UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d)
of the Securities Exchange Act of 1934
Date of Report (Date of earliest event reported): April 7, 2025
RHYTHM PHARMACEUTICALS, INC.
(Exact name of registrant as specified in its charter)
Delaware |
|
001-38223 |
|
46-2159271 |
(State or other jurisdiction |
|
(Commission |
|
(IRS Employer |
222 Berkeley Street
12th Floor
Boston, MA 02116
(Address of principal executive offices) (Zip Code)
Registrant’s telephone number, including area code: (857) 264-4280
N/A
(Former name or former address, if changed since last report)
Check the appropriate box below if the Form 8-K filing is intended to simultaneously satisfy the filing obligation of the registrant under any of the following provisions:
☐ Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425)
☐ Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12)
☐ Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b))
☐ Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c))
Securities registered pursuant to Section 12(b) of the Act:
Title of each class |
Trading |
Name of each exchange on which registered |
Common Stock, $0.001 par value per share |
RYTM |
The Nasdaq Stock Market LLC (Nasdaq Global Market) |
Indicate by check mark whether the registrant is an emerging growth company as defined in Rule 405 of the Securities Act of 1933 (§230.405 of this chapter) or Rule 12b-2 of the Securities Exchange Act of 1934 (§240.12b-2 of this chapter).
Emerging growth company ☐
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Item 7.01. Regulation FD Disclosure.
On April 7, 2025, Rhythm Pharmaceuticals, Inc. (“Rhythm”) issued a press release and published a corporate presentation announcing topline results from its Phase 3 TRANSCEND clinical trial evaluating setmelanotide in patients with acquired hypothalamic obesity, which are summarized under Item 8.01 below. The presentation is available in the “Events & Presentations” portion of the Company's website at ir.rhythmtx.com. A copy of the press release and presentation are furnished as Exhibit 99.1 and Exhibit 99.2, respectively, to this Current Report on Form 8-K.
The information contained in Item 7.01 of this Current Report (including Exhibits 99.1 and 99.2 attached hereto) shall not be deemed “filed” for purposes of Section 18 of the Securities Exchange Act of 1934, as amended (the “Exchange Act”), or otherwise subject to the liabilities of that section, nor shall they be deemed incorporated by reference in any filing under the Securities Act of 1933, as amended, or the Exchange Act, whether made before or after the date hereof, except as expressly provided by specific reference in such a filing.
Item 8.01. Other Events
On April 7, 2025, Rhythm announced topline results from its Phase 3 TRANSCEND clinical trial evaluating setmelanotide in patients with acquired hypothalamic obesity, which are summarized below.
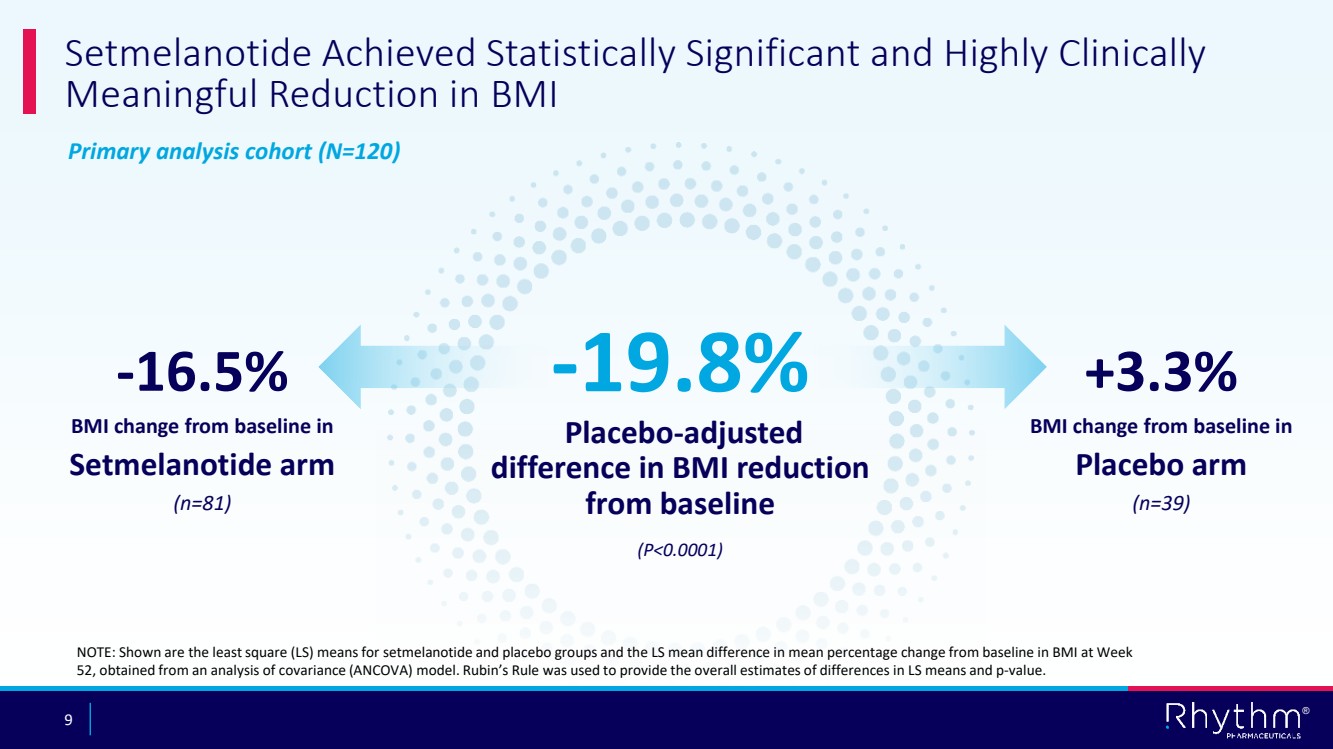
The global trial met its primary endpoint with a highly statistically significant and clinically meaningful reduction in body mass index (BMI) with setmelanotide in both adult and pediatric patients versus placebo.
Highlights from the top-line data include:
• |
-19.8% placebo-adjusted difference in BMI reduction (N=120), and primary endpoint of mean BMI reduction of -16.5% from baseline for all patients on setmelanotide therapy (n=81) compared with +3.3% BMI change for patients on placebo (n=39) at 52 weeks (p<0.0001); |
