UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, DC 20549
FORM 10-K
(Mark one)
☒ |
ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended December 31, 2023
OR
☐ |
TRANSITION REPORT PURSUANT TO SECTION 13 OR 15 (d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from to
Commission File Number: 001-41740
Apogee Therapeutics, Inc.
(Exact name of registrant as specified in its charter)
Delaware |
88-0588063 |
(State or other jurisdiction of |
(I.R.S. Employer |
incorporation or organization) |
Identification Number) |
221 Crescent St., Building 17, Suite 102b
Waltham, MA 02453
(650) 394-5230
(Address including zip code, and telephone number including area code, of registrant’s principal executive offices)
Former name, former address and former fiscal year, if changed since last report: N/A
Securities registered pursuant to Section 12(b) of the Exchange Act:
Title of each class |
Trading Symbol(s) |
Name of each exchange on which registered |
Common Stock, par value $0.00001 per share |
APGE |
The Nasdaq Global Market |
Securities registered pursuant to Section 12(b) of the Exchange Act: None.
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☐ No ☒
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ☐ No ☒
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ☒ No ☐
Indicate by check mark whether the registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405 of Regulation S-T (§ 232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit such files). Yes ☒ No ☐
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company, or an emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company,” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
Large accelerated filer |
☐ |
Accelerated filer |
☐ |
Non-accelerated filer |
☒ |
Smaller reporting company |
☒ |
|
|
Emerging growth company |
☒ |
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Indicate by check mark whether the registrant has filed a report on and attestation to its management’s assessment of the effectiveness of its internal control over financial reporting under Section 404(b) of the Sarbanes-Oxley Act (15 U.S.C. 7262(b)) by the registered public accounting firm that prepared or issued its audit report. ☐
If securities are registered pursuant to Section 12(b) of the Act, indicate by check mark whether the financial statements of the registrant included in the filing reflect the correction of an error to previously issued financial statements. ☐
Indicate by check mark whether any of those error corrections are restatements that required a recovery analysis of incentive-based compensation received by any of the registrant’s executive officers during the relevant recovery period pursuant to §240.10D-1(b). ☐
The registrant was not a public company as of the last business day of its most recently completed second fiscal quarter and therefore cannot calculate the aggregate market value of the voting and non-voting common equity held by non-affiliates as of such date.
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes ☐ No ☒
As of February 23, 2024, the registrant had 50,655,671 shares of common stock, $0.00001 par value per share, outstanding, comprised of 37,169,029 shares of voting common stock, $0.00001 par value per share, and 13,486,642 shares of non-voting common stock, $0.00001 par value per share.
DOCUMENTS INCORPORATED BY REFERENCE
None.
TABLE OF CONTENTS
Explanatory Note
As used in this Annual Report on Form 10-K (this “Annual Report”), unless the context otherwise requires, references to “we,” “us,” “our,” the “Company,” “Apogee” and similar references refer: (1) following the consummation of our Reorganization (as defined elsewhere in this Annual Report) on July 13, 2023 in connection with our initial public offering, to Apogee Therapeutics, Inc. and our subsidiary, and (2) prior to the completion of our Reorganization, to Apogee Therapeutics, LLC and its subsidiary. See “Management’s Discussion and Analysis of Financial Condition and Results of Operations”—“Reorganization” in this Annual Report for further information.
2
SPECIAL NOTE REGARDING FORWARD-LOOKING STATEMENTS
This Annual Report contains “forward-looking statements” within the meaning of the federal securities laws, which statements are subject to substantial risks and uncertainties and are based on current expectations, estimates, forecasts and assumptions. All statements other than statements of historical fact included in this Annual Report, including statements concerning our plans, objectives, goals, strategies, future events, future revenues or performance, capital requirements or financing needs, capital expenditures, commitments, preclinical studies, clinical trials, plans or intentions relating to product candidates, expected markets and business trends and other statements, including those discussed under the sections titled “Risk Factors” and “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and elsewhere in this Annual Report, are forward-looking statements. In some cases, you can identify forward-looking statements by terms such as “may,” “might,” “will,” “would,” “shall,” “objective,” “intend,” “target,” “should,” “could,” “can,” “expect,” “anticipate,” “believe,” “design,” “estimate,” “forecast,” “predict,” “potential,” “plan,” “seek,” or “continue” or the negative of these terms and similar expressions intended to identify forward-looking statements. Forward-looking statements reflect our current views with respect to future events. Given the significant risks and uncertainties, you should not place undue reliance on these forward-looking statements.
