|
State of Delaware
|
001-35776
|
98-1359336
|
|
(State or Other Jurisdiction of Incorporation)
|
(Commission File Number)
|
(IRS Employer Identification No.)
|
|
103 Carnegie Center
Suite 300
|
||
|
Princeton, New Jersey
|
08540
|
|
|
(Address of Principal Executive Offices)
|
(Zip Code)
|
| ☐ |
Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425)
|
| ☐ |
Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12)
|
| ☐ |
Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b))
|
| ☐ |
Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c))
|
|
Title of each class
|
Trading
Symbol(s)
|
Name of each exchange on which registered
|
||
|
Common Stock, par value $0.0001 per share
|
GRCE
|
The Nasdaq Stock Market LLC
|
| Item 2.02 |
Results of Operations and Financial Condition.
|
|
Item 8.01
|
Other Events.
|
| Item 9.01 |
Exhibits.
|
|
Exhibit
|
Description
|
|
|
Press Release, dated November 13, 2025.
|
||
|
Corporate Presentation, dated November 13, 2025.
|
||
|
104
|
Cover Page Interactive Data File (embedded within the Inline XBRL document)
|
|
GRACE THERAPEUTICS, INC.
|
|||
|
Date:
|
November 13, 2025
|
By:
|
/s/ Prashant Kohli
|
|
Prashant Kohli
|
|||
|
Chief Executive Officer
|

|
|
• |
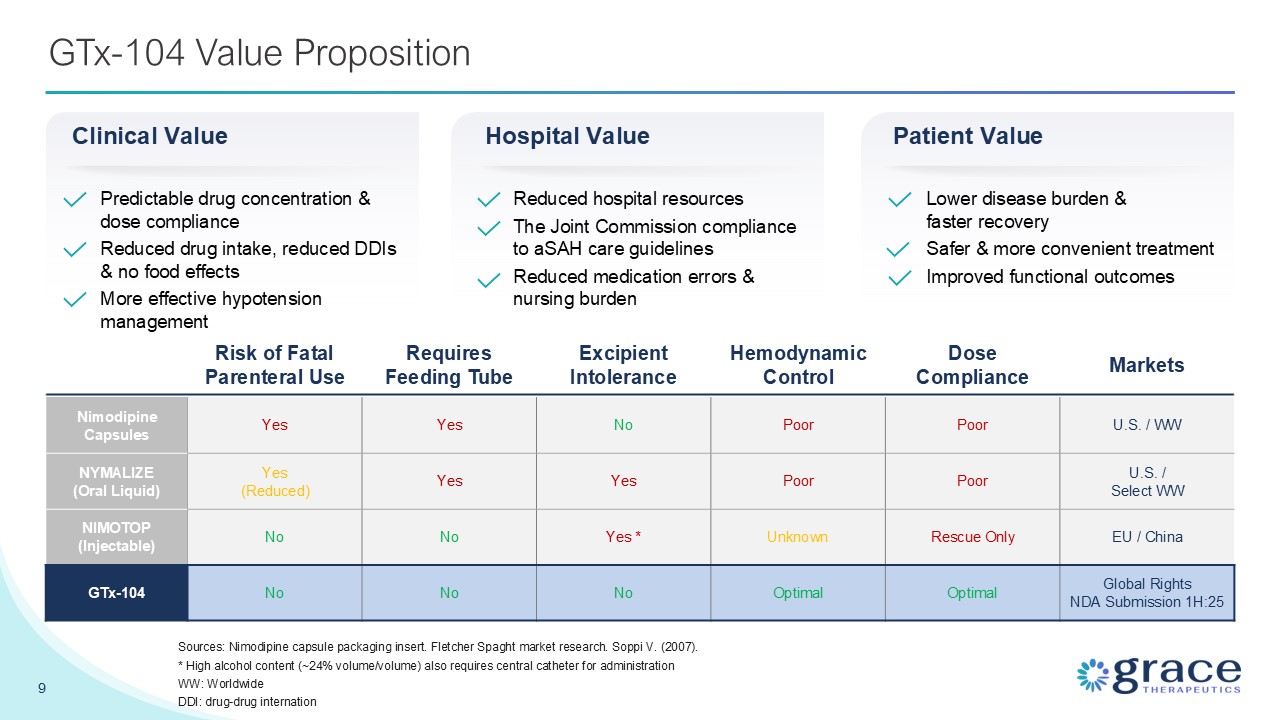
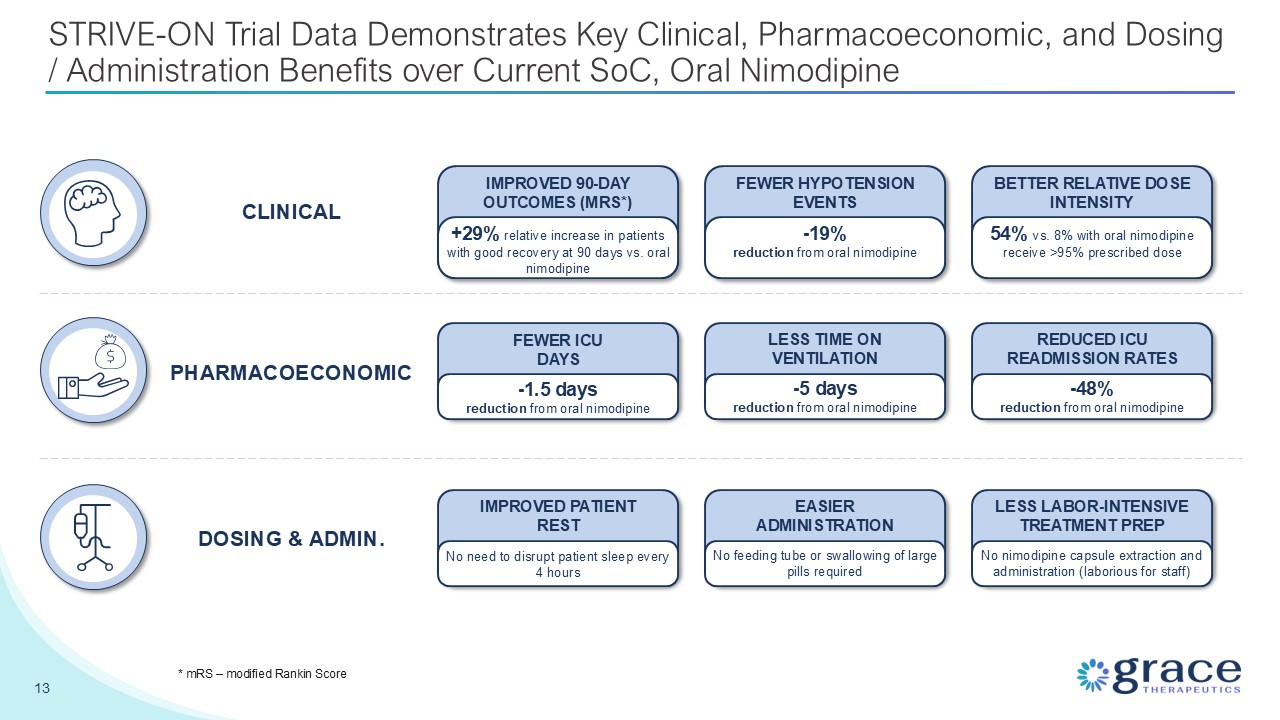
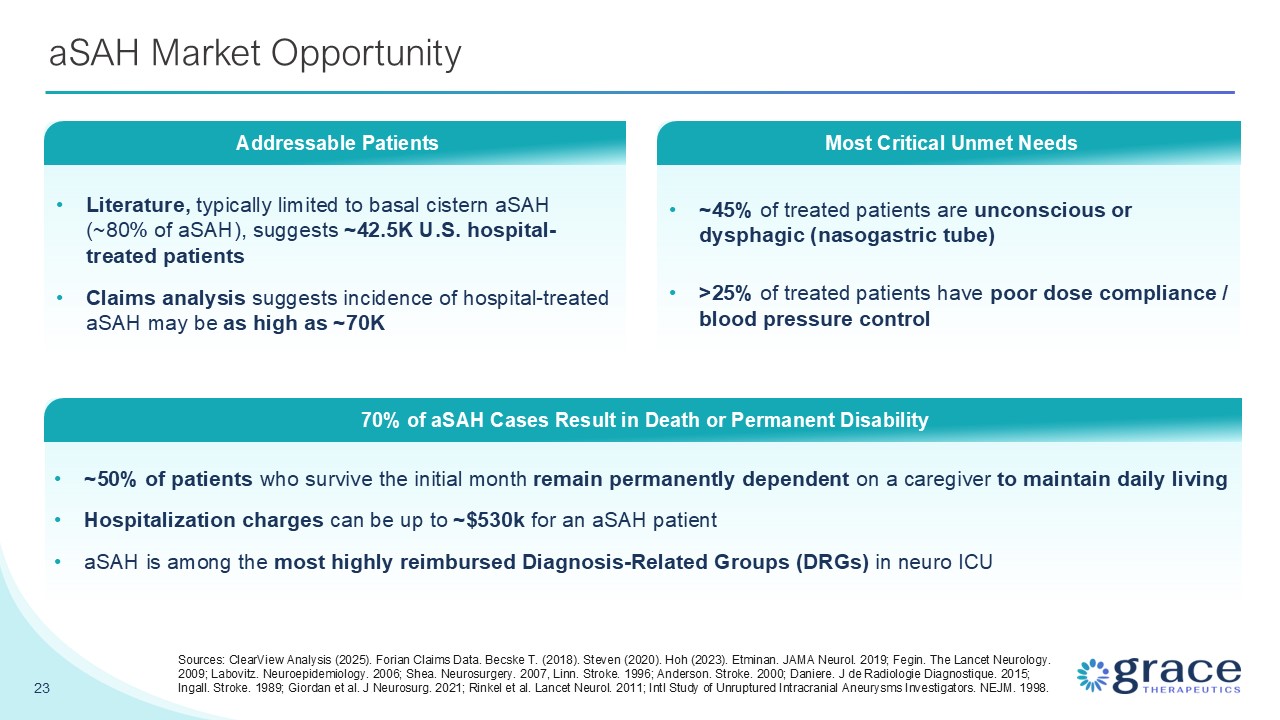
On August 22, 2025, the FDA accepted the Company’s NDA for GTx-104 for formal review, establishing April 23, 2026 as its PDUFA target date. The
application is supported by a comprehensive data package, including positive data obtained from the Company’s Phase 3 STRIVE-ON safety trial of GTx-104, whereby it met its primary endpoint and provided evidence of clinical benefit when
