UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d) of
The Securities Exchange Act of 1934
Date of Report (Date of Earliest Event Reported): April 3, 2024
Commission File No. 001-14778
Soligenix, Inc.
(Exact name of small business issuer as specified in its charter)
DELAWARE |
|
41-1505029 |
(State or other jurisdiction of |
|
(I.R.S. Employer |
|
|
|
|
29 Emmons Drive, Suite B-10 Princeton, NJ |
|
08540 |
(Address of principal executive offices) |
|
(Zip Code) |
(609) 538-8200
(Issuer’s telephone number, including area code)
Check the appropriate box below if the Form 8-K filing is intended to simultaneously satisfy the filing obligation of the registrant under any of the following provisions (see General Instruction A.2. below):
☐ Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425)
☐ Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12)
☐ Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b))
☐ Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c))
Securities registered pursuant to Section 12(b) of the Act:
Title of each class |
|
Trading Symbol(s) |
|
Name of each exchange on which registered |
Common Stock, par value $.001 per share |
|
SNGX |
|
The Nasdaq Capital Market |
Indicate by check mark whether the registrant is an emerging growth company as defined in Rule 405 of the Securities Act of 1933 (§230.405 of this chapter) or Rule 12b-2 of the Securities Exchange Act of 1934 (§240.12b-2 of this chapter).
Emerging growth company ☐
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
w
Item 8.01. Other Events.
On April 3, 2024, Soligenix, Inc. (the “Company”) issued a press release announcing the receipt of agreement from the European Medicines Agency on the key design components of a confirmatory Phase 3 placebo-controlled study evaluating the safety and efficacy of HyBryte™ (synthetic hypericin) in the treatment of cutaneous T-cell lymphoma patients with early-stage disease. This confirmatory 18-week study is expected to enroll approximately 80 patients in the United States and Europe and is targeted to begin patient enrollment by the end of 2024 with top-line results anticipated in the second half of 2026. A copy of the press release is filed as Exhibit 99.1 to this Current Report on Form 8-K and incorporated herein by reference.
The Company updated its corporate presentation (the “Presentation”) as of April 3, 2024 to incorporate information relating to the confirmatory Phase 3 placebo-controlled study evaluating the safety and efficacy of HyBryte™ in the treatment of cutaneous T-cell lymphoma patients with early-stage disease. The slides from the Presentation are attached hereto as Exhibit 99.2. The Presentation also will be posted on the Company’s website at www.soligenix.com.
Safe Harbor for Forward-Looking Statements
Certain statements contained in this report may constitute forward-looking statements within the meaning of Section 27A of the Securities Act of 1933 and Section 21E of the 1934 Act. All statements, other than statements of historical fact, are statements that could be deemed forward-looking statements, including statements containing the words “predicts,” “plans,” “expects,” “anticipates,” “believes,” “goal,” “target,” “estimate,” “potential,” “may,” “might,” “could,” “see,” “seek,” “forecast,” and similar words. Forward-looking statements are based on the Company’s current plans and expectations and involve risks and uncertainties which are, in many instances, beyond the Company’s control, and which could cause actual results to differ materially from those included in or contemplated or implied by the forward-looking statements. Such risks and uncertainties include, among others, the risks, uncertainties and factors detailed in the Company’s filings with the U.S. Securities and Exchange Commission (the “SEC”), including in the Company’s Annual Report for the year ended December 31, 2023 on Form 10-K, which was filed with the SEC. As a result of such risks, uncertainties and factors, the Company’s actual results may differ materially from any future results, performance or achievements discussed in or implied by the forward-looking statements contained herein. The Company is providing the information in this report as of the date hereof and assumes no obligations to update the information included in this report or revise any forward-looking statements, whether as a result of new information, future events or otherwise.
Item 9.01.Financial Statements and Exhibits.
(d) Exhibits.
Exhibit No. |
|
Description |
99.1 |
||
99.2 |
||
104 |
Cover Page Interactive Data File (embedded within the Inline XBRL document) |
|
|
|
|
2
SIGNATURE
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
|
Soligenix, Inc. |
|
|
|
|
April 3, 2024 |
By: |
/s/ Christopher J. Schaber |
|
|
Christopher J. Schaber, Ph.D. |
|
|
President and Chief Executive Officer |
|
|
(Principal Executive Officer) |
3
EXHIBIT 99.1

Soligenix Announces Agreement on the Design of a Second Confirmatory Placebo-Controlled Trial for HyBryte™
With the European Medicines Agency
Randomized Study with 18 Weeks Continuous Treatment Expected to Replicate and Extend Results from the First, Statistically Significant Phase 3 Study
Princeton, NJ – April 3, 2024 – Soligenix, Inc. (Nasdaq: SNGX) (Soligenix or the Company), a late-stage biopharmaceutical company focused on developing and commercializing products to treat rare diseases where there is an unmet medical need, announced today that it has received agreement from the European Medicines Agency (EMA) on the key design components of a confirmatory Phase 3 placebo-controlled study evaluating the safety and efficacy of HyBryte™ (synthetic hypericin) in the treatment of cutaneous T-cell lymphoma (CTCL) patients with early-stage disease. This confirmatory 18-week study is expected to enroll approximately 80 patients in the United States and Europe and is targeted to begin patient enrollment by the end of 2024 with top-line results anticipated in the second half of 2026.
The confirmatory study, called FLASH2 (Fluorescent Light Activated Synthetic Hypericin 2), replicates the double-blind, placebo-controlled design used in the first successful Phase 3 FLASH study that consisted of three 6-week treatment cycles (18 weeks total), with the primary efficacy assessment occurring at the end of the initial 6 week double-blind, placebo-controlled treatment cycle (Cycle 1). However, the second study extends the double-blind, placebo-controlled assessment to 18 weeks of continuous treatment (no “between-Cycle” treatment breaks) with the primary endpoint assessment occurring at the end of the 18-week timepoint. In the first Phase 3 study, a treatment response of 49% (p<0.0001 vs patients receiving placebo in Cycle 1) was observed in patients completing 18 weeks (3 cycles) of therapy. In this second study, all important clinical study design components remain the same as in the first FLASH study, including the primary endpoint and key inclusion-exclusion criteria. The extended treatment for a continuous 18 weeks in a single cycle is expected to statistically demonstrate HyBryte’s™ increased effect over a more prolonged, “real world” treatment course.
“In treating CTCL, which is a chronic cancer with no cure, long-term safety is a strong driver of treatment choice. Most current treatment options for CTCL are associated with significant safety concerns, including black-box warnings,” stated Brian Poligone, MD, PhD, Director of the Rochester Skin Lymphoma Medical Group, Fairport, NY. “Clinical studies with HyBryte™ have demonstrated strong and rapid efficacy with a very benign safety profile, with broad applicability across different lesion types, different skin tones and different disease stages.
I know I can speak for my colleagues that have been involved with these studies when I say that the data generated to date has been extremely compelling. This second study is very similar to the first FLASH study, and should build on these compelling data, while allowing us to more closely treat as we would in a ‘real world’ setting. We believe the outcome of this trial will further validate the utility of HyBryte™ in early-stage CTCL and we look forward to participating in this important study.”
“With its chronic course and major impact on patient quality of life, CTCL is an orphan disease in urgent need of additional treatment options that are well-tolerated and safe over the long term,” stated Christopher Schaber, PhD, President and Chief Executive Officer of Soligenix. “Studies to date have indicated a substantial increase in efficacy with longer treatment and similar performance against both patch and plaque lesions. These results are derived from one of the largest studies ever conducted in CTCL, and we believe this second study will both substantiate and improve upon these results. Given our extensive engagement with the CTCL community, our esteemed Medical Advisory Board and our previous trial experience with this disease, we anticipate being able to accelerate enrollment in support of this study, including the potential to enroll previously identified and treated HyBryte™ patients from the FLASH study. Discussions with the FDA on an appropriate study design remain ongoing. While collaborative, the agency has expressed a preference for a longer duration comparative study over a placebo-controlled trial. Given the shorter time to potential commercial revenue and the similar trial design to the first FLASH study afforded by the EMA accepted protocol, we will initiate that study. At the same time, we will continue discussions with the FDA on modifying the development path to adequately address their feedback.”
The confirmatory Phase 3, randomized, double-blind, placebo-controlled, multicenter study includes approximately 80 subjects with early-stage CTCL. It will evaluate the efficacy and safety of HyBryte™ topically applied to CTCL lesions twice weekly for 18 weeks, with each application followed 21 (±3) hours later by the administration of safe, visible light at a wavelength of 500 to 650 nm. The light will be administered starting at 6 J/cm2 twice weekly. This will be increased upwards by 2 J/cm2 until: 1) the patient experiences a Grade 1 erythema, 2) the patient reaches the maximum dose of 30 J/cm2, or 3) the patient cannot tolerate the treatment time, whichever comes first. All of the patient’s lesions that are readily available for exposure to the visible light source will be treated and 3 to 5 index lesions in each patient will be prospectively identified and indexed for the modified composite assessment of index lesions severity (mCAILS) evaluation prior to randomization (baseline). The primary efficacy endpoint will be assessed on the percent of patients in each of the two treatment groups (i.e., HyBryte™ and placebo) achieving a Partial or Complete Response (yes/no) of the treated lesions defined as a ≥ 50% reduction in the total mCAILS score for the 3-5 index lesions following 18 weeks of treatment compared to the total mCAILS score at baseline. Other secondary measures will assess treatment response (including duration), degree of improvement, time to relapse and safety. Following treatment, all patients will be followed every 4 weeks for a total of 12 weeks (through Week 30). The Data Monitoring Committee (DMC) will conduct one (1) interim analysis when approximately 60% of the total subjects have completed the primary endpoint evaluation. The primary efficacy endpoint and the key safety endpoints will be analyzed. A sample size recalculation may be performed after examining the assumptions or the trial halted for either futility, safety concerns, or overwhelming efficacy. Soligenix, participating clinical investigators, and any personnel involved in trial conduct will remain blinded to study treatment until completion of the trial.