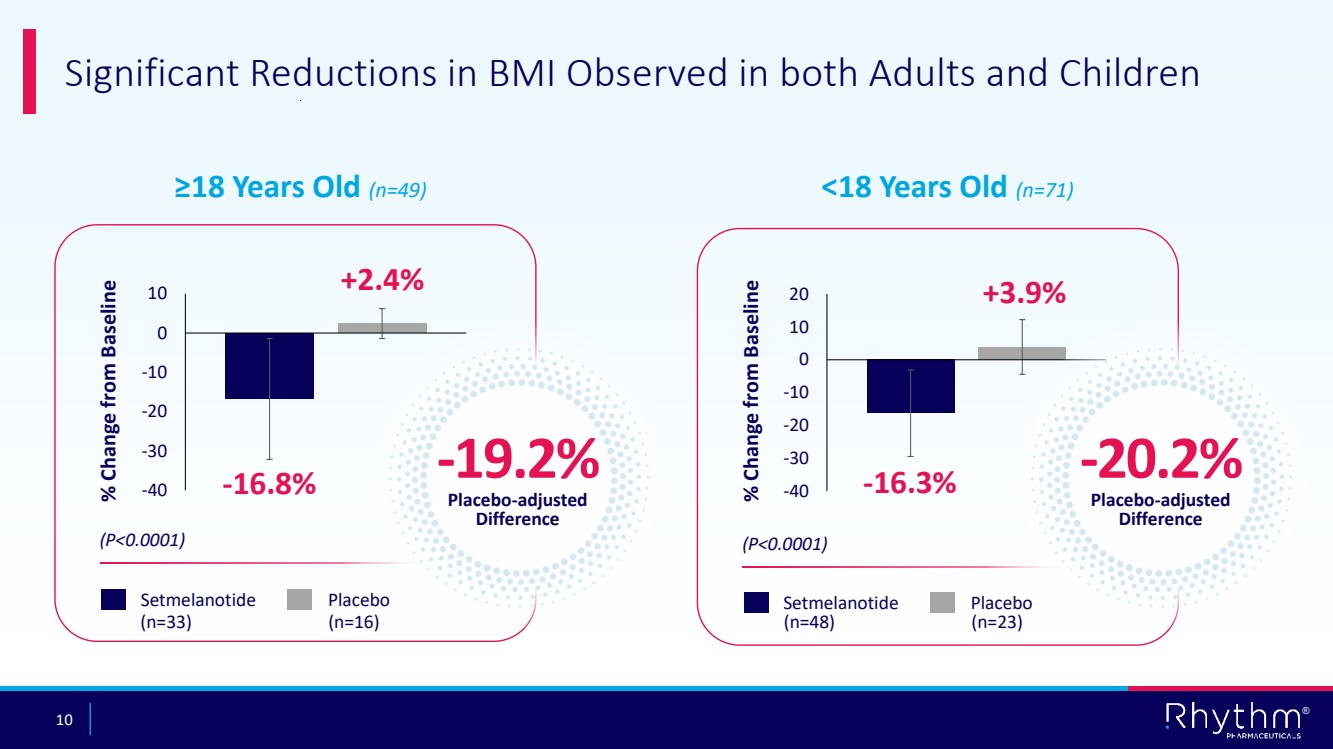
| - | For patients 18 years and older, -19.2% placebo-adjusted difference in BMI reduction (n=49), and primary endpoint of mean BMI reduction of -16.8% from baseline for all patients on setmelanotide therapy (n=33) compared with +2.4% BMI change for patients on placebo (n=16) at 52 weeks (p<0.0001) |
| - | For patients younger than 18 years, -20.2% placebo-adjusted difference in BMI reduction (n=71), and primary endpoint of mean BMI reduction of -16.3% from baseline for all patients on setmelanotide therapy (n=48) compared with +3.9% BMI change for patients on placebo (n=23) at 52 weeks (p<0.0001). |
• |
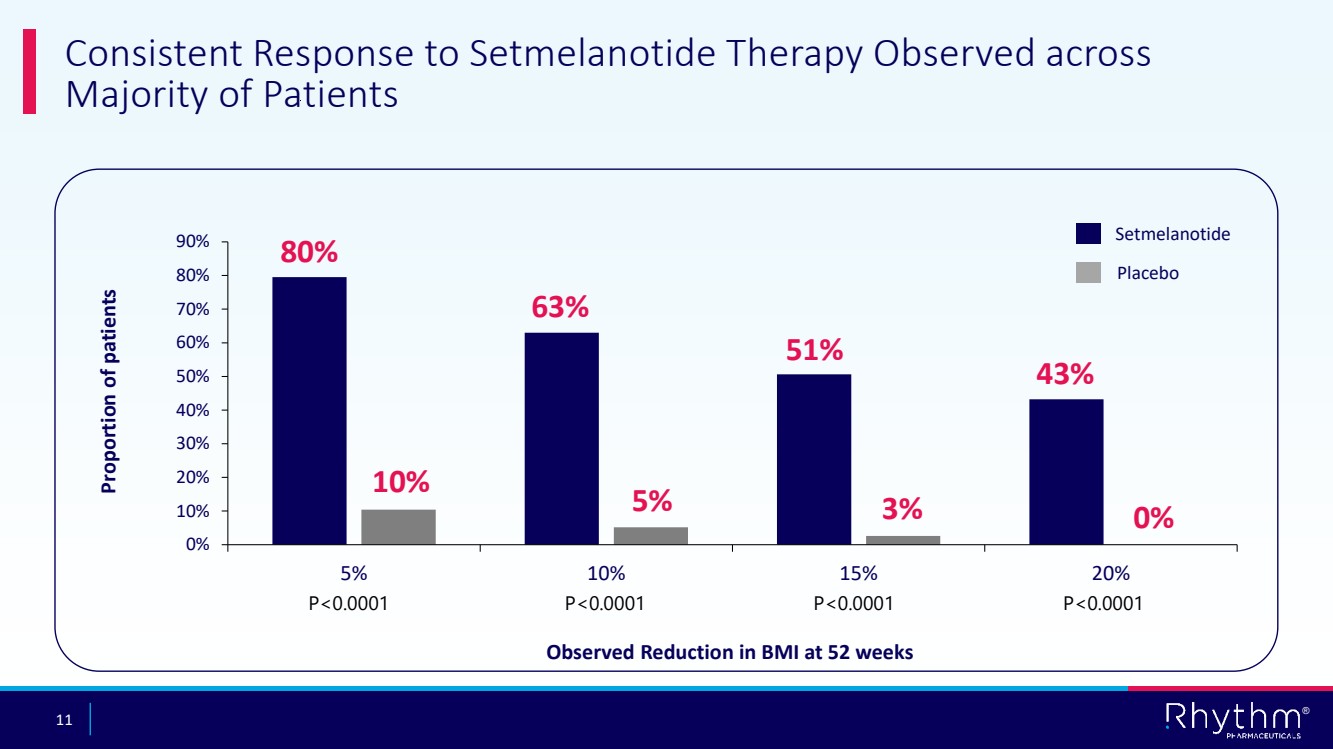
80% of patients on setmelanotide achieved BMI reduction of 5% or greater at 52 weeks |
| - | 63% of patients on setmelanotide achieved BMI reduction of 10% or greater at 52 weeks; |
| - | 51% of patients on setmelanotide achieved BMI reduction of 15% or greater reduction at 52 weeks; and |
| - | 43% of patients on setmelanotide achieved BMI reduction of 20% or greater at 52 weeks. |
The double-blinded, 52-week trial primary analysis cohort consisted of 120 patients, randomized 2:1. In addition to the primary endpoint and other data points above, clinically meaningful improvements were observed across key secondary endpoints at week 52, including:
•83% percent of patients on setmelanotide therapy achieved 5% or greater reduction in BMI (n=33 patients 18 or older) or BMI Z score reduction of 0.2 or greater points (n=48 patients younger than 18); and
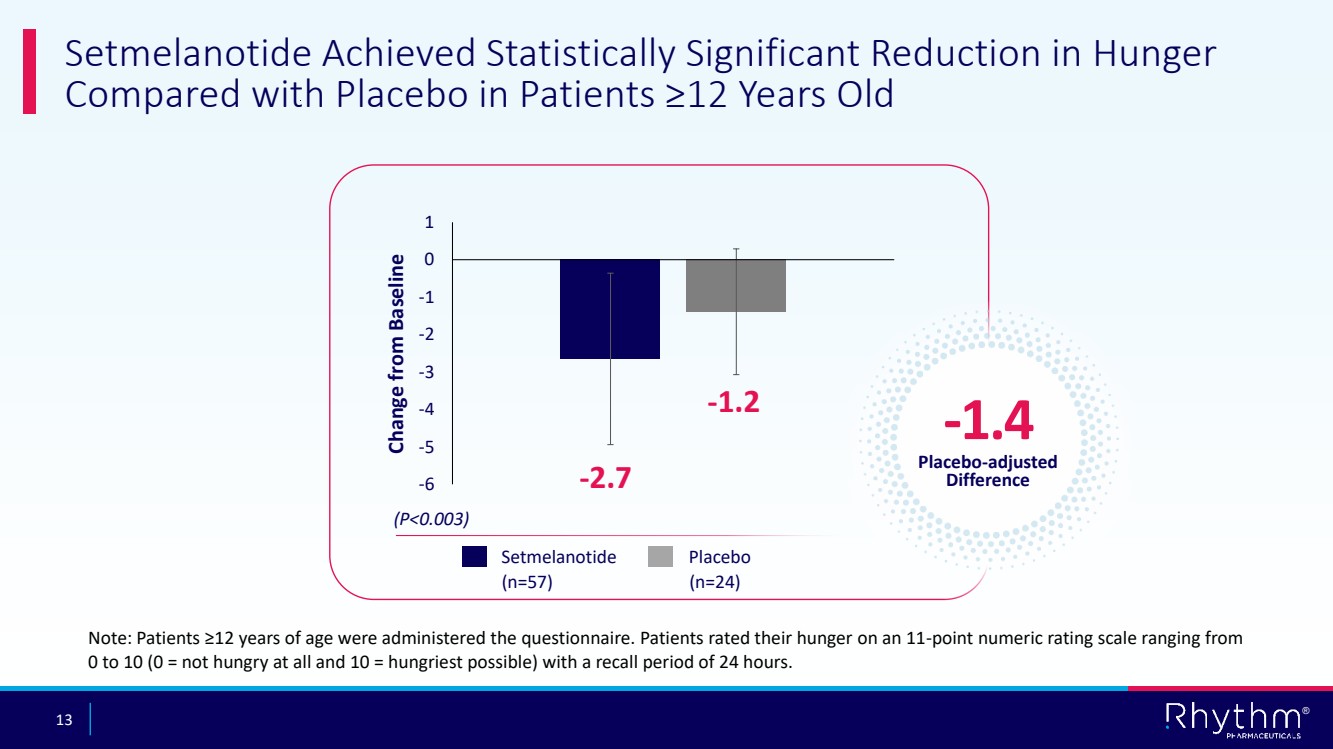
•-1.4 placebo-adjusted mean change in weekly average of the daily maximal hunger score for patients 12 years old or older (n=81) (p=0.003).
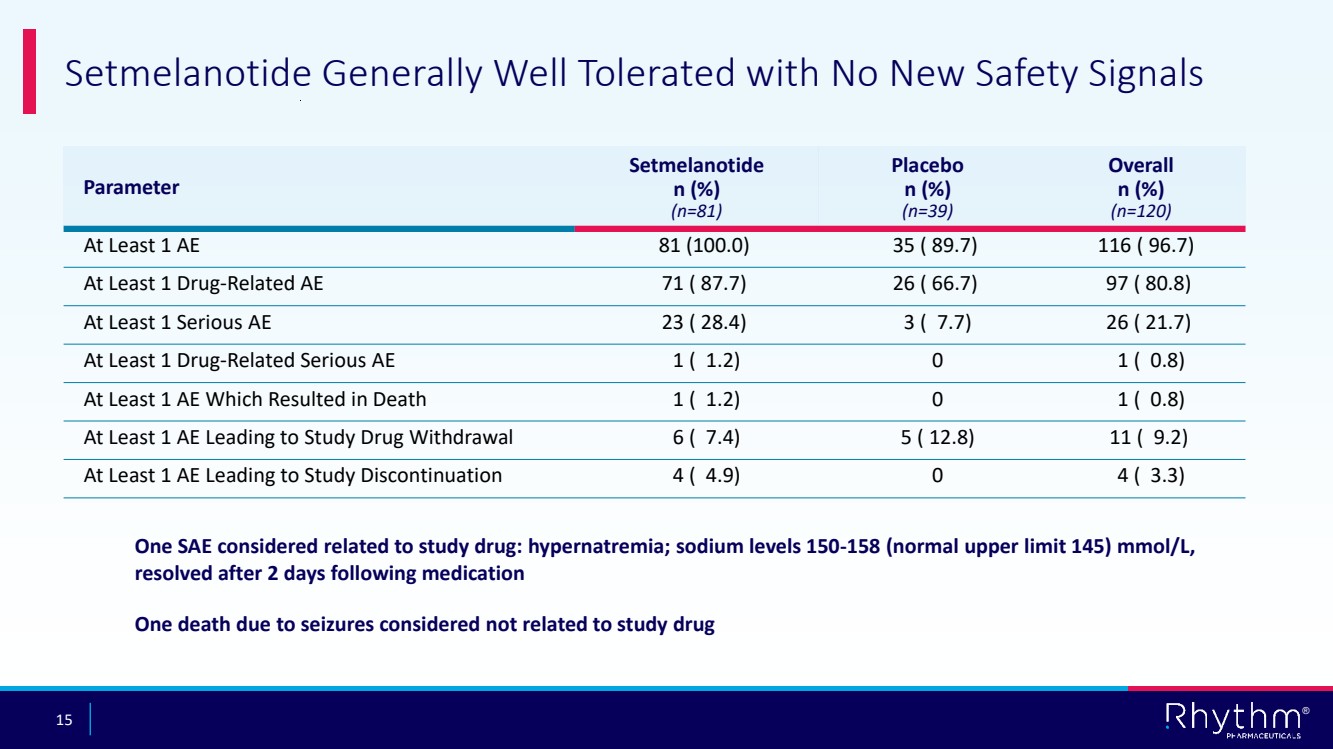
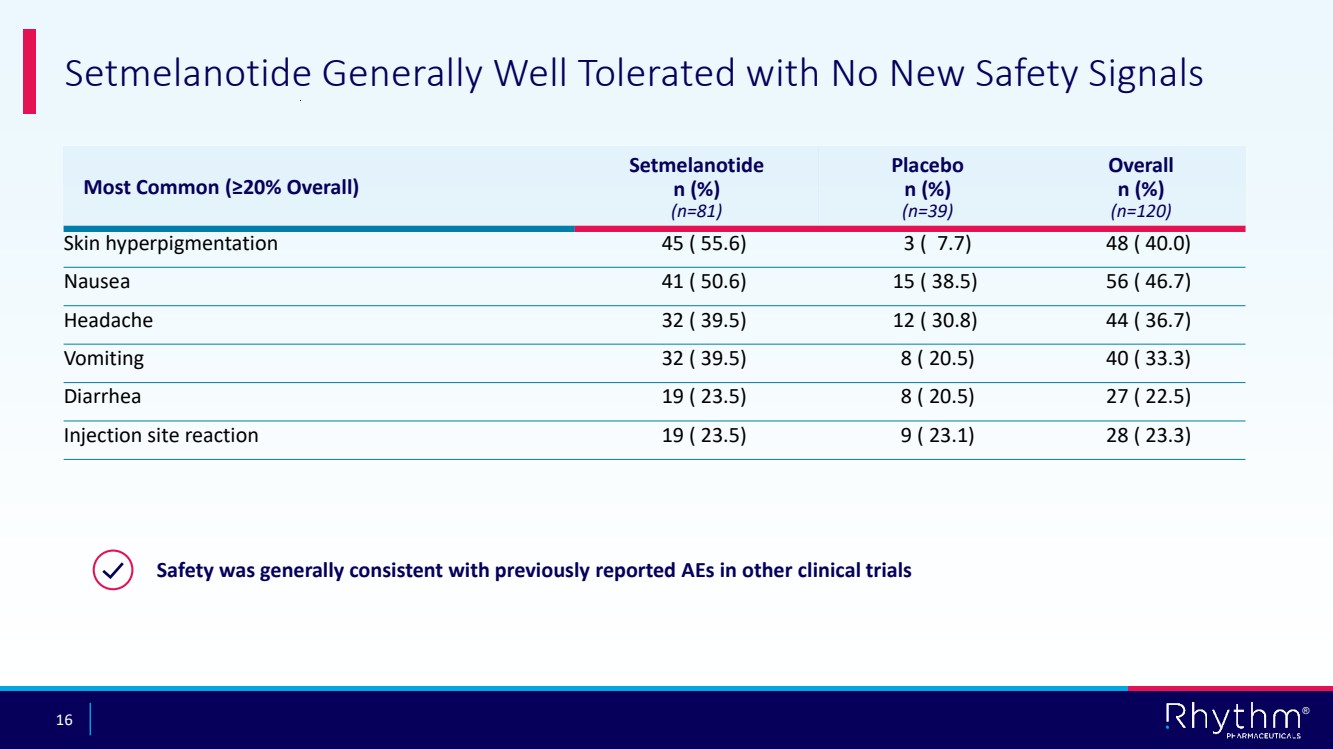
No new safety signals with setmelanotide were observed, in line with setmelanotide’s well-established and well-understood safety profile. Consistent with prior clinical experience, setmelanotide was generally well tolerated in the TRANSCEND study. The most common treatment-emergent adverse events (affecting >20% of patients treated with setmelanotide) were nausea, vomiting, diarrhea, injection site reaction, skin hyperpigmentation and headache. Only one drug-related serious adverse event was reported, and no serious adverse events leading to study discontinuation were reported. The breakdown of the reported adverse events is as below:
Parameter |
Setmelanotide |
Placebo |
Overall |
At Least 1 AE |
81 (100.0) |
35 (89.7) |
116 (96.7) |
At Least 1 Drug-Related AE |
71 (87.7) |
26 (66.7) |
97 (80.8) |
At Least 1 Serious AE |
23 (28.4) |
3 (7.7) |
26 (21.7) |
At Least 1 Drug-Related Serious AE |
1 (1.2) |
0 |
1 (0.8) |
At Least 1 AE Which Resulted in Death |
1 (1.2) |
0 |
1 (0.8) |
At Least 1 AE Leading to Study Drug Withdrawal |
6 (7.4) |
5 (12.8) |
11 (9.2) |
At Least 1 AE Leading to Study Discontinued |
4 (4.9) |
0 |
4 (3.3) |
Most Common (≥20% Overall) |
Setmelanotide |
Placebo |
Overall |
Skin hyperpigmentation |
45 (55.6) |
3 (7.7) |
48 (40.0) |
Nausea |
41 (50.6) |
15 (38.5) |
56 (46.7) |
Headache |
32 (39.5) |
12 (30.8) |
44 (36.7) |
Vomiting |
32 (39.5) |
8 (20.5) |
40 (33.3) |
Diarrhea |
19 (23.5) |
8 (20.5) |
27 (22.5) |
Injection site reaction |
19 (23.5) |
9 (23.1) |
28 (23.3) |
Also on April 7, 2025, the Company announced that it expects existing cash and cash equivalents and short-term investments to be sufficient to fund planned operations into 2027.
