UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934
Date of Report (date of earliest event reported): August 18, 2025
iBio, Inc.
(Exact name of registrant as specified in charter)
Delaware
(State or other jurisdiction of incorporation)
| 001-35023 | 26-2797813 |
| (Commission File Number) | (IRS Employer Identification No.) |
11750 Sorrento Valley Road, Suite 200
San Diego, California 92121
(Address of principal executive offices and zip code)
(979) 446-0027
(Registrant’s telephone number including area code)
N/A
(Former Name and Former Address)
Check the appropriate box below if the Form 8-K filing is intended to simultaneously satisfy the filing obligation of registrant under any of the following provisions:
| ¨ | Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425) |
| ¨ | Soliciting material pursuant to Rule 14a-12(b) under the Exchange Act (17 CFR 240.14a-12) |
| ¨ | Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)) |
| ¨ | Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section 12(b) of the Act:
| Title of each class | Trading Symbol(s) | Name of each exchange on which registered |
| Common Stock, $0.001 par value per share | IBIO | The Nasdaq Stock Market LLC |
Indicate by check mark whether the registrant is an emerging growth company as defined in Rule 405 of the Securities Act of 1933 (§230.405 of this chapter) or Rule 12b-2 of the Securities Exchange Act of 1934 (§240.12b-2 of this chapter).
Emerging growth company ¨
If an emerging growth company, indicate by checkmark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ¨
Item 2.02. Results of Operations and Financial Condition.
On a preliminary unaudited basis, iBio, Inc., a Delaware company (the “Company,” “we” or “our”) expects to report that it had cash, cash equivalents and restricted cash of $8.8 million as of June 30, 2025.
The preliminary financial results above are the Company’s preliminary estimates based on currently available information and are subject to completion of the Company’s financial closing procedures. They do not present all necessary information for an understanding of the Company’s financial condition as of June 30, 2025. The Company’s independent registered public accounting firm has not conducted an audit or review of and does not express an opinion or any other form of assurance with respect to, the preliminary unaudited results. It is possible that the Company or its independent registered public accounting firm may identify items that require the Company to make adjustments to the preliminary estimates set forth above. We expect to complete our audited financial statements for the year ended June 30, 2025 later this quarter . Accordingly, undue reliance should not be placed on the preliminary estimates.
Item 8.01. Other Events.
Corporate Presentation
On August 18, 2025, the Company posted an updated corporate presentation on its website (the “Presentation”) for use in meetings with investors, analysts and others, which discusses the development of its obesity and cardiometabolic diseases pipeline.
The Presentation is attached as Exhibit 99.1 to this Current Report on Form 8-K and is incorporated herein by reference.
Business Description
The Company has updated its business description as set forth below:
Overview
We are a preclinical stage biotechnology company leveraging the power of Artificial Intelligence (“AI”) for the development of hard-to-drug precision antibodies in the cardiometabolic and obesity space. Our core mission is to harness the potential of AI and machine learning (“ML”) to unveil elusive biologics that stand out and have evaded other scientists. Through our innovative AI Drug Discovery Platform, we have been able to identify differentiated molecules aimed to address unmet needs by current GLP-1 receptor agonists.
We believe the future of obesity care lies not just in weight loss—but in quality weight loss. Current interventional therapies such as GLP-1 receptor agonists have ushered in a breakthrough era, yet challenges remain: muscle loss, fat regain after treatment cessation, and long-term tolerability. We are developing second-generation therapies to meet these unmet needs, using the power of AI-guided antibody design and advanced screening technologies. Our obesity strategy is built on three key principles. First, we aim to develop next-generation antibody therapeutics addressing limitations of current approved treatments, offering options with a goal to preserve muscle mass, target fat selectively, and provide durable weight loss with improved tolerability. Second, we are focusing on targets with strong human validation, which we believe both helps reduce development risk and increase the likelihood of clinical success. Lastly, we apply our integrated AI Drug Discovery Platform and deep scientific expertise to rapidly generate development-ready biologics, enabling us to move with speed and precision in a competitive and fast-evolving field. Our current therapeutics being developed are all in preclinical development. We have not completed any clinical trials in humans for any therapeutic protein product candidate produced using our technology and there is a risk that we will be unsuccessful in developing or commercializing any product candidates. As we continue to leverage our technology stack and develop our existing immune-oncology pre-clinical pipeline, we are also seeking strategic partners with the capabilities to more rapidly advance these programs towards the clinic.
Our current pre-clinical product candidate pipeline is set forth below.

IBIO-610
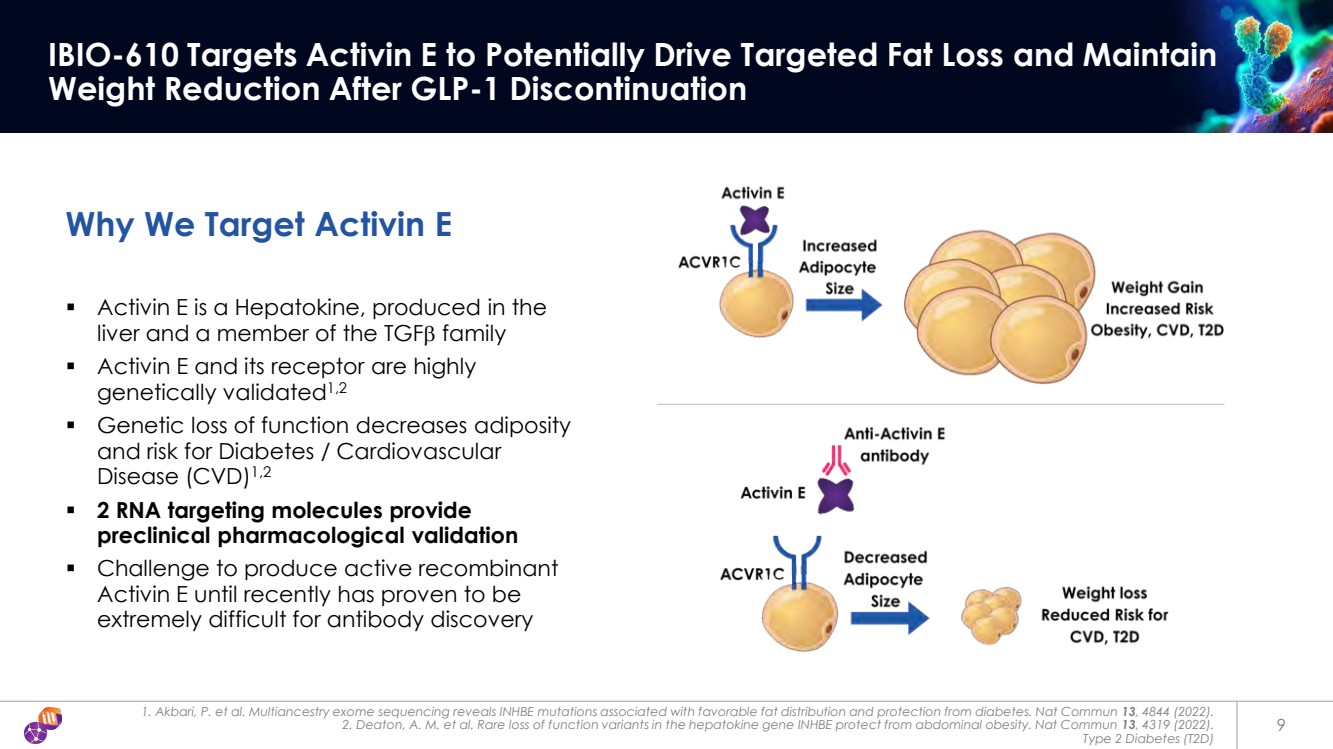
Activin E, like myostatin, is part of the TGF-β superfamily and has been implicated in the regulation of energy homeostasis and overall metabolic health. Human genetic studies provide compelling support for Activin E as a therapeutic target, as individuals carrying loss-of-function variants of the INHBE gene exhibit reduced visceral fat, improved lipid profiles, and lower risk of cardiometabolic diseases.
By leveraging our AI Drug Discovery Platform, we believe we have successfully identified the first antibody inhibiting Activin E. Preclinical data from multiple in vitro cell-based assays, including one on a human adipocyte cell line, demonstrated robust blockade of Activin E-mediated signaling. The antibody has been evaluated in multiple pre-clinical studies in a model of diet-induced obesity (DIO) in mice, both alone with bi-weekly dosing and in combination with semaglutide dosed daily. These results suggest IBIO-610 may induce fat-selective weight loss.
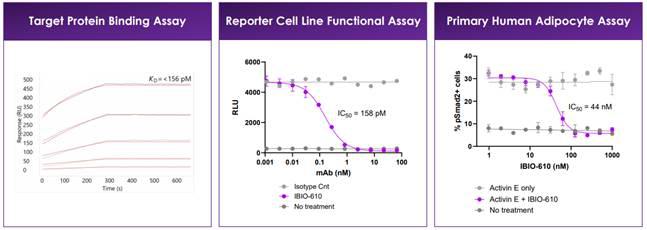
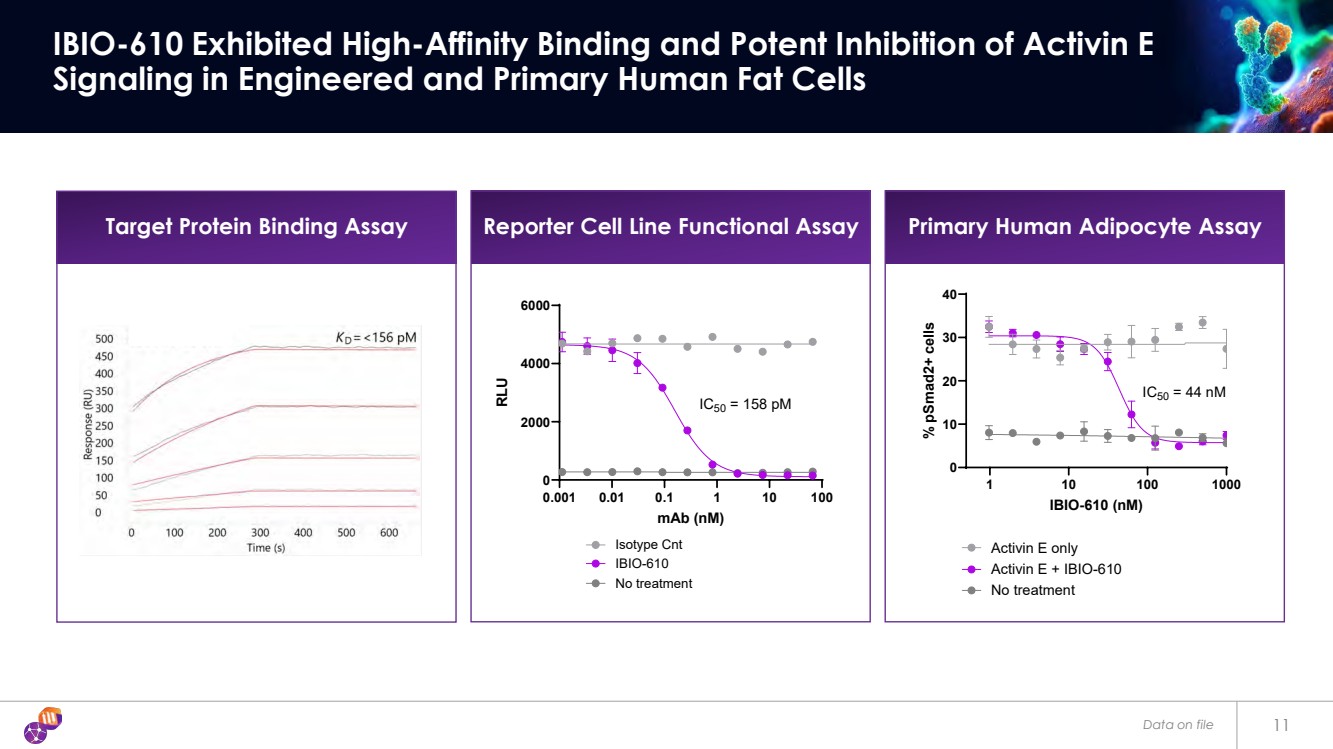
In vitro characterization of IBIO-610. Target protein binding measured via SPR. Reporter cell line assay used HEK293 reporter cell line with ALK7 receptor stably integrated. 200pM Activin E used. Differentiated human adipocyte, treated with 100nM Activin E.
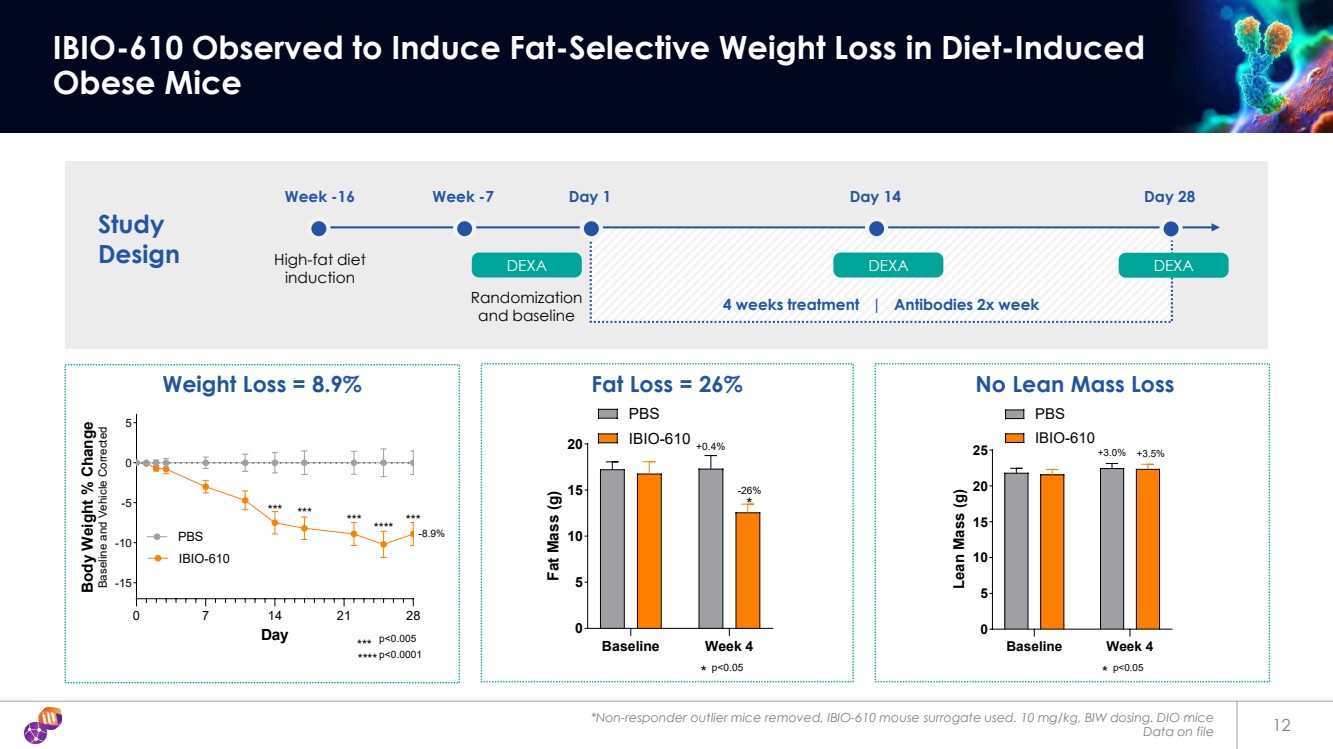
In a DIO mouse model, IBIO-610 was administered biweekly at 10 mg/kg for four weeks to evaluate its effects as a monotherapy. Treated mice were observed to have a 8.9% reduction in body weight compared to baseline and placebo, with body composition analysis revealing a 26% reduction in fat mass and no measurable loss of lean mass. Outlier non-responder mice were excluded.