There are a number of risks, uncertainties and other factors that could cause our actual results to differ materially from the forward-looking statements expressed or implied in this Annual Report. Such risks, uncertainties and other factors include, among others, the following:
| ● | our plans to develop and commercialize our programs for the treatment of atopic dermatitis, asthma, chronic obstructive pulmonary disease and related inflammatory and immunology indications with high unmet need; |
| ● | our ability to obtain funding for our operations, including funding necessary to complete the development and commercialization of our programs; |
| ● | the timing and focus of our ongoing and future preclinical studies and clinical trials and the reporting of data from those studies and trials; |
| ● | the beneficial characteristics, safety, efficacy and therapeutic effects of our programs; |
| ● | our plans relating to the further development of our programs, including additional indications we may pursue; |
| ● | the size of the market opportunity for our programs, including our estimates of the number of patients who suffer from the diseases we are targeting; |
| ● | our continued reliance on third parties to conduct additional preclinical studies and clinical trials of our programs and for the manufacture of our product candidates for preclinical studies and clinical trials; |
| ● | the success, cost and timing of our preclinical and clinical development activities and planned clinical trials; |
| ● | our plans regarding, and our ability to obtain, and negotiate favorable terms of, any collaboration, licensing or other arrangements that may be necessary or desirable to develop, manufacture or commercialize our programs; |
| ● | the timing of and our ability to obtain and maintain regulatory approvals for our programs, as well as future programs; |
| ● | the rate and degree of market acceptance and clinical utility of our programs; |
| ● | the success of competing treatments that are or may become available; |
3
| ● | our ability to attract and retain key management and technical personnel; |
| ● | our expectations regarding our ability to obtain, maintain and enforce intellectual property protection for our programs; |
| ● | our financial performance; |
| ● | the period over which we estimate our existing cash and cash equivalents, and marketable securities will be sufficient to fund our future operating expenses and capital expenditure requirements; |
| ● | our expectations regarding the period during which we will qualify as an emerging growth company under the Jumpstart Our Business Startups Act of 2012; and |
| ● | our anticipated use of our existing resources |
These and other risks and uncertainties and other factors, including those discussed under the section titled “Risk Factors” of this Annual Report, may cause our actual results and outcomes, or timing of our results or outcomes, to differ materially and adversely from the forward-looking statements expressed or implied in this Annual Report including factors disclosed in the sections titled “Risk Factors” and “Management’s Discussion and Analysis of Financial Condition and Results of Operations.” You should evaluate all forward-looking statements made in this Annual Report in the context of these risks and uncertainties.
We caution you that the risks, uncertainties and other factors referred to above and elsewhere in this Annual Report may not contain all of the risks, uncertainties and other factors that may affect us, our future results or operations. Moreover, new risks may emerge from time to time. It is not possible for us to predict all risks. In addition, we cannot assure you that we will realize the results, benefits or developments that we expect or anticipate or, even if substantially realized, that they will result in the consequences or affect us or our business in the way expected.
All forward-looking statements in this Annual Report apply only as of the date made and are expressly qualified in their entirety by this and other cautionary statements included in this Annual Report. Except as required by law, we undertake no obligation to publicly update or revise any forward-looking statements, whether as a result of new information, subsequent events, changes in assumptions or circumstances or otherwise.
In addition, statements such as “we believe” and similar statements reflect our beliefs and opinions on the relevant subject. These statements are based upon information available to us as of the date of this Annual Report, and while we believe we have a reasonable basis for such statements, our information may be limited or incomplete, and our statements should not be read to indicate that we have conducted an exhaustive inquiry into, or review of, all potentially available relevant information. These statements are inherently uncertain and you are cautioned not to unduly rely upon these statements.