Item 9.01. Financial Statements and Exhibits.
(d) Exhibits
The following Exhibits 99.1 and 99.2 shall be deemed to be furnished and not filed.
Exhibit |
|
|
No. |
|
Description |
99.1 |
|
|
99.2 |
|
|
104 |
|
Cover Page Interactive Data File (embedded within the inline XBRL document) |
SIGNATURES
Pursuant to the requirements of the Securities Exchange Act of 1934, as amended, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
|
RHYTHM PHARMACEUTICALS, INC. |
|
|
|
|
Date: April 7, 2025 |
By: |
/s/ Hunter Smith |
|
|
Hunter Smith |
|
|
Chief Financial Officer |
Exhibit 99.1

Rhythm Pharmaceuticals Announces Pivotal Phase 3 TRANSCEND Trial Meets Primary Endpoint with -19.8% Placebo-adjusted BMI Reduction in Patients (N=120) with Acquired Hypothalamic Obesity
-- Patients with acquired hypothalamic obesity on setmelanotide therapy (n=81) achieved mean BMI change of -16.5% compared with +3.3% for placebo (n=39) at 52 weeks (p<0.0001) --
-- -19.2% placebo-adjusted BMI reduction achieved in adult patients 18 years old and older (n=49) at 52 weeks --
-- -20.2% placebo-adjusted BMI reduction achieved in patients younger than 18 years old (n=71) at 52 weeks --
-- Regulatory submissions in the U.S. and EU anticipated to be completed in the third quarter of 2025 --
-- Company to host conference call today at 8 a.m. ET --
BOSTON, April 7, 2025 – Rhythm Pharmaceuticals, Inc. (Nasdaq: RYTM), a global commercial-stage biopharmaceutical company focused on transforming the lives of patients living with rare neuroendocrine diseases, today announced positive topline results from the pivotal Phase 3 TRANSCEND trial evaluating setmelanotide, a melanocortin-4 receptor (MC4R) agonist, for the treatment of acquired hypothalamic obesity. The global trial met its primary endpoint with a statistically significant and highly clinically meaningful reduction in body mass index (BMI) with setmelanotide in both adult and pediatric patients versus placebo.
Highlights from the topline data include:
· |
-19.8% placebo-adjusted difference in BMI reduction (N=120); |
· |
Primary endpoint of mean BMI reduction of -16.5% from baseline for all patients on setmelanotide therapy (n=81) compared with +3.3% BMI change for patients on placebo (n=39) at 52 weeks (p<0.0001); and |
· |
80% of patients on setmelanotide achieved BMI reduction of 5% or greater at 52 weeks. |
“Acquired hypothalamic obesity is a serious disease resulting from damage to the hypothalamus, often due to brain tumors or their treatment or certain other injuries resulting in accelerated weight gain, hyperphagia and reduction in energy expenditure. There is an urgent need for effective treatments as current approaches, including lifestyle interventions and pharmacotherapy intended for general obesity, have shown limited effectiveness in achieving long-term, durable weight loss,” said Susan Phillips, MD, pediatric endocrinologist at Rady Children’s Hospital-San Diego and professor of pediatrics at UC San Diego School of Medicine. “These data are highly clinically meaningful, offering hope that a new targeted therapy may become available for patients – both adults and children – living with acquired hypothalamic obesity.”
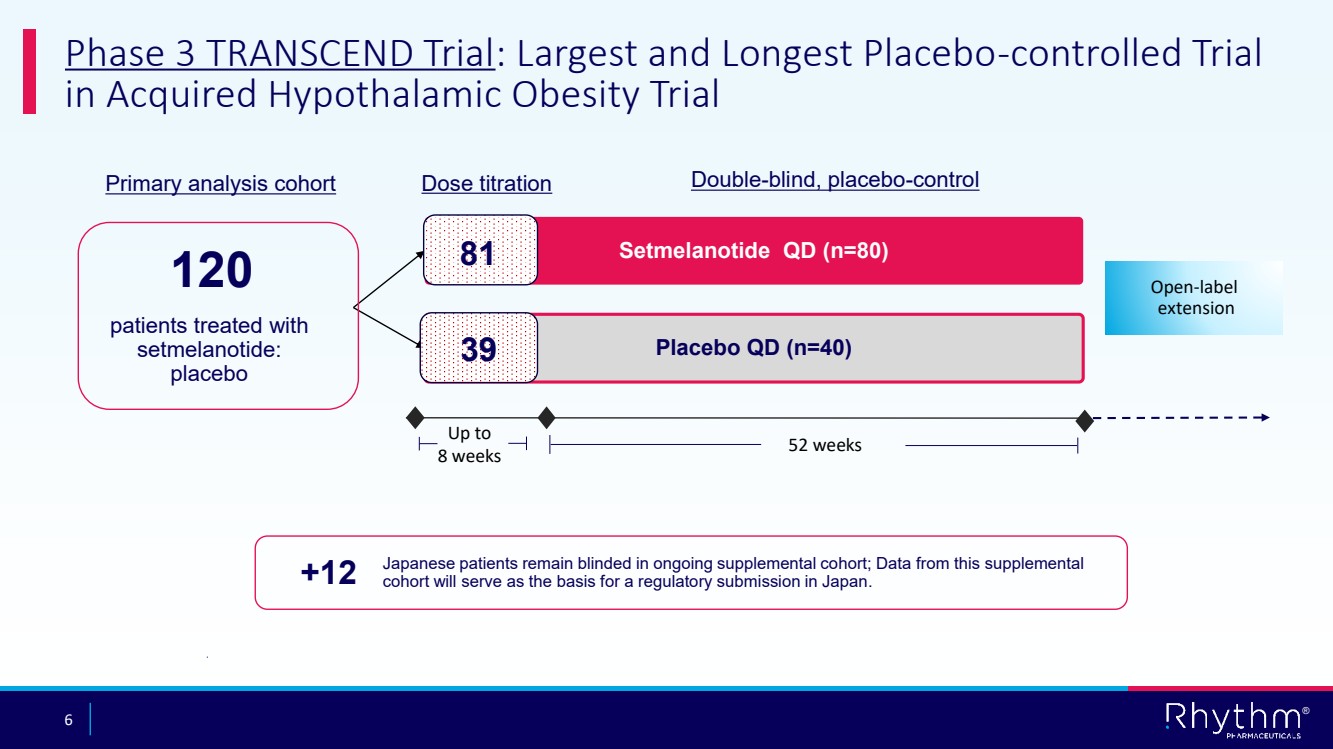
The global Phase 3 TRANSCEND trial is believed to be the largest and longest placebo-controlled trial to evaluate a therapy for patients with acquired hypothalamic obesity. The double-blinded, 52-week trial enrolled 120 patients, randomized 2:1. In addition to the primary endpoint and other data points above, clinically meaningful improvements were observed across key secondary endpoints at week 52, including:
· |
83% percent of patients on setmelanotide therapy achieved 5% or greater reduction in BMI (n=33 patients 18 or older) or BMI Z-score reduction of 0.2 or greater points (n=48 patients younger than 18); and |
· |
-1.4 placebo-adjusted mean change in weekly average of the daily maximal hunger score for patients 12 years old or older (n=81) (p=0.003). |
No new safety signals with setmelanotide were observed, in line with setmelanotide’s well-established and well-understood safety profile. Consistent with prior clinical experience, setmelanotide was generally well tolerated in the TRANSCEND study. The most common treatment-emergent adverse events (affecting >20% of participants) were nausea, vomiting, diarrhea, injection site reaction, skin hyperpigmentation and headache. No serious adverse events leading to study discontinuation were reported.
“This 12-month placebo-controlled trial required an incredible commitment from patients, their families and clinical staff for which we are extremely grateful. The highly clinically meaningful results from the TRANSCEND study potentially represent a transformational milestone for Rhythm,” said David Meeker, M.D., Chairman, President and Chief Executive Officer of Rhythm. “Given these compelling new efficacy data with setmelanotide in a broader patient population than in our Phase 2 trial, we are preparing to submit a supplemental New Drug Application to the FDA and a Type II variation request to the European Medicines Agency in the third quarter of 2025. These planned submissions could pave the way for setmelanotide to become the first-ever approved therapy for these patients. In addition, these strong results with an MC4R agonist increase our confidence in the development of our next-generation MC4R agonists, currently in ongoing Phase 1/2 clinical trials in acquired hypothalamic obesity.”
Rhythm anticipates presenting full data from the TRANSCEND study at an upcoming medical meeting.
Conference Call Information
Rhythm Pharmaceuticals will host a live conference call and webcast at 8:00 a.m. ET today to discuss these clinical data. Participants may register for the conference call here. A webcast of the call will also be available under “Events and Presentations” in the Investor Relations section of the Rhythm Pharmaceuticals website at https://ir.rhythmtx.com/. The archived webcast will be available on Rhythm Pharmaceuticals’ website approximately two hours after the conference call and will be available for at least 30 days following the call.
About the Phase 3 TRANSCEND Trial
The global, randomized, double-blind, placebo-controlled Phase 3 TRANSCEND trial evaluated the efficacy and safety of setmelanotide in patients with acquired hypothalamic obesity. A total of 120 patients age 4 years and older were randomized 2:1 to either a daily subcutaneous injection of setmelanotide (80 patients) or placebo (40 patients). The primary endpoint was mean percent change in body mass index (BMI) from baseline after 52 weeks of treatment. Secondary endpoints assess daily hunger, hyperphagia (extreme unsatisfied drive to consume food), weight, quality of life and safety and tolerability. A supplemental cohort of 12 Japanese patients remains ongoing with completion and topline data anticipated in the first quarter of 2026.