compared to orally administered nimodipine. These data were presented at the Neurocritical Care annual meeting, held in Montreal, Quebec, Canada in
September 2025.
|
|
|
• |
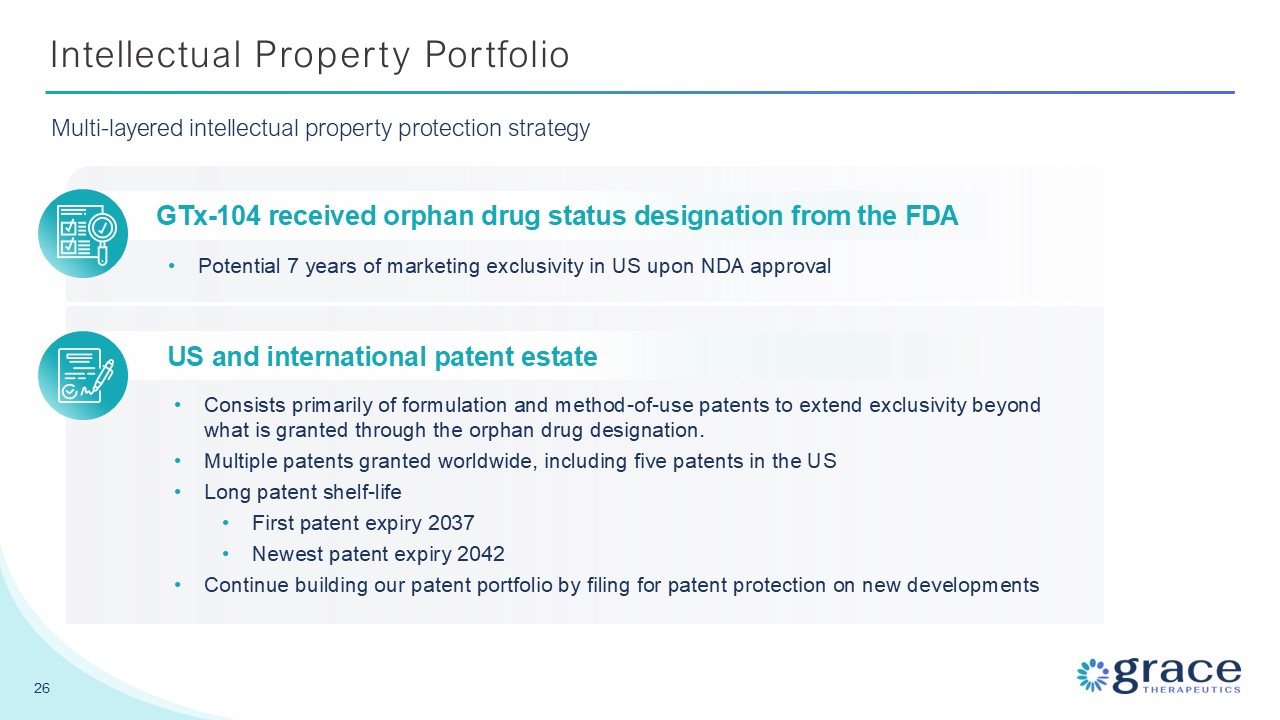
On September 16, 2025, U.S. Patent and Trademark Office issued a U.S. Patent No. 12,414,943, titled “Nimodipine Parenteral Administration”. The new method of use patent covers the
dosing regimen for IV administration of nimodipine used in the Phase 3 STRIVE-ON safety trial for GTx-104. Grace Therapeutics has established a multi-layered intellectual property estate for GTx-104, including five patents on the
composition of the Company’s formulation of nimodipine, which provide patent protection to 2037. The new patent on the IV dosing regimen for GTx-104 strengthens the Company’s intellectual property position and extends protection to 2043.