2
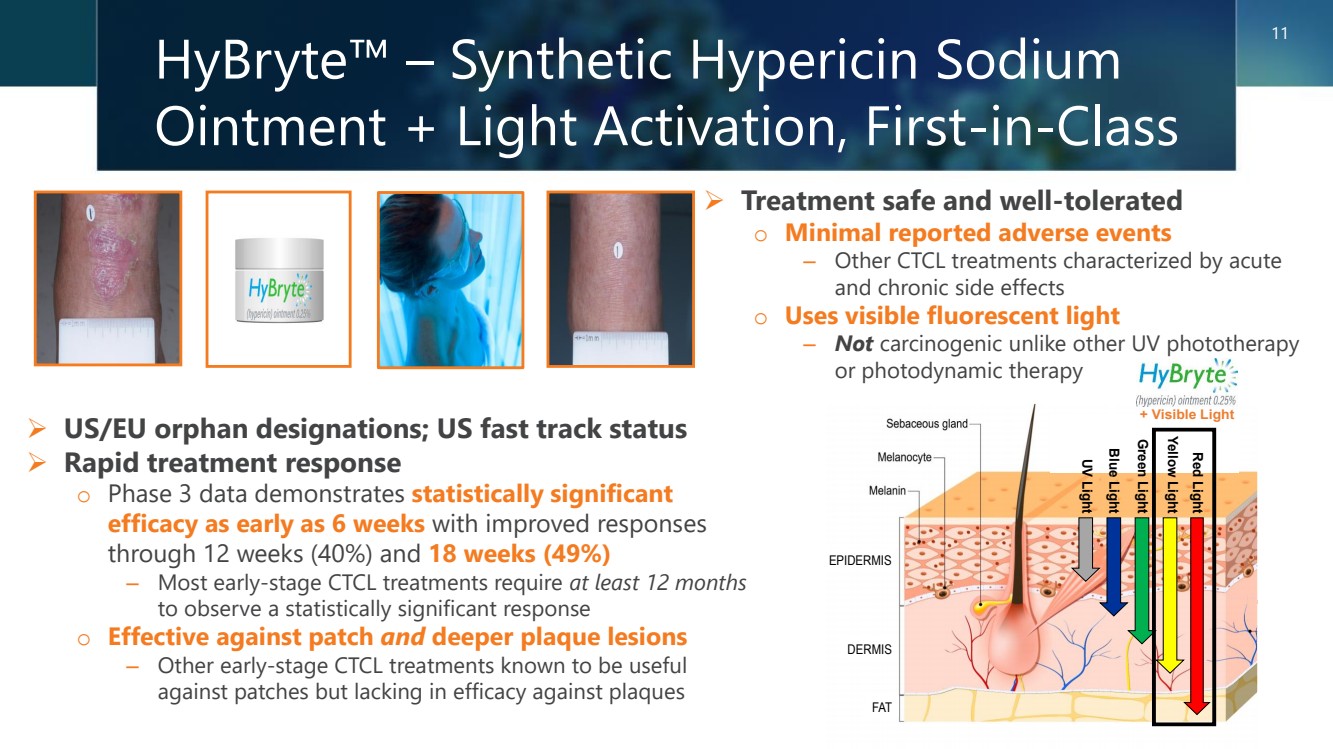
About HyBryte™
HyBryte™ (research name SGX301) is a novel, first-in-class, photodynamic therapy utilizing safe, visible light for activation. The active ingredient in HyBryte™ is synthetic hypericin, a potent photosensitizer that is topically applied to skin lesions that is taken up by the malignant T-cells, and then activated by safe, visible light approximately 24 hours later. The use of visible light in the red-yellow spectrum has the advantage of penetrating more deeply into the skin (much more so than ultraviolet light) and therefore potentially treating deeper skin disease and thicker plaques and lesions. This treatment approach avoids the risk of secondary malignancies (including melanoma) inherent with the frequently employed DNA-damaging drugs and other phototherapy that are dependent on ultraviolet exposure. Combined with photoactivation, hypericin has demonstrated significant anti-proliferative effects on activated normal human lymphoid cells and inhibited growth of malignant T-cells isolated from CTCL patients. In a published Phase 2 clinical study in CTCL, patients experienced a statistically significant (p=0.04) improvement with topical hypericin treatment whereas the placebo was ineffective. HyBryte™ has received orphan drug and fast track designations from the FDA, as well as orphan designation from the EMA.
The published Phase 3 FLASH trial enrolled a total of 169 patients (166 evaluable) with Stage IA, IB or IIA CTCL. The trial consisted of three treatment cycles. Treatments were administered twice weekly for the first 6 weeks and treatment response was determined at the end of the 8th week of each cycle. In the first double-blind treatment cycle (Cycle 1), 116 patients received HyBryte™ treatment (0.25% synthetic hypericin) and 50 received placebo treatment of their index lesions. A total of 16% of the patients receiving HyBryte™ achieved at least a 50% reduction in their lesions (graded using a standard measurement of dermatologic lesions, the CAILS score) compared to only 4% of patients in the placebo group at 8 weeks (p=0.04) during the first treatment cycle (primary endpoint). HyBryte™ treatment in this cycle was safe and well tolerated.
In the second open-label treatment cycle (Cycle 2), all patients received HyBryte™ treatment of their index lesions. Evaluation of 155 patients in this cycle (110 receiving 12 weeks of HyBryte™ treatment and 45 receiving 6 weeks of placebo treatment followed by 6 weeks of HyBryte™ treatment), demonstrated that the response rate among the 12-week treatment group was 40% (p<0.0001 vs the placebo treatment rate in Cycle 1). Comparison of the 12-week and 6-week treatment groups also revealed a statistically significant improvement (p<0.0001) between the two groups, indicating that continued treatment results in better outcomes. HyBryte™ continued to be safe and well tolerated. Additional analyses also indicated that HyBryte™ is equally effective in treating both plaque (response 42%, p<0.0001 relative to placebo treatment in Cycle 1) and patch (response 37%, p=0.0009 relative to placebo treatment in Cycle 1) lesions of CTCL, a particularly relevant finding given the historical difficulty in treating plaque lesions in particular.
The third (optional) treatment cycle (Cycle 3) was focused on safety and all patients could elect to receive HyBryte™ treatment of all their lesions. Of note, 66% of patients elected to continue with this optional compassionate use / safety cycle of the study. Of the subset of patients that received HyBryte™ throughout all 3 cycles of treatment, 49% of them demonstrated a positive treatment response (p<0.0001 vs patients receiving placebo in Cycle 1). Moreover, in a subset of patients evaluated in this cycle, it was demonstrated that HyBryte™ is not systemically available, consistent with the general safety of this topical product observed to date.
3
At the end of Cycle 3, HyBryte™ continued to be well tolerated despite extended and increased use of the product to treat multiple lesions.
Overall safety of HyBryte™ is a critical attribute of this treatment and was monitored throughout the three treatment cycles (Cycles 1, 2 and 3) and the 6-month follow-up period. HyBryte’s™ mechanism of action is not associated with DNA damage, making it a safer alternative than currently available therapies, all of which are associated with significant and sometimes fatal, side effects. Predominantly these include the risk of melanoma and other malignancies, as well as the risk of significant skin damage and premature skin aging. Currently available treatments are only approved in the context of previous treatment failure with other modalities and there is no approved front-line therapy available. Within this landscape, treatment of CTCL is strongly motivated by the safety risk of each product. HyBryte™ potentially represents the safest available efficacious treatment for CTCL. With very limited systemic absorption, a compound that is not mutagenic and a light source that is not carcinogenic, there is no evidence to date of any potential safety issues.
The Phase 3 FLASH study was partially funded by the National Cancer Institute via a Phase II SBIR grant (#1R44CA210848-01A1) awarded to Soligenix, Inc. In addition, the FDA awarded an Orphan Products Development grant to support the evaluation of HyBryte™ for expanded treatment in patients with early-stage CTCL, including in the home use setting. The grant, totaling $2.6 million over 4 years, was awarded to the University of Pennsylvania that was a leading enroller in the Phase 3 FLASH study.
About Cutaneous T-Cell Lymphoma (CTCL)
CTCL is a class of non-Hodgkin’s lymphoma (NHL), a type of cancer of the white blood cells that are an integral part of the immune system. Unlike most NHLs which generally involve B-cell lymphocytes (involved in producing antibodies), CTCL is caused by an expansion of malignant T-cell lymphocytes (involved in cell-mediated immunity) normally programmed to migrate to the skin. These malignant cells migrate to the skin where they form various lesions, typically beginning as patches and may progress to raised plaques and tumors. Mortality is related to the stage of CTCL, with median survival generally ranging from about 12 years in the early stages to only 2.5 years when the disease has advanced. There is currently no cure for CTCL. Typically, CTCL lesions are treated and regress but usually return either in the same part of the body or in new areas.
CTCL constitutes a rare group of NHLs, occurring in about 4% of the more than 1.2 million individuals living with the disease. It is estimated, based upon review of historic published studies and reports and an interpolation of data on the incidence of CTCL that it affects approximately 30,000 individuals in the U.S. (based on SEER data, with approximately 3,200 new cases seen annually) and over 20,000 individuals in Europe (based on 5-year prevalence data, with approximately 5,600 new cases annually).
4
About Soligenix, Inc.
Soligenix is a late-stage biopharmaceutical company focused on developing and commercializing products to treat rare diseases where there is an unmet medical need. Our Specialized BioTherapeutics business segment is developing and moving toward potential commercialization of HyBryte™ (SGX301 or synthetic hypericin sodium) as a novel photodynamic therapy utilizing safe visible light for the treatment of cutaneous T-cell lymphoma (CTCL). With successful completion of the second Phase 3 study, regulatory approvals will be sought to support potential commercialization worldwide. Development programs in this business segment also include expansion of synthetic hypericin (SGX302) into psoriasis, our first-in-class innate defense regulator (IDR) technology, dusquetide (SGX942) for the treatment of inflammatory diseases, including oral mucositis in head and neck cancer, and (SGX945) in Behçet’s Disease.
Our Public Health Solutions business segment includes development programs for RiVax®, our ricin toxin vaccine candidate, as well as our vaccine programs targeting filoviruses (such as Marburg and Ebola) and CiVax™, our vaccine candidate for the prevention of COVID-19 (caused by SARS-CoV-2). The development of our vaccine programs incorporates the use of our proprietary heat stabilization platform technology, known as ThermoVax®. To date, this business segment has been supported with government grant and contract funding from the National Institute of Allergy and Infectious Diseases (NIAID), the Defense Threat Reduction Agency (DTRA) and the Biomedical Advanced Research and Development Authority (BARDA).
For further information regarding Soligenix, Inc., please visit the Company’s website at https://www.soligenix.com and follow us on LinkedIn and Twitter at @Soligenix_Inc.