About Acquired Hypothalamic Obesity
Acquired hypothalamic obesity is a rare form of obesity that occurs following damage to the hypothalamic region of the brain, which includes the melanocortin-4 receptor (MC4R) pathway and is responsible for controlling physiological functions such as hunger and weight regulation. Acquired hypothalamic obesity most frequently follows the growth or surgical removal of craniopharyngioma, astrocytoma or other rare brain tumors. Additional causes of injury may include traumatic brain injury, stroke, or inflammation due to infection. Patients experience accelerated weight gain, a reduction in energy expenditure, and hyperphagia (a chronic pathological condition characterized by insatiable hunger, impaired satiety, and persistent abnormal food-seeking behaviors) leading to severe obesity within six to 12 months following tumor resection or other injury.
Rhythm estimates there are 5,000 to 10,000 people living with hypothalamic obesity in the U.S., 5,000 to 8,000 people living with hypothalamic obesity in Japan, and 3,500 to 10,000 people living with hypothalamic obesity in the E.U.
Setmelanotide Indication
In the United States, setmelanotide is indicated to reduce excess body weight and maintain weight reduction long term in adult and pediatric patients aged 2 years and older with syndromic or monogenic obesity due to Bardet-Biedl syndrome (BBS) or Pro-opiomelanocortin (POMC), proprotein convertase subtilisin/kexin type 1 (PCSK1), or leptin receptor (LEPR) deficiency as determined by an FDA-approved test demonstrating variants in POMC, PCSK1, or LEPR genes that are interpreted as pathogenic, likely pathogenic, or of uncertain significance (VUS).
In the European Union and the United Kingdom, setmelanotide is indicated for the treatment of obesity and the control of hunger associated with genetically confirmed BBS or loss-of-function biallelic POMC, including PCSK1, deficiency or biallelic LEPR deficiency in adults and children 2 years of age and above. In the European Union and the United Kingdom, setmelanotide should be prescribed and supervised by a physician with expertise in obesity with underlying genetic etiology.
Limitations of Use
Setmelanotide is not indicated for the treatment of patients with the following conditions as setmelanotide would not be expected to be effective:
· |
Obesity due to suspected POMC, PCSK1, or LEPR deficiency with POMC, PCSK1, or LEPR variants classified as benign or likely benign |
· |
Other types of obesity not related to BBS or POMC, PCSK1, or LEPR deficiency, including obesity associated with other genetic syndromes and general (polygenic) obesity |
Contraindication
Prior serious hypersensitivity to setmelanotide or any of the excipients in IMCIVREE. Serious hypersensitivity reactions (e.g., anaphylaxis) have been reported.
WARNINGS AND PRECAUTIONS
Disturbance in Sexual Arousal: Spontaneous penile erections in males and sexual adverse reactions in females have occurred. Inform patients that these events may occur and instruct patients who have an erection lasting longer than 4 hours to seek emergency medical attention.
Depression and Suicidal Ideation: Depression, suicidal ideation and depressed mood have occurred. Monitor patients for new onset or worsening depression or suicidal thoughts or behaviors. Consider discontinuing IMCIVREE if patients experience suicidal thoughts or behaviors, or clinically significant or persistent depression symptoms occur.
Hypersensitivity Reactions: Serious hypersensitivity reactions (e.g., anaphylaxis) have been reported. If suspected, advise patients to promptly seek medical attention and discontinue IMCIVREE.
Skin Hyperpigmentation, Darkening of Pre-existing Nevi, and Development of New
Melanocytic Nevi: Generalized or focal increases in skin pigmentation, darkening of pre-existing nevi, development of new melanocytic nevi and increase in size of existing melanocytic nevi have occurred. Perform a full body skin examination prior to initiation and periodically during treatment to monitor pre-existing and new pigmented lesions.
Risk of Serious Adverse Reactions Due to Benzyl Alcohol Preservative in Neonates and Low Birth Weight Infants: IMCIVREE is not approved for use in neonates or infants. Serious and fatal adverse reactions including “gasping syndrome” can occur in neonates and low birth weight infants treated with benzyl alcohol preserved drugs.
ADVERSE REACTIONS
Most common adverse reactions (incidence ≥20%) included skin hyperpigmentation, injection site reactions, nausea, headache, diarrhea, abdominal pain, vomiting, depression, and spontaneous penile erection.
USE IN SPECIFIC POPULATIONS
Treatment with IMCIVREE is not recommended when breastfeeding. Discontinue IMCIVREE when pregnancy is recognized unless the benefits of therapy outweigh the potential risks to the fetus.
To report SUSPECTED ADVERSE REACTIONS, contact Rhythm Pharmaceuticals at +1 (833) 789-6337 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. See section 4.8 of the Summary of Product Characteristics for information on reporting suspected adverse reactions in Europe.
Please see the full Prescribing Information for additional Important Safety Information.
About Rhythm Pharmaceuticals
Rhythm is a commercial-stage biopharmaceutical company committed to transforming the lives of patients and their families living with rare neuroendocrine diseases. Rhythm’s lead asset, IMCIVREE® (setmelanotide), an MC4R agonist designed to treat hyperphagia and severe obesity, is approved by the U.S. Food and Drug Administration (FDA) to reduce excess body weight and maintain weight reduction long term in adult and pediatric patients 2 years of age and older with syndromic or monogenic obesity due to Bardet-Biedl syndrome (BBS) or genetically confirmed pro-opiomelanocortin (POMC), including proprotein convertase subtilisin/kexin type 1 (PCSK1), deficiency or leptin receptor (LEPR) deficiency. Both the European Commission (EC) and the UK’s Medicines & Healthcare Products Regulatory Agency (MHRA) have authorized setmelanotide for the treatment of obesity and the control of hunger associated with genetically confirmed BBS or genetically confirmed loss-of-function biallelic POMC, including PCSK1, deficiency or biallelic LEPR deficiency in adults and children 2 years of age and above. Additionally, Rhythm is advancing a broad clinical development program for setmelanotide in other rare diseases, as well as investigational MC4R agonists bivamelagon and RM-718, and a preclinical suite of small molecules for the treatment of congenital hyperinsulinism. Rhythm’s headquarters is in Boston, MA.
Forward-Looking Statements This press release contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. All statements contained in this press release that do not relate to matters of historical fact should be considered forward-looking statements, including without limitation statements regarding our pivotal Phase 3 TRANSCEND study evaluating setmelanotide for the treatment of acquired hypothalamic obesity and the potential for setmelanotide to treat hypothalamic obesity; the safety, efficacy, potential benefits of, and clinical design or progress of any of our products or product candidates at any dosage or in any indication; our expectations surrounding potential regulatory submissions, progress, or approvals and timing thereof for any of our product candidates, including the anticipated supplemental New Drug Application to the FDA and a Type II variation request to the European Medicines Agency; the estimated market size and addressable population for our drug products, including setmelanotide for the treatment of hypothalamic obesity; the future announcement of data from our other ongoing clinical trials, including the Japanese cohort of our Phase 3 trial evaluating setmelanotide for patients with acquired hypothalamic obesity; our participation in and presentation of the full data from the TRANSCEND study at an upcoming medical meeting; and the timing of any of the foregoing. Statements using words such as “expect”, “anticipate”, “believe”, “may”, “will”, “aim” and similar terms are also forward-looking statements. Such statements are subject to numerous risks and uncertainties, including, but not limited to, our ability to enroll patients in clinical trials, the design and outcome of clinical trials, the ability to achieve necessary regulatory approvals, risks associated with data analysis and reporting, positive results from earlier clinical trials of setmelanotide may not be predictive of the results of later clinical trials of setmelanotide, interim, topline and preliminary data that we announced may change as more patient data become available, setmelanotide may cause undesirable side effects that could delay or prevent additional regulatory approvals or limit the commercial profile of approved labeling, Breakthrough Therapy designation by the FDA may not lead to a faster development, regulatory review or approval process, and nor does it increase the likelihood that setmelanotide will receive additional marketing approvals in the United States, failure to identify and develop additional product candidates, unfavorable pricing regulations, third-party reimbursement practices or healthcare reform initiatives, risks associated with the laws and regulations governing our international operations and the costs of any related compliance programs, the impact of competition, risks related to the commercialization and market acceptance of IMCIVREE for the treatment of hypothalamic obesity in the medical community and with third-party payors, and the other important factors discussed under the caption “Risk Factors” in our Annual Report on Form 10-K for the year ended December 31, 2024 and our other filings with the Securities and Exchange Commission. Except as required by law, we undertake no obligations to make any revisions to the forward-looking statements contained in this press release or to update them to reflect events or circumstances occurring after the date of this press release, whether as a result of new information, future developments or otherwise.
# # #
Corporate Contact:
David Connolly
Head of Investor Relations and Corporate Communications
Rhythm Pharmaceuticals, Inc.