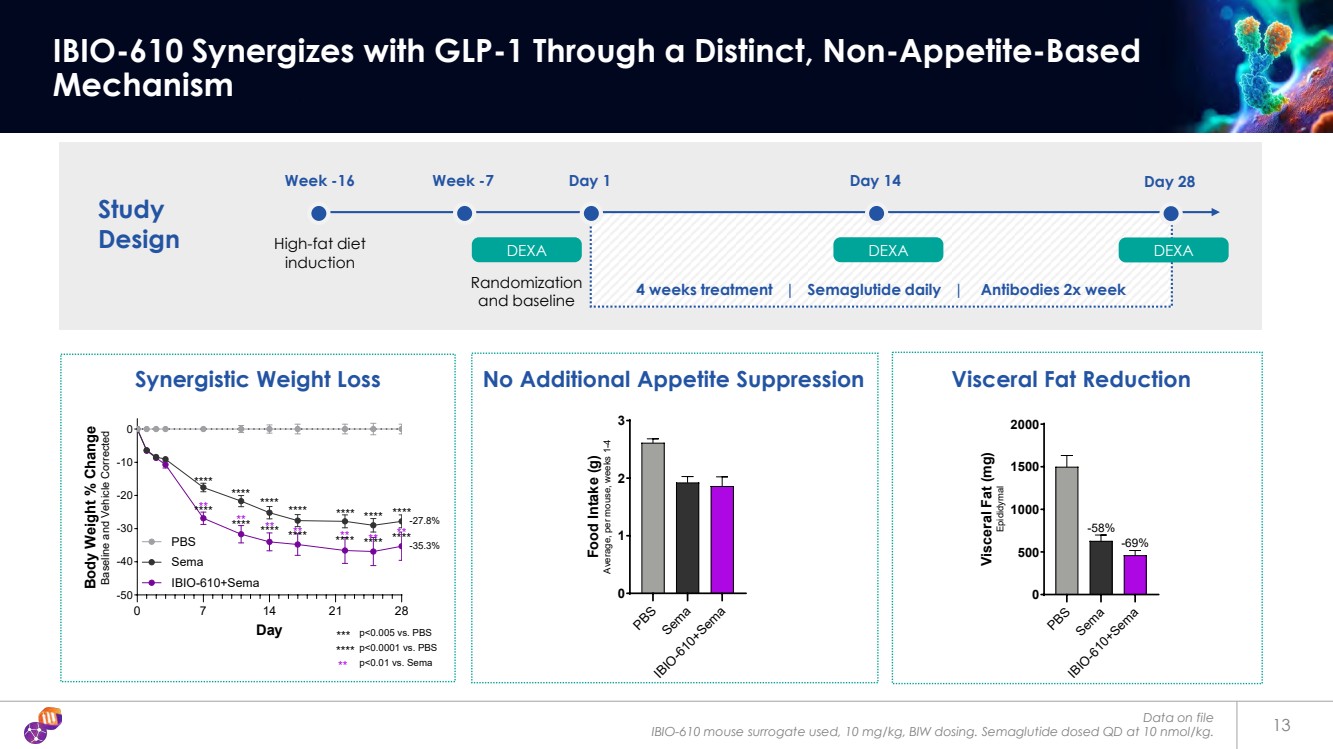
To test potential combination therapy with incretin treatments, IBIO-610 was dosed biweekly alongside daily semaglutide. While semaglutide alone produced a 27.8% reduction in body weight (baseline and placebo adjusted), the combination resulted in a more pronounced 35.3% weight loss, without any additive effect on food intake. The combination also led to a greater reduction in visceral fat compared to semaglutide alone, suggesting complementary mechanisms that enhance metabolic benefit.
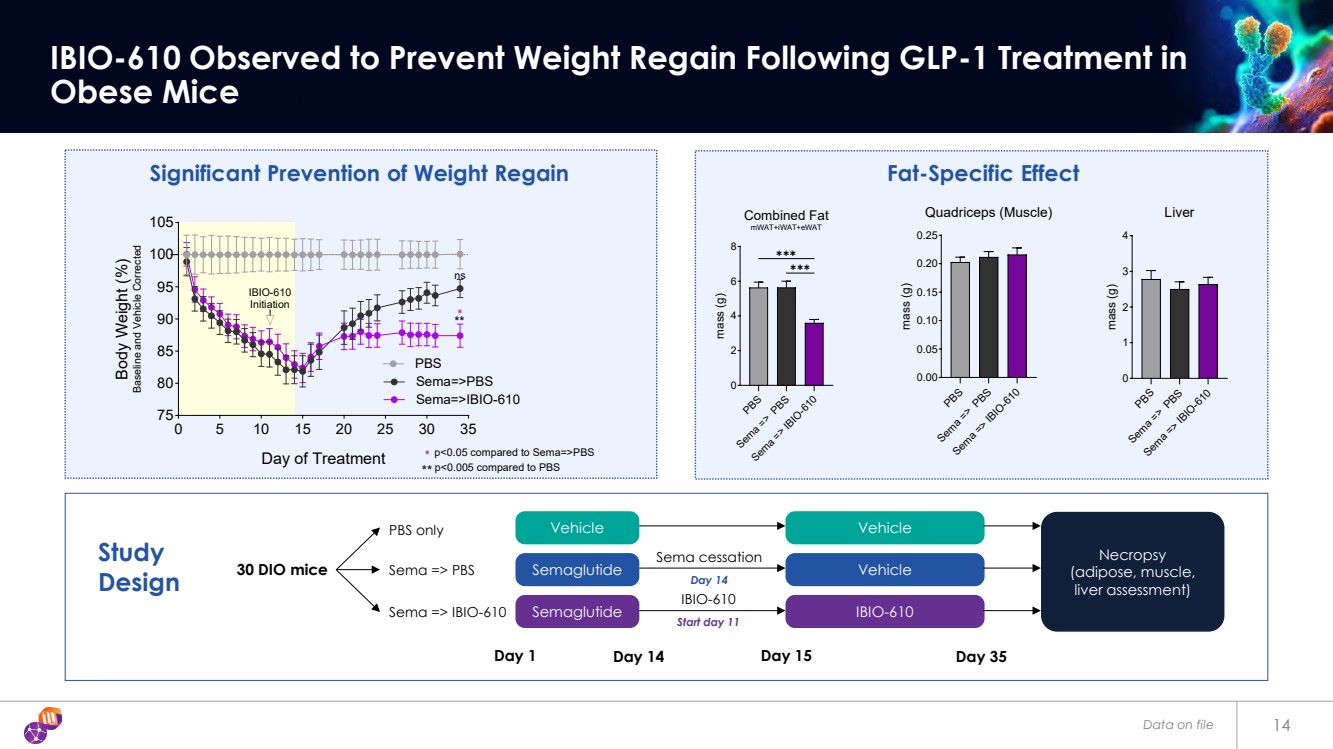
IBIO-610 was also tested as a maintenance therapy following cessation of semaglutide treatment. In this model, DIO mice were first dosed with semaglutide for two weeks, leading to approximately 18% weight loss. Upon stopping semaglutide, control mice regained 71% of the lost weight within three weeks, with fat mass levels returning to those of untreated animals. In contrast, mice receiving IBIO-610 at the time of semaglutide discontinuation regained only 28% of the lost weight and retained significantly lower fat mass at study termination, highlighting the potential of IBIO-610 to prevent rebound weight gain.
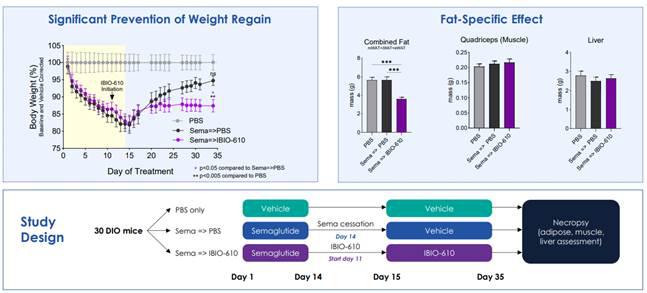
Prevention of weight regain after cessation of GLP-1 treatment in mouse model of obesity by IBIO-600. n=10 per group, IBIO-610 dosed S.C. at 10 mg/kg twice per week. Semaglutide dosed at 10nmol/kg S.C. daily. Organ weights determined via necropsy.
Myostatin x Activin A Bispecific Antibody
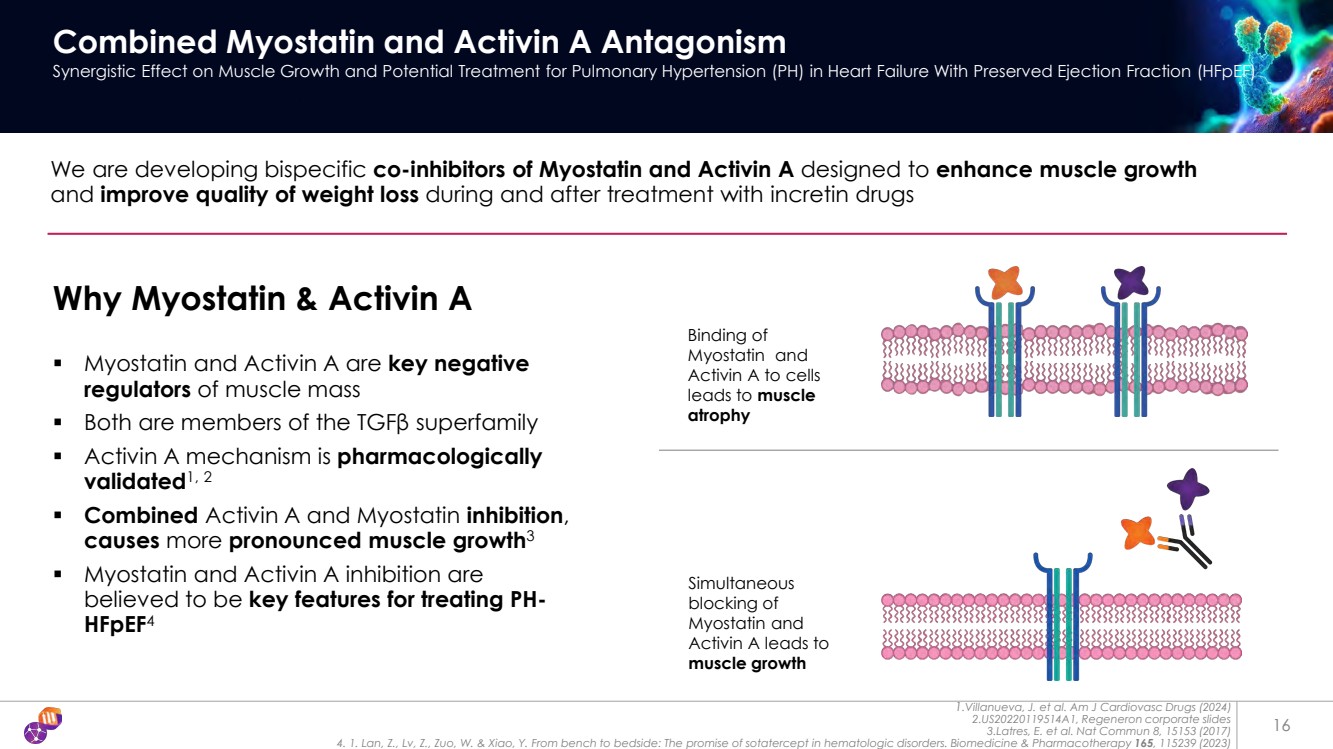
Activin A is another member of the TGF-β family and is known to modulate muscle growth among its various biological functions. The therapeutic potential of targeting Activin A has been observed in garetosmab, an Activin A antagonist antibody that exhibited promising outcomes in early clinical trials and in published Non-Human Primate (“NHP”) data.
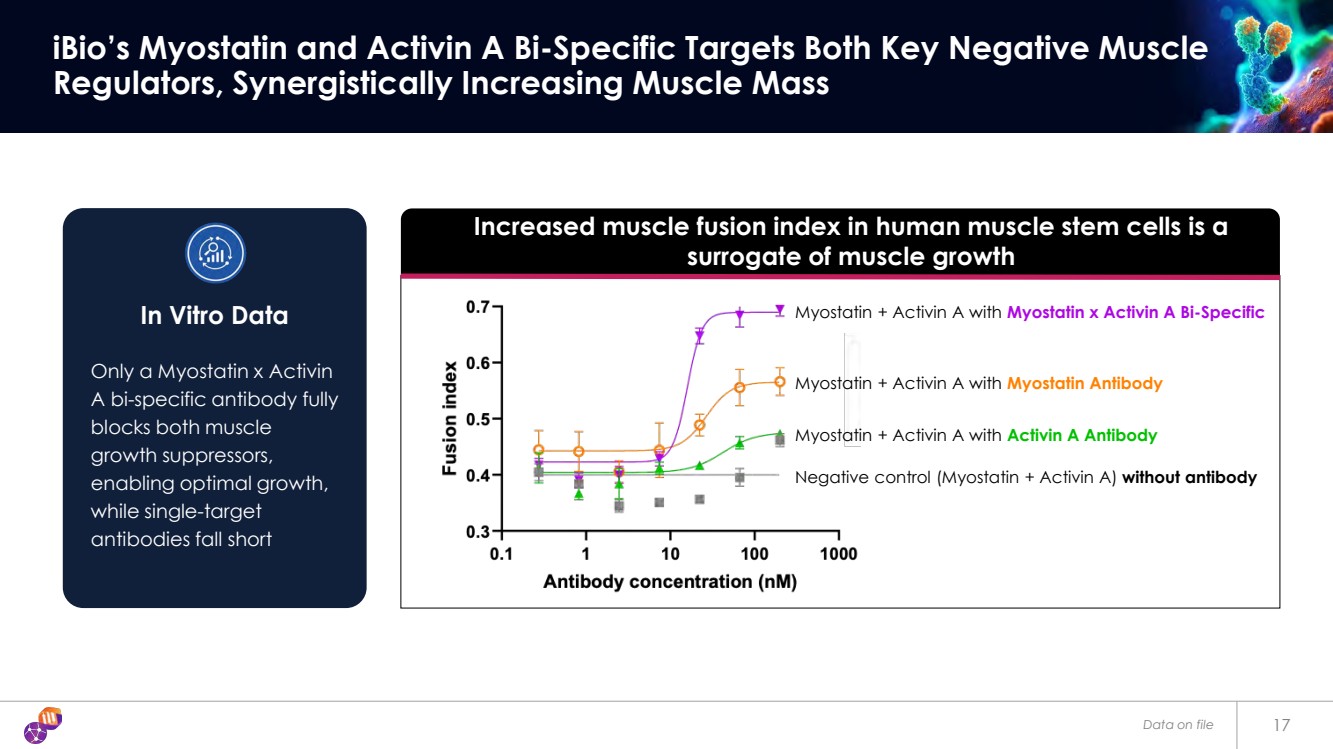
Building on these insights, we initiated a program to develop a bispecific antibody targeting both myostatin and Activin A. Leveraging our StableHu™ platform and mammalian display, this program is in late discovery, where multiple parameters, such as binding affinity, expression levels, and stability, are being optimized. Early in vitro findings in human muscle progenitor cells suggest that the bispecific candidate induces a stronger differentiation of progenitor cells into mature muscle cells compared to antibodies targeting only myostatin or Activin A alone. Increased muscle fusion index in human muscle stem cells, as shown in the chart below, is a surrogate of muscle growth.