This press release may contain forward-looking statements that reflect Soligenix, Inc.’s current expectations about its future results, performance, prospects and opportunities, including but not limited to, potential market sizes, patient populations and clinical trial enrollment. Statements that are not historical facts, such as “anticipates,” “estimates,” “believes,” “hopes,” “intends,” “plans,” “expects,” “goal,” “may,” “suggest,” “will,” “potential,” or similar expressions, are forward-looking statements. These statements are subject to a number of risks, uncertainties and other factors that could cause actual events or results in future periods to differ materially from what is expressed in, or implied by, these statements, and include the expected amount and use of proceeds from the offering and the expected closing date of the offering. Soligenix cannot assure you that it will be able to successfully develop, achieve regulatory approval for or commercialize products based on its technologies, particularly in light of the significant uncertainty inherent in developing therapeutics and vaccines against bioterror threats, conducting preclinical and clinical trials of therapeutics and vaccines, obtaining regulatory approvals and manufacturing therapeutics and vaccines, that product development and commercialization efforts will not be reduced or discontinued due to difficulties or delays in clinical trials or due to lack of progress or positive results from research and development efforts, that it will be able to successfully obtain any further funding to support product development and commercialization efforts, including grants and awards, maintain its existing grants which are subject to performance requirements, enter into any biodefense procurement contracts with the U.S. Government or other countries, that it will be able to compete with larger and better financed competitors in the biotechnology industry, that changes in health care practice, third party reimbursement limitations and Federal and/or state health care reform initiatives will not negatively affect its business, or that the U.S. Congress may not pass any legislation that would provide additional funding for the Project BioShield program. In addition, there can be no assurance as to the timing or success of any of its clinical/preclinical trials. Despite the statistically significant result achieved in the first HyBryte™ (SGX301) Phase 3 clinical trial for the treatment of cutaneous T-cell lymphoma, there can be no assurance that the second HyBryte™ (SGX301) Phase 3 clinical trial will be successful or that a marketing authorization from the FDA or EMA will be granted. Additionally, although the EMA has agreed to the key design components of the second HyBryte™ (SGX301) Phase 3 clinical trial, no assurance can be given that the Company will be able to modify the development path to adequately address the FDA’s concerns or that the FDA will not require a longer duration comparative study. Notwithstanding the result in the first HyBryte™ (SGX301) Phase 3 clinical trial for the treatment of cutaneous T-cell lymphoma and the Phase 2a clinical trial of SGX302 for the treatment of psoriasis, there can be no assurance as to the timing or success of the clinical trials of SGX302 for the treatment of psoriasis.
5
Despite the positive efficacy results demonstrated in the Phase 2 and 3 clinical studies of SGX942 for the treatment of oral mucositis due to chemoradiation therapy for head and neck cancer, there can be no assurance as to the timing or success of the clinical trials of SGX945 for the treatment of Behçet’s Disease. Further, there can be no assurance that RiVax® will qualify for a biodefense Priority Review Voucher (PRV) or that the prior sales of PRVs will be indicative of any potential sales price for a PRV for RiVax®. Also, no assurance can be provided that the Company will receive or continue to receive non-dilutive government funding from grants and contracts that have been or may be awarded or for which the Company will apply in the future. These and other risk factors are described from time to time in filings with the Securities and Exchange Commission (the “SEC”), including, but not limited to, the Company’s preliminary prospectus (Registration No. 333-271049) filed with the SEC on May 4, 2023, and Soligenix’s reports on Forms 10-Q and 10-K. Unless required by law, Soligenix assumes no obligation to update or revise any forward-looking statements as a result of new information or future events.
Company Contact:
Jonathan Guarino, CPA, CGMA
Senior Vice President and Chief Financial Officer
(609) 538-8200 | www.soligenix.com
Soligenix, Inc.
29 Emmons Drive, Suite B-10
Princeton, NJ 08540
# # #
6
|
Rising to the Challenges of Rare Disease Treatment NASDAQ: SNGX April 03, 2024 |