857-264-4280
dconnolly@rhythmtx.com
Media Contact:
Sheryl Seapy
Real Chemistry
(949) 903-4750
sseapy@realchemistry.com
|
© 2025. Rhythm Pharmaceuticals, Inc. All rights reserved. Rhythm and its logo are trademarks of Rhythm Pharmaceuticals, Inc. ® April 7, 2025 Rhythm Pharmaceuticals Positive Topline Results from Phase 3 Trial Evaluating Setmelanotide in Patients with Acquired Hypothalamic Obesity |
|
2 ® This presentation and the accompanying oral presentation contain forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. All statements contained in this presentation that do not relate to matters of historical fact should be considered forward-looking statements, including without limitation statements regarding our pivotal Phase 3 TRANSCEND study evaluating setmelanotide for the treatment of acquired hypothalamic obesity and the potential for setmelanotide to treat hypothalamic obesity; the safety, efficacy, potential benefits of, and clinical design or progress of any of our products or product candidates at any dosage or in any indication; our expectations surrounding potential regulatory submissions, progress, or approvals and timing thereof for any of our product candidates, including the anticipated supplemental New Drug Application to the FDA and a Type II variation request to the European Medicines Agency; the estimated market size and addressable population for our drug products, including setmelanotide for the treatment of hypothalamic obesity; the future announcement of data from our other ongoing clinical trials, including the Japanese cohort of our Phase 3 trial evaluating setmelanotide for patients with acquired hypothalamic obesity; our participation in and presentation of the full data from the TRANSCEND study at an upcoming medical meeting; and the timing of any of the foregoing. Statements using words such as “expect”, “anticipate”, “believe”, “may”, “will”, “aim” and similar terms are also forward-looking statements. Such statements are subject to numerous risks and uncertainties, including, but not limited to, our ability to enroll patients in clinical trials, the design and outcome of clinical trials, the ability to achieve necessary regulatory approvals, risks associated with data analysis and reporting, positive results from earlier clinical trials of setmelanotide may not be predictive of the results of later clinical trials of setmelanotide, interim, topline and preliminary data that we announced may change as more patient data become available, setmelanotide may cause undesirable side effects that could delay or prevent additional regulatory approvals or limit the commercial profile of approved labeling, Breakthrough Therapy designation by the FDA may not lead to a faster development, regulatory review or approval process, and nor does it increase the likelihood that setmelanotide will receive additional marketing approvals in the United States, failure to identify and develop additional product candidates, unfavorable pricing regulations, third-party reimbursement practices or healthcare reform initiatives, risks associated with the laws and regulations governing our international operations and the costs of any related compliance programs, the impact of competition, risks related to the commercialization and market acceptance of IMCIVREE for the treatment of hypothalamic obesity in the medical community and with third-party payors, and the other important factors discussed under the caption “Risk Factors” in our Annual Report on Form 10-K for the year ended December 31, 2024 and our other filings with the Securities and Exchange Commission. Except as required by law, we undertake no obligations to make any revisions to the forward-looking statements contained in this press release or to update them to reflect events or circumstances occurring after the date of this press release, whether as a result of new information, future developments or otherwise. Industry and Other Data Unless otherwise indicated, information contained in this presentation concerning our industry and the markets in which Rhythm operates, including its general expectations, market position and market opportunity, is based on its management’s estimates and research, as well as industry and general publications and research, surveys and studies conducted by third parties. While we believe the information from these third-party publications, research, surveys and studies is reliable, it does not guarantee the accuracy or completeness of such information, and Rhythm has not independently verified this