIMER’S DISEASE (GRN SNP)*7–8 * rs5848 single nucleotide polymorphism (SNP) 1. Greaves CV, et al. J Neurol 2019; 266:2075-2086. 2. Galvin JE, et al. Neurology 2017; 89:2049-2056. 3. Onyike CU, et al. Int Rev Psychiatry 2013; 25:130-137. 4. Moore KM, et al. Lancet Neurol 2020; 19: 145–156. 5. Brown et al. Neuroepi 2021; 55:342-353. 6. CDC ALS Registry Dashboard. 7. Sheng J, et al. Gene 2014; 141-145. 8. Alz Assoc. 2023 Alzheimer’s Disease Facts and Figures. Alzheimers Dement 2023;19. Estimated Prevalence (US and EU) Current clinical programs |
|
6 Anticipated Upcoming Milestones and Data Readouts 1H 2025 2H 2025 1H 2026 Report 12-month Dose 1 and interim Dose 2 data FTD-C9orf72 Initiate dosing of FTD-C9orf72 patients Seek regulatory feedback on registrational trial design FTD-GRN Milestones |
|
PBFT02 Frontotemporal Dementia |
|
8 FTD: A Devastating Adult Disease OVERVIEW • Fatal adult-onset neurodegenerative disease affecting the frontal and temporal lobes of the brain, characterized by a decline in behavior, language and executive function • One of the most common causes of early-onset dementia worldwide, disproportionately affecting individuals aged 40-65 years CLINICAL SYMPTOMS Disease progression is rapid and degenerative, including loss of speech, loss of expression, behavioral changes and immobility On average, people with FTD live 8 years after the onset of symptoms |
|
9 Progranulin Deficiency is the Defining Characteristic of FTD-GRN and Leads to Neurodegeneration Progranulin is critical to maintaining CNS cell homeostasis Rhinn H et al. Trends Pharmacol Sci. 2022, 43:641-652 |
|
10 Elevated PGRN Increases Potential for Improved Cellular Function • Progranulin is a secreted protein that binds to cell membrane receptors to affect multiple intracellular pathways –Major role is regulating intracellular lysosomal activity –Extracellular PGRN is endocytosed via multiple receptors • Driving elevated PGRN levels in the extracellular space increases the amount of PGRN available to enter target CNS cells • Able to leverage cross-correction mechanism: secreted PGRN can be taken up by non-transduced cells Paushter et al. Acta Neuropathol. 2018;136:1-17. Rhinn et al. Trends Pharmacol Sci. 2022; 43:641-652. |
|
11 Preclinical NHP: AAV1 Achieved the Highest Levels of CSF PGRN • AAV1 resulted in superior CSF hPGRN levels, 5x higher than AAV5 and AAVhu68 (an AAV9 variant) vectors, after ICM administration Rhesus macaques (n=2/gp) ICM-delivered AAV.hPGRN (3.3 x 1011 GC/g brain), day 0 *Size and duration of elevation muted by immune response to human PGRN. Shading: Healthy adult sample range for CSF PGRN, n = 61 (Passage Bio data) CSF, cerebrospinal fluid; GC, genome copies; ICM, intra-cisterna magna; NHP, non-human primate. Reference: Hinderer et al., Ann Clin Trans Neurol. 2020; 7:1843-1853 Human PGRN in NHP CSF Vector Comparison |
|
12 Preclinical NHP: ICM Administration of PBFT02 Led to Broad Distribution of Vector Throughout Brain/Spinal Cord Vector Biodistribution in NHPs 90 days post-ICM PBFT02 • Robust, dose-dependent vector delivery to cortical and sub-cortical brain regions affected in FTD • NHP low dose, equivalent to clinical Dose 1 of PBFT02 in upliFT-D study, resulted in ~10⁴ GC/μg DNA in all sampled areas throughout the brain n=3/gp. Data are mean +/- SEM. CBL, cerebellum; Cerv, cervical; DRG, dorsal root ganglion; FCX, frontal cortex; GC, genome copies; Hipp, hippocampus; ICM, intra-cisterna magna; LLoQ, lower limit of quantitation; Lumb, lumbar; OCX, occipital cortex; PCX, parietal cortex; TCX, temporal cortex; Thor, thoracic; Veh, vehicle |