|
Forward-Looking Statements This presentation contains forward-looking statements. All statements other than statements of historical facts contained in this presentation, including statements regarding our future results of operations and financial position, business strategy, prospective products and product candidates and their development, regulatory approvals, ability to commercialize our products and product candidates and attract collaborators, reimbursement for our product candidates, research and development costs, timing and likelihood of success, plans and objectives of management for future operations, our ability to obtain and maintain intellectual property protection for our product candidates and their development, competing therapies, and future results of current and anticipated products and product candidates, are forward-looking statements. These statements involve known and unknown risks and uncertainties, such as experienced with the COVID-19 outbreak, and other important factors that may cause our actual results, performance or achievements to be materially different from any future results, performance or achievements expressed or implied by the forward-looking statements, many of which are disclosed in detail in our reports and other documents filed with the Securities and Exchange Commission. Because forward-looking statements are inherently subject to risks and uncertainties, some of which cannot be predicted or quantified and some of which are beyond our control, you should not rely on these forward-looking statements as predictions of future events. The events and circumstances reflected in our forward-looking statements may not be achieved or occur and actual results could differ materially from those projected in the forward-looking statements. Except as required by applicable law, we do not plan to publicly update or revise any forward-looking statements contained herein, whether as a result of any new information, future events, changed circumstances, or otherwise. Certain information contained in this presentation and statements made orally during this presentation relate to or are based on studies, publications, surveys and other data obtained from third-party sources. In addition, no independent source has evaluated the reasonableness or accuracy of Soligenix, Inc. internal estimates and no reliance should be made on any information or statements made in this presentation relating to or based on such internal estimates. 2 |
|
Company Description Soligenix, Inc. is a late-stage biopharmaceutical company focused on developing and commercializing products to treat rare diseases where there is an unmet medical need Two areas of focus: ➢ A Specialized BioTherapeutics segment dedicated to the development of products for orphan diseases and areas of unmet medical need in oncology and inflammation ➢ A Public Health Solutions segment that develops vaccines and therapeutics for military and civilian applications in the areas of ricin exposure, emerging and antibiotic resistant infectious disease, and viral disease including Ebola, Marburg and COVID-19 3 |
|
Investment Highlights ➢ Robust pipeline consisting of multiple fast track and/or orphan designated products, with potential for significant commercial returns of ~$2B in global annual sales ➢ Late clinical-stage assets, one with successful Phase 3 data readout o Cutaneous T-cell lymphoma (HyBryte™ or SGX301) – Positive statistically significant results achieved in first Phase 3 study; published JAMA Dermatology – Second confirmatory Phase 3 study of similar design accepted by EMA; FDA discussions remain ongoing – Confirmatory Phase 3 double-blind, placebo-controlled study in ~80 patients to initiate in 2H 2024 – Significant commercial opportunity in area of unmet medical need; estimated global market potential >$250M o Psoriasis (SGX302) – Positive and statistically significant results achieved in Phase 1/2 proof of concept (POC) study – Phase 2a study in mild-to-moderate psoriasis ongoing; clinical success achieved in 2 of 4 Cohort 2 patients – Significant commercial opportunity in area of unmet medical need; estimated global market potential >$1B o Behçet's disease (SGX945) – Phase 2a study in aphthous ulcers in Behçet's Disease; FDA IND & protocol cleared, fast track designation received – Significant commercial opportunity in area of unmet medical need; estimated global market potential >$200M ➢ Collaborations with biotech, academia and government agencies ➢ Non-dilutive government funding helps cover operating expenses o NIH grant awards supporting vaccine development; potential for up to 3 Priority Review Vouchers (PRVs) ➢ Experienced management team and renowned advisors with record of success 4 |
|