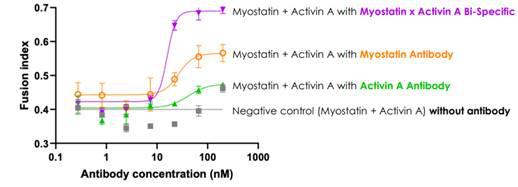
Reversal of the myostatin or Activin A-mediated inhibition of human muscle stem cell fusion
IBIO-600
Myostatin, also known as growth differentiation factor 8 (GDF8), is a member of the transforming growth factor-β (TGF-β) family that regulates and limits skeletal muscle growth. A loss of function in the myostatin gene eliminates this inhibitory effect, leading to increased muscle mass and strength. This genetic alteration results in significant muscle hypertrophy (increased size) and hyperplasia (increased number of muscle fibers). While these effects can enhance muscle development, they may also have implications for overall metabolism and cardiovascular health.
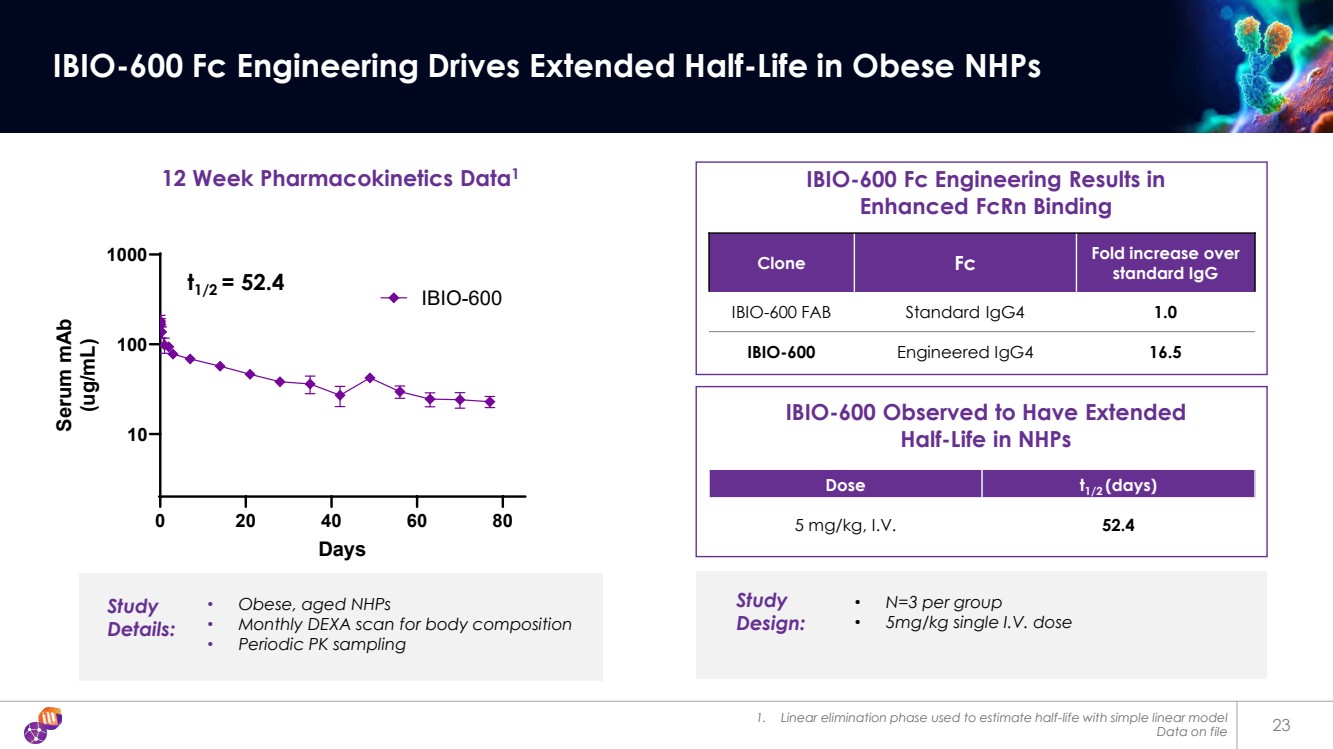
In April 2024, as result of our collaboration with AstralBio, we initiated a program to discover and develop a long-acting anti-myostatin antibody. Using our StableHu platform coupled with mammalian display, we optimized hit antibodies across multiple parameters, including affinity for myostatin, binding to the FcRn receptor, expression levels in mammalian cells, and resistance to poly-reactivity and aggregation. The final candidate, IBIO-600, was also observed to have a beneficial profile between thermostability and resistance to stress conditions during initial testing.
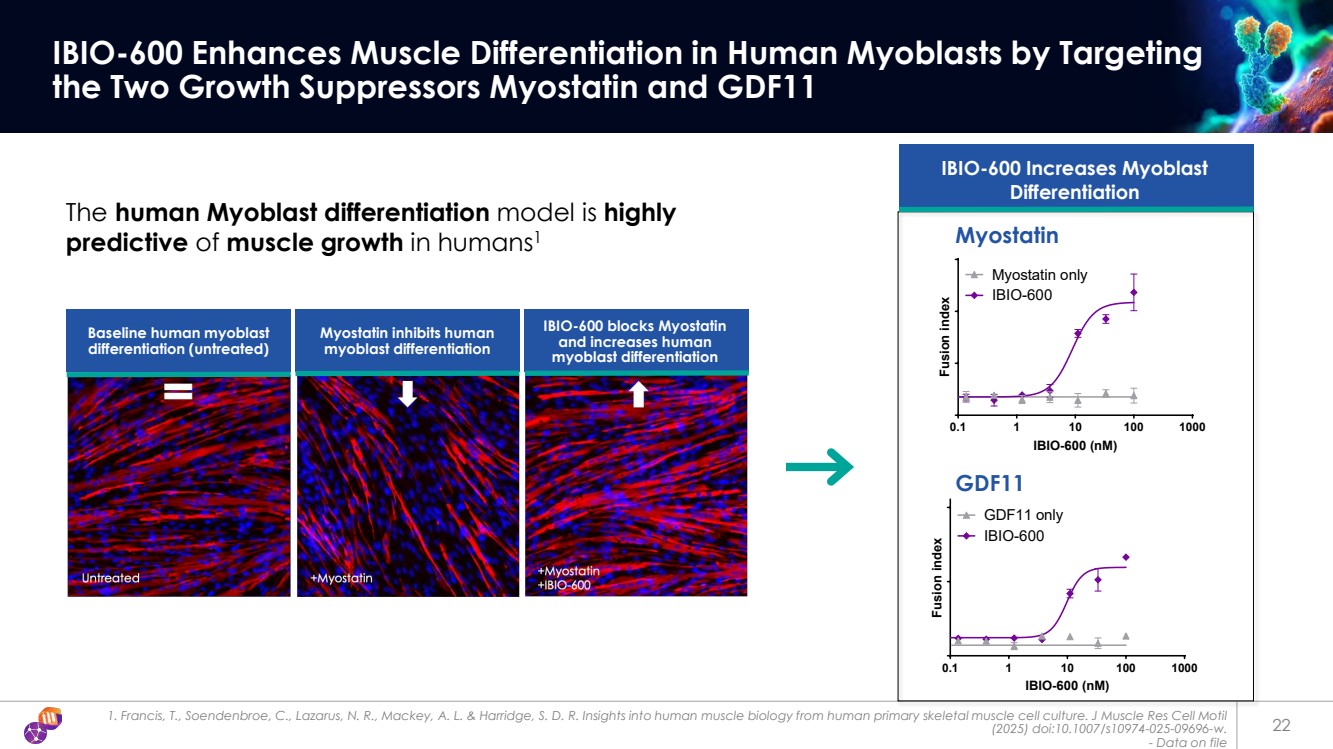
In vitro, IBIO-600 was evaluated in human muscle progenitor cells, where it potently inhibited myostatin. This inhibition facilitated the differentiation of progenitor cells into mature human muscle cells. In interim data from a preclinical study in obese mice, we observed that IBIO-600 dose-dependently prevented lean mass loss when administered in combination with a GLP-1 receptor agonist.
In November 2024, we manufactured a non-cGMP batch of IBIO-600 for a NHP study in obese and elderly NHPs. The primary goal of the study was to assess the pharmacokinetic (“PK”) profile of IBIO-600. The study consisted of two dose levels, a low dose of 5 mg/kg and a high dose of 50 mg/kg, with a single subcutaneous injection in each case. In addition to monitoring PK in serum, the study analyzed body composition changes over time by employing DEXA scans, measuring lean and fat mass.
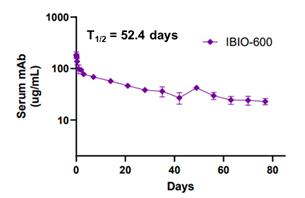
Serum concentration of IBIO-600 in obese NHPs after a single 5 mg/kg I.V. dose. n=3
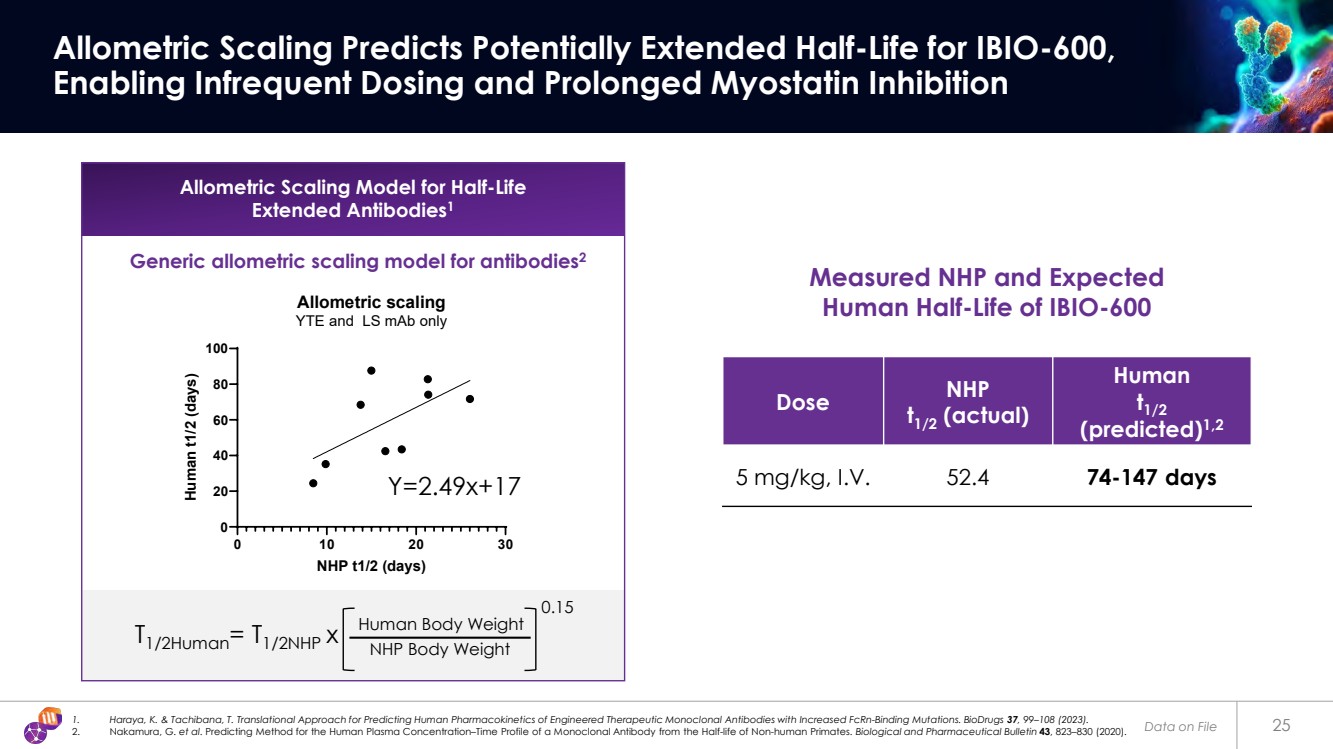
The study consisted of six NHPs, sorted randomly into the low and high dose groups. IBIO-600 promoted an increase in lean mass and a reduction in fat mass from baseline values. Standard PK calculations indicated the half-life of IBIO-600 in NHPs was approximately 40 to 52 days. By using multiple allometric scaling approaches, we estimated the half-life in humans of IBIO-600 as falling with a range of 57-147 days.
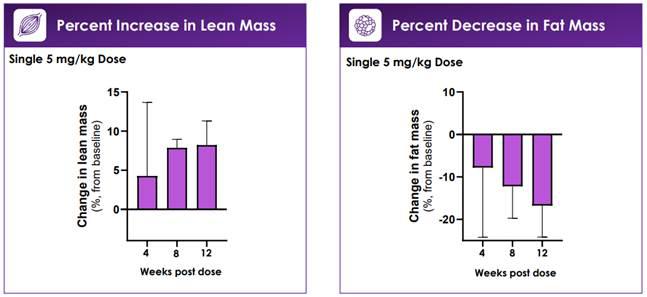
Change in Lean and Fat Mass in obese NHPs treated with a single 5 mg/kg I.V. dose of IBIO-600. N=3 per group. Region of Interest DEXA scan on gluteal and thigh region.
Following the NHP pharmacokinetic study, we initiated Chemistry, Manufacturing, and Controls manufacturing and nonclinical toxicology activities to support advancement of IBIO-600 toward clinical development. We have established a stable cell line, completed process and formulation development, and manufactured a good laboratory practices (“GLP”) toxicology batch at 200L scale. In parallel, we launched a nonclinical toxicology program, initiating both rat and NHP dose range finding studies as well as a rat GLP tox study, with plans underway for an NHP GLP tox study. All studies are progressing as planned, with no notable safety findings observed to date. We intend to continue progressing the development of IBIO-600 through IND in obesity and other muscle sparing diseases.
AI Discovery Tools
Through our innovative AI Drug Discovery Platform, we champion a culture of innovation by identifying novel targets, forging strategic collaborations to enhance efficiency, diversify pipelines, with the goal of accelerating preclinical processes. Our proprietary technology stack is designed to minimize downstream development risks by employing AI-guided epitope-steering and monoclonal antibody (“mAb”) optimization.