|
13 Preclinical Grn–/– Mice: Expression of hPGRN Improved Lysosomal Dysfunction and Neuroinflammation in the Brain Greatest pathological benefit was associated with the highest PGRN levels in the CSF Lipofuscin deposition and microglial activation are hallmark pathologies seen in FTD; Improvements in both measures were seen in cerebral cortex, thalamus, and hippocampus after PBFT02 administration Grn–/– and WT mice (n=14-15/gp) ICV-administered PBFT02 or vehicle (V). Baseline controls were untreated mice on Day 1. Bars: mean +/- SEM. # ## p < 0.01, ### p < 0.005 vs WT control; *p < 0.05, ***p < 0.005 vs GRN-/-+ V , one-way ANOVA followed by Tukey’s multiple comparisons test. GRN, granulin gene; ICV, Intra-cerebroventricular; PGRN, progranulin; WT, wildtype PBFT02 reduced lipofuscin deposition at all doses, suggesting improved lysosomal dysfunction Dose-dependent elevations in CSF PGRN after PBFT02 led to progressive reductions in microglial activation Thalamus Lipofuscin Thalamus CD68 Immunohistochemistry |
|
14 TRIAL DESIGN upliFT-D: Global Phase 1/2 Trial with PBFT02 DURATION 2 years; with additional 3 years of follow-up for safety and durability of effect PRIMARY ENDPOINTS Safety and tolerability SECONDARY ENDPOINTS Biomarkers • Progranulin (CSF, plasma) • GFAP (CSF, plasma) • vMRI • Retinal nerve fiber layer and retinal lipofuscin deposits via OCT • NfL (CSF, plasma) Clinical • CDR + NACC FTLD sum of boxes EXPLORATORY BIOMARKERS • Cathepsin D (CSF) • LAMP 1 (CSF) • Lys-GL1 (CSF) COHORT 1 (n=5) Dose 1 COHORT 2 (n=5) Dose 1 / Dose 2 COHORT 3 (n=3-5) COHORT 4 (n=3-5) Dose 2 COHORT 5 (n=3-5) IDMC review Phase Multicenter Open-label Dose exploration study 1/2 Complete Dose 1: 3.3e10 GC/g estimated brain weight Dose 2: 1.6e10 GC/g estimated brain weight FTD-GRN FTD-C9orf72 |
|
15 Intra-Cisterna Magna (ICM) Administration • Directly deliver vector into the CSF via a single injection –Allows for broad CNS biodistribution1 –Lower doses compared to IV systemic delivery –Reduced impact of neutralizing antibodies • Brief (<60 min), non-surgical, CT-guided procedure for precise delivery to the cisterna magna Cisterna –Procedure avoids penetration of brain tissue magna 1. Hinderer et. al, Hum Gene Ther. 2018; 29:15-24. |
|
16 upliFT-D: Interim Safety Profile • In 5 of 7 patients, all treatment emergent AEs were mild to moderate in severity • 2 of 7 patients experienced a total of 3 SAEs – Patient 1: asymptomatic venous sinus thrombosis (VST) and hepatotoxicity, leading to a revised immunosuppression regimen in all subsequent patients** – Patient 7: asymptomatic VST, completely resolved prior to day 30 following treatment with anticoagulants. No evidence of hepatotoxicity, immune response or other laboratory abnormalities • No evidence of a clinically significant immune response following introduction of new immunosuppression regimen • No evidence