information. Management’s estimates are derived from publicly available information, their knowledge of the company's industry and their assumptions based on such information and knowledge, which they believe to be reasonable. This data involves a number of assumptions and limitations which are necessarily subject to a high degree of uncertainty and risk due to a variety of factors, including those described in our periodic reports filed with the Securities and Exchange Commission under the captions “Cautionary Note Regarding Forward Looking Statements,” “Summary Risk Factors” and “Risk Factors.” These and other factors could cause Rhythm’s future performance and market expectations to differ materially from its assumptions and estimates. Forward-looking Statements |
|
3 ® David Meeker, MD Chair, President and Chief Executive Officer Hunter C. Smith Chief Financial Officer On Today’s Call Susan Phillips, MD Pediatric Endocrinologist at Rady Children's Hospital-San Diego Professor of Pediatrics at UC San Diego School of Medicine |
|
4 ® David Meeker, MD Chair, President and CEO |
|
5 ® Acquired Hypothalamic Obesity Represents Significant Global Opportunity Rare, life-changing disease with severe impact and burden on patients and families Significant unmet need with no approved therapies Identified, actively engaged patient community Setmelanotide achieved highly clinically meaningful BMI reduction in largest, placebo-controlled study ever conducted in acquired hypothalamic obesity |
|
6 ® Phase 3 TRANSCEND Trial: Largest and Longest Placebo-controlled Trial in Acquired Hypothalamic Obesity Trial Setmelanotide QD (n=80) Double-blind, placebo-control Placebo QD (n=40) Up to 8 weeks 52 weeks Dose titration Open-label extension patients treated with setmelanotide: placebo 120 Primary analysis cohort +12 Japanese patients remain blinded in ongoing supplemental cohort; Data from this supplemental cohort will serve as the basis for a regulatory submission in Japan. 81 39 |
|
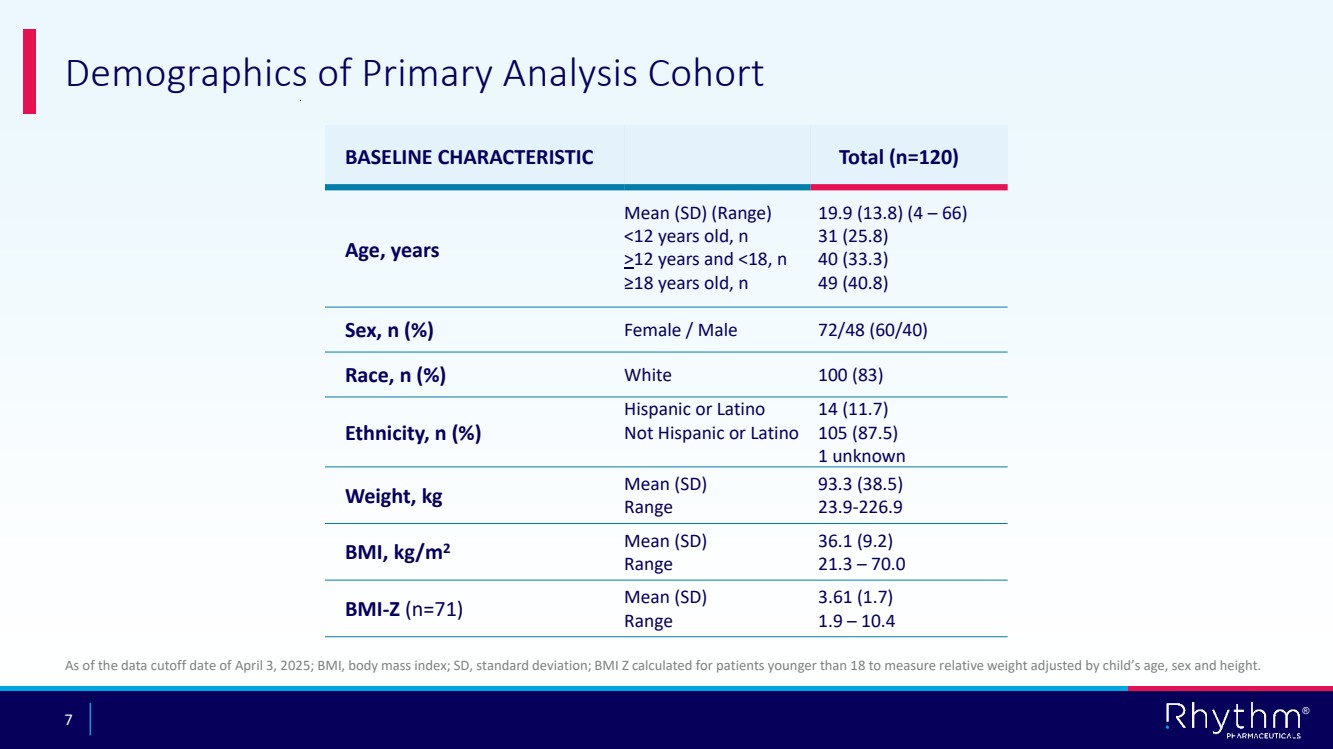
7 ® BASELINE CHARACTERISTIC Total (n=120) Age, years Mean (SD) (Range) <12 years old, n >12 years and <18, n ≥18 years old, n 19.9 (13.8) (4 – 66) 31 (25.8) 40 (33.3) 49 (40.8) Sex, n (%) Female / Male 72/48 (60/40) Race, n (%) White 100 (83) Ethnicity, n (%) Hispanic or Latino Not Hispanic or Latino 14 (11.7) 105 (87.5) 1 unknown Weight, kg Mean (SD) Range 93.3 (38.5) 23.9-226.9 BMI, kg/m2 Mean (SD) Range 36.1 (9.2) 21.3 – 70.0 BMI-Z (n=71) Mean (SD) Range 3.61 (1.7) 1.9 – 10.4 Demographics of Primary Analysis Cohort As of the data cutoff date of April 3, 2025; BMI, body mass index; SD, standard deviation; BMI Z calculated for patients younger than 18 to measure relative weight adjusted by child’s age, sex and height. |
|
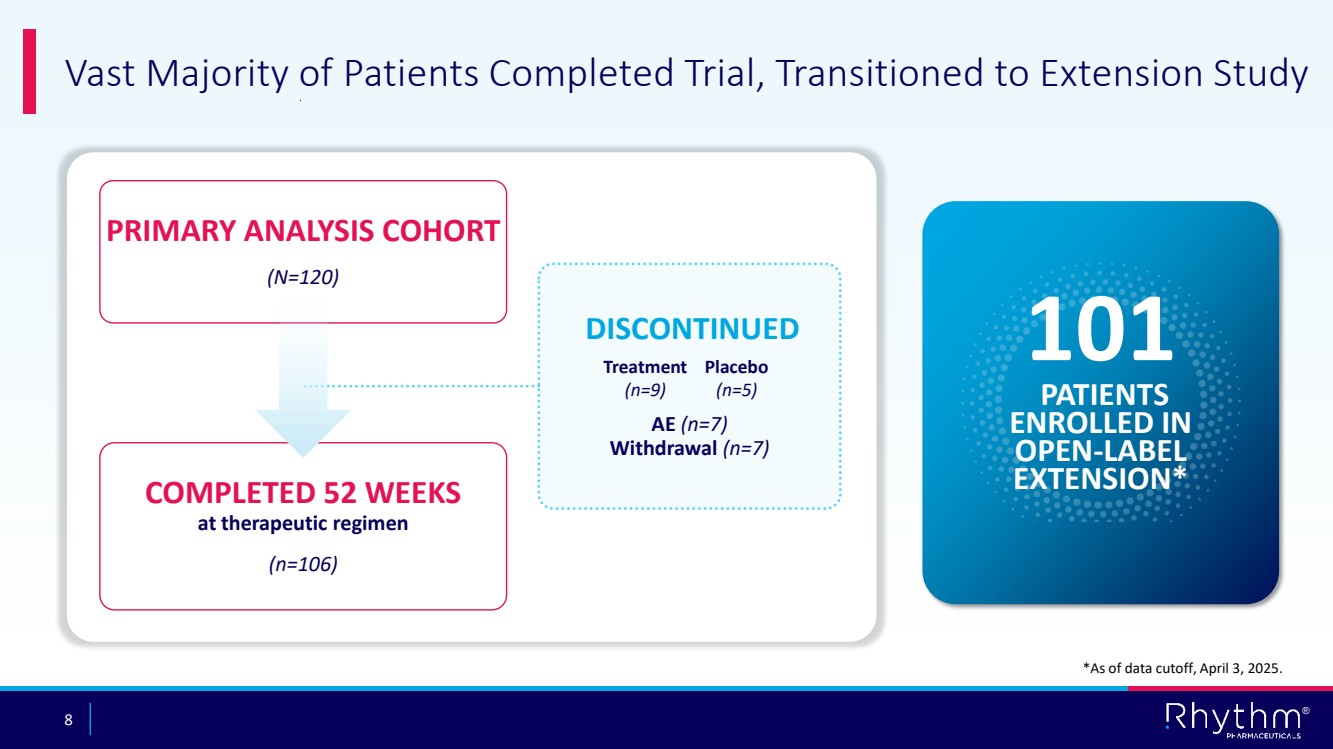
8 ® COMPLETED 52 WEEKS at therapeutic regimen (n=106) PRIMARY ANALYSIS COHORT (N=120) Vast Majority of Patients Completed Trial, Transitioned to Extension Study DISCONTINUED AE (n=7) Withdrawal (n=7) 101 PATIENTS ENROLLED IN OPEN-LABEL EXTENSION* Treatment (n=9) Placebo (n=5) *As of data cutoff, April 3, 2025. |
|
9 ® Setmelanotide Achieved Statistically Significant and Highly Clinically Meaningful Reduction in BMI Primary analysis cohort (N=120) -19.8% Placebo-adjusted difference in BMI reduction from baseline (P<0.0001) -16.5% BMI change from baseline in Setmelanotide arm (n=81) +3.3% BMI change from baseline in Placebo arm (n=39) NOTE: Shown are the least square (LS) means for setmelanotide and placebo groups and the LS mean difference in mean percentage change from baseline in BMI at Week 52, obtained from an analysis of covariance (ANCOVA) model. Rubin’s Rule was used to provide the overall estimates of differences in LS means and p-value. |
|
10 ® -40 -30 -20 -10 0 10 20 % Change from Baseline -16.3% +3.9% -40 -30 -20 -10 0 10 Significant Reductions in BMI Observed in both Adults and Children ≥18 Years Old (n=49) (P<0.0001) Setmelanotide Placebo % Change from Baseline <18 Years Old (n=71) -19.2% Placebo-adjusted Difference -16.8% +2.4% (P<0.0001) Setmelanotide Placebo -20.2% Placebo-adjusted Difference (n=33) (n=16) (n=48) (n=23) |
|
11 ® 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 5% 10% 15% 20% Proportion of patients Consistent Response to Setmelanotide Therapy Observed across Majority of Patients 5% 3% 51% 0% 43% Setmelanotide Placebo 10% 80% 63% P<0.0001 P<0.0001 P<0.0001 P<0.0001 Observed Reduction in BMI at 52 weeks |
|
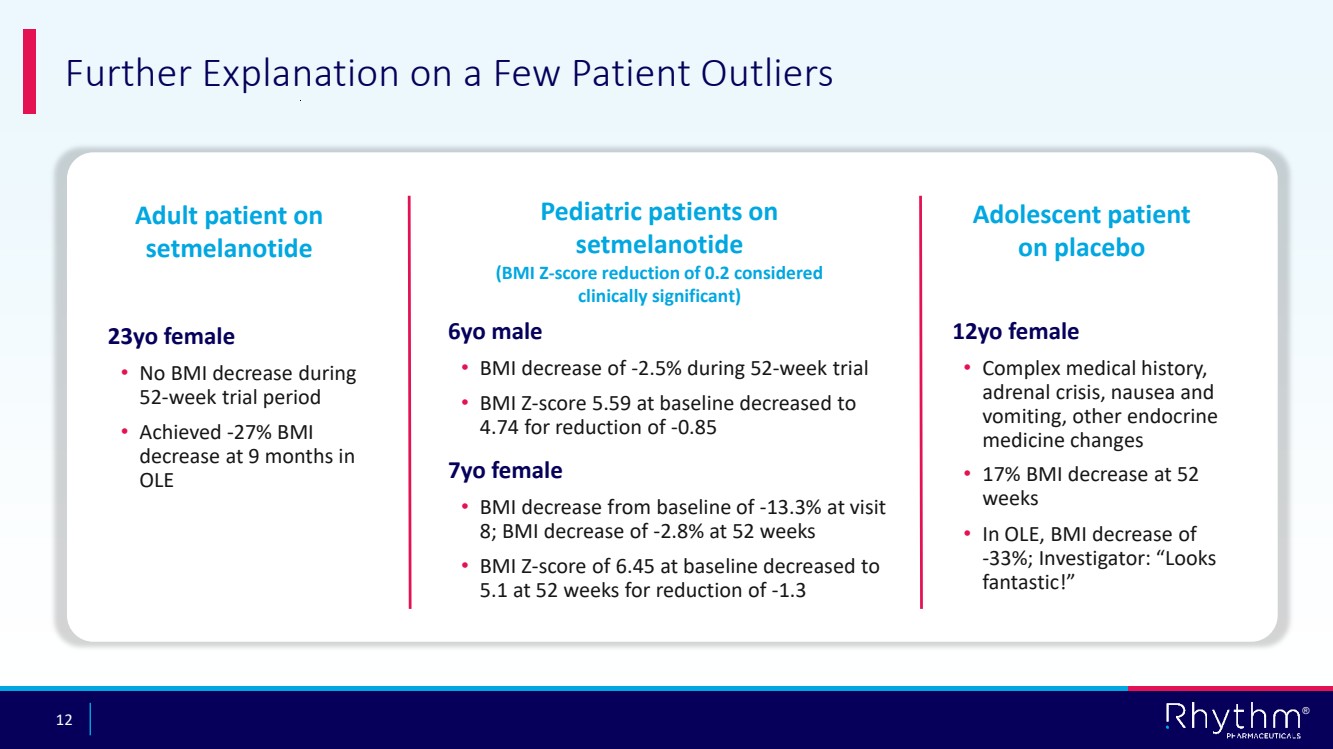