Our proprietary technology stack combines Epitope Steering, our patented AI engine that directs antibody binding to precisely defined regions of target proteins, increasing selectivity and therapeutic impact; StableHu, a generative AI tool that rapidly optimizes antibodies for expression, stability, and manufacturability; and mammalian display-based multidimensional screening, enabling simultaneous optimization of affinity, specificity, and half-life in a single selection step. Together, these tools power a fully integrated platform that allows us to go from concept to in vivo proof-of-concept within weeks, accelerating the development of first-in-class and best-in-class biologics. Our EngageTx technology enables us to target bi-specific molecules. Data from a number of in vitro tumor cell-killing assays suggests that our most advanced MUC16 clone, when combined with eight distinct CD3 binders using our EngageTx technology, revealed a potency range of approximately 33,000 fold. With the ability to navigate sequence diversity and promote Human-Cyno cross reactivity while mitigating cytokine release, our goal is to enhance agility and bolster preclinical safety assessments. Another key feature of our technology stack is our ShieldTx™ masking technology, which keeps antibodies inactive until they reach diseased tissue. At that point, the masks are removed and the antibodies become active, all with the goal of broadening the therapeutic window and potentially improving both efficacy and safety.
Partnered Programs
Amylin Receptor Agonist Engineered Antibody
In collaboration with AstralBio, we are working to develop an amylin receptor antibody, a potentially highly promising mechanism in obesity treatment. Along with AstralBio, we are discovering and optimizing both dual amylin and calcitonin receptor (DACRA)-like engineered antibodies, and selective amylin receptor agonist antibodies while avoiding engagement of the calcitonin receptor. Improved selectivity may translate into tolerability and efficacy advantages. Leveraging our AI Drug Discovery Platform, combining soluble G protein-coupled receptor (“GPCR”) analogues with mammalian display, we have engineered agonists with tailored activity across specific amylin receptor subtypes, showcasing our ability to address complex membrane protein targets with precision.
Risk Factors
The Company has updated certain of its risk factors. The risk factors listed below should be read in conjunction with the risk factors disclosed in the Company’s Annual Report on Form 10-K for the year ended June 30, 2024 and its Quarterly Reports on Form 10-Q for the quarters ended September 30, 2024, December 31, 2024 and March 31, 2025.
Our most advanced product candidates depend on intellectual property licensed from third parties and termination of any of these or future licenses could result in the loss of significant rights, which could adversely affect our business, results of operations and financial condition.
We are dependent on patents, know-how and proprietary technology, some of which is owned and some of which is licensed from others. With respect to our obesity and cardiometabolic program, we have a license to four provisional applications for a future U.S. patent application that relate to our leading anti-myostatin antibody product candidate, IBIO-600, alone and when used in combination with Activin A. In addition, we have a license to three provisional applications for a future U.S. patent application that relate to our Activin E engineered antibody candidate, IBIO-610. These licenses exist under two exclusive license agreements (the “AstralBio Licenses”) with AstralBio granting us exclusive, worldwide licenses to develop, manufacture, commercialize and otherwise exploit, IBIO-600 and IBIO-610, which are our most advanced preclinical product candidates. Any termination of these licenses could result in the loss of significant rights and could harm our ability to commercialize our product candidates. The AstralBio Licenses impose, and we expect that future license and acquisition agreements will impose, various diligence, milestone payments and other obligations on us. If we fail to comply with our obligations under current or future intellectual property license agreements, we may be required to pay damages and the licensor may have the right to terminate the license. Any termination of these licenses could result in the loss of significant rights and could harm our ability to develop, manufacture and/or commercialize our product candidates.
Moreover, if disputes over intellectual property that we have licensed prevent or impair our ability to maintain our current licensing arrangements on commercially acceptable terms, we may be unable to successfully develop and commercialize the affected product candidates. Our business also would suffer if any current or future licensors fail to abide by the terms of the license, if the licensors fail to enforce licensed patents against infringing third parties, if the licensed patents or other rights are found to be invalid or unenforceable, or if we are unable to enter into necessary licenses on acceptable terms. Moreover, our licensors may own or control intellectual property that has not been licensed to us and, as a result, we may be subject to claims, regardless of their merit, that we are infringing or otherwise violating the licensor’s rights.
Our AI/ML platform leverages internal data as well as data from third parties. Defects in, or loss of access to, our databases or those of third parties may impair our ability to discover additional targets and develop our product candidates.
We use our AI/ML platform to improve our target discovery programs by improving the hit finding and lead optimization process and by helping us identify desired epitope targets on target proteins. Our AI/ML platform accesses and has been trained using third-party databases. If access to this data is lost or limited, or if this data becomes outdated, it may delay or otherwise adversely affect our ability to develop our product candidates. Our AI/ML platform is the subject of several patent filings in the U.S. including one issued patent and one pending patent application directed to our epitope-steering AI engine; two provisional applications for a future patent application directed to our optimized next-generation CD3 T-cell engager antibody EngageTx platform; and a patent application directed to our ShieldTx antibody masking technology. Certain aspects of our AI/ML program are also protected by trade secrets. However, our competitors may render our approaches obsolete, by advances in existing technological approaches or the development of new or different approaches, potentially eliminating the advantages in our drug discovery process that we believe we derive from our research approach and proprietary technologies.
Our proprietary software tools are inherently complex and may contain defects or errors. Errors may result from the interface of our hardware or proprietary software tools with our data or third-party systems and data. The risk of errors is particularly significant when new software or hardware is first introduced or when new versions or enhancements of existing software or hardware are implemented. Any errors, defects, disruptions or other performance problems with our software, hardware or data sets could hurt our ability to gather valuable insights that we intend to use to assist in developing our current and future product candidates and drive our drug discoveries. We outsource the majority of the core network infrastructure relating to our AI/ML platform to third-party hosting services. We have limited control, if any, over any of these third parties, and we cannot guarantee that such third-party providers will not experience system interruptions, outages or delays or deterioration in their performance. We have experienced, and expect that in the future we may again experience, interruptions, delays and outages in service and availability from time to time due to a variety of factors, including infrastructure changes, human or software errors, website hosting disruptions and capacity constraints.
Furthermore, the development and use of AI/ML present various privacy and security risks that may impact our business. AI/ML are subject to privacy and data security laws, as well as increasing regulation and scrutiny. For example, several jurisdictions around the globe, including Europe and certain U.S. states, have proposed, enacted or are considering laws governing the development and use of AI/ML. We expect other jurisdictions will adopt similar laws. Additionally, certain privacy laws extend rights to consumers (such as the right to delete certain personal data) and regulate automated decision making, which may be incompatible with our use of AI/ML. These obligations may make it harder for us to conduct our business using AI/ML, lead to regulatory fines or penalties, require us to change our business practices or retrain our AI/ML or prevent or limit our use of AI/ML. For example, the Federal Trade Commission has required other companies to turn over (or disgorge) valuable insights or trainings generated through the use of AI/ML where they allege the company has violated privacy and consumer protection laws. If we cannot use AI/ML or our use is restricted, our preclinical research and development programs may be less efficient, or we may be at a competitive disadvantage. The occurrence of any of the foregoing events could prevent us from leveraging our AI/ML capability and software to help us develop our product candidates more efficiently than existing industry tools and have a material adverse effect on our business, financial condition, results of operations or prospects.
Inappropriate or controversial data practices by data scientists, engineers and end-users of our or our competitors’ products could also impair the acceptance of AI products. Though our business practices are designed to mitigate many of these risks, if we enable or offer AI products that are controversial because of their purported or real impact on human rights, privacy, employment, or other social issues, we may experience brand or reputational harm.
Our investments in deploying AI technologies may be substantial and may be more expensive than anticipated. If our AI Drug Discovery Platform does not function reliably, fails to meet expectations in terms of performance, or cannot be fully utilized due to increasing regulation or reputational concerns, we may be unable to provide such services we’ve contracted for with third parties, our customers may stop using our products, or our competitors may incorporate AI technology into their products or services more successfully than we do, all of which may impair our ability to effectively compete in the market.
Preclinical and clinical development involves a lengthy and expensive process, with an uncertain outcome. We or our collaborators may incur additional costs or experience delays in completing, or ultimately be unable to complete, the development and commercialization of our current product candidates or any future product candidates.
All of our product candidates are in preclinical development. The risks associated with our product candidates not proceeding through clinical development is high. We expect it will be many years before we commercialize any product candidate, if ever. The product candidates we are developing are unproven, which makes it difficult to accurately predict the challenges we may face with respect to our product candidates as they proceed through development. It is also impossible to predict whether our clinical trials will proceed through registrational trials and when or if any of our product candidates will receive regulatory approval. To obtain the requisite regulatory approvals to commercialize any product candidates, we must demonstrate through extensive preclinical studies and lengthy, complex and expensive clinical trials that our product candidates are safe and effective in humans. Clinical testing can take many years to complete, and its outcome is inherently uncertain. Commencing any future clinical trials is subject to finalizing the trial design and submitting an application to the FDA or a comparable foreign regulatory authority. Even after we make our submission, the FDA or comparable foreign regulatory authority could disagree that we have satisfied their requirements to commence our clinical trials or disagree with our trial design, which may require us to complete additional studies or trials, amend our protocols or impose stricter conditions on the commencement of clinical trials.
Alternative technologies may supersede our technologies or make them noncompetitive, which would harm our ability to generate future revenue.
The manufacture of precision antibodies and use of artificial intelligence to do so is intensely competitive. There are currently extensive research efforts in this field, which result in rapid technological progress that can render existing technologies obsolete or economically noncompetitive. If our competitors succeed in developing more effective technologies or render our technologies obsolete or noncompetitive, our business will suffer. Many universities, public agencies and established pharmaceutical, biotechnology, and other life sciences companies with substantially greater resources than we have are developing and using technologies and are actively engaging in the development of products similar to or competitive with our technologies and products. To remain competitive, we must continue to invest in new technologies and improve existing technologies. To make such renewing investment we will need to obtain additional financing and/or collaborations. If we are unable to secure such financing, we will not have sufficient resources to continue such investment. In addition, they also have significantly greater experience in the discovery and development of products, as well as in obtaining regulatory approvals of those products in the United States and in foreign countries. Our current and potential future competitors also have significantly more experience commercializing drugs that have been approved for marketing. Mergers and acquisitions in the pharmaceutical and biotechnology industries could result in even more resources being concentrated among a small number of our competitors.
Our competitors may develop technologies and products or devise methods and processes for protein expression that are faster, safer, more efficient or less costly than that which can be achieved using our technologies which may render our technologies obsolete. Our competitors might succeed in obtaining regulatory approval for competitive products more rapidly than we can for our product candidates. In addition, the pharmaceutical and biotechnology industry is characterized by rapid technological change. Because our research approach integrates many technologies, it may be difficult for us to remain current with the rapid changes in each technology. If we fail to stay at the forefront of technological change, we may be unable to compete effectively. Our competitors may render our technologies obsolete by advancing their existing technological approaches or developing new or different approaches. There has been and continues to be substantial academic and commercial research effort devoted to the development of such methods and processes. If successful competitive methods are developed, it may undermine the commercial basis for our products and our technologies and related services.
For our obesity and cardiometabolic disease, not only will we compete with fully integrated pharmaceutical companies, but we will also compete with various companies that have developed or are trying to develop weight-loss treatments or cardiovascular therapies. Certain of our competitors have substantially greater capital resources, large customer bases, broader product lines, sales forces, greater marketing and management resources, larger research and development staffs with extensive facilities and equipment than we do and have more established reputations as well as global distribution channels. Our most significant competitors, among others, are fully integrated pharmaceutical companies such as Eli Lilly and Company, Novo Nordisk A/S, Amgen Inc., Bristol-Myers Squibb Company, Merck & Co., Inc., Novartis AG, MedImmune, LLC (a wholly owned subsidiary of AstraZeneca plc), Johnson & Johnson, Pfizer Inc., Merck KGaA and Sanofi SA, and more established biotechnology companies such as Genentech, Inc. (a member of the Roche Group), Gilead Sciences, Inc. and its subsidiary Kite Pharma, Inc, and Regeneron Pharmaceuticals. We also compete with additional companies who are more advanced in the obesity and cardiometabolic space, such as Keros Therapeutics, Inc., Scholar Rock, Inc., Biohaven, Ltd., Structure Therapeutics, Inc., Viking Therapeutics, Inc., Veru Therapeutics Inc., Zealand Pharma A/S, Metsera Therapeutics, Inc., Terns Pharmaceuticals, Inc., Skye Bioscience, Inc., SixPeaks Bio AG, Laekna, Inc., Wave Life Sciences Ltd., Arrowhead Pharmaceuticals, Inc., Alnylam Pharmaceuticals, Inc., and Helicore Biopharmaceuticals, Inc., as well as tech enabled drug discovery companies such as Recursion, Inc., Abcellera Biologics, Inc., Cellarity, Inc., BenevolentAI, and others, some of which have substantially greater financial, technical, sales, marketing, and human resources than we do.
We may conduct our initial clinical studies for IBIO-610 and our other product candidates outside of the United States. However, the FDA and other foreign equivalents may not accept data from such studies, in which case our development plans will be delayed, which could materially harm our business.
We may conduct our Phase 1 clinical studies for IBIO-610 and other product candidates in Australia, Canada or other foreign countries. The acceptance of study data from clinical studies conducted outside the United States or another jurisdiction by the FDA or applicable foreign authority may be subject to certain conditions or may not be accepted at all. In cases where data from foreign clinical studies are intended to serve as the sole basis for marketing approval in the United States, the FDA will generally not approve the application on the basis of foreign data alone unless (i) the data are applicable to the U.S. population and U.S. medical practice; (ii) the studies were performed by clinical investigators of recognized competence and pursuant to good clinical practices (“GCP”) regulations; and (iii) the data may be considered valid without the need for an on-site inspection by the FDA, or if the FDA considers such inspection to be necessary, the FDA is able to validate the data through an on-site inspection or other appropriate means. In addition, even where the foreign study data are not intended to serve as the sole basis for approval, the FDA will not accept the data as support for an application for marketing approval unless the study is well-designed and well-conducted in accordance with GCP requirements and the FDA is able to validate the data from the study through an onsite inspection if deemed necessary. Many foreign regulatory authorities have similar approval requirements. In addition, such foreign studies would be subject to the applicable local laws of the foreign jurisdictions where the studies are conducted. There can be no assurance that the FDA or any applicable foreign authority will accept data from studies conducted outside of the United States or the applicable jurisdiction. If the FDA or any applicable foreign authority does not accept such data, it would result in the need for additional studies, which could be costly and time-consuming, and which may result in current or future product candidates that we may develop not receiving approval for commercialization in the applicable jurisdiction.
We believe that clinical data generated in Australia and Canada or other foreign countries will be accepted by the FDA and its foreign equivalents outside of the United States; however, there can be no assurance the FDA or applicable foreign authorities will accept data from any other clinical studies that we may conduct in Australia, Canada or other foreign countries. If the FDA or applicable foreign authorities do not accept any such data, we would likely be required to conduct additional Phase 1 clinical studies, which would be costly and time consuming, and delay aspects of our development plan, which could harm our business.
Conducting clinical studies outside the United States exposes us to additional risks, including risks associated with:
| · | additional foreign regulatory requirements; |
| · | foreign exchange fluctuations; |
| · | compliance with foreign manufacturing, customs, shipment and storage requirements; |
| · | cultural differences in medical practice and clinical research; and |
| · | diminished protection of intellectual property in some countries. |
Item 9.01. Financial Statements and Exhibits.