of DRG toxicity • No complications during ICM administration Interim Safety Highlights* Dose 1 PBFT02 in FTD-GRN Patients (n=7) *Patient safety follow-up ranged from 1 to 18 months post-dosing as of data cutoff of December 9, 2024 **Patient 1 received oral prednisone 60 mg daily through day 60; subsequent patients received a revised immunosuppressive regimen of 1g methylprednisolone IV daily to day 3, followed by oral prednisone 60 mg to day 60, then taper AE, adverse event; DRG, dorsal root ganglion; ICM, intra-cisterna magna; SAE, serious adverse event; VST, venous sinus thrombosis. Remaining patients in Cohort 2 to receive Dose 2 (50% Dose 1) |
|
17 PBFT02 Generated Robust, Durable Increases in CSF PGRN Shading: Healthy adult sample range for CSF PGRN (range: 3.28 – 8.15 ng/mL, mean: 4.76 ng/mL, n = 61) (Passage Bio data) CSF, cerebrospinal fluid 0 10 20 30 40 0 1 6 12 18 CSF PGRN, ng/mL Time (months) Dose 1 Progranulin, CSF P1 P2 P3 P4 P5 P6 Potential best-in-class PGRN profile • Consistent elevation from baseline • Durable to 18 months • Levels overall plateauing by 6 months Baseline M1 M6 M12 M18 N 6 6 4 2 1 Min 1.5 8.0 13.2 22.3 35.9 Max 2.9 17.3 27.3 34.0 35.9 Mean 2.3 12.4 20.0 28.2 - CSF Progranulin (ng/mL) in FTD-GRN Patients |
|
18 • Plasma PGRN levels remained below normal levels up to 12 months post-dose in FTD-GRN patients • PGRN increased only in the CSF, where it has potential to reduce neurodegeneration Plasma PGRN Levels Remained Below Normal Levels Post-Dose Shading: Lower limit of healthy adult sample range for plasma PGRN (91.6 – 372.4 ng/mL, n = 56) (Passage Bio data) 0 50 100 150 0 1 3 6 12 Plasma PGRN, ng/mL Time (months) Dose 1 Progranulin, Plasma P1 P2 P3 P4 P5 P6 |
|
19 Plasma NfL Showed Early Evidence of Improvement in a Disease Progression Biomarker vs. Natural History 29.0% -15% -12.7% -10% -5% 0% 5% 10% 15% 20% 25% 30% 35% % Change Plasma NfL Annual Rate of Change Natural History (n=15) PBFT02 (n=2) 1 Natural history: 15 symptomatic FTD-GRN patients; mean years since diagnosis: 2.9 (Saracino et al, 2021; ). Average time since diagnosis in PBFT02 patients 2 years (n=2). 2 van der Ende et al, Lancet Neurol 2019; 18:1103-11. NfL, neurofilament light chain J Neurol Neurosurg Psych 92:1278-1288 • Plasma NfL is the only FTD-GRN disease progression biomarker with published longitudinal natural history data available1,2 • Both PBFT02-treated patients had a reduced annual rate of change in plasma NfL compared to published natural history data |
|
20 PBFT02 Offers Best-in-Class Therapeutic Potential PBFT02 Product Candidate AAV1 gene therapy delivering GRN Anti-sortilin antibody AAV9 gene therapy delivering GRN Stage of Development Phase 1/2 Phase 3 Phase 1/2 Route of Administration ICM IV ICM Expected Frequency of Administration One Time Monthly One Time CSF PGRN Level1 13-27 ng/mL at 6m (n=4) ~4-5 ng/mL (n=9)2 ~4-8 ng/mL at 12m (n=7 higher dose)3 Durability of CSF PGRN Expression1 Durable at 18m (n=1) n/a (monthly admin) Declining from 2 to 12m (n=7 higher dose)3 PBFT02 uniquely positioned to offer a one-time therapy capable of achieving highest progranulin levels 1 Clinical evidence based on public disclosure. Results are derived from different clinical trials at different points in time. No head-to-head trials have been conducted among the results shown. Comparing the results from different trials may be unreliable due to different protocol designs, trial design, patient selection and populations, number of patients, trial endpoints, trial objectives and other parameters that may not be the same between trials. 2 Alector 2021 AAIC presentation. 3 Lilly/Prevail AD/PD Mar 2024 presentation and abstract. |