4
Part I
Item 1. Business
Overview
We are a clinical stage biotechnology company seeking to develop differentiated biologics for the treatment of atopic dermatitis (AD), asthma, chronic obstructive pulmonary disease (COPD) and related inflammatory and immunology (I&I) indications with high unmet need. Our antibody programs are designed to overcome limitations of existing therapies by targeting well-established mechanisms of action and incorporating advanced antibody engineering to optimize half-life and other properties. Our two most advanced programs are APG777 and APG808, which we are initially developing for the treatment of AD and COPD, respectively. With our broad pipeline and depth of expertise, we believe we can deliver value and meaningful benefit to patients underserved by today’s standard of care. See the section titled “—Recent Developments” for program updates.
APG777 is a subcutaneous (SQ) extended half-life monoclonal antibody (mAb) targeting IL-13. AD is a chronic inflammatory skin disorder that affects approximately 40 million adults and 18 million children in the United States, France, Germany, Italy, Japan, Spain and the United Kingdom, 40% of which have moderate-to-severe disease. Based on our preclinical studies, we believe APG777 can be dosed either every two or every three months in maintenance, which, if our clinical trials are successful, would represent a significant improvement compared to first generation IL-13 antibodies that are dosed every two to four weeks. In August 2023, we announced the dosing of our first participant in our first clinical trial for APG777 in Australia. The APG777 Phase 1 trial is a double-blind, placebo-controlled study in healthy volunteers and consists of a single-ascending dose (SAD) component and a multiple-ascending dose (MAD) component. The trial enrolled 40 healthy adult subjects into three SAD and two MAD cohorts. The primary endpoint is safety and a key secondary endpoint is pharmacokinetics (PK). The Phase 1 trial is ongoing and we have announced initial safety and PK data from this trial. We have filed an investigational new drug application (IND) in support of a Phase 1 trial in healthy volunteers in the United States for subjects of Japanese descent and have received a “study may proceed” letter from the FDA for the trial. We anticipate initiating a Phase 2 trial in AD in the United States and internationally in the first half of 2024. Based on our initial clinical data, we may initiate a Phase 2 trial in asthma and expect to further evaluate opportunities to develop APG777 for other I&I indications, including alopecia areata (AA), chronic rhinosinusitis with nasal polyps (CRSwNP), chronic spontaneous urticaria (CSU), eosinophilic esophagitis (EoE) and prurigo nodularis (PN).
APG808 is an SQ extended half-life mAb targeting IL-4Rα, a target with clinical validation across eight different Type 2 allergic diseases. COPD is a heterogenous, progressive respiratory condition characterized by cough, dyspnea and airflow obstruction that affects approximately 32 million adults 40 years of age and older in the United States, France, Germany, Italy, Japan, Spain and the United Kingdom. Based on our preclinical studies, we believe APG808 can be dosed either every six weeks or every two months in maintenance, which, if our clinical trials are successful, would represent a significant improvement compared to first generation IL-4Rα antibodies that are dosed every two weeks. In November 2023, we finalized the nomination of a development candidate for our APG808 program for the treatment of COPD. Since then, we have completed a toxicology program that included a one-month GLP toxicology study in mice with the NOAEL observed at 1,000 mg/kg/dose. In February 2024, we received regulatory approval to commence a first-in-human clinical trial in Australia. We expect to enter the clinic with APG808 in healthy volunteers followed by a potential Phase 1b trial in asthma and/or a Phase 2 trial in COPD (pending data from the Phase 1 trial and following the submission of an IND or foreign equivalent to support such trials).
Our earlier-stage programs, APG990 and APG222, utilize advanced antibody engineering to target OX40L and both IL-13 and OX40L, respectively, which we are initially developing for the treatment of AD. OX40L occurs higher up in the inflammatory pathway than IL-13 or IL-4Rα and potentially broadens the impact on the inflammatory cascade. With current approved biologics only targeting two mechanisms of action (IL-13 and IL4Rα) in AD, OX40L could represent another therapeutic option for patients, especially the portion of patients who do not benefit from currently available treatments. We expect to nominate a development candidate for APG990 in 2024. In addition, we believe that blocking multiple targets, such as simultaneous inhibition of IL-13 and OX40L in APG222, could allow us to provide benefit to patients with AD and other I&I indications. We recently added a new program that also utilizes advanced antibody engineering for an undisclosed target.