(d) Exhibits
| Exhibit No. | Description | |
| 99.1 | Corporate Presentation of iBio, Inc., dated August 2025 | |
| 104 | Cover Page Interactive Data File (embedded within the Inline XBRL document) |
SIGNATURES
Pursuant to the requirements of the Securities Exchange Act of 1934, as amended, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
| Date: August 18, 2025 | IBIO, INC. | |
| By: | /s/ Marc A. Banjak | |
| Name: Marc A. Banjak | ||
| Title: Chief Legal Counsel | ||
Exhibit 99.1
|
Breakthrough Antibodies for Obesity and Cardiometabolic Diseases Corporate Presentation August 2025 |
|
Certain statements in this presentation constitute "forward -looking statements" within the meaning of the Private Securities Litigation Reform Act of 1995, as amended. Words such as "may," "might," "will," "should," "believe," "expect," "anticipate," "estimate," "continue," "predict," "forecast," "project," "plan," "intend" or similar expressions, or statements regarding intent, belief, or current expectations, are forward -looking statements. These forward - looking statements are based upon current estimates and includes statements regarding near term catalysts. While iBio, Inc., a Delaware corporation (including its consolidated subsidiaries, “iBio,” the “Company,” “we,” “us” or “our”) believes these forward -looking statements are reasonable, undue reliance should not be placed on any such forward - looking statements, which are based on information available to us on the date of this presentation. These forward -looking statements are subject to various risks and uncertainties, many of which are difficult to predict that could cause actual results to differ materially from current expectations and assumptions from those set forth or implied by any forward -looking statements. Important factors that could cause actual results to differ materially from current expectations include, among others, the Company’s ability to obtain regulatory approvals for commercialization of its product candidates, or to comply with ongoing regulatory requirements, regulatory limitations relating to its ability to promote or commercialize its product candidates for specific indications, acceptance of its product candidates in the marketplace and the successful development, marketing or sale of products, its ability to attain license agreements, the continued maintenance and growth of its patent estate, its ability to establish and maintain collaborations, its ability to obtain or maintain the capital or grants necessary to fund its research and development activities, competition, its ability to retain its key employees or maintain its Nasdaq Stock Market listing, and the other factors discussed in the Company’s most recent Annual Report on Form 10-K and the Company’s subsequent filings with the SEC, including subsequent periodic reports on Forms 10-Q and 8-K. The information in this presentation is provided only as of today, and we undertake no obligation to update any forward -looking statements contained in this presentation on account of new information, future events, or otherwise, except as required by law. Forward looking statements 2 |
|
Revolution Sparked a New Era in Obesity Treatment Evolution Will Define Its Future Incretin Class Agonists Have Revolutionized Obesity Treatment >10% of American adults have taken a GLP-11 Interventional weight loss previously only achievable via surgery Attention is Shifting to Therapies That Build on That Foundation Durability of weight loss Lean mass preservation and fat-specific weight loss Improved tolerability and convenience 1. KFF Health Tracking Poll May 2024: The Public’s Use and Views of GLP-1 Drugs, KFF, May 10, 2025 3 |
|
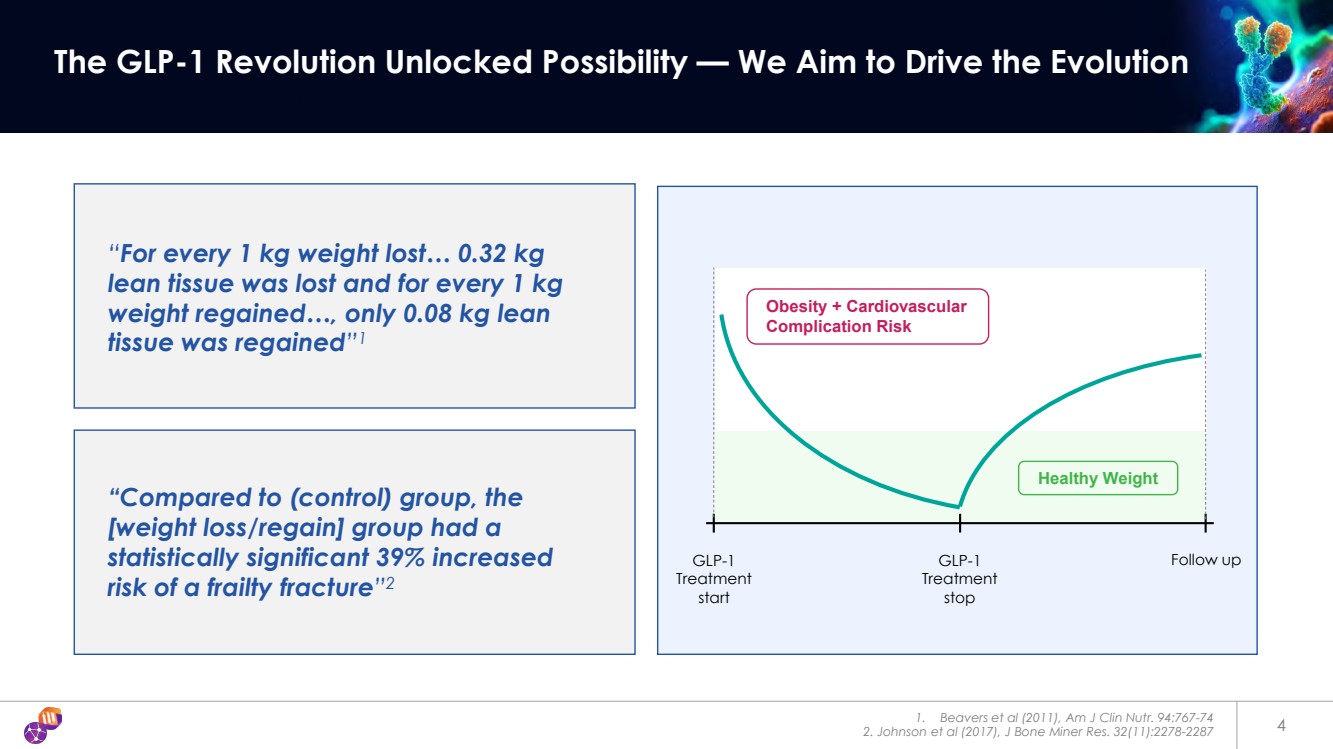
“For every 1 kg weight lost… 0.32 kg lean tissue was lost and for every 1 kg weight regained…, only 0.08 kg lean tissue was regained”1 1. Beavers et al (2011), Am J Clin Nutr. 94:767-74 2. Johnson et al (2017), J Bone Miner Res. 32(11):2278-2287 4 The GLP-1 Revolution Unlocked Possibility — We Aim to Drive the Evolution GLP-1 Treatment start GLP-1 Treatment stop Follow up Obesity + Cardiovascular Complication Risk “Compared to (control) group, the [weight loss/regain] group had a statistically significant 39% increased risk of a frailty fracture”2 Healthy Weight |
|
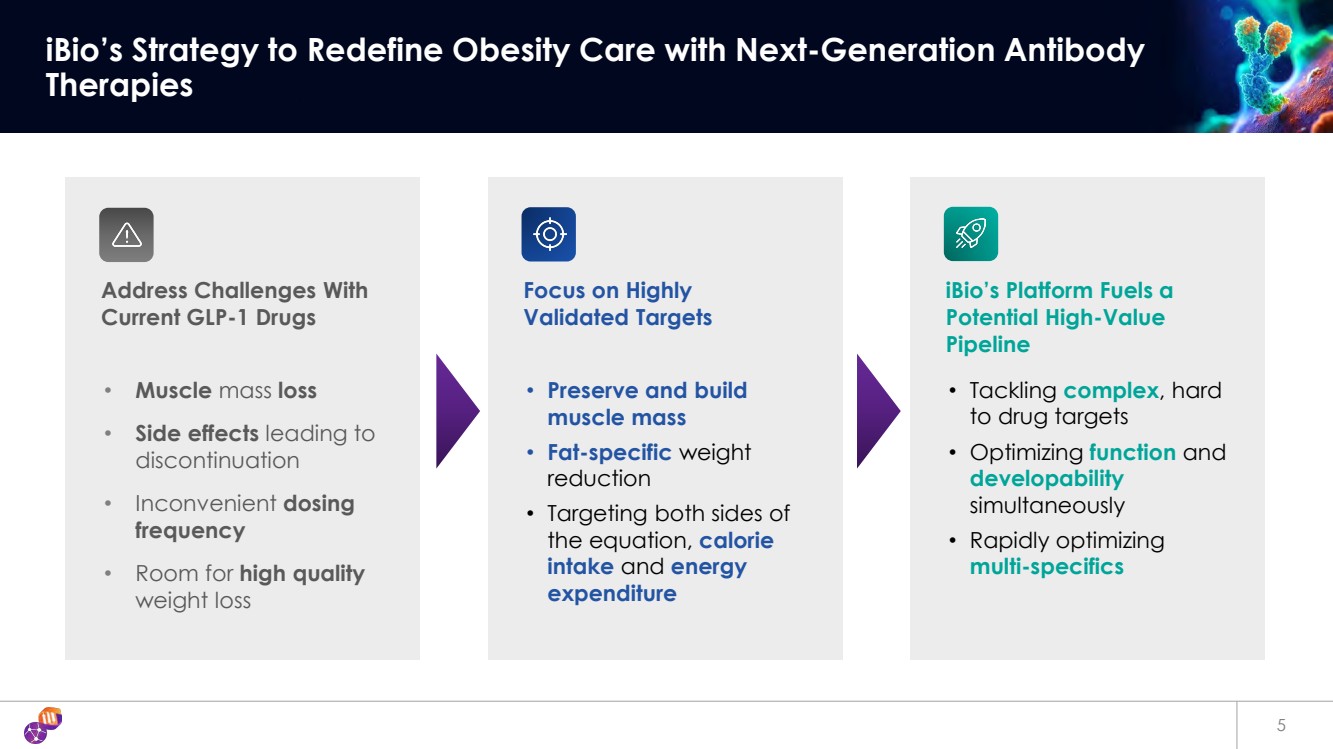
5 iBio’s Strategy to Redefine Obesity Care with Next-Generation Antibody Therapies Address Challenges With Current GLP-1 Drugs • Muscle mass loss • Side effects leading to discontinuation • Inconvenient dosing frequency • Room for high quality weight loss Focus on Highly Validated Targets • Preserve and build muscle mass • Fat-specific weight reduction • Targeting both sides of the equation, calorie intake and energy expenditure iBio’s Platform Fuels a Potential High-Value Pipeline • Tackling complex, hard to drug targets • Optimizing function and developability simultaneously • Rapidly optimizing multi-specifics |
|
Next Generation Antibodies for Obesity Targeting Key Gaps in Current Care Corporate Highlights Lead Programs IBIO-610: Activin E antibody Myostatin x Activin A: Bispecific Antibody Pipeline 3 early-stage high novelty programs and 2 partnered programs Discovery to development candidate in as little as 7 months AI engine delivers precisely targeted antibodies with promising developability IBIO-600: Long-acting myostatin antibody Anticipated Near Term Catalysts* 6 Myostatin x Activin A IND equivalent filing expected in 1H 2027 IBIO-610 IND equivalent filing expected in 2026 IBIO-610 Phase 1 expected to be initiated in 1H 2027 * Financing Dependent |