Grace has also been granted Orphan Drug Designation from the FDA, which provides GTx-104 with seven years of marketing exclusivity in United States upon FDA approval of the Company’s NDA.
|
|
|
• |
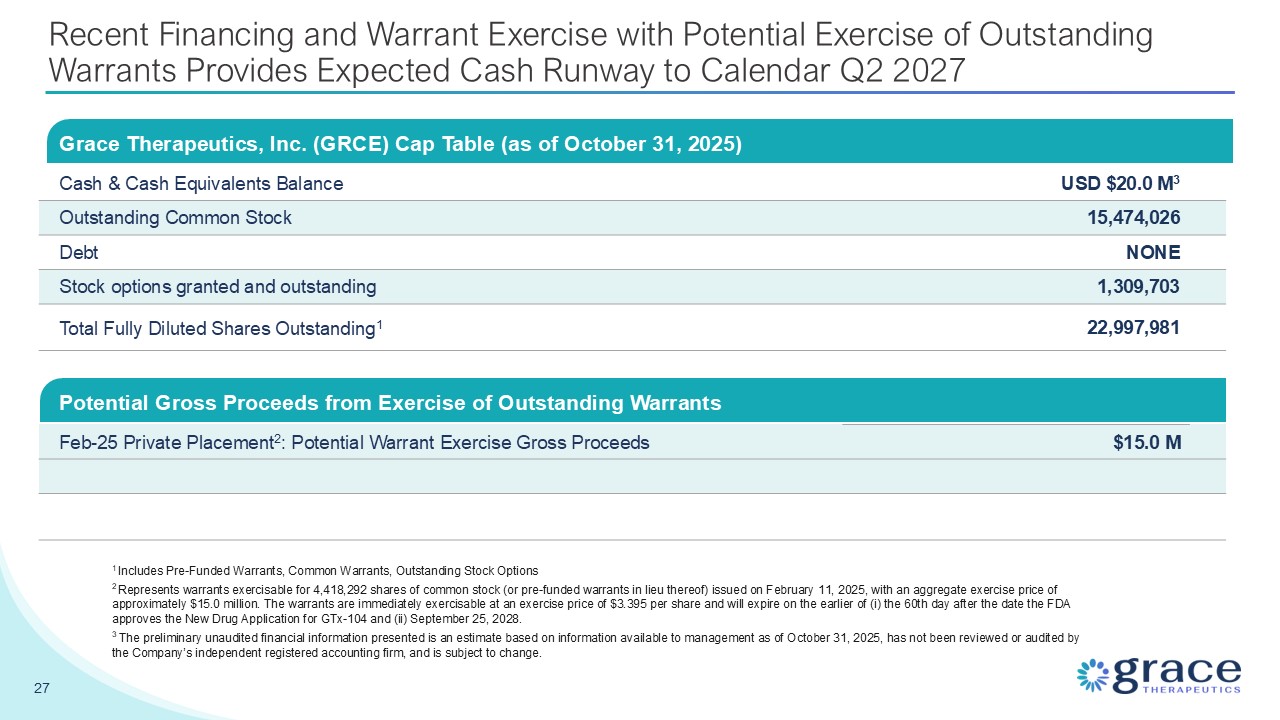
On October 23, 2025, the Company announced that it has secured approximately $4.0 million in additional funding through exercises of
common warrants that were previously issued in a private placement that the Company closed in September 2023. The Company issued 1,345,464 new shares of common stock at an exercise price of $3.003 per share. The remaining 1,190,927 common
warrants issued in the 2023 private placement expired as the 60th day after the FDA’s acceptance for review of the Company’s NDA for GTx-104 has passed. The Company estimates that its cash and cash equivalents were approximately $20.0
million as of October 31, 2025.