5
We believe that each of our programs has the potential to impact multiple additional I&I indications.
Recent Developments
APG777 Positive Interim Phase 1 Data
On March 5, 2024, we announced positive interim Phase 1 data from our first-in-human study of APG777, one of our lead product candidates being developed as a frontline treatment for moderate-to-severe AD and other inflammatory diseases. Pharmacokinetic (PK) data showed a half-life of approximately 75 days across doses tested and Pharmacodynamic (PD) data showed deep and sustained inhibition of key AD biomarkers pSTAT6 and TARC for approximately three months (longest available follow-up available, with inhibition still ongoing at time of the data cut). Results from the trial exceeded our trial objectives and support the potential for APG777, a novel anti-IL-13 antibody, to optimize exposure levels in 16-week induction and be dosed once every three or six months in maintenance. These findings represent the potential for improved clinical responses from greater exposures in induction and significantly less frequent dosing in maintenance compared to currently approved biologic therapies, which are dosed at every two to four weeks, a potential major advancement for patients with AD and other inflammatory diseases.
APG777, in single doses up to 1,200mg and multiple doses of 300mg, was well tolerated and showed a favorable safety profile, in line with the existing body of third-party evidence for the safety of the anti-IL-13 class. Based on these data, we plan to initiate a randomized, placebo-controlled, Phase 2 clinical trial in patients with moderate-to-severe AD in the first half of 2024 ahead of schedule.
Key Phase 1 Interim Findings
The Phase 1 trial is a first-in-human, randomized, double-blind, placebo-controlled study designed to evaluate safety and PK of APG777 in healthy volunteers. The study enrolled 40 healthy adult participants into three SAD and two MAD cohorts. Doses of subcutaneous APG777 evaluated in the study included 300mg, 600mg and 1,200mg.
APG777’s PK differentiation supports further development of APG777 as a treatment for moderate-to-severe AD and other inflammatory diseases. APG777’s potentially best-in-class PK profile, including a half-life of approximately 75 days, supports testing higher exposures of drug in induction to potentially achieve improved clinical responses; and testing of maintenance dosing of every three or six months, representing two to four injections per year compared to the current treatment paradigm of 13 to 26 injections per year. Dose-proportional increases in serum concentrations and key parameters (e.g., Cmax, AUC) were observed in the Phase 1 trial. PK was consistent across subjects with low variability.
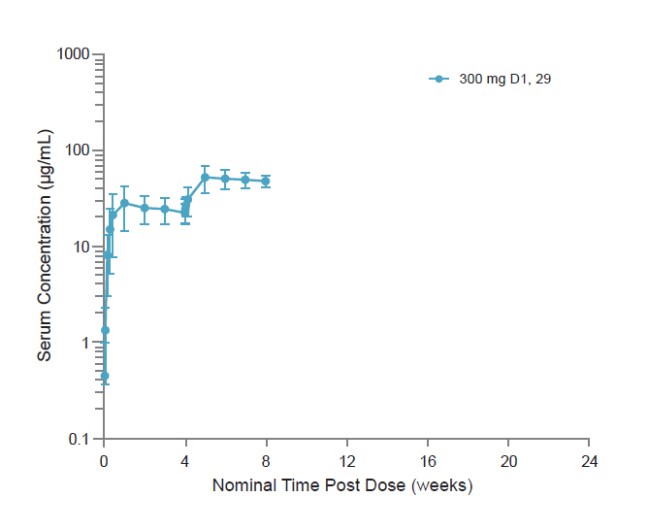
Figures A and B show single- and multi-dose concentration-time profiles, respectively, from the ongoing Phase 1 trial.