|
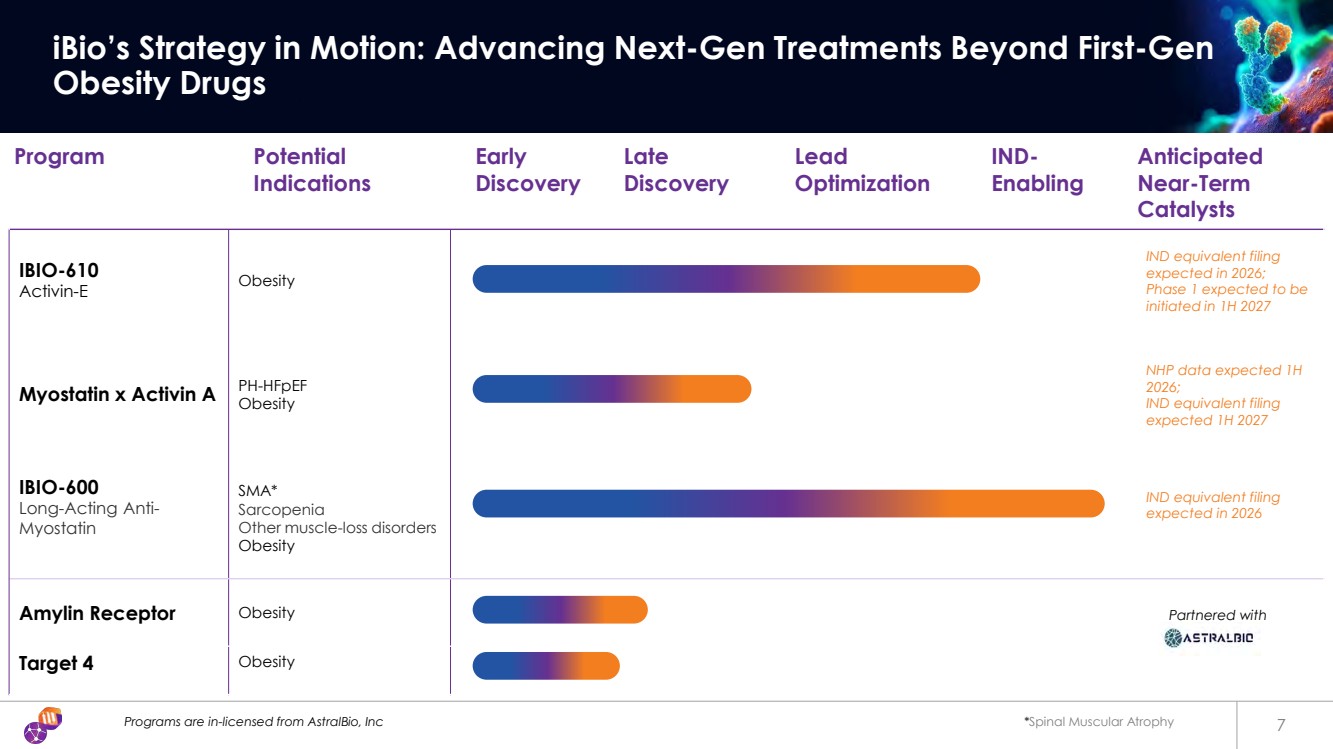
Programs are in-licensed from AstralBio, Inc *Spinal Muscular Atrophy 7 iBio’s Strategy in Motion: Advancing Next-Gen Treatments Beyond First-Gen Obesity Drugs Program Potential Indications Early Discovery Late Discovery Lead Optimization IND-Enabling Anticipated Near-Term Catalysts IBIO-610 Activin-E Obesity IND equivalent filing expected in 2026; Phase 1 expected to be initiated in 1H 2027 Myostatin x Activin A PH-HFpEF Obesity NHP data expected 1H 2026; IND equivalent filing expected 1H 2027 IBIO-600 Long-Acting Anti-Myostatin SMA* Sarcopenia Other muscle-loss disorders Obesity IND equivalent filing expected in 2026 Amylin Receptor Obesity Target 4 Obesity Partnered with |
|
IBIO-610 Anti-Activin E Antibody |
|
1. Akbari, P. et al. Multiancestry exome sequencing reveals INHBE mutations associated with favorable fat distribution and protection from diabetes. Nat Commun 13, 4844 (2022). 2. Deaton, A. M. et al. Rare loss of function variants in the hepatokine gene INHBE protect from abdominal obesity. Nat Commun 13, 4319 (2022). Type 2 Diabetes (T2D) 9 IBIO-610 Targets Activin E to Potentially Drive Targeted Fat Loss and Maintain Weight Reduction After GLP-1 Discontinuation Why We Target Activin E Activin E is a Hepatokine, produced in the liver and a member of the TGFβ family Activin E and its receptor are highly genetically validated1,2 Genetic loss of function decreases adiposity and risk for Diabetes / Cardiovascular Disease (CVD)1,2 2 RNA targeting molecules provide preclinical pharmacological validation Challenge to produce active recombinant Activin E until recently has proven to be extremely difficult for antibody discovery |
|
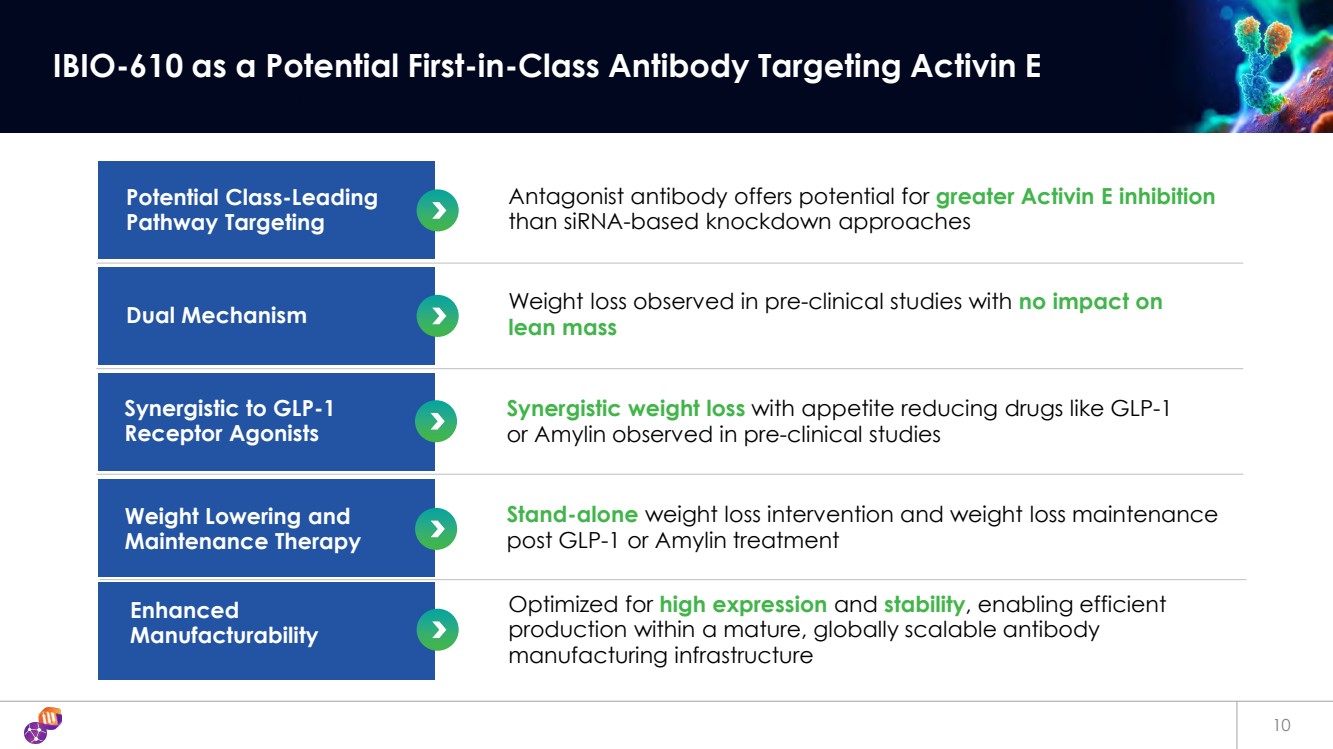
10 IBIO-610 as a Potential First-in-Class Antibody Targeting Activin E Antagonist antibody offers potential for greater Activin E inhibition than siRNA-based knockdown approaches Potential Class-Leading Pathway Targeting Weight loss observed in pre-clinical studies with no impact on lean mass Dual Mechanism Synergistic weight loss with appetite reducing drugs like GLP-1 or Amylin observed in pre-clinical studies Synergistic to GLP-1 Receptor Agonists Stand-alone weight loss intervention and weight loss maintenance post GLP-1 or Amylin treatment Weight Lowering and Maintenance Therapy Optimized for high expression and stability, enabling efficient production within a mature, globally scalable antibody manufacturing infrastructure Enhanced Manufacturability |
|
Target Protein Binding Assay Reporter Cell Line Functional Assay Primary Human Adipocyte Assay Data on file 11 IBIO-610 Exhibited High-Affinity Binding and Potent Inhibition of Activin E Signaling in Engineered and Primary Human Fat Cells 0.001 0.01 0.1 1 10 100 0 2000 4000 6000 mAb (nM) RLU Isotype Cnt IBIO-610 No treatment IC50 = 158 pM 1 10 100 1000 0 10 20 30 40 IBIO-610 (nM) % pSmad2+ cells No treatment Activin E only Activin E + IBIO-610 IC50 = 44 nM |
|
*Non-responder outlier mice removed, IBIO-610 mouse surrogate used. 10 mg/kg, BIW dosing. DIO mice Data on file 12 IBIO-610 Observed to Induce Fat-Selective Weight Loss in Diet-Induced Obese Mice 0 7 14 21 28 -15 -10 -5 0 5 Day Body Weight % Change Baseline and Vehicle Corrected PBS IBIO-610 -8.9% *** *** *** *** **** p<0.0001 p<0.005 *** **** Baseline Week 4 0 5 10 15 20 Fat Mass (g) * p<0.05 * +0.4% -26% PBS IBIO-610 Weight Loss = 8.9% Fat Loss = 26% No Lean Mass Loss Baseline Week 4 0 5 10 15 20 25 Lean Mass (g) * p<0.05 +3.0% +3.5% PBS IBIO-610 Study Design Week -16 High-fat diet induction Week -7 DEXA Day 1 DEXA Day 14 DEXA Day 28 Randomization and baseline 4 weeks treatment | Antibodies 2x week |
|
Data on file IBIO-610 mouse surrogate used, 10 mg/kg, BIW dosing. Semaglutide dosed QD at 10 nmol/kg. 13 IBIO-610 Synergizes with GLP-1 Through a Distinct, Non-Appetite-Based Mechanism Synergistic Weight Loss No Additional Appetite Suppression Visceral Fat Reduction Study Design Week -16 High-fat diet induction Week -7 DEXA Day 1 DEXA Day 14 DEXA Day 28 Randomization and baseline 4 weeks treatment | Semaglutide daily | Antibodies 2x week 0 7 14 21 28 -50 -40 -30 -20 -10 0 Day Body Weight % Change Baseline and Vehicle Corrected PBS Sema IBIO-610+Sema -27.8% -35.3% p<0.0001 vs. PBS p<0.005 vs. PBS p<0.01 vs. Sema **** *** ** **** ** **** ** **** **** ** **** ** **** ** ** **** ** **** **** **** **** **** **** **** PBS Sema IBIO-610+Sema 0 1 2 3 Food Intake (g) Average, per mouse, weeks 1-4 PBS Sema IBIO-610+Sema 0 500 1000 1500 2000 Visceral Fat (mg) Epididymal -58% -69% |
|
Data on file 14 IBIO-610 Observed to Prevent Weight Regain Following GLP-1 Treatment in Obese Mice Significant Prevention of Weight Regain Fat-Specific Effect Study Design 0 5 10 15 20 25 30 35 75 80 85 90 95 100 105 Day of Treatment Body Weight (%) Baseline and Vehicle Corrected PBS Sema=>PBS Sema=>IBIO-610 IBIO-610 Initiation ns *** ** * p<0.05 compared to Sema=>PBS p<0.005 compared to PBS PBS Sema => PBS Sema => IBIO-610 0 2 4 6 8 Combined Fat mWAT+iWAT+eWAT mass (g) ✱✱✱ ✱✱✱ PBS Sema => PBS Sema => IBIO-610 0.00 0.05 0.10 0.15 0.20 0.25 Quadriceps (Muscle) mass (g) PBS Sema => PBS Sema => IBIO-610 0 1 2 3 4 Liver mass (g) Vehicle Semaglutide Semaglutide 30 DIO mice PBS only Sema => PBS Sema => IBIO-610 Day 1 Sema cessation Day 14 IBIO-610 Start day 11 Day 14 Vehicle Vehicle IBIO-610 Day 15 Day 35 Necropsy (adipose, muscle, liver assessment) |
|
The Next Wave of iBio Innovation Early Pre-Clinical Programs |
|