12 ® Further Explanation on a Few Patient Outliers Adult patient on setmelanotide 23yo female • No BMI decrease during 52-week trial period • Achieved -27% BMI decrease at 9 months in OLE Pediatric patients on setmelanotide (BMI Z-score reduction of 0.2 considered clinically significant) 6yo male • BMI decrease of -2.5% during 52-week trial • BMI Z-score 5.59 at baseline decreased to 4.74 for reduction of -0.85 7yo female • BMI decrease from baseline of -13.3% at visit 8; BMI decrease of -2.8% at 52 weeks • BMI Z-score of 6.45 at baseline decreased to 5.1 at 52 weeks for reduction of -1.3 Adolescent patient on placebo 12yo female • Complex medical history, adrenal crisis, nausea and vomiting, other endocrine medicine changes • 17% BMI decrease at 52 weeks • In OLE, BMI decrease of -33%; Investigator: “Looks fantastic!” |
|
13 ® Setmelanotide Achieved Statistically Significant Reduction in Hunger Compared with Placebo in Patients ≥12 Years Old Note: Patients ≥12 years of age were administered the questionnaire. Patients rated their hunger on an 11-point numeric rating scale ranging from 0 to 10 (0 = not hungry at all and 10 = hungriest possible) with a recall period of 24 hours. -6 -5 -4 -3 -2 -1 0 1 Setmelanotide Placebo Change from Baseline (n=57) (n=24) -2.7 -1.2 -1.4 Placebo-adjusted Difference (P<0.003) |
|
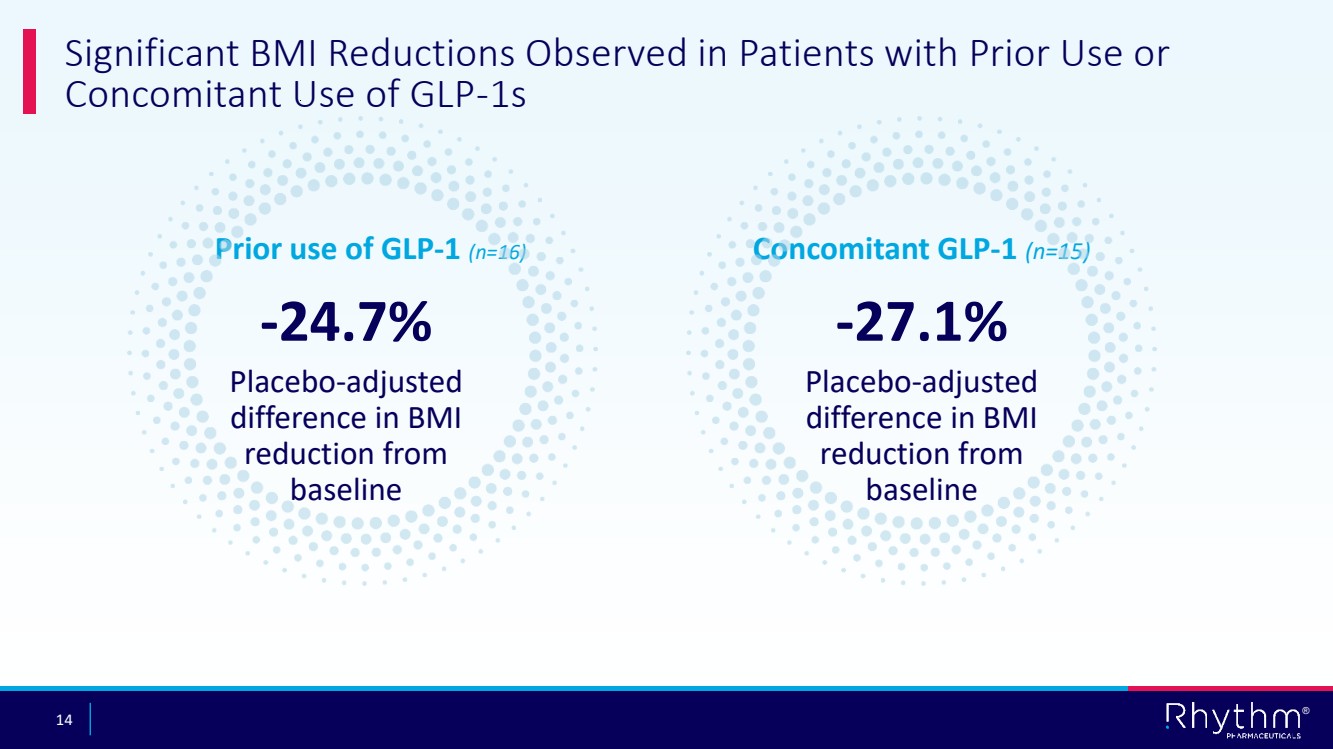
14 ® Significant BMI Reductions Observed in Patients with Prior Use or Concomitant Use of GLP-1s -24.7% Placebo-adjusted difference in BMI reduction from baseline Prior use of GLP-1 (n=16) Concomitant GLP-1 (n=15) -27.1% Placebo-adjusted difference in BMI reduction from baseline |
|
15 ® Setmelanotide Generally Well Tolerated with No New Safety Signals Parameter Setmelanotide n (%) (n=81) Placebo n (%) (n=39) Overall n (%) (n=120) At Least 1 AE 81 (100.0) 35 ( 89.7) 116 ( 96.7) At Least 1 Drug-Related AE 71 ( 87.7) 26 ( 66.7) 97 ( 80.8) At Least 1 Serious AE 23 ( 28.4) 3 ( 7.7) 26 ( 21.7) At Least 1 Drug-Related Serious AE 1 ( 1.2) 0 1 ( 0.8) At Least 1 AE Which Resulted in Death 1 ( 1.2) 0 1 ( 0.8) At Least 1 AE Leading to Study Drug Withdrawal 6 ( 7.4) 5 ( 12.8) 11 ( 9.2) At Least 1 AE Leading to Study Discontinuation 4 ( 4.9) 0 4 ( 3.3) One SAE considered related to study drug: hypernatremia; sodium levels 150-158 (normal upper limit 145) mmol/L, resolved after 2 days following medication One death due to seizures considered not related to study drug |
|
16 ® Setmelanotide Generally Well Tolerated with No New Safety Signals Most Common (≥20% Overall) Setmelanotide n (%) (n=81) Placebo n (%) (n=39) Overall n (%) (n=120) Skin hyperpigmentation 45 ( 55.6) 3 ( 7.7) 48 ( 40.0) Nausea 41 ( 50.6) 15 ( 38.5) 56 ( 46.7) Headache 32 ( 39.5) 12 ( 30.8) 44 ( 36.7) Vomiting 32 ( 39.5) 8 ( 20.5) 40 ( 33.3) Diarrhea 19 ( 23.5) 8 ( 20.5) 27 ( 22.5) Injection site reaction 19 ( 23.5) 9 ( 23.1) 28 ( 23.3) Safety was generally consistent with previously reported AEs in other clinical trials |
|
17 ® Susan Phillips, MD Pediatric endocrinologist at Rady Children's Hospital-San Diego; Professor of pediatrics at UC San Diego School of Medicine |
|
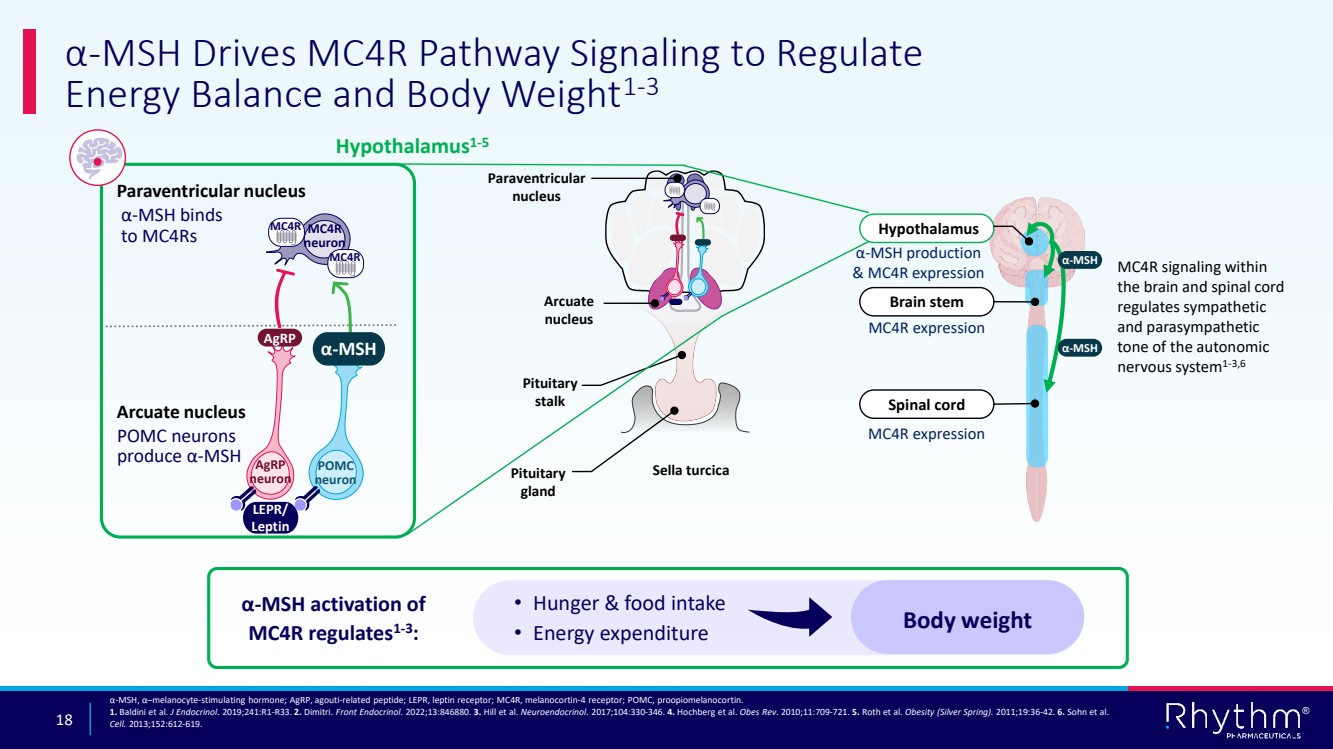
18 ® α-MSH Drives MC4R Pathway Signaling to Regulate Energy Balance and Body Weight1-3 α-MSH, α–melanocyte-stimulating hormone; AgRP, agouti-related peptide; LEPR, leptin receptor; MC4R, melanocortin-4 receptor; POMC, proopiomelanocortin. 1. Baldini et al. J Endocrinol. 2019;241:R1-R33. 2. Dimitri. Front Endocrinol. 2022;13:846880. 3. Hill et al. Neuroendocrinol. 2017;104:330-346. 4. Hochberg et al. Obes Rev. 2010;11:709-721. 5. Roth et al. Obesity (Silver Spring). 2011;19:36-42. 6. Sohn et al. Cell. 2013;152:612-619. Arcuate nucleus Paraventricular nucleus Sella turcica Pituitary stalk MC4R expression MC4R expression MC4R signaling within the brain and spinal cord regulates sympathetic and parasympathetic tone of the autonomic nervous system1-3,6 α-MSH production & MC4R expression Hypothalamus1-5 Paraventricular nucleus α-MSH binds to MC4Rs Arcuate nucleus POMC neurons produce α-MSH LEPR/ Leptin AgRP neuron AgRP POMC neuron α-MSH MC4R neuron MC4R MC4R Hypothalamus Brain stem Spinal cord α-MSH α-MSH α-MSH activation of MC4R regulates1-3 : • Hunger & food intake • Energy expenditure Body weight Pituitary gland |
|
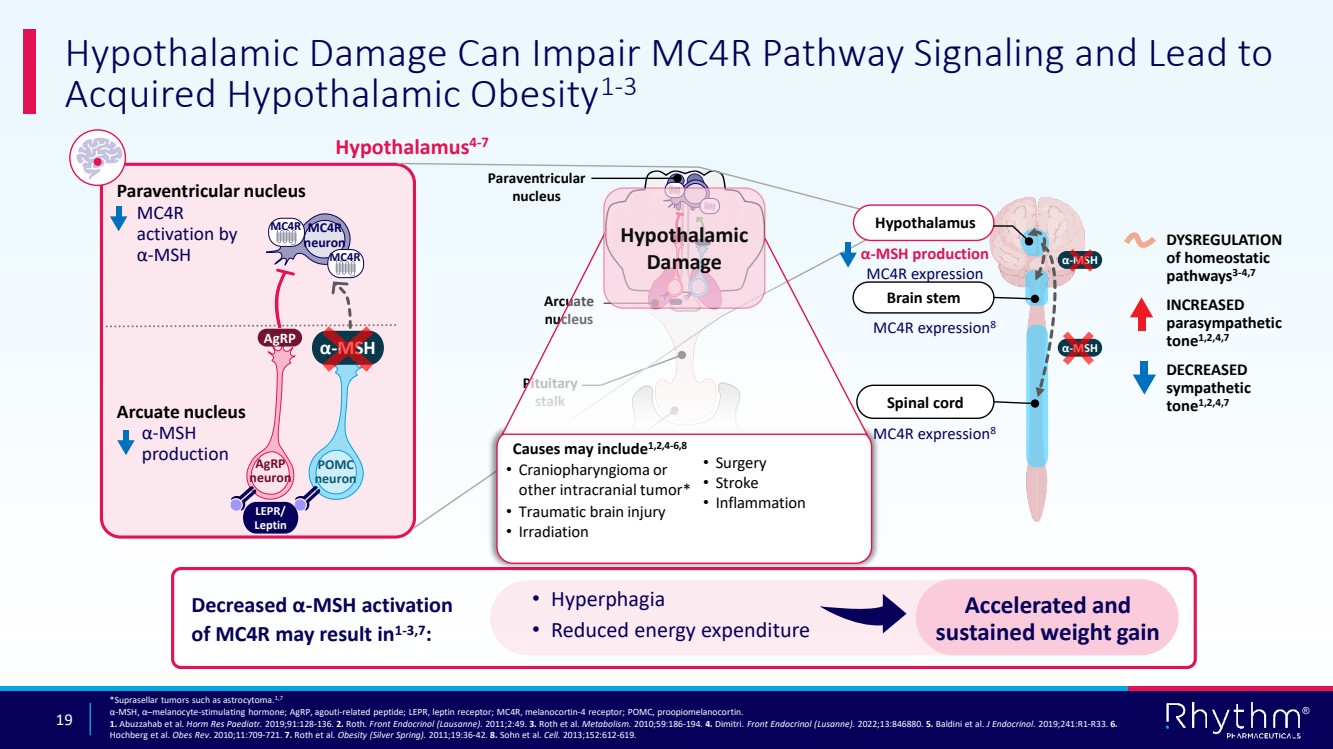