|
21 Summary: FTD-GRN SAFETY1 PBFT02 Dose 1 •In 5 of 7 patients, all treatment emergent AEs were mild to moderate • 2 of 7 patients experienced a total of 3 SAEs •No evidence of clinically significant immune response following introduction of new immunosuppression regimen •No evidence of DRG toxicity •No complications during ICM administration BIOMARKERS • Potential best-in-class PGRN profile at Dose 1 • Robust, consistent elevation of CSF PGRN •Durable response to 18 months •No increase in plasma PGRN levels up to 12-months • Plasma NfL in treated patients showed early evidence of improvement vs. natural history ANTICIPATED NEXT STEPS • Evaluating Dose 2 in subsequent Cohort 2 patients • Report 12-month Dose 1 and interim Dose 2 data in 2H 2025 • Seek regulatory feedback on registrational trial design in 1H 2026 1. Patient safety follow-up ranged from 1 to 18 months post-dosing as of data cutoff of December 9, 2024 AE, adverse event: DRG, dorsal root ganglion; ICM, intra-cisterna magna; SAE, serious adverse event; |
|
Looking Ahead |
|
23 PBFT02 has Potential to Correct Underlying Pathology in FTD-GRN, FTD-C9orf72 and ALS TDP-43 pathology is a hallmark of multiple neurodegenerative diseases1 • TDP-43 mislocalizes from nucleus to cytoplasm • Forms inclusion bodies associated with neurodegeneration 1. Rhinn H et al. Trends Pharmacol Sci. 2022; 43:641-652 |
|
24 TDP-43 pathology due to lysosomal dysfunction (GRN/ TMEM106 double knockout, DKO) reduced by AAV.hPGRN1 Elevated PGRN Ameliorates TDP-43 Pathology in Preclinical Models AAV delivered hPGRN to mouse brain TDP-43 pathology in DKO mice reduced by AAV.hPGRN Elevated PGRN reduced insoluble TDP-43 in mouse spinal cord Elevated PGRN extended survival of TDP-43 mutant mice Elevated PGRN ameliorated TDP-43 pathology and disease course in a preclinical model2 • Elevated PGRN also prevented degeneration of large axon fibers in TDP-43 mice • PGRN neuroprotection from pleiotropic effect, not single pathway 1. Reich et al. Sci Transl Med. 2024; 16(750); 2. Beel et al. Mol Neurodegen. 2018: 13:55.; Laird et al. PLoS One 2010; 5:e13368. DKO, double gene knockout; GRN, granulin gene; PGRN, progranulin; TDP-43, transactive response DNA binding protein 43 kDa † PGRN increased to >2x endogenous levels |
|
25 GRN rs5848 SNP associated with accelerated disease in FTD-C9orf72 patients Decreased PGRN Associated with Greater Disease Severity in Multiple CNS Conditions GRN rs5848 SNP associated with accelerated disease in FTD-C9orf72 patients 1. van Blitterswijk et al. Mol Neurodegen. 2014; 9:38 AD, Alzheimer’s disease; ALS, amyotrophic lateral sclerosis; GRN, granulin gene; PGRN, progranulin; SNP, single nucleotide polymorphism PGRN SNPs are genetic risk factors for CNS diseases • GRN rs5848 SNP results in ~15% reduction in PGRN levels • PGRN SNPs increase risk for, and worsen severity of, FTD/ALS-C9orf72 and AD1 |