16 Combined Myostatin and Activin A Antagonism Synergistic Effect on Muscle Growth and Potential Treatment for Pulmonary Hypertension (PH) in Heart Failure With Preserved Ejection Fraction (HFpEF) We are developing bispecific co-inhibitors of Myostatin and Activin A designed to enhance muscle growth and improve quality of weight loss during and after treatment with incretin drugs Why Myostatin & Activin A Myostatin and Activin A are key negative regulators of muscle mass Both are members of the TGFβ superfamily Activin A mechanism is pharmacologically validated1, 2 Combined Activin A and Myostatin inhibition, causes more pronounced muscle growth3 Myostatin and Activin A inhibition are believed to be key features for treating PH-HFpEF4 1.Villanueva, J. et al. Am J Cardiovasc Drugs (2024) 2.US20220119514A1, Regeneron corporate slides 3.Latres, E. et al. Nat Commun 8, 15153 (2017) 4. 1. Lan, Z., Lv, Z., Zuo, W. & Xiao, Y. From bench to bedside: The promise of sotatercept in hematologic disorders. Biomedicine & Pharmacotherapy 165, 115239 (2023) Binding of Myostatin and Activin A to cells leads to muscle atrophy Simultaneous blocking of Myostatin and Activin A leads to muscle growth |
|
Data on file 17 iBio’s Myostatin and Activin A Bi-Specific Targets Both Key Negative Muscle Regulators, Synergistically Increasing Muscle Mass Increased muscle fusion index in human muscle stem cells is a surrogate of muscle growth Negative control (Myostatin + Activin A) without antibody Myostatin + Activin A with Activin A Antibody Myostatin + Activin A with Myostatin Antibody Myostatin + Activin A with Myostatin x Activin A Bi-Specific Only a Myostatin x Activin A bi-specific antibody fully blocks both muscle growth suppressors, enabling optimal growth, while single-target antibodies fall short In Vitro Data |
|
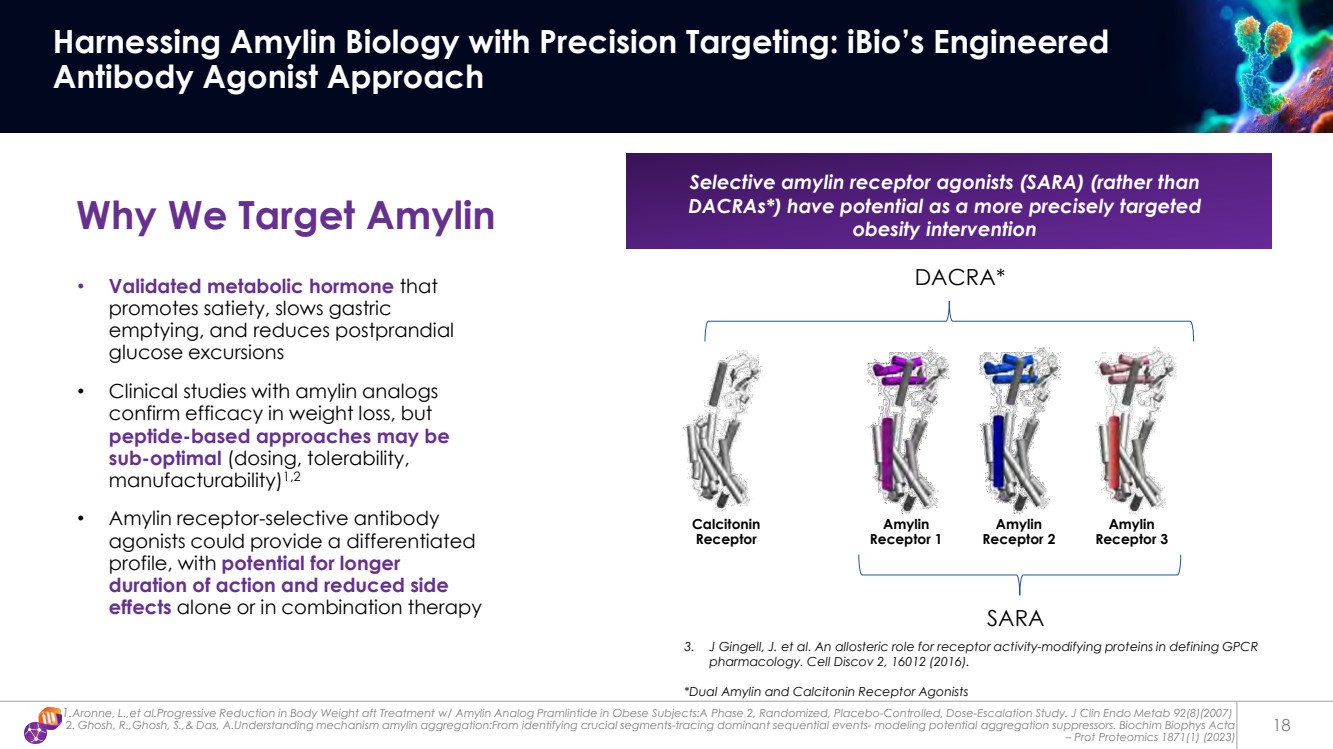
1.Aronne, L.,et al.Progressive Reduction in Body Weight aft Treatment w/ Amylin Analog Pramlintide in Obese Subjects:A Phase 2, Randomized, Placebo-Controlled, Dose-Escalation Study. J Clin Endo Metab 92(8)(2007) 2. Ghosh, R.,Ghosh, S.,& Das, A.Understanding mechanism amylin aggregation:From identifying crucial segments-tracing dominant sequential events- modeling potential aggregation suppressors. Biochim Biophys Acta – Prot Proteomics 1871(1) (2023) 18 Harnessing Amylin Biology with Precision Targeting: iBio’s Engineered Antibody Agonist Approach Why We Target Amylin Selective amylin receptor agonists (SARA) (rather than DACRAs*) have potential as a more precisely targeted obesity intervention • Validated metabolic hormone that promotes satiety, slows gastric emptying, and reduces postprandial glucose excursions • Clinical studies with amylin analogs confirm efficacy in weight loss, but peptide-based approaches may be sub-optimal (dosing, tolerability, manufacturability)1,2 • Amylin receptor-selective antibody agonists could provide a differentiated profile, with potential for longer duration of action and reduced side effects alone or in combination therapy DACRA* 3. J Gingell, J. et al. An allosteric role for receptor activity-modifying proteins in defining GPCR pharmacology. Cell Discov 2, 16012 (2016). *Dual Amylin and Calcitonin Receptor Agonists Calcitonin Receptor Amylin Receptor 1 Amylin Receptor 2 Amylin Receptor 3 SARA |
|
IBIO-600 Long-Acting Anti-Myostatin Antibody |
|
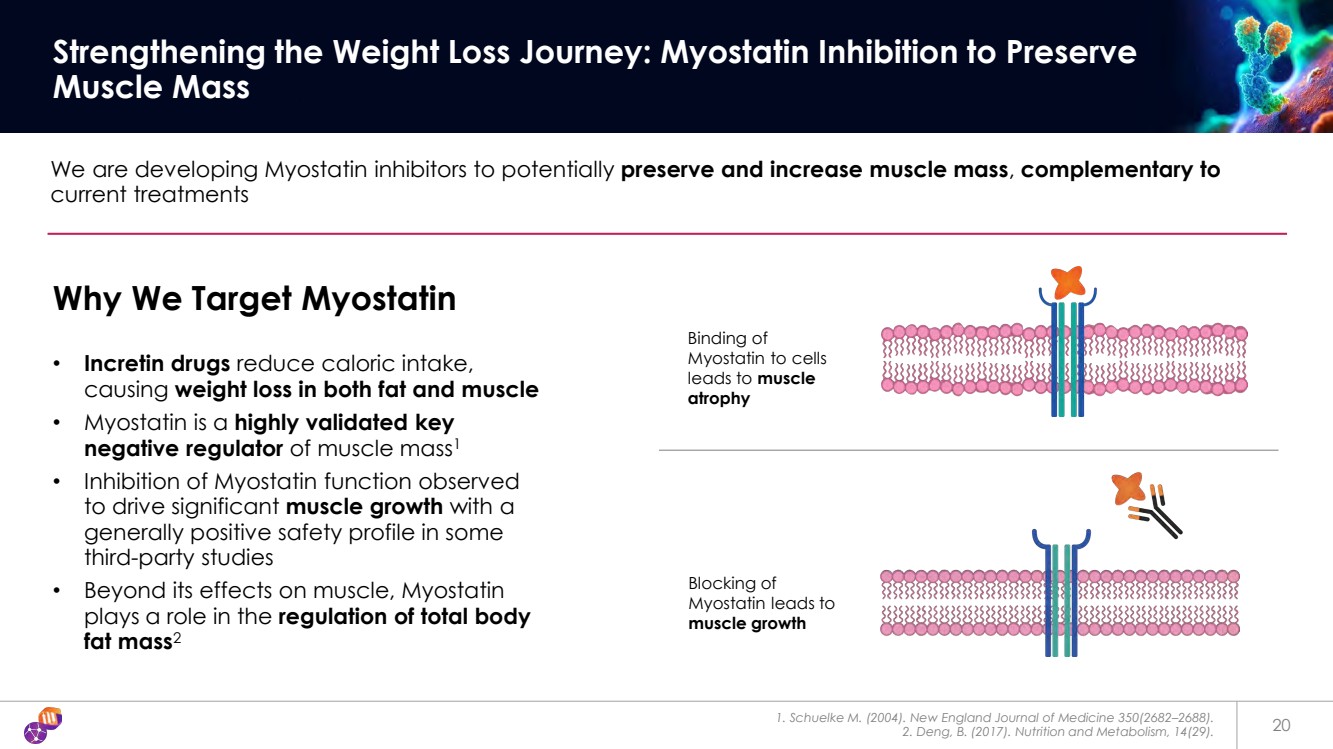
1. Schuelke M. (2004). New England Journal of Medicine 350(2682–2688). 2. Deng, B. (2017). Nutrition and Metabolism, 14(29). 20 Strengthening the Weight Loss Journey: Myostatin Inhibition to Preserve Muscle Mass We are developing Myostatin inhibitors to potentially preserve and increase muscle mass, complementary to current treatments Why We Target Myostatin • Incretin drugs reduce caloric intake, causing weight loss in both fat and muscle • Myostatin is a highly validated key negative regulator of muscle mass1 • Inhibition of Myostatin function observed to drive significant muscle growth with a generally positive safety profile in some third-party studies • Beyond its effects on muscle, Myostatin plays a role in the regulation of total body fat mass2 Binding of Myostatin to cells leads to muscle atrophy Blocking of Myostatin leads to muscle growth |
|
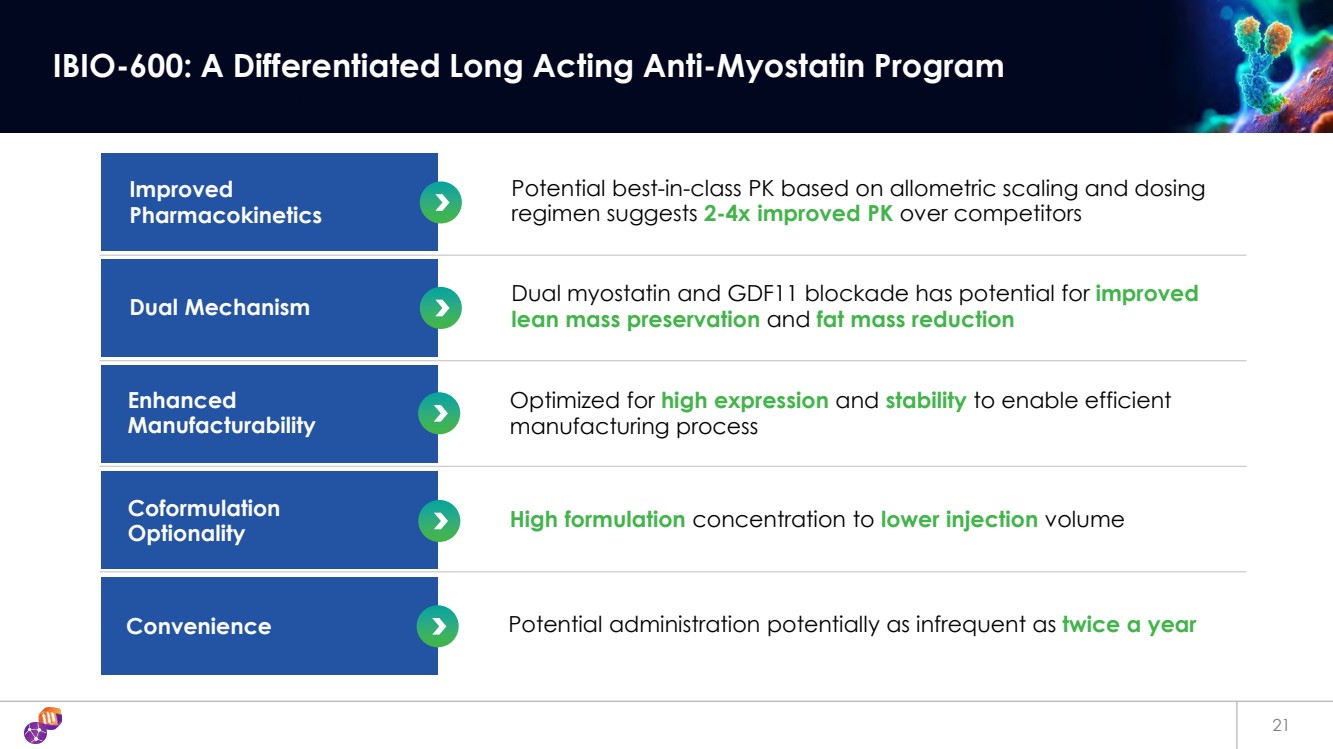
21 IBIO-600: A Differentiated Long Acting Anti-Myostatin Program Potential best-in-class PK based on allometric scaling and dosing regimen suggests 2-4x improved PK over competitors Improved Pharmacokinetics Dual myostatin and GDF11 blockade has potential for improved lean mass preservation and fat mass reduction Dual Mechanism Optimized for high expression and stability to enable efficient manufacturing process Enhanced Manufacturability High formulation concentration to lower injection volume Coformulation Optionality Convenience Potential administration potentially as infrequent as twice a year |
|
1. Francis, T., Soendenbroe, C., Lazarus, N. R., Mackey, A. L. & Harridge, S. D. R. Insights into human muscle biology from human primary skeletal muscle cell culture. J Muscle Res Cell Motil (2025) doi:10.1007/s10974-025-09696-w. - Data on file 22 IBIO-600 Enhances Muscle Differentiation in Human Myoblasts by Targeting the Two Growth Suppressors Myostatin and GDF11 IBIO-600 Increases Myoblast Differentiation Baseline human myoblast differentiation (untreated) Myostatin inhibits human myoblast differentiation IBIO-600 blocks Myostatin and increases human myoblast differentiation The human Myoblast differentiation model is highly predictive of muscle growth in humans1 0.1 1 10 100 1000 IBIO-600 (nM) Fusion index Myostatin only IBIO-600 0.1 1 10 100 1000 IBIO-600 (nM) Fusion index GDF11 only IBIO-600 Myostatin GDF11 |
|