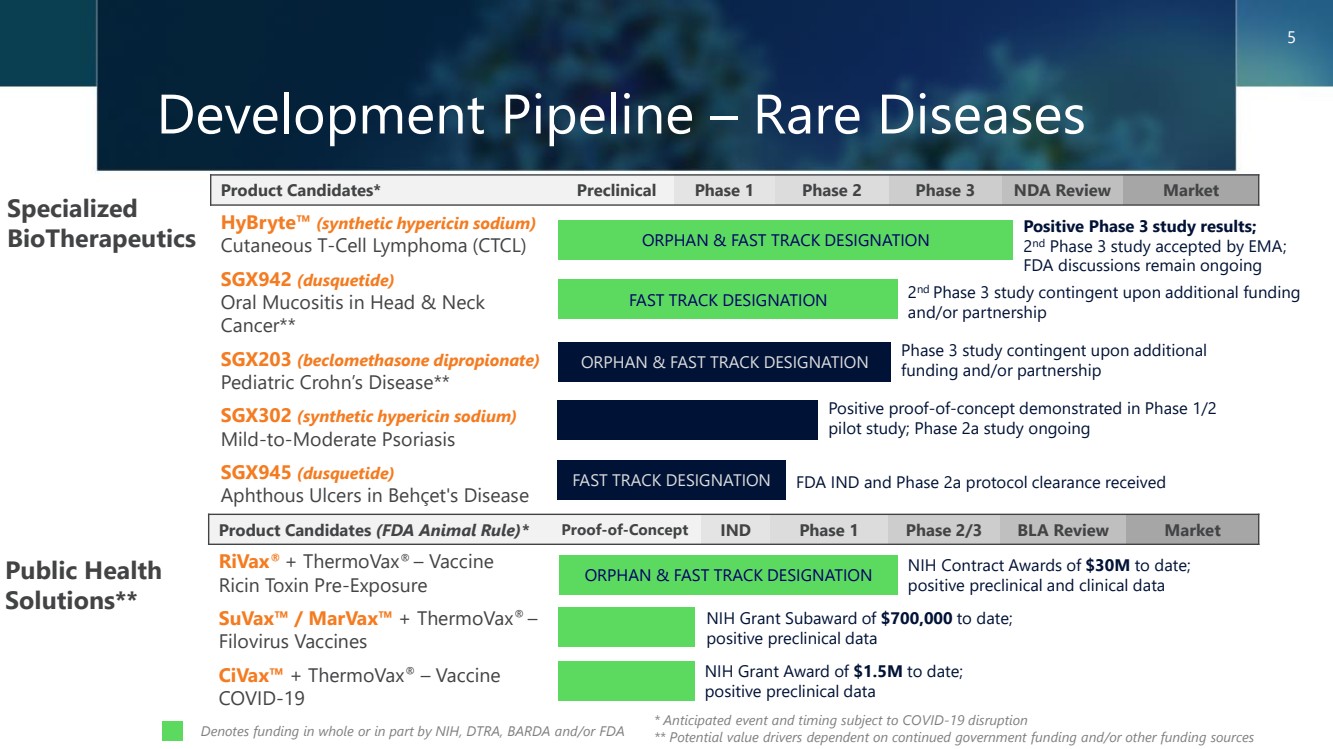
Development Pipeline – Rare Diseases Product Candidates* Preclinical Phase 1 Phase 2 Phase 3 NDA Review Market HyBryte™ (synthetic hypericin sodium) Cutaneous T-Cell Lymphoma (CTCL) SGX942 (dusquetide) Oral Mucositis in Head & Neck Cancer** SGX203 (beclomethasone dipropionate) Pediatric Crohn’s Disease** SGX302 (synthetic hypericin sodium) Mild-to-Moderate Psoriasis SGX945 (dusquetide) Aphthous Ulcers in Behçet's Disease Specialized BioTherapeutics Public Health Solutions** Product Candidates (FDA Animal Rule)* Proof-of-Concept IND Phase 1 Phase 2/3 BLA Review Market RiVax® + ThermoVax® – Vaccine Ricin Toxin Pre-Exposure SuVax™ / MarVax™ + ThermoVax® – Filovirus Vaccines CiVax™ + ThermoVax® – Vaccine COVID-19 2 nd Phase 3 study contingent upon additional funding and/or partnership * Anticipated event and timing subject to COVID-19 disruption ** Potential value drivers dependent on continued government funding and/or other funding sources Phase 3 study contingent upon additional funding and/or partnership Positive proof-of-concept demonstrated in Phase 1/2 pilot study; Phase 2a study ongoing NIH Contract Awards of $30M to date; positive preclinical and clinical data Positive Phase 3 study results; 2 nd Phase 3 study accepted by EMA; FDA discussions remain ongoing Denotes funding in whole or in part by NIH, DTRA, BARDA and/or FDA ORPHAN & FAST TRACK DESIGNATION FAST TRACK DESIGNATION ORPHAN & FAST TRACK DESIGNATION ORPHAN & FAST TRACK DESIGNATION 5 NIH Grant Award of $1.5M to date; positive preclinical data NIH Grant Subaward of $700,000 to date; positive preclinical data FAST TRACK DESIGNATION FDA IND and Phase 2a protocol clearance received |
|
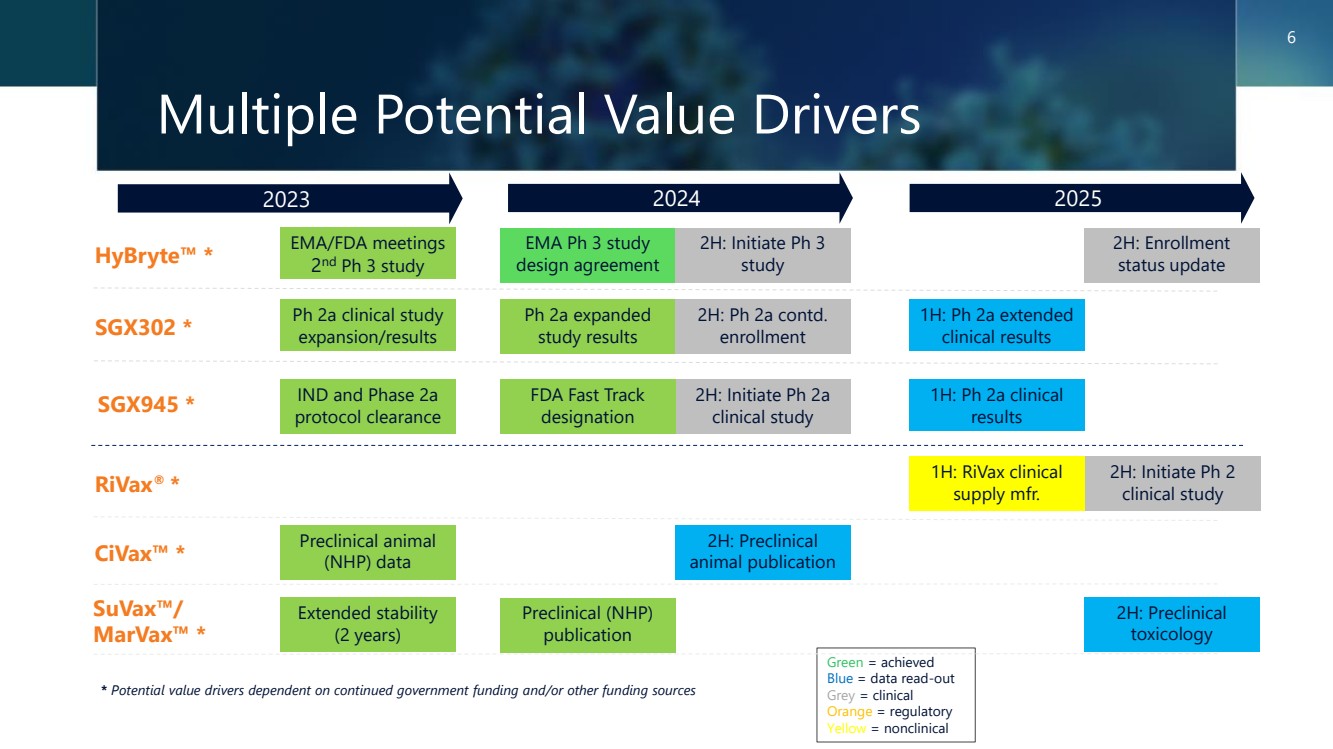
Multiple Potential Value Drivers 2023 2024 2025 * Potential value drivers dependent on continued government funding and/or other funding sources Green = achieved Blue = data read-out Grey = clinical Orange = regulatory Yellow = nonclinical 6 HyBryte™ * RiVax® * CiVax™ * SuVax™/ MarVax™ * SGX302 * Ph 2a clinical study expansion/results Preclinical (NHP) publication Preclinical animal (NHP) data EMA/FDA meetings 2 nd Ph 3 study SGX945 * IND and Phase 2a protocol clearance Extended stability (2 years) EMA Ph 3 study design agreement 2H: Initiate Ph 3 study 2H: Enrollment status update Ph 2a expanded study results 2H: Ph 2a contd. enrollment 1H: Ph 2a extended clinical results 2H: Initiate Ph 2a clinical study 1H: Ph 2a clinical results 1H: RiVax clinical supply mfr. 2H: Initiate Ph 2 clinical study 2H: Preclinical animal publication 2H: Preclinical toxicology FDA Fast Track designation |
|
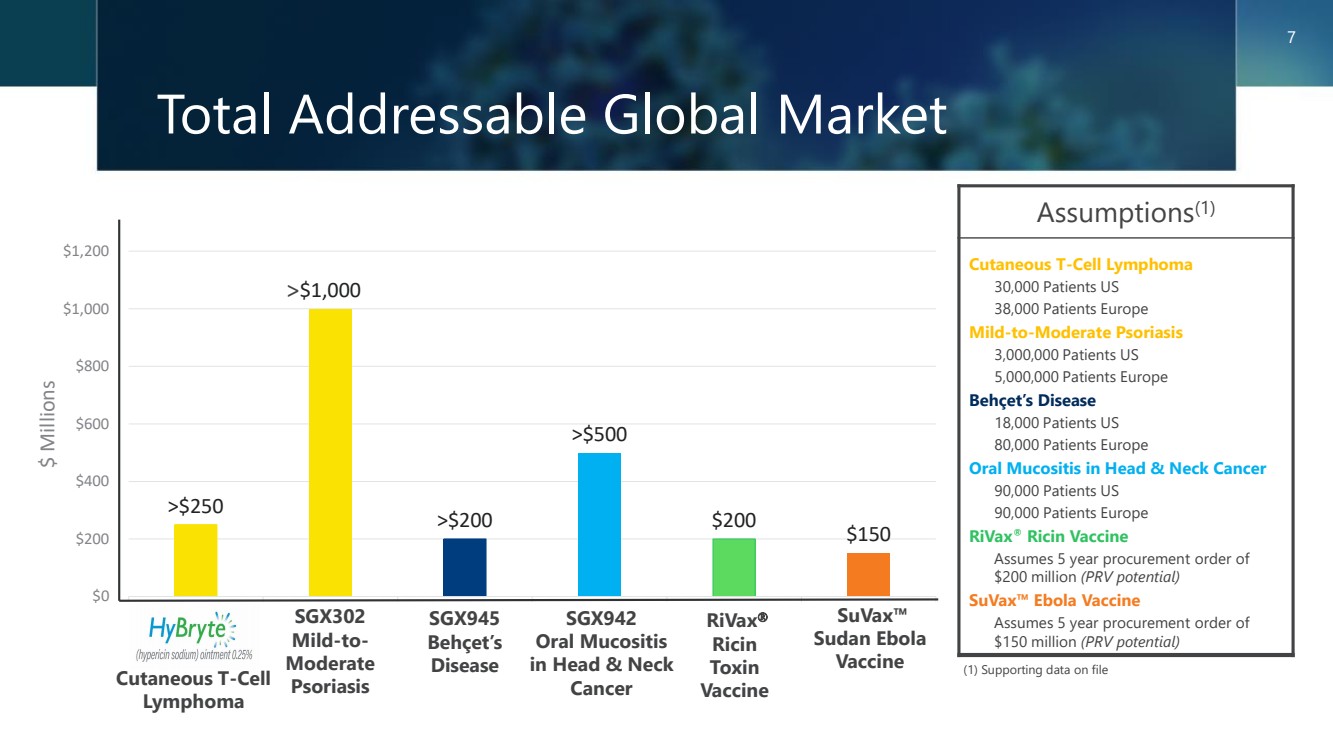
>$250 $1,000 >$200 >$500 $200 $150 $0 $200 $400 $600 $800 $1,000 $1,200 $ Millions Total Addressable Global Market Assumptions(1) Cutaneous T-Cell Lymphoma 30,000 Patients US 38,000 Patients Europe Mild-to-Moderate Psoriasis 3,000,000 Patients US 5,000,000 Patients Europe Behçet’s Disease 18,000 Patients US 80,000 Patients Europe Oral Mucositis in Head & Neck Cancer 90,000 Patients US 90,000 Patients Europe RiVax® Ricin Vaccine Assumes 5 year procurement order of $200 million (PRV potential) SuVax™ Ebola Vaccine Assumes 5 year procurement order of $150 million (PRV potential) (1) Supporting data on file SGX302 Mild-to-Moderate Psoriasis RiVax Ricin Toxin Vaccine 7 SGX942 Oral Mucositis in Head & Neck Cancer > SuVax™ Sudan Ebola Vaccine Cutaneous T-Cell Lymphoma SGX945 Behçet’s Disease |
|
Specialized BioTherapeutics Targeted Approach to Treating Oncology & Inflammation 8 |
|
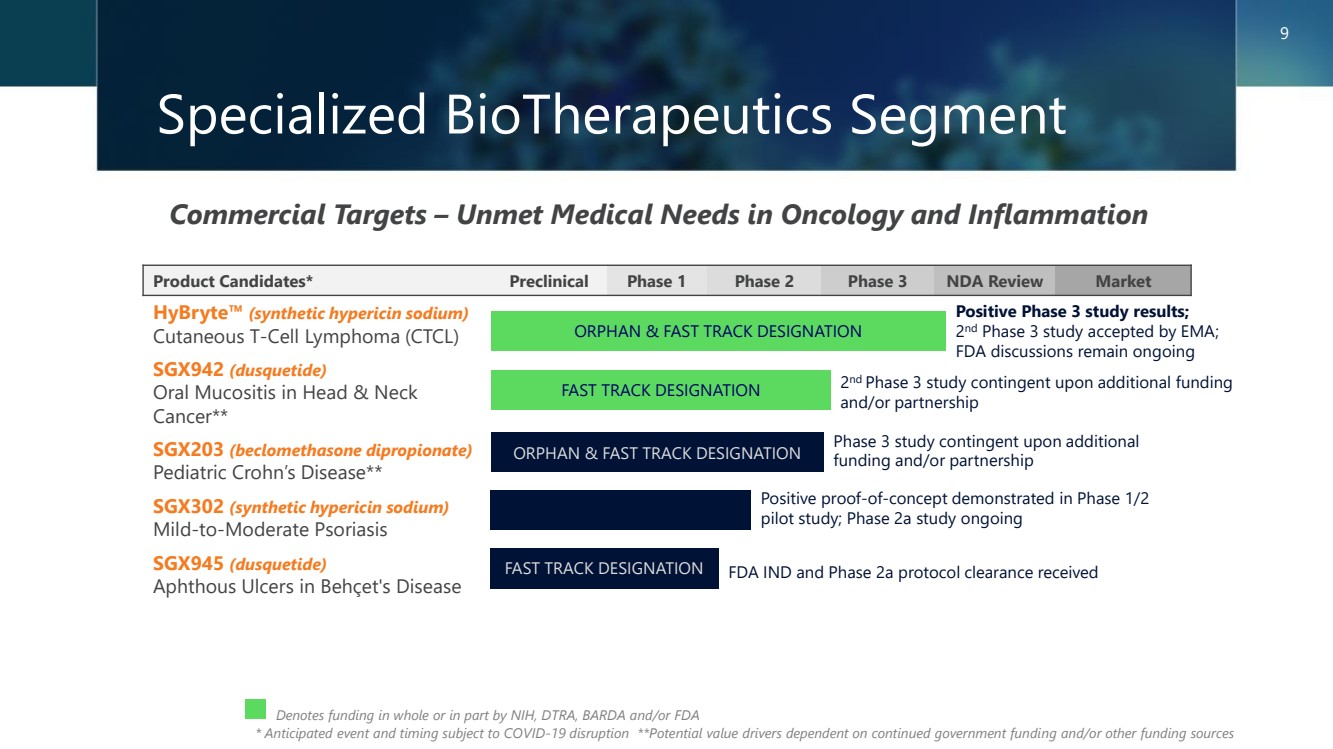
Specialized BioTherapeutics Segment 9 Commercial Targets – Unmet Medical Needs in Oncology and Inflammation * Anticipated event and timing subject to COVID-19 disruption **Potential value drivers dependent on continued government funding and/or other funding sources Denotes funding in whole or in part by NIH, DTRA, BARDA and/or FDA Product Candidates* Preclinical Phase 1 Phase 2 Phase 3 NDA Review Market HyBryte™ (synthetic hypericin sodium) Cutaneous T-Cell Lymphoma (CTCL) SGX942 (dusquetide) Oral Mucositis in Head & Neck Cancer** SGX203 (beclomethasone dipropionate) Pediatric Crohn’s Disease** SGX302 (synthetic hypericin sodium) Mild-to-Moderate Psoriasis SGX945 (dusquetide) Aphthous Ulcers in Behçet's Disease 2 nd Phase 3 study contingent upon additional funding and/or partnership Phase 3 study contingent upon additional funding and/or partnership Positive proof-of-concept demonstrated in Phase 1/2 pilot study; Phase 2a study ongoing ORPHAN & FAST TRACK DESIGNATION FAST TRACK DESIGNATION ORPHAN & FAST TRACK DESIGNATION FAST TRACK DESIGNATION FDA IND and Phase 2a protocol clearance received Positive Phase 3 study results; 2 nd Phase 3 study accepted by EMA; FDA discussions remain ongoing |