19 ® Hypothalamic Damage Can Impair MC4R Pathway Signaling and Lead to Acquired Hypothalamic Obesity1-3 *Suprasellar tumors such as astrocytoma.1,7 α-MSH, α–melanocyte-stimulating hormone; AgRP, agouti-related peptide; LEPR, leptin receptor; MC4R, melanocortin-4 receptor; POMC, proopiomelanocortin. 1. Abuzzahab et al. Horm Res Paediatr. 2019;91:128-136. 2. Roth. Front Endocrinol (Lausanne). 2011;2:49. 3. Roth et al. Metabolism. 2010;59:186-194. 4. Dimitri. Front Endocrinol (Lusanne). 2022;13:846880. 5. Baldini et al. J Endocrinol. 2019;241:R1-R33. 6. Hochberg et al. Obes Rev. 2010;11:709-721. 7. Roth et al. Obesity (Silver Spring). 2011;19:36-42. 8. Sohn et al. Cell. 2013;152:612-619. Paraventricular nucleus Arcuate nucleus Sella turcica Pituitary stalk Pituitary gland MC4R expression8 Decreased α-MSH activation of MC4R may result in1-3,7: • Hyperphagia • Reduced energy expenditure Accelerated and sustained weight gain DOWNSTREAM UPSTREAM Hypothalamus4-7 Paraventricular nucleus Arcuate nucleus AgRP neuron AgRP POMC neuron α-MSH MC4R neuron MC4R MC4R α-MSH production MC4R expression Hypothalamus Brain stem Spinal cord α-MSH α-MSH MC4R expression8 DYSREGULATION of homeostatic pathways3-4,7 INCREASED parasympathetic tone1,2,4,7 DECREASED sympathetic tone1,2,4,7 Causes may include1,2,4-6,8 • Surgery • Stroke • Inflammation • Craniopharyngioma or other intracranial tumor* • Traumatic brain injury • Irradiation α-MSH production MC4R activation by α-MSH LEPR/ Leptin Hypothalamic Damage |
|
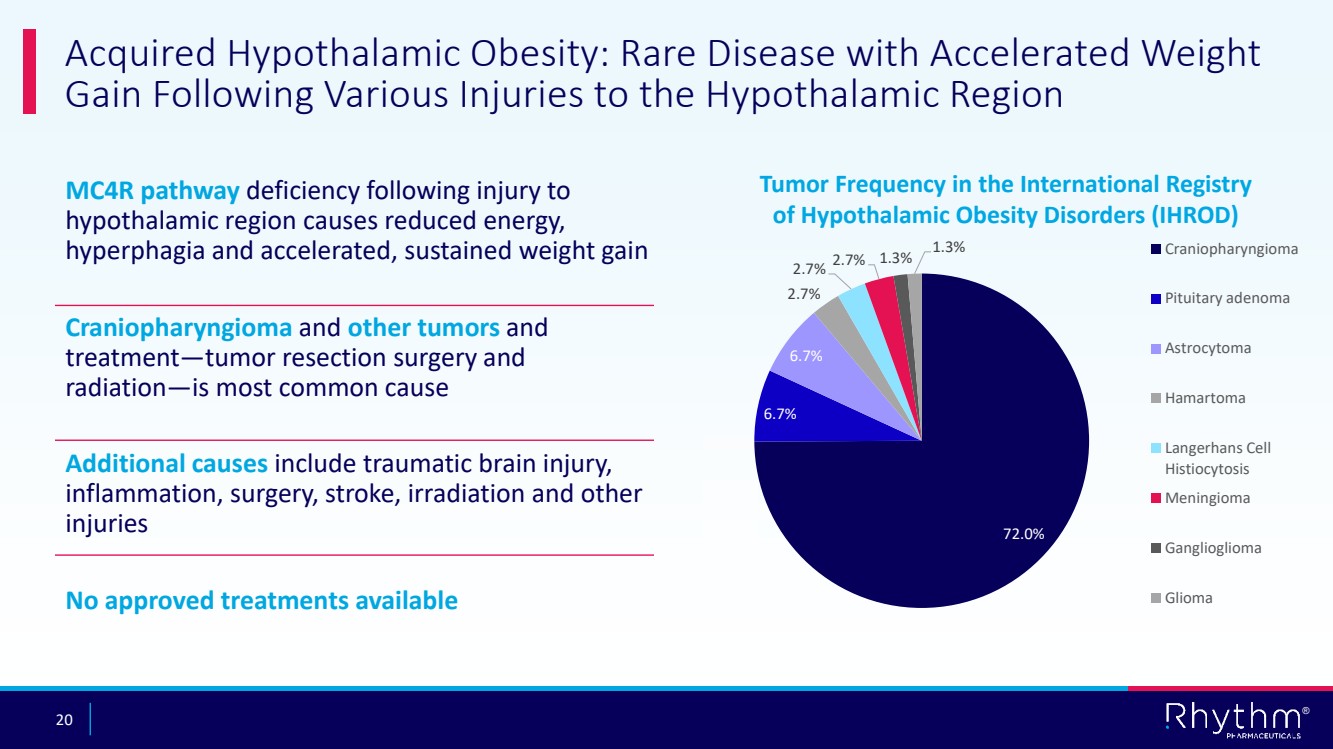
20 ® Acquired Hypothalamic Obesity: Rare Disease with Accelerated Weight Gain Following Various Injuries to the Hypothalamic Region MC4R pathway deficiency following injury to hypothalamic region causes reduced energy, hyperphagia and accelerated, sustained weight gain Craniopharyngioma and other tumors and treatment—tumor resection surgery and radiation—is most common cause Additional causes include traumatic brain injury, inflammation, surgery, stroke, irradiation and other injuries No approved treatments available 72.0% 6.7% 6.7% 2.7% 2.7% 2.7% 1.3% 1.3% Tumor Frequency in the International Registry of Hypothalamic Obesity Disorders (IHROD) Craniopharyngioma Pituitary adenoma Astrocytoma Hamartoma Langerhans Cell Histiocytosis Meningioma Ganglioglioma Glioma |
|
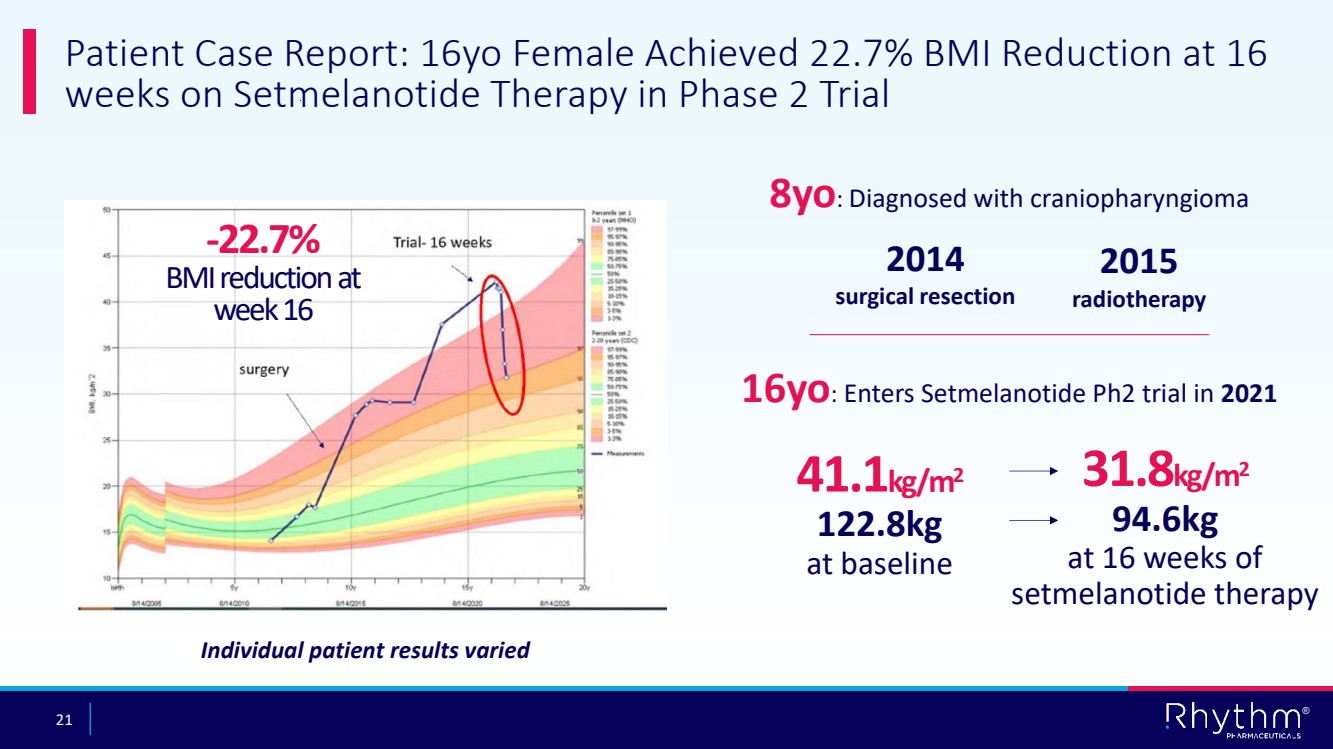
21 ® Patient Case Report: 16yo Female Achieved 22.7% BMI Reduction at 16 weeks on Setmelanotide Therapy in Phase 2 Trial 41.1kg/m2 122.8kg at baseline 8yo: Diagnosed with craniopharyngioma 2014 surgical resection 2015 radiotherapy 16yo: Enters Setmelanotide Ph2 trial in 2021 31.8kg/m2 94.6kg at 16 weeks of setmelanotide therapy -22.7% BMI reduction at week 16 Individual patient results varied |
|
22 ® AUGUST 2021 AUGUST 2024 2013 7yo before tumor diagnosis |
|
23 ® David Meeker, MD Chair, President and CEO |
|
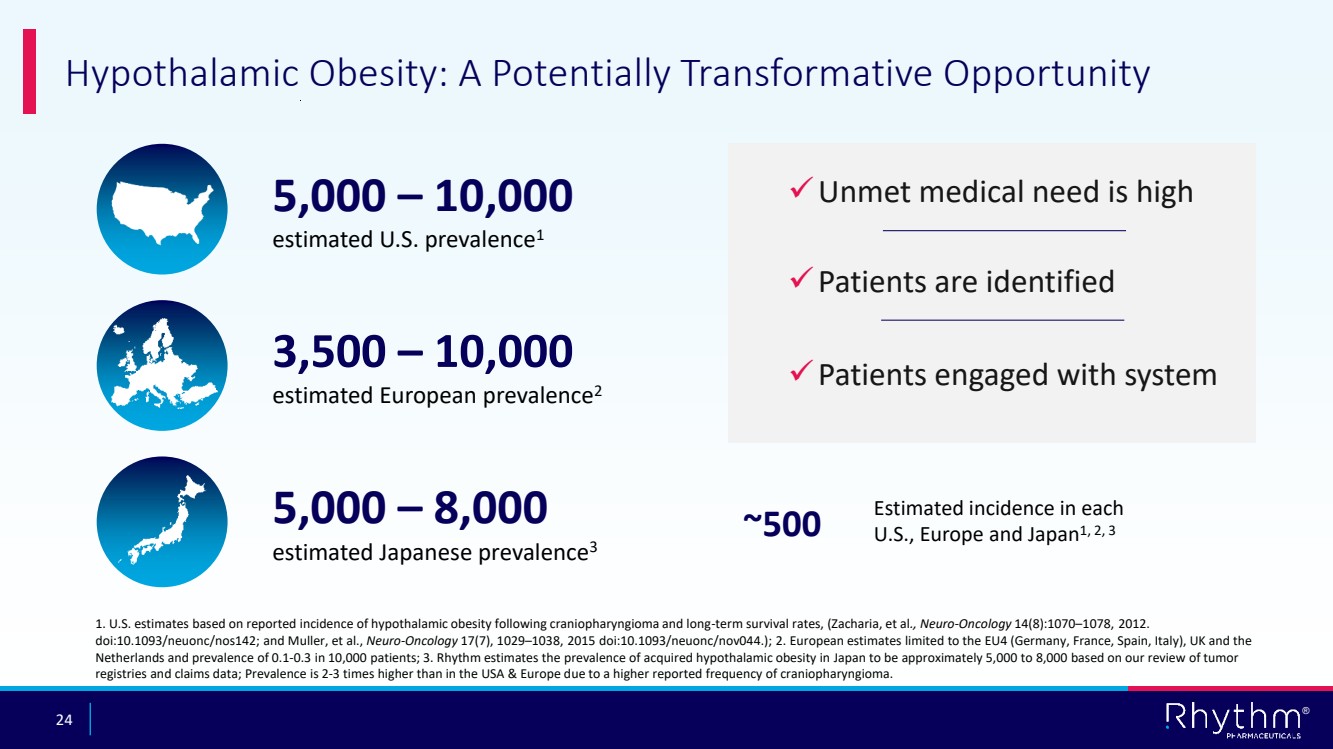
24 ® Hypothalamic Obesity: A Potentially Transformative Opportunity 1. U.S. estimates based on reported incidence of hypothalamic obesity following craniopharyngioma and long-term survival rates, (Zacharia, et al., Neuro-Oncology 14(8):1070–1078, 2012. doi:10.1093/neuonc/nos142; and Muller, et al., Neuro-Oncology 17(7), 1029–1038, 2015 doi:10.1093/neuonc/nov044.); 2. European estimates limited to the EU4 (Germany, France, Spain, Italy), UK and the Netherlands and prevalence of 0.1-0.3 in 10,000 patients; 3. Rhythm estimates the prevalence of acquired hypothalamic obesity in Japan to be approximately 5,000 to 8,000 based on our review of tumor registries and claims data; Prevalence is 2-3 times higher than in the USA & Europe due to a higher reported frequency of craniopharyngioma. 5,000 – 10,000 estimated U.S. prevalence1 3,500 – 10,000 estimated European prevalence2 5,000 – 8,000 estimated Japanese prevalence3 ✓Unmet medical need is high ✓Patients are identified ✓Patients engaged with system Estimated incidence in each U.S., Europe and Japan ~500 1, 2, 3 |
|
25 ® Focus on Global Regulatory Strategy US EU UK CANADA JAPAN Regulatory submissions in the U.S. and EU expected to be completed in Q3 2025 |
|
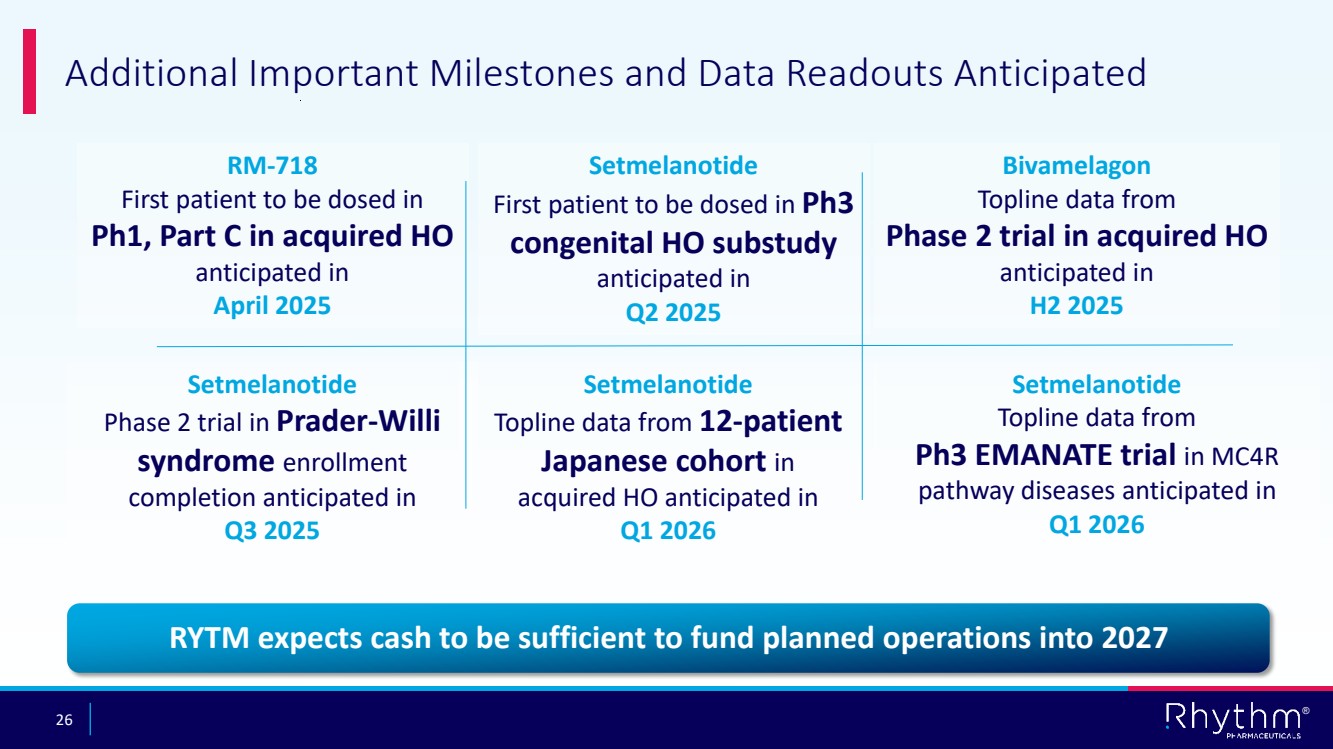
26 ® Additional Important Milestones and Data Readouts Anticipated Bivamelagon Topline data from Phase 2 trial in acquired HO anticipated in H2 2025 RM-718 First patient to be dosed in Ph1, Part C in acquired HO anticipated in April 2025 Setmelanotide Topline data from 12-patient Japanese cohort in acquired HO anticipated in Q1 2026 Setmelanotide Phase 2 trial in Prader-Willi syndrome enrollment completion anticipated in Q3 2025 Setmelanotide Topline data from Ph3 EMANATE trial in MC4R pathway diseases anticipated in Q1 2026 RYTM expects cash to be sufficient to fund planned operations into 2027 Setmelanotide First patient to be dosed in Ph3 congenital HO substudy anticipated in Q2 2025 |
|
27 ® Questions? |