6
Figure A—Single-dose concentration-time profile
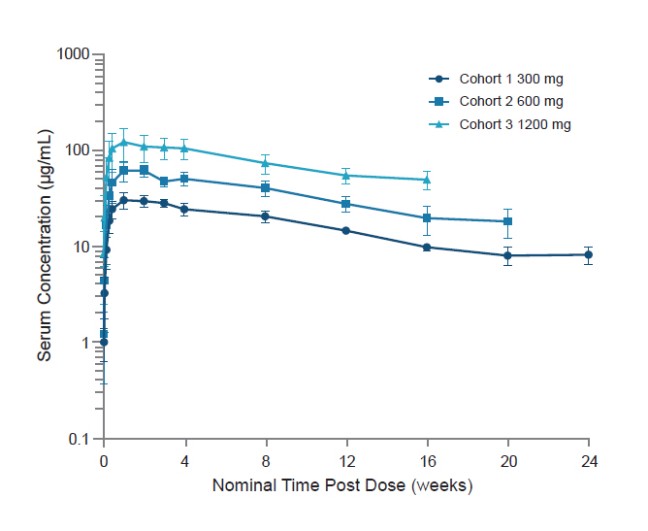
Figure B—Multi-dose concentration-time profile
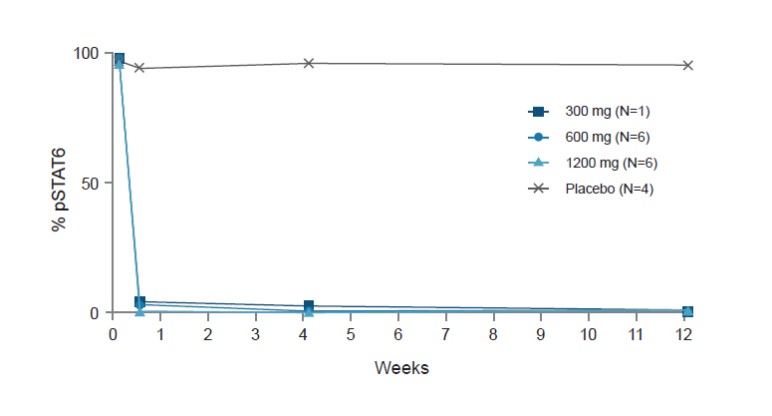
Single doses of APG777 demonstrated a deep and sustained effect on PD markers for approximately three months (longest follow-up available with inhibition still ongoing at time of data cut). Single doses of APG777 suppressed pSTAT6, one of the first downstream markers of IL-13 pathway inhibition, with near-complete inhibition (both in terms of median and mean percent change from baseline) for approximately three months.
7
Single doses of APG777 suppressed TARC, an inflammatory mediator and the most strongly correlated biomarker to AD severity, with deep and sustained inhibition for approximately three months.
Figure C shows pSTAT6 and TARC as biomarkers of IL-13 engagement and AD severity.
Figure C—pSTAT6 and TARC are biomarkers of IL-13 target engagement and AD severity
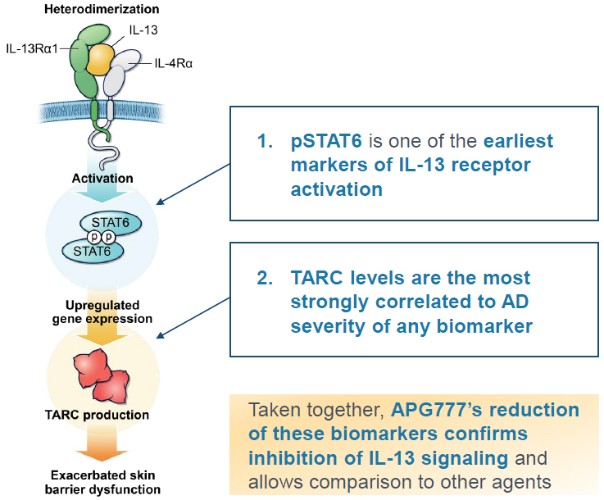
Figure D shows pSTAT6 inhibition data for APG777 from our Phase 1 trial.
Figure D—Median percent change from baseline in pSTAT6
8
Figure E shows TARC inhibiton data for APG777 from our Phase 1 trial in 6 healthy volunteers receiving a single SC injection of 300mg of APG777.