|
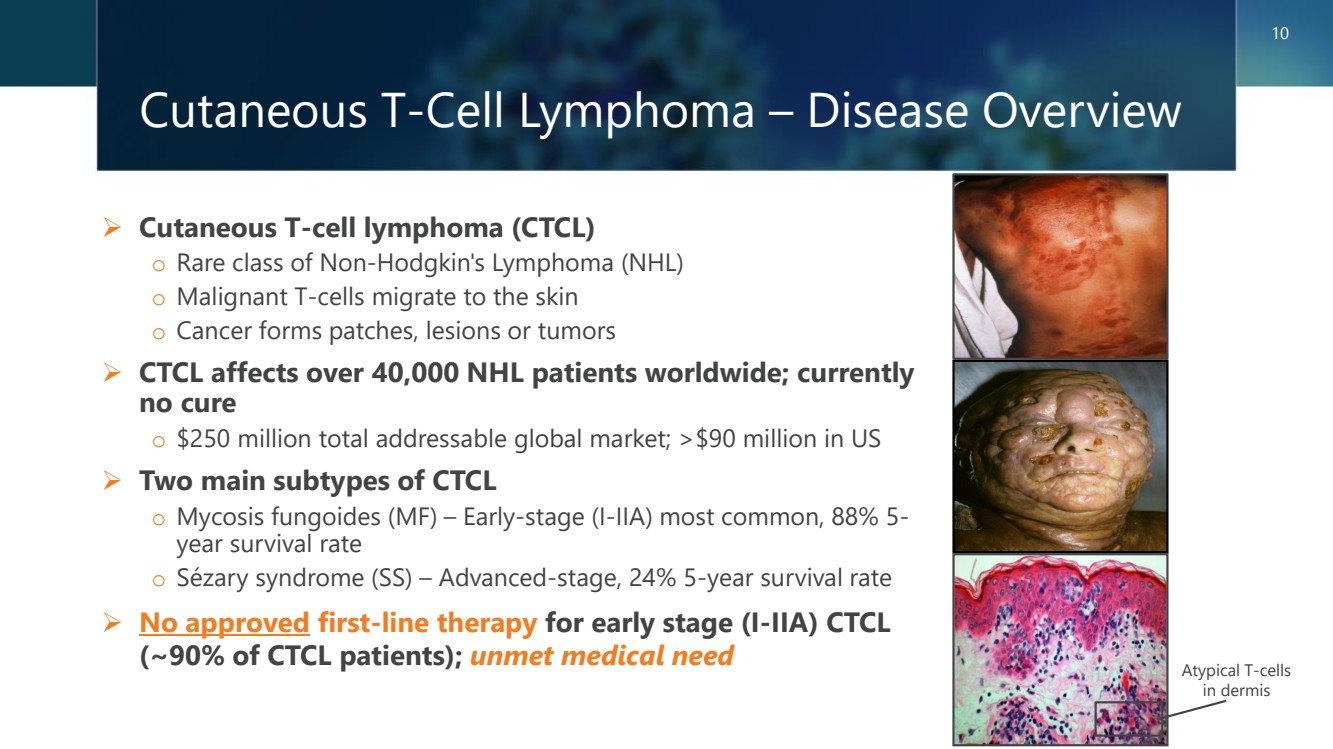
Cutaneous T-Cell Lymphoma – Disease Overview ➢ Cutaneous T-cell lymphoma (CTCL) o Rare class of Non-Hodgkin's Lymphoma (NHL) o Malignant T-cells migrate to the skin o Cancer forms patches, lesions or tumors ➢ CTCL affects over 40,000 NHL patients worldwide; currently no cure o $250 million total addressable global market; >$90 million in US ➢ Two main subtypes of CTCL o Mycosis fungoides (MF) – Early-stage (I-IIA) most common, 88% 5- year survival rate o Sézary syndrome (SS) – Advanced-stage, 24% 5-year survival rate ➢ No approved first-line therapy for early stage (I-IIA) CTCL (~90% of CTCL patients); unmet medical need 10 Atypical T-cells in dermis |
|
HyBryte™ – Synthetic Hypericin Sodium Ointment + Light Activation, First-in-Class ➢ Treatment safe and well-tolerated o Minimal reported adverse events ‒ Other CTCL treatments characterized by acute and chronic side effects o Uses visible fluorescent light ‒ Not carcinogenic unlike other UV phototherapy or photodynamic therapy 11 ➢ US/EU orphan designations; US fast track status ➢ Rapid treatment response o Phase 3 data demonstrates statistically significant efficacy as early as 6 weeks with improved responses through 12 weeks (40%) and 18 weeks (49%) ‒ Most early-stage CTCL treatments require at least 12 months to observe a statistically significant response o Effective against patch and deeper plaque lesions ‒ Other early-stage CTCL treatments known to be useful against patches but lacking in efficacy against plaques EPIDERMIS DERMIS FAT UV Light Blue Light Green Light Yellow Light Red Light + Visible Light |
|
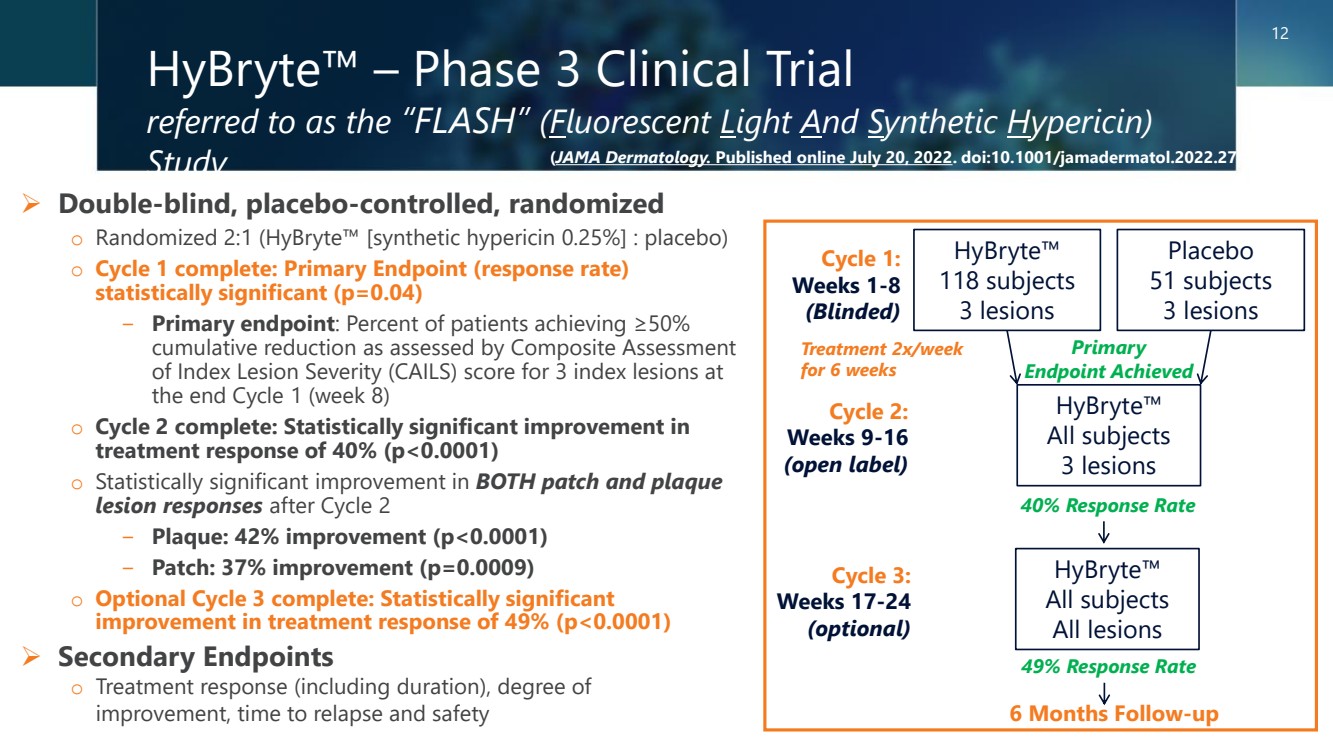
HyBryte™ – Phase 3 Clinical Trial referred to as the “FLASH” (Fluorescent Light And Synthetic Hypericin) Study ➢ Double-blind, placebo-controlled, randomized o Randomized 2:1 (HyBryte™ [synthetic hypericin 0.25%] : placebo) ➢ Secondary Endpoints o Treatment response (including duration), degree of improvement, time to relapse and safety HyBryte™ 118 subjects 3 lesions Placebo 51 subjects 3 lesions HyBryte™ All subjects 3 lesions HyBryte™ All subjects All lesions Cycle 1: Weeks 1-8 Cycle 2: Weeks 9-16 Cycle 3: Weeks 17-24 (optional) Primary Endpoint Achieved 6 Months Follow-up o Cycle 1 complete: Primary Endpoint (response rate) statistically significant (p=0.04) − Primary endpoint: Percent of patients achieving ≥50% cumulative reduction as assessed by Composite Assessment of Index Lesion Severity (CAILS) score for 3 index lesions at the end Cycle 1 (week 8) o Cycle 2 complete: Statistically significant improvement in treatment response of 40% (p<0.0001) o Statistically significant improvement in BOTH patch and plaque lesion responses after Cycle 2 − Plaque: 42% improvement (p<0.0001) − Patch: 37% improvement (p=0.0009) o Optional Cycle 3 complete: Statistically significant improvement in treatment response of 49% (p<0.0001) 12 49% Response Rate 40% Response Rate Treatment 2x/week for 6 weeks (JAMA Dermatology. Published online July 20, 2022. doi:10.1001/jamadermatol.2022.2749) (open label) (Blinded) |
|
HyBryte™ – Development Status ➢ Positive Phase 3 FLASH study successfully completed in 2020 o Largest double-blind, randomized, placebo-controlled clinical trial ever conducted in CTCL o FDA and EMA require a second confirmatory Phase 3 clinical trial ➢ Second confirmatory Phase 3 study (FLASH2) of similar design but with 18 week double-blind, placebo-controlled treatment duration compared to only 6 weeks in first FLASH study; agreed with EMA o Study to enroll ~80 patients in both the US and Europe o Key criteria: inclusion/exclusion and primary endpoint same ➢ FLASH2 study to be initiated in 2H2024 o Enrollment anticipated to require ~18 months o Enrollment of patients previously treated in first FLASH study acceptable ➢ FLASH and FLASH2 trials to support potential marketing approvals worldwide 13 |
|
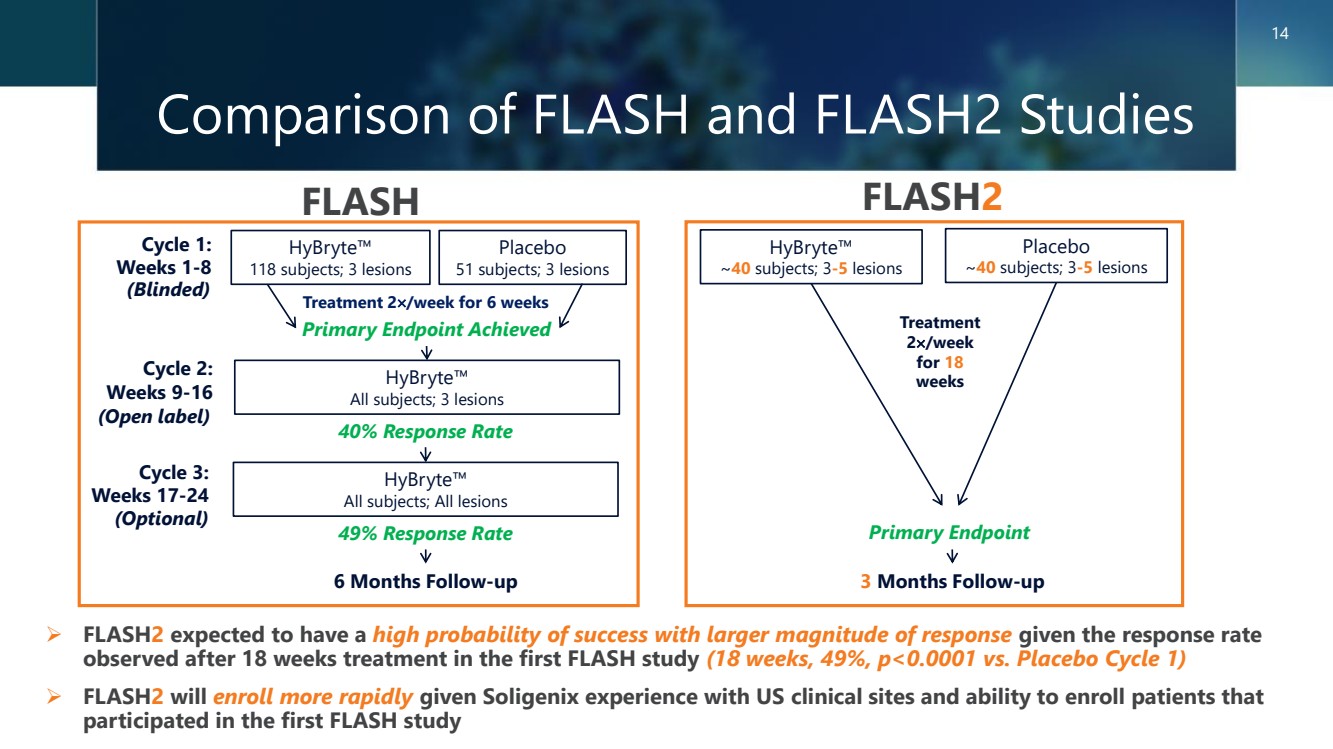
Comparison of FLASH and FLASH2 Studies 14 FLASH FLASH2 ➢ FLASH2 expected to have a high probability of success with larger magnitude of response given the response rate observed after 18 weeks treatment in the first FLASH study (18 weeks, 49%, p<0.0001 vs. Placebo Cycle 1) ➢ FLASH2 will enroll more rapidly given Soligenix experience with US clinical sites and ability to enroll patients that participated in the first FLASH study HyBryte™ 118 subjects; 3 lesions Placebo 51 subjects; 3 lesions HyBryte™ All subjects; 3 lesions HyBryte™ All subjects; All lesions Cycle 1: Weeks 1-8 Cycle 2: Weeks 9-16 Cycle 3: Weeks 17-24 (Optional) Primary Endpoint Achieved 6 Months Follow-up 49% Response Rate 40% Response Rate Treatment 2/week for 6 weeks HyBryte™ ~40 subjects; 3-5 lesions Placebo ~40 subjects; 3-5 lesions Treatment 2/week for 18 weeks 3 Months Follow-up Primary Endpoint (Open label) (Blinded) |