|
|
Grace Therapeutics Contact:
|
|
|
|
|
| Prashant Kohli |
|
|
Chief Executive Officer
|
|
|
Tel: 609-322-1602
|
|
|
Email: info@gracetx.com
|
|
|
www.gracetx.com
|
|
|
|
|
|
Investor Relations:
|
|
|
|
|
| LifeSci Advisors | |
|
Mike Moyer
|
|
|
Managing Director
|
|
|
Phone: 617-308-4306
|
|
|
Email: mmoyer@lifesciadvisors.com
|
|
September 30,2025
|
March 31,2025
|
|||||||
|
(Expressed in thousands except share data)
|
$
|
$
|
||||||
|
Assets
|
||||||||
|
Current assets:
|
||||||||
|
Cash and cash equivalents
|
16,862
|
22,133
|
||||||
|
Receivables
|
20
|
126
|
||||||
|
Prepaid expenses
|
416
|
453
|
||||||
|
Total current assets
|
17,298
|
22,712
|
||||||
|
Equipment, net
|
12
|
15
|
||||||
|
Intangible assets
|
41,128
|
41,128
|
||||||
|
Goodwill
|
8,138
|
8,138
|
||||||
|
Total assets
|
66,576
|
71,993
|
||||||
|
Liabilities and Stockholders’ equity
|
||||||||
|
Current liabilities:
|
||||||||
|
Trade and other payables
|
1,245
|
1,930
|
||||||
|
Total current liabilities
|
1,245
|
1,930
|
||||||
|
Derivative warrant liabilities
|
201
|
1,141
|
||||||
|
Deferred tax liability
|
2,312
|
2,312
|
||||||
|
Total liabilities
|
3,758
|
5,383
|
||||||
|
Commitments and contingencies
|
||||||||
|
Stockholders’ equity:
|
||||||||
|
Preferred stock, $0.0001 par value per share; 10,000,000 authorized; none issued and outstanding as of September 30, 2025
and March 31, 2025
|
—
|
—
|
||||||
|
Common stock, $0.0001 par value per share; 100,000,000 authorized; 14,128,562 and 13,718,106 shares issued and outstanding
as of September 30, 2025 and March 31, 2025, respectively
|
1
|
1
|
||||||
|
Additional paid-in capital
|
293,842
|
293,334
|
||||||
|
Accumulated other comprehensive loss
|
(6,038
|
)
|
(6,038
|
)
|
||||
|
Accumulated deficit
|
(224,987
|
)
|
(220,687
|
)
|
||||
|
Total stockholders’ equity
|
62,818
|
66,610
|
||||||
|
Total liabilities and stockholders’ equity
|
66,576
|
71,993
|
||||||
|
Three months ended
|
Six months ended
|
|||||||||||||||
|
September 30, 2025
|
September 30, 2024
|
September 30, 2025
|
September 30, 2024
|
|||||||||||||
|
(Expressed in thousands, except share and per share data)
|
$
|
$
|
$
|
$
|
||||||||||||
|
Operating expenses
|
||||||||||||||||
|
Research and development expenses, net of government assistance
|
(568
|
)
|
(2,976
|
)
|
(1,523
|
)
|
(5,684
|
)
|
||||||||
|
General and administrative expenses
|
(1,961
|
)
|
(1,855
|
)
|
(4,096
|
)
|
(4,109
|
)
|
||||||||
|
Loss from operating activities
|
(2,529
|
)
|
(4,831
|
)
|
(5,619
|
)
|
(9,793
|
)
|
||||||||
|
Foreign exchange (loss) gain
|
(8
|
)
|
13
|
3
|
5
|
|||||||||||
|
Change in fair value of derivative warrant liabilities
|
1,427
|
362
|
940
|
1,756
|
||||||||||||
|
Interest and other income, net
|
172
|
172
|
375
|
407
|
||||||||||||
|
Total other income, net
|
1,591
|
547
|
1,318
|
2,168
|
||||||||||||
|
Loss before income tax recovery
|
(938
|
)
|
(4,284
|
)
|
(4,301
|
)
|
(7,625
|
)
|
||||||||
|
Income tax benefit
|
—
|
852
|
—
|
1,576
|
||||||||||||
|
Net loss and total comprehensive loss
|
(938
|
)
|
(3,432
|
)
|
(4,301
|
)
|
(6,049
|
)
|
||||||||
|
Basic and diluted loss per share
|
(0.06
|
)
|
(0.30
|
)
|
(0.27
|
)
|
(0.53
|
)
|
||||||||
|
Weighted-average number of shares outstanding
|
15,924,522
|
11,506,234
|
15,924,522
|
11,506,234
|
||||||||||||