|
26 Critical Manufacturing Milestones Achieved to Enable Late-Stage Development Functional Potency Assay Developed assay and reached alignment with FDA on suitability of assay for PBFT02 release Robust Manufacturing Process Completed development of high-productivity, suspension-based manufacturing process Registrational Study Approach • Seek feedback on registrational strategy in 1H 2026 • Leverage recent GTx precedents for utilizing natural history (NHS) data as external control • Analyze existing FTD-GRN NHS databases with >300 patients |
|
27 Upcoming Milestones and Corporate Updates PIPELINE • Advancing Huntington’s disease preclinical program BALANCE SHEET • Cash balance of ~$77 million as of 12/31/24 * • Cash runway into 1Q 2027 * Based on cash, cash equivalents and marketable securities TIMING MILESTONE FTD-GRN 2H 2025 Report 12-month Dose 1 and interim Dose 2 data 1H 2026 Seek regulatory feedback on registrational trial design FTD-C9orf72 1H 2025 Initiate dosing of FTD-C9orf72 patients |
|
28 REDEFINING THE COURSE OF NEURODEGENERATIVE CONDITIONS Advancing potential best-in-class, one-time progranulin raising FTD-GRN gene therapy Established suspension-based PBFT02 manufacturing process to support late-stage development Strong cash position with runway expected to the end of 1Q 2027* Exploring benefits of elevated progranulin in multiple adult neurodegenerative diseases * Based on cash, cash equivalents and marketable securities as of December 31, 2024. |
|
Thank You passagebio.com | NASDAQ: PASG |
|
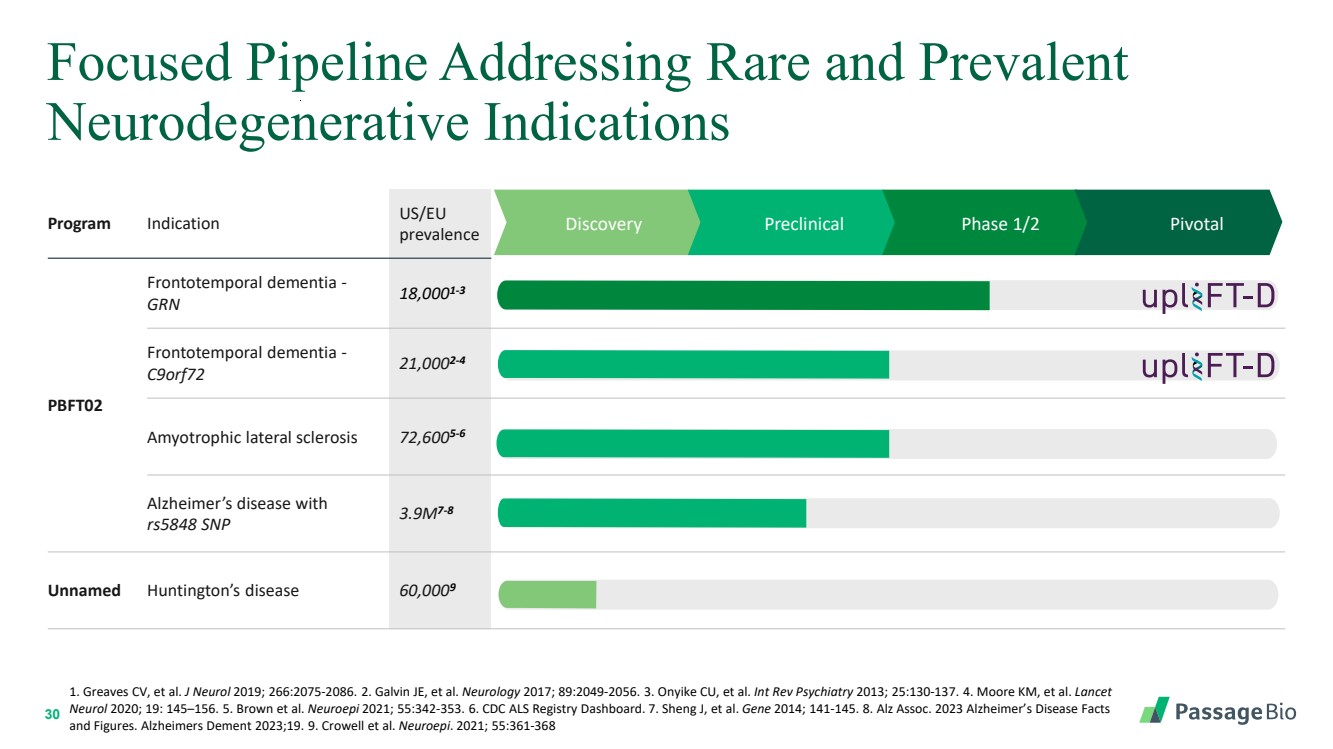
30 Program Indication US/EU prevalence Discovery Preclinical Phase 1/2 Pivotal PBFT02 Frontotemporal dementia - GRN 18,0001-3 Frontotemporal dementia - C9orf72 21,0002-4 Amyotrophic lateral sclerosis 72,6005-6 Alzheimer’s disease with rs5848 SNP 3.9M7-8 Unnamed Huntington’s disease 60,0009 Focused Pipeline Addressing Rare and Prevalent Neurodegenerative Indications 1. Greaves CV, et al. J Neurol 2019; 266:2075-2086. 2. Galvin JE, et al. Neurology 2017; 89:2049-2056. 3. Onyike CU, et al. Int Rev Psychiatry 2013; 25:130-137. 4. Moore KM, et al. Lancet Neurol 2020; 19: 145–156. 5. Brown et al. Neuroepi 2021; 55:342-353. 6. CDC ALS Registry Dashboard. 7. Sheng J, et al. Gene 2014; 141-145. 8. Alz Assoc. 2023 Alzheimer’s Disease Facts and Figures. Alzheimers Dement 2023;19. 9. Crowell et al. Neuroepi. 2021; 55:361-368 |
|
31 Demonstrated Leadership LEADERSHIP TEAM Deep experience in rare disease, CNS disorders and genetic medicines Eden Fucci SVP Technical Operations BOARD OF DIRECTORS Maxine Gowen, Ph.D. Chairwoman Athena Countouriotis, M.D. Avenzo Therapeutics Derrell Porter, M.D. cTRL Therapeutics Dolan Sondhi, Ph.D. Weill Cornell Medicine Sandip Kapadia Harmony Biosciences Saqib Islam, J.D. SpringWorks Thomas Kassberg Ultragenyx William Chou, M.D. President & Chief Executive Officer Stuart Henderson Chief Business Officer William Chou, M.D. President & Chief Executive Officer Chip Cale General Counsel & Corporate Secretary Kathleen Borthwick Chief Financial Officer Karl Whitney, Ph.D. SVP Global Regulatory Affairs Sue Browne, Ph.D. Chief Scientific Officer |