|
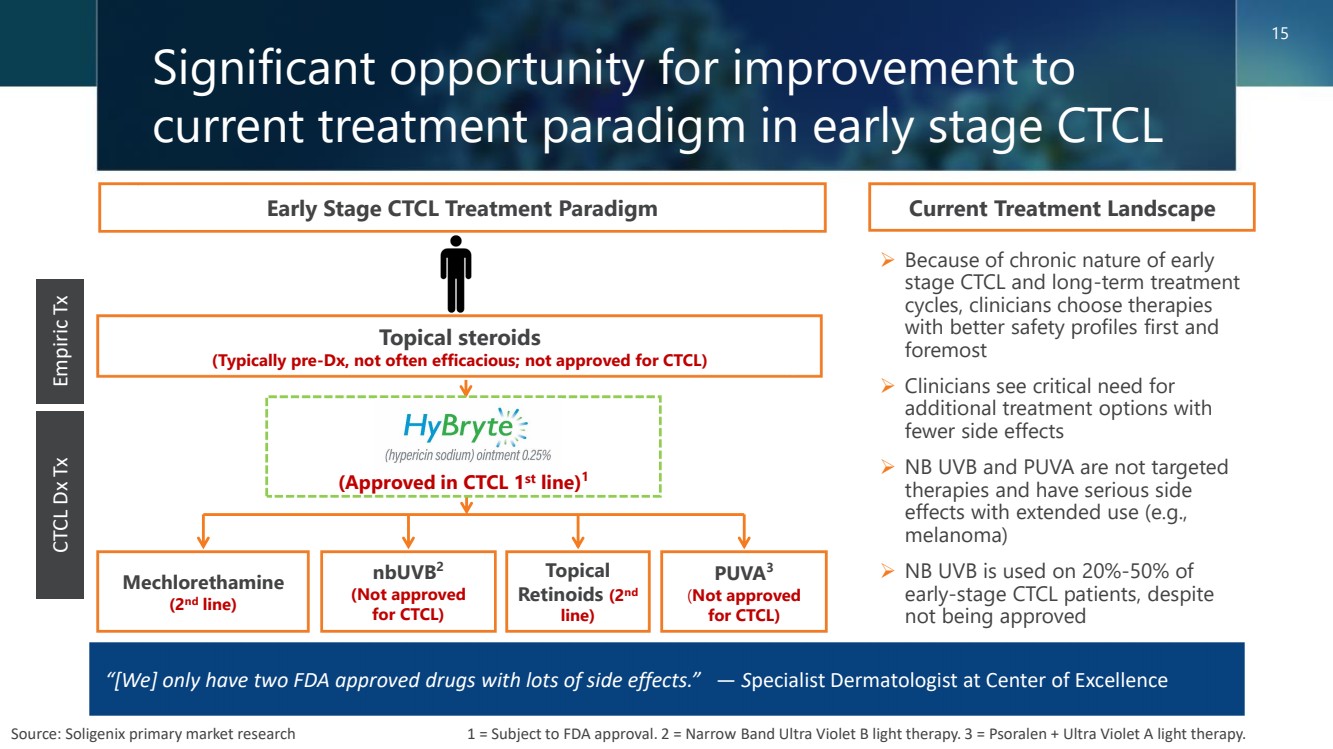
➢ Because of chronic nature of early stage CTCL and long-term treatment cycles, clinicians choose therapies with better safety profiles first and foremost ➢ Clinicians see critical need for additional treatment options with fewer side effects ➢ NB UVB and PUVA are not targeted therapies and have serious side effects with extended use (e.g., melanoma) ➢ NB UVB is used on 20%-50% of early-stage CTCL patients, despite not being approved Current Treatment Landscape Empiric Tx CTCL Dx Tx “[We] only have two FDA approved drugs with lots of side effects.” — Specialist Dermatologist at Center of Excellence Early Stage CTCL Treatment Paradigm Topical steroids (Typically pre-Dx, not often efficacious; not approved for CTCL) nbUVB2 (Not approved for CTCL) Mechlorethamine (2nd line) Topical Retinoids (2nd line) PUVA3 (Not approved for CTCL) Source: Soligenix primary market research 1 = Subject to FDA approval. 2 = Narrow Band Ultra Violet B light therapy. 3 = Psoralen + Ultra Violet A light therapy. Significant opportunity for improvement to current treatment paradigm in early stage CTCL (Approved in CTCL 1st line)1 15 |
|
HyBryte™ a Significant Commercial Opportunity Addressing a Clear Unmet Need ➢ Clinicians see need for additional treatment options with fewer side effects ➢ Most patients cycle through several treatments over course of their disease ➢ Chronic nature of early stage CTCL and dissatisfaction with current therapies provides opportunity for HyBryte™ ➢ Derms like efficacy of HyBryte™; rapid response with equal effect on both patches and plaques ➢ Derms like safety of HyBryte™; use of safe, visible light vs. UV light exposure ➢ 4 of 5 Derms likely to prescribe HyBryte™ ➢ Planned launch focused on high volume CTCL specialists ➢ Targeted sales force of ~20 reps; reaching >80% of high volume prescribers ➢ Partnership with medical device company, Daavlin, allows convenient end-to-end business solution for companion light unit to customers ➢ Treatment will not have large financial impact on payers; low/no barriers to access as reimbursement can occur under existing CPT code ➢ Competing 2nd line products with inferior profiles have achieved similar sales ➢ Life cycle management upside, with potential to transition to home use setting Unmet Need Positive Feedback Sales Potential >$250M WW Annual Net Sales Efficient Commercialization Source: Soligenix primary market research 16 |
|
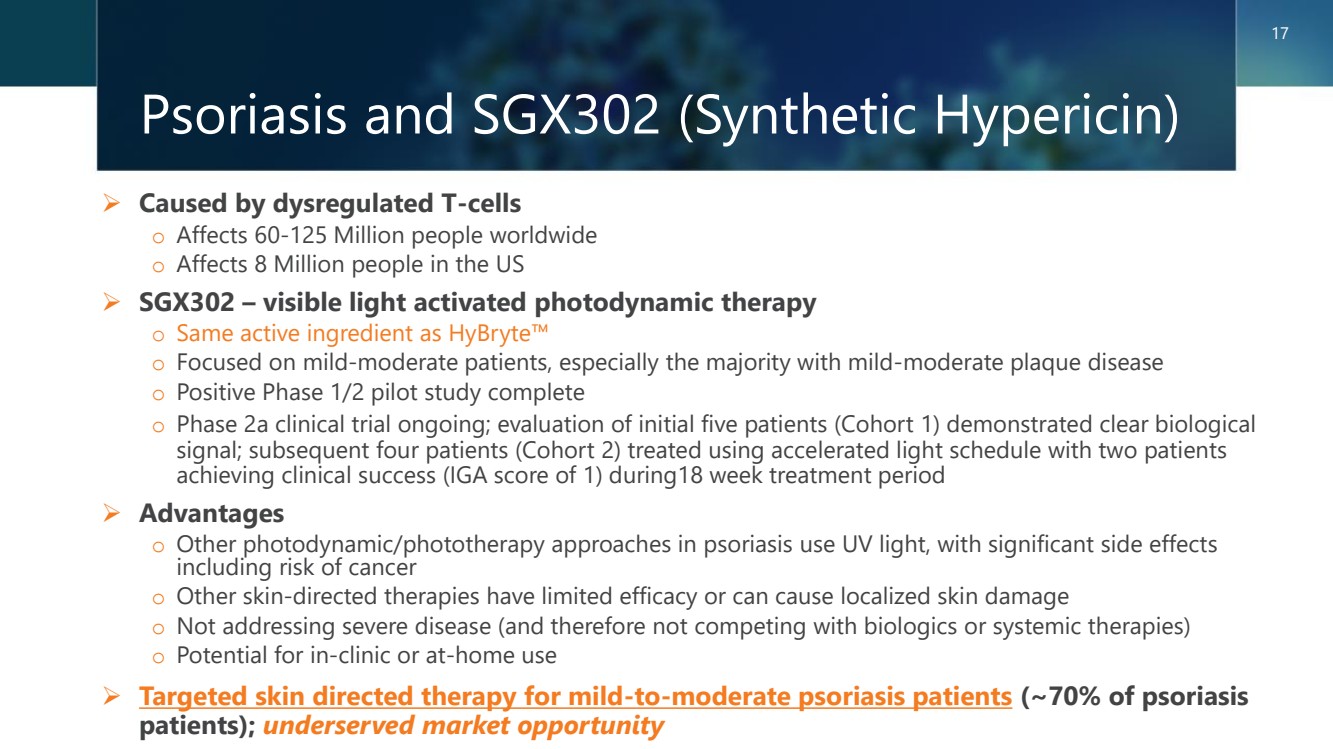
Psoriasis and SGX302 (Synthetic Hypericin) ➢ Caused by dysregulated T-cells o Affects 60-125 Million people worldwide o Affects 8 Million people in the US ➢ SGX302 – visible light activated photodynamic therapy o Same active ingredient as HyBryte™ o Focused on mild-moderate patients, especially the majority with mild-moderate plaque disease o Positive Phase 1/2 pilot study complete o Phase 2a clinical trial ongoing; evaluation of initial five patients (Cohort 1) demonstrated clear biological signal; subsequent four patients (Cohort 2) treated using accelerated light schedule with two patients achieving clinical success (IGA score of 1) during18 week treatment period ➢ Advantages o Other photodynamic/phototherapy approaches in psoriasis use UV light, with significant side effects including risk of cancer o Other skin-directed therapies have limited efficacy or can cause localized skin damage o Not addressing severe disease (and therefore not competing with biologics or systemic therapies) o Potential for in-clinic or at-home use ➢ Targeted skin directed therapy for mild-to-moderate psoriasis patients (~70% of psoriasis patients); underserved market opportunity 17 |
|
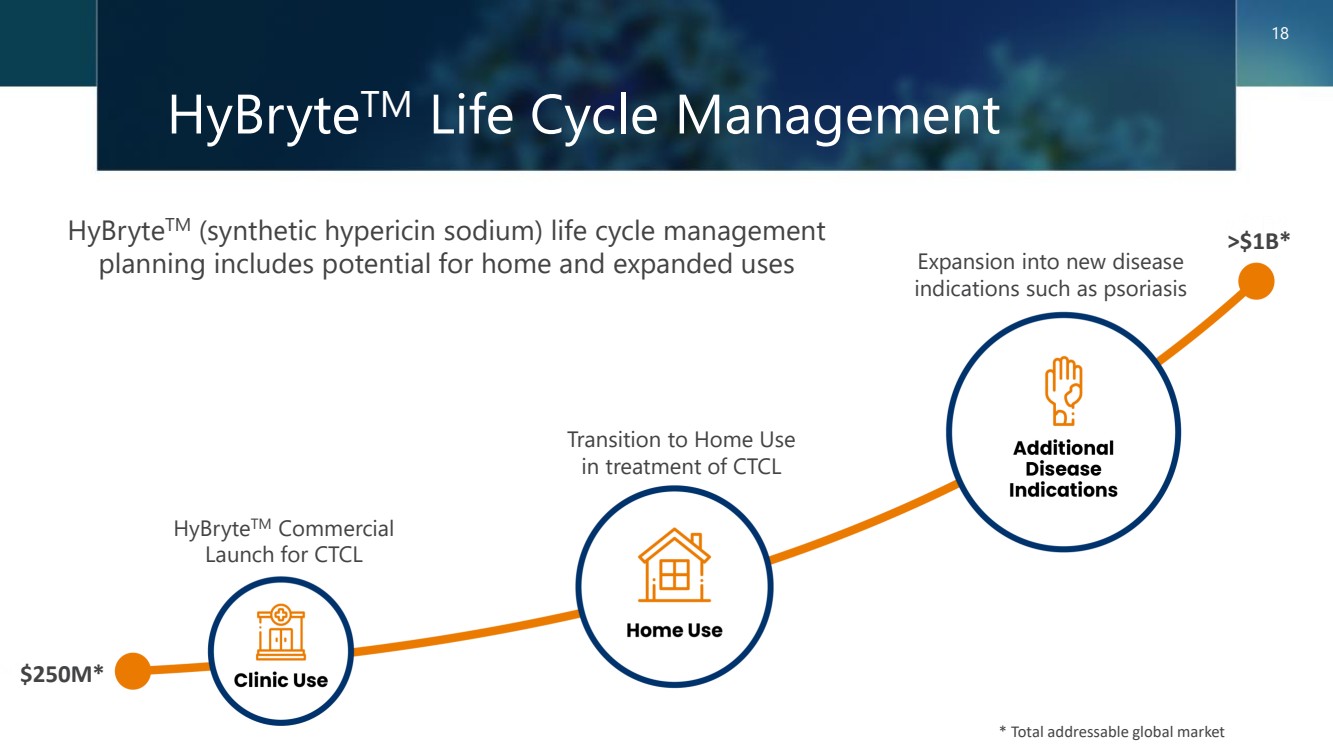
HyBryteTM Life Cycle Management 18 * Total addressable global market HyBryteTM (synthetic hypericin sodium) life cycle management planning includes potential for home and expanded uses * Total addressable global market $250M* >$1B* HyBryteTM Commercial Launch for CTCL Transition to Home Use in treatment of CTCL Expansion into new disease indications such as psoriasis |
|
Public Health Solutions Addressing Critical Concerns for Industry and Government 19 |
|
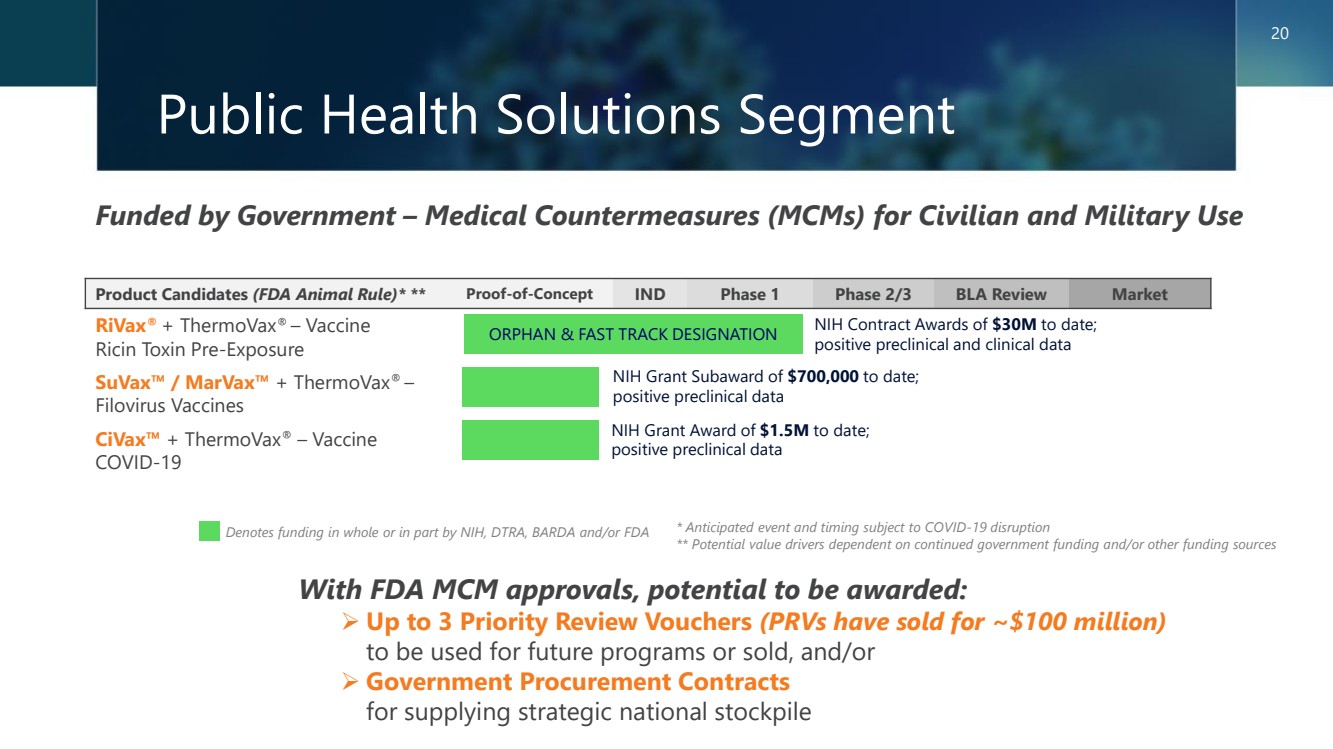