1. Linear elimination phase used to estimate half-life with simple linear model Data on file 23 IBIO-600 Fc Engineering Drives Extended Half-Life in Obese NHPs Dose t1/2 (days) 5 mg/kg, I.V. 52.4 IBIO-600 Fc Engineering Results in Enhanced FcRn Binding Clone Fc Fold increase over standard IgG IBIO-600 FAB Standard IgG4 1.0 IBIO-600 Engineered IgG4 16.5 IBIO-600 Observed to Have Extended Half-Life in NHPs 12 Week Pharmacokinetics Data1 0 20 40 60 80 10 100 1000 Days Serum mAb (ug/mL) IBIO-600 Study Details: • Obese, aged NHPs • Monthly DEXA scan for body composition • Periodic PK sampling Study Design: • N=3 per group • 5mg/kg single I.V. dose t1/2 = 52.4 |
|
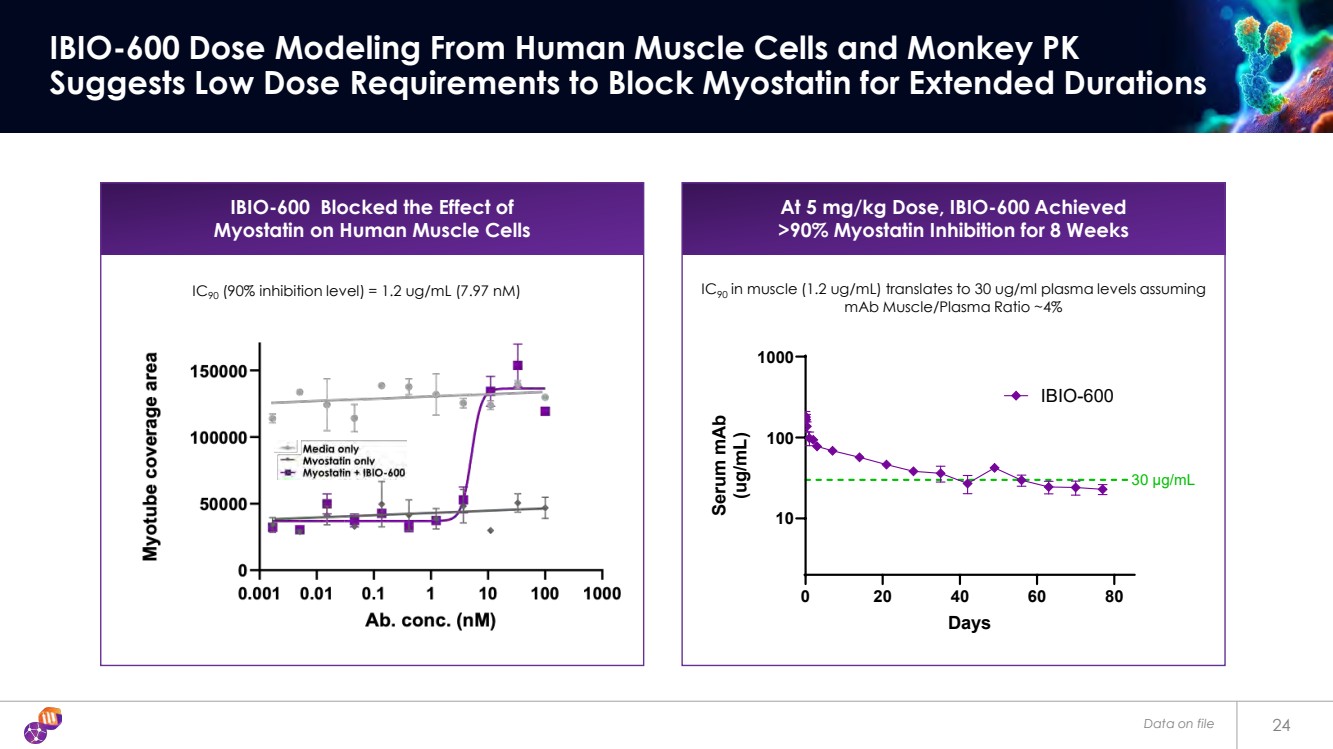
24 IBIO-600 Dose Modeling From Human Muscle Cells and Monkey PK Suggests Low Dose Requirements to Block Myostatin for Extended Durations IBIO-600 Blocked the Effect of Myostatin on Human Muscle Cells IC90 (90% inhibition level) = 1.2 ug/mL (7.97 nM) 0 20 40 60 80 10 100 1000 Days Serum mAb (ug/mL) IBIO-600 30 μg/mL At 5 mg/kg Dose, IBIO-600 Achieved >90% Myostatin Inhibition for 8 Weeks IC90 in muscle (1.2 ug/mL) translates to 30 ug/ml plasma levels assuming mAb Muscle/Plasma Ratio ~4% Data on file |
|
Data on File 25 Allometric Scaling Predicts Potentially Extended Half-Life for IBIO-600, Enabling Infrequent Dosing and Prolonged Myostatin Inhibition Y=2.49x+17 0 10 20 30 0 20 40 60 80 100 Allometric scaling YTE and LS mAb only NHP t1/2 (days) Human t1/2 (days) Dose NHP t1/2 (actual) Human t1/2 (predicted)1,2 5 mg/kg, I.V. 52.4 74-147 days Measured NHP and Expected Human Half-Life of IBIO-600 Allometric Scaling Model for Half-Life Extended Antibodies1 Generic allometric scaling model for antibodies2 T1/2Human= T1/2NHP x Human Body Weight NHP Body Weight 0.15 1. Haraya, K. & Tachibana, T. Translational Approach for Predicting Human Pharmacokinetics of Engineered Therapeutic Monoclonal Antibodies with Increased FcRn-Binding Mutations. BioDrugs 37, 99–108 (2023). 2. Nakamura, G. et al. Predicting Method for the Human Plasma Concentration–Time Profile of a Monoclonal Antibody from the Half-life of Non-human Primates. Biological and Pharmaceutical Bulletin 43, 823–830 (2020). |
|
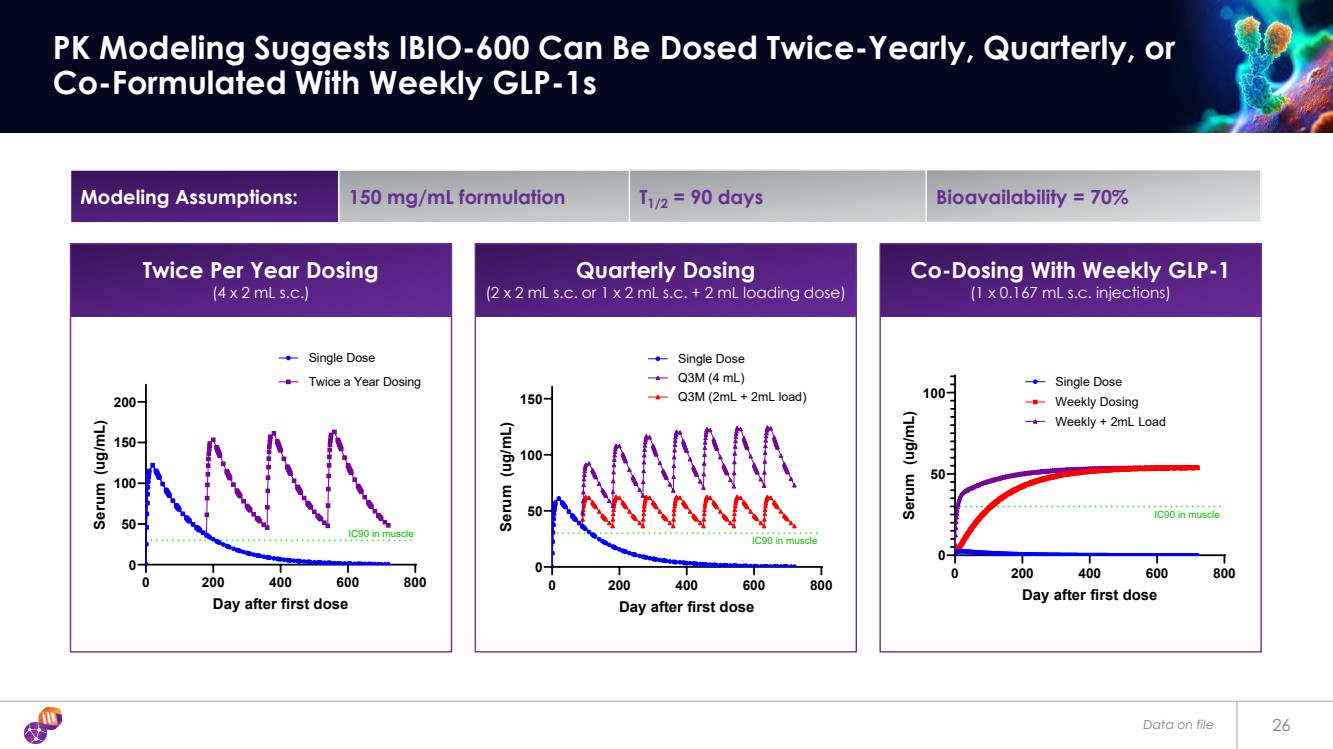
Data on file 26 PK Modeling Suggests IBIO-600 Can Be Dosed Twice-Yearly, Quarterly, or Co-Formulated With Weekly GLP-1s Twice Per Year Dosing (4 x 2 mL s.c.) 0 200 400 600 800 0 50 100 150 200 Day after first dose Serum (ug/mL) Single Dose Twice a Year Dosing IC90 in muscle 0 200 400 600 800 0 50 100 Day after first dose Serum (ug/mL) Single Dose Weekly Dosing IC90 in muscle Weekly + 2mL Load Modeling Assumptions: 150 mg/mL formulation T1/2 = 90 days Bioavailability = 70% Quarterly Dosing (2 x 2 mL s.c. or 1 x 2 mL s.c. + 2 mL loading dose) 0 200 400 600 800 0 50 100 150 Day after first dose Serum (ug/mL) Single Dose Q3M (4 mL) IC90 in muscle Q3M (2mL + 2mL load) Co-Dosing With Weekly GLP-1 (1 x 0.167 mL s.c. injections) |
|
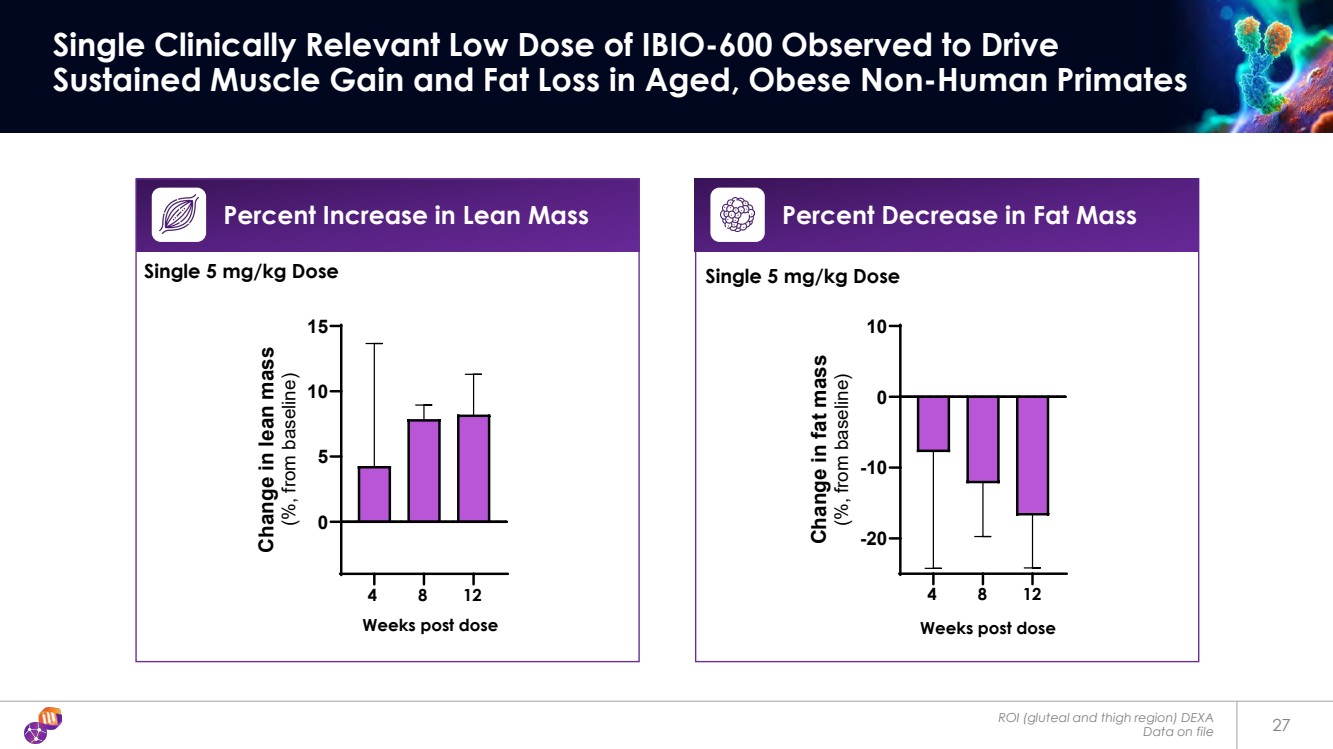
ROI (gluteal and thigh region) DEXA Data on file 27 Single Clinically Relevant Low Dose of IBIO-600 Observed to Drive Sustained Muscle Gain and Fat Loss in Aged, Obese Non-Human Primates Percent Increase in Lean Mass Weeks post dose 0 5 10 15 Change in lean mass (%, from baseline) 4 8 12 -20 -10 0 10 Change in fat mass (%, from baseline) 4 8 12 Weeks post dose Percent Decrease in Fat Mass Single 5 mg/kg Dose Single 5 mg/kg Dose |
|
Technology Stack |
|
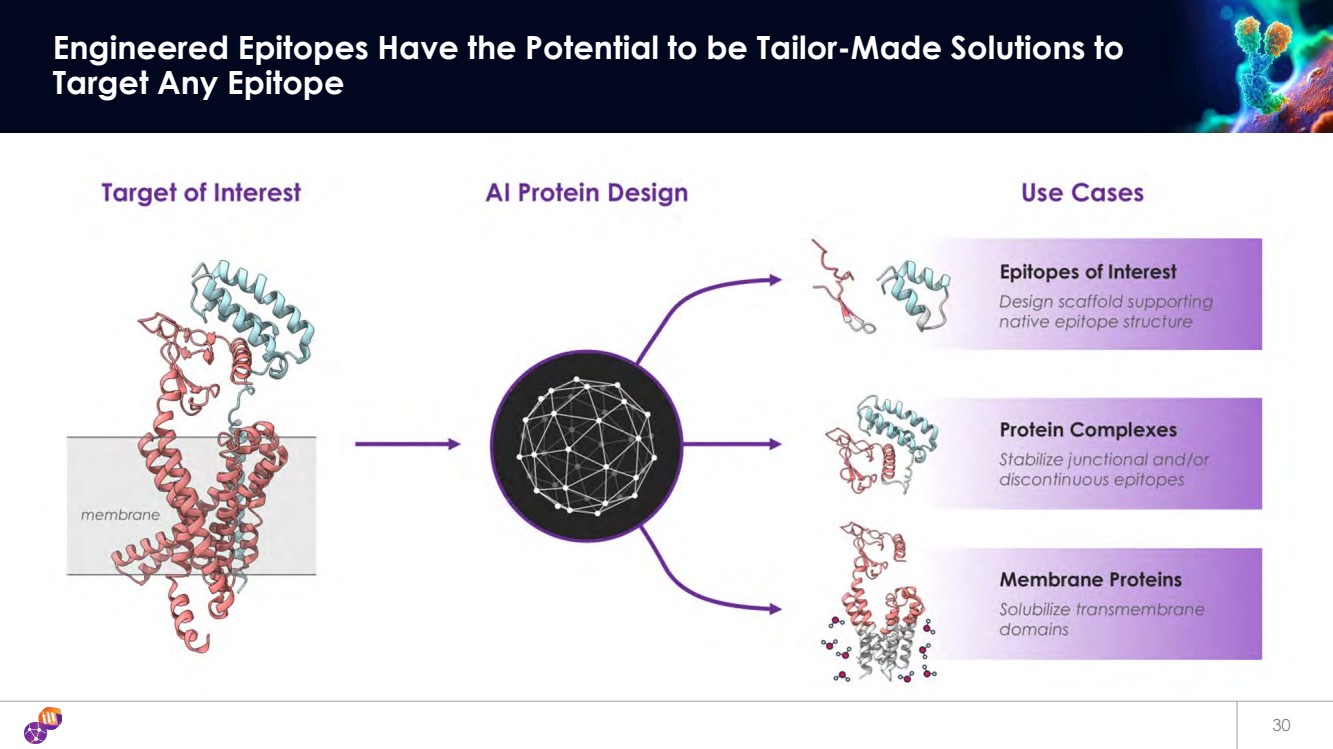
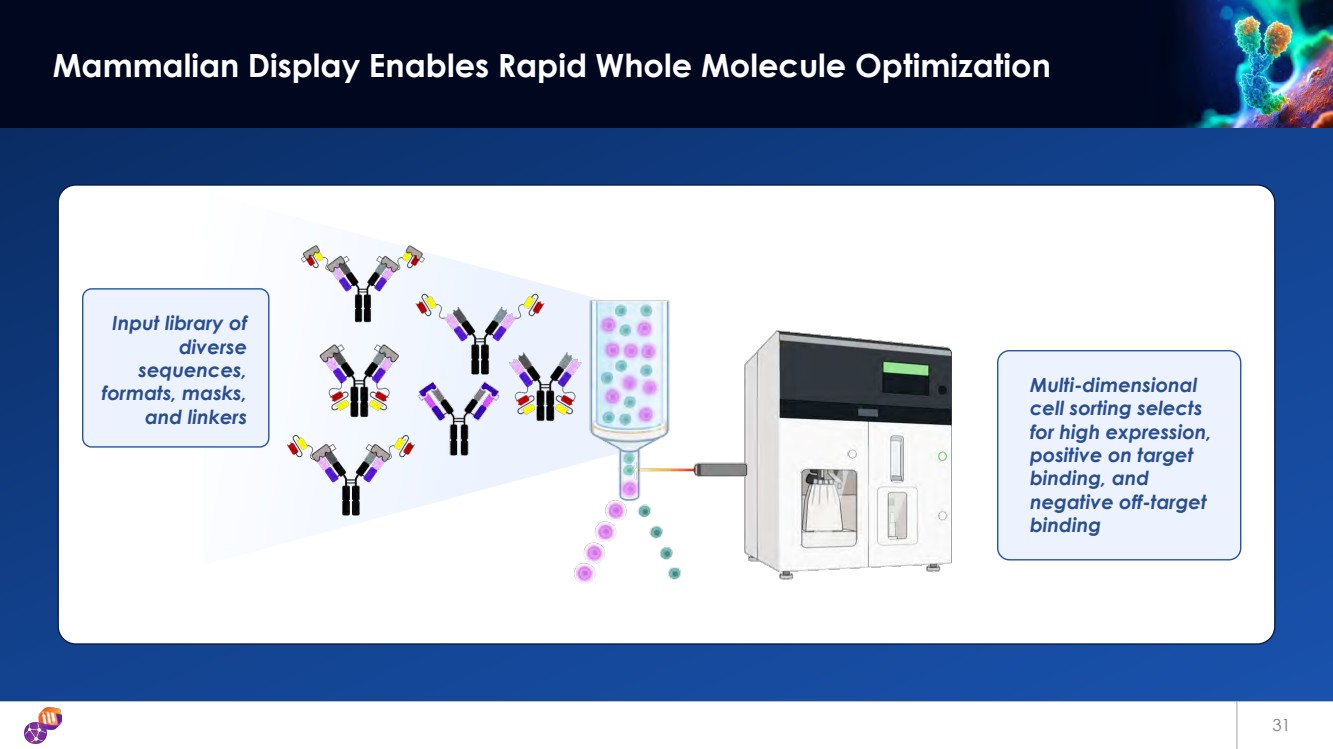
Toward Any Epitope on Any Drug Target AI Epitope Engineering and Antibody Optimization Engines unlock challenging target classes • Multi-layer technology platform addresses multiple challenges in Ab discovery • Patented Epitope Steering technology • Single-step Ab StableHu x Mammalian Display • Masked (ShieldTx®) Antibodies • T-cell engager panel (EngageTx ) iBio’s Discovery Engine iBio’s Proprietary AI Technology Platform We use our Tech Stack to generate new IP against hard-to-drug targets – from idea to Development Candidate in 7 months • Selectively targets functional epitopes • Epitopes with complex modes of action • Unlocks novel target classes • Accelerates discovery of Ab against validated targets AI-guided precision hits that are epitope class agnostic • Gen AI creates mammalian display libraries with phage-like diversity • Single-shot multidimensional lead optimization • Compatible with multi-specific antibody formats • Antibody format agnostic Generative AI meets mammalian display: Ab optimization in 3 weeks 29 |
|
30 Engineered Epitopes Have the Potential to be Tailor-Made Solutions to Target Any Epitope |
|
31 Mammalian Display Enables Rapid Whole Molecule Optimization Input library of diverse sequences, formats, masks, and linkers Multi-dimensional cell sorting selects for high expression, positive on target binding, and negative off-target binding |
|
Corporate Summary |
|
33 A Leadership Team with Deep Industry Experience Deep expertise in cardiometabolic disorders Marc Banjak CLO Martin Brenner, DVM, Ph.D. CEO & CSO Kristi Sarno Senior VP BD Felipe Duran CFO |
|
Executive Summary Corporate Highlights Differentiated Pipeline Aiming to Solve for the Challenges of today’s GLP1’s Focus on increased quality of weight loss (IBIO-610, Myostatin x Activin A) Developability (IBIO-610) Patented AI-Driven Discovery Tech Stack Advance a highly developable pre-clinical pipeline Designed to solve high-value, hard-to-drug targets Financial Highlights $8.8M in cash and restricted cash and cash equivalents as of June 30, 2025 ~19.7M shares outstanding as of August 11, 2025 34 |