Figure E—Median % changes from baseline in TARC inhibition
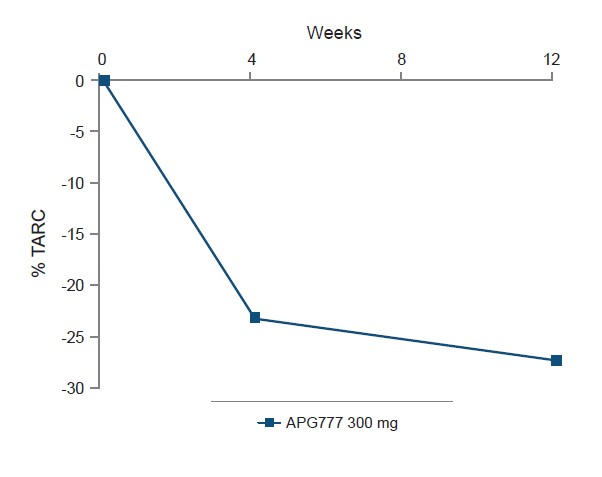
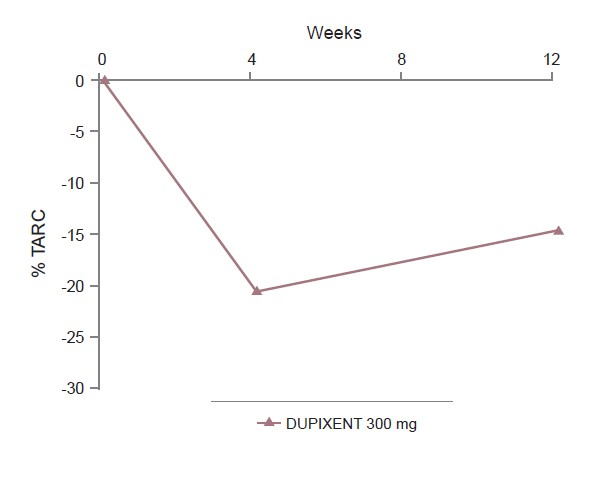
Figure F shows TARC inhibition for DUPIXENT using data derived from a third–party Phase 1 trial with 6 healthy volunteers receiving a single SC injection of 300 mg DUPIXENT.
9
Figure F—Median % changes from baseline in TARC inhibition
Single doses of APG777 up to 1,200mg and multiple doses of 300mg were well tolerated with a favorable safety profile consistent with the existing third-party data supporting the safety of the anti-IL-13 class. The most common treatment-emergent adverse events (TEAEs) were vascular access site pain, vessel puncture site bruise, headache, and vascular access bruising. 60% of participants observed at least one TEAE; 15% of participants observed at least one drug-related adverse event (AE). There were no Grade 3 TEAEs or severe adverse events related to study drug. No AEs led to discontinuation of the study.
Phase 2 Trial in AD
Following our positive interim results, we plan to advance APG777 into a randomized, placebo-controlled, 16-week Phase 2 clinical trial in patients with moderate-to-severe AD.
The integrated Phase 2 AD trial is expected to initiate in the first half of 2024 with 16-week topline data from Part A expected in the second half of 2025. Part A is expected to enroll approximately 110 patients randomized 2:1 to APG777 and placebo with primary endpoint of mean percentage changes in EASI score from baseline to Week 16. Part B of the Phase 2 trial is a randomized, placebo-controlled dose optimization with approximately 360 patients randomized 1:1:1:1 to high, medium, or low dose APG777 and placebo with primary endpoint of mean percentage changes in EASI score from baseline to Week 16. All patients benefiting from treatment will continue to APG777 maintenance, which will evaluate three- to six-month dosing.
The integrated design is expected to provide for significant timeline acceleration by combining Phase 2a and Phase 2b elements into a single study protocol. All Part A sites are also expected to participate in Part B, which should avoid delays for site startup between the two parts. Doses in the Phase 2 trial are enabled by APG777’s potentially best-in-class PK profile, extended half-life, and high-concentration formulation. Our 180mg/mL formulation enables a 44% higher dose of APG777 compared to lebrikizumab in the same volume.
The APG777 Phase 2 induction regimen is designed to exceed lebrikizumab (an IL-13 inhibitor with an overlapping epitope with APG777) exposures by approximately 30 to 40% with potential for improved clinical outcomes and maintenance regimen is designed to equal lebrikizumab’s exposures.