Public Health Solutions Segment Funded by Government – Medical Countermeasures (MCMs) for Civilian and Military Use With FDA MCM approvals, potential to be awarded: ➢ Up to 3 Priority Review Vouchers (PRVs have sold for ~$100 million) to be used for future programs or sold, and/or ➢ Government Procurement Contracts for supplying strategic national stockpile * Anticipated event and timing subject to COVID-19 disruption ** Potential value drivers dependent on continued government funding and/or other funding sources Denotes funding in whole or in part by NIH, DTRA, BARDA and/or FDA 20 Product Candidates (FDA Animal Rule)* ** Proof-of-Concept IND Phase 1 Phase 2/3 BLA Review Market RiVax® + ThermoVax® – Vaccine Ricin Toxin Pre-Exposure SuVax™ / MarVax™ + ThermoVax® – Filovirus Vaccines CiVax™ + ThermoVax® – Vaccine COVID-19 NIH Contract Awards of $30M to date; positive preclinical and clinical data ORPHAN & FAST TRACK DESIGNATION NIH Grant Award of $1.5M to date; positive preclinical data NIH Grant Subaward of $700,000 to date; positive preclinical data |
|
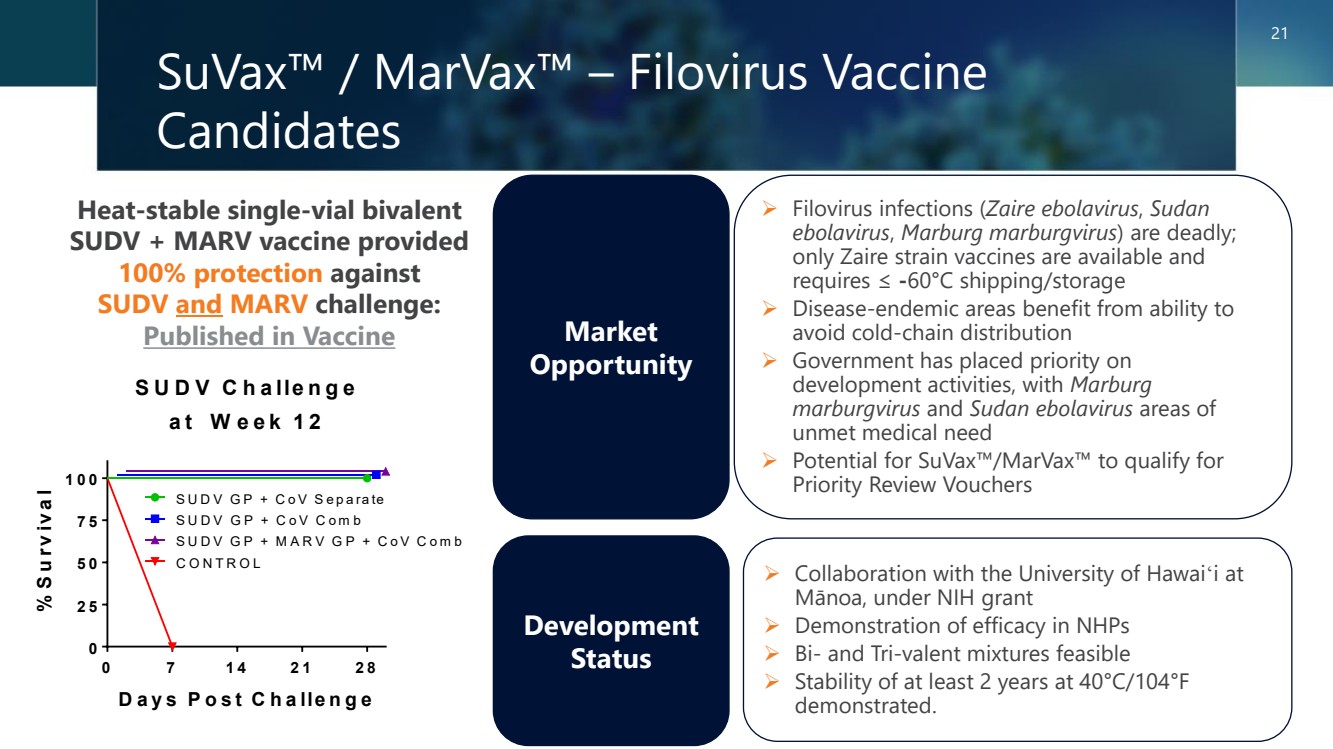
SuVax™ / MarVax™ – Filovirus Vaccine Candidates Heat-stable single-vial bivalent SUDV + MARV vaccine provided 100% protection against SUDV and MARV challenge: Published in Vaccine Market Opportunity ➢ Filovirus infections (Zaire ebolavirus, Sudan ebolavirus, Marburg marburgvirus) are deadly; only Zaire strain vaccines are available and requires ≤ -60°C shipping/storage ➢ Disease-endemic areas benefit from ability to avoid cold-chain distribution ➢ Government has placed priority on development activities, with Marburg marburgvirus and Sudan ebolavirus areas of unmet medical need ➢ Potential for SuVax™/MarVax™ to qualify for Priority Review Vouchers Development Status ➢ Collaboration with the University of Hawaiʻi at Mānoa, under NIH grant ➢ Demonstration of efficacy in NHPs ➢ Bi- and Tri-valent mixtures feasible ➢ Stability of at least 2 years at 40°C/104°F demonstrated. 21 0 7 1 4 2 1 2 8 0 2 5 5 0 7 5 1 0 0 S U D V C h a lle n g e a t W e e k 1 2 D a y s P o s t C h a lle n g e % S u rv iv a l S U D V G P + C o V S e p a ra te S U D V G P + C o V C o m b S U D V G P + M A R V G P + C o V C o m b C O N T R O L |
|
Experienced Management and Board of Directors Christopher J. Schaber, PhD Chairman, President & CEO • 30 years of experience • Discovery Laboratories (COO) • Acute Therapeutics (Co-Founder) • Ohmeda Pharmaceuticals • The Liposome Company • Wyeth Ayerst Richard Straube, MD Chief Medical Officer • 35 years of experience • Stealth Peptides Inc. • INO Therapeutics • Ohmeda Pharmaceuticals • Centocor Oreola Donini, PhD Chief Scientific Officer • 20 years of experience • Inimex Pharmaceuticals • ESSA Pharma, Inc. • Kinetek Pharmaceuticals Jonathan Guarino, CPA, CGMA Chief Financial Officer • 25 years of experience • Hepion Pharmaceuticals, Inc. • Covance, Inc. • BlackRock, Inc. • Barnes & Noble, Inc. • PricewaterhouseCoopers LLP Gregg Lapointe, CPA, MBA • 30 years of experience • Cerium Pharmaceuticals (CEO) • Formerly of Sigma-Tau Pharmaceuticals, AstenJohnson, PricewaterhouseCoopers Diane Parks • 30 years of experience • Formerly of Kite Pharma, Pharmacyclics, Amgen, Genentech Robert Rubin, MD • 40 years of experience • Georgetown School of Medicine • Formerly of The Lewin Group • Former U.S. Assistant Surgeon General Jerome Zeldis, MD, PhD • 35 years of experience • Formerly of Celgene Corporation (CMO), Sandoz, Janssen Research Institute, Sorrento, Celularity, NexImmune 22 |
|
In Summary ➢ Robust pipeline consisting of multiple fast track and/or orphan designated products, with potential for significant commercial returns of ~$2B in global annual sales ➢ Late clinical-stage assets, one with successful Phase 3 data readout o Cutaneous T-cell lymphoma (HyBryte™ or SGX301) – Positive statistically significant results achieved in first Phase 3 study; published JAMA Dermatology – Second confirmatory Phase 3 study of similar design accepted by EMA; FDA discussions remain ongoing – Confirmatory Phase 3 double-blind, placebo-controlled study in ~80 patients to initiate in 2H 2024 – Significant commercial opportunity in area of unmet medical need; estimated global market potential >$250M o Psoriasis (SGX302) – Positive and statistically significant results achieved in Phase 1/2 proof of concept (POC) study – Phase 2a study in mild-to-moderate psoriasis ongoing; clinical success achieved in 2 of 4 Cohort 2 patients – Significant commercial opportunity in area of unmet medical need; estimated global market potential >$1B o Behçet's disease (SGX945) – Phase 2a study in aphthous ulcers in Behçet's Disease; FDA IND & protocol cleared, fast track designation received – Significant commercial opportunity in area of unmet medical need; estimated global market potential >$200M ➢ Collaborations with biotech, academia and government agencies ➢ Non-dilutive government funding helps cover operating expenses o NIH grant awards supporting vaccine development; potential for up to 3 Priority Review Vouchers (PRVs) ➢ Experienced management team and renowned advisors with record of success 23 |
|
Thank you www.soligenix.com NASDAQ: SNGX 24 Follow us on: facebook.com/soligenix/ twitter.com/Soligenix_Inc linkedin.com/company/soligenix-inc-/ youtube.com/c/SoligenixInc |