10
In Phase 3 studies, approximately 30% higher exposure seen in lebrikizumab low bodyweight group resulted in numerically higher efficacy than the overall study population across all key endpoints, including EASI-75 and more stringent endpoints such as EASI-90 and IGA 0/1. Approximately 30 to 40% higher induction exposures for APG777 than lebrikizumab are based on a planned six injection induction regimen given in the first sixteen weeks of APG777 treatment. This is approximately half as many of the 11 injections of lebrikizumab given during the same period. At 52 weeks, exposures of APG777 dosed every three months are designed to exceed those of lebrikizumab and exposures of APG777 dosed every six months are designed to equal those of lebrikizumab.
We also may evaluate APG777 in expansion indications including initiating a Phase 2 trial in asthma in 2025.
APG808 Phase 1 Trial
On March 5, 2024, we also announced that our Phase 1 APG808 healthy volunteer clinical trial is expected to enter the clinic ahead of scheduled in the first half of 2024 following receipt of regulatory clearance in February 2024. In addition, we expect interim Phase 1 PK and safety data in healthy volunteers in the second half of 2024, ahead of prior guidance, and initial proof-of-concept data in asthma in the first half of 2025. We expect to initiate a proof-of-concept clinical trial in patients with COPD in 2025, pending positive data from Phase 1 trial and regulatory clearance.
APG990 and APG222
On March 5, 2024, we also announced that our early-stage programs, APG990 and APG222, are progressing to candidate selection. We expect to nominate a candidate for APG990 in 2024 and initiate a Phase 1 trial in healthy volunteers in 2025. We plan to provide more detailed updates on our earlier pipeline programs and combination strategy in an R&D Day in the fourth quarter of 2024.
Our Approach
Our goal is to discover and develop new therapies for a range of I&I indications. We aim to accomplish this goal by focusing on known biologic drivers of disease and utilizing advanced antibody engineering to develop product candidates with optimized properties that have the potential to overcome limitations of existing therapies. For instance, our two most advanced programs, APG777 and APG808, bind to the same epitopes, or binding sites, on IL-13 and IL-4Rα as lebrikizumab and DUPIXENT (dupilumab), respectively, based on our head-to-head preclinical studies, but are designed to include extended half-life technologies and other optimized properties. When designing our programs, we test multiple half-life extension technologies, including YTE and LS amino acid modifications, to identify the optimal candidate to advance against each target. YTE amino acid modifications are a triple modification (M252Y/S254T/T256E) introduced into the antibody, while LS amino acid modifications are a double modification (M428L/N434S). YTE and LS amino acid modifications are proven half-life extension technologies that have the potential to significantly improve the PK profile and reduce injection burden compared to existing agents. In addition to extended half-life, our antibody engineering programs are designed to improve antibody candidate attributes, including in vitro potency, bioavailability and decreased PK variability, as well as those attributes essential for manufacturability and high concentration formulation (i.e. viscosity, solubility and stability) to generate optimized antibodies. We believe our approach will enable us to develop a portfolio of therapies that are differentiated compared to the currently available standards of care and address unmet medical needs for I&I indications, including the potential for improved dosing and/or efficacy.
Biologics Are Common Treatments for I&I Diseases
Over the last two decades, biologics have become more common for the treatment of a wide range of I&I indications and remain the core therapeutic modality today. New treatments for I&I indications have largely been driven by biologics, which accounted for nearly 90% of I&I product revenues. Given the overlapping mechanistic drivers of many I&I indications, indication expansion remains a consistent hallmark of many I&I products. Broadly, mAbs have been developed to target both diseases driven by T helper type 1 (Th1) immune responses, which involve IL-2, interferon-γ and lymphotoxin-α and an associated neutrophilic response, and diseases driven by T helper type 2 (Th2) immune responses, which involve IL-4, IL-5 and IL-13 and an associated eosinophilic response.
11
As one example, psoriasis, with a moderate-to-severe population estimated to be approximately 9.2 million patients, had the first biologic approved in 2008 and an additional six biologics approved from that time to 2023. Only one other indication, psoriatic arthritis, has more approved biologics. By contrast, the moderate-to-severe AD population, which is estimated to be approximately 25.1 million patients, has only two approved biologics, which leaves a large unmet need for patients with AD.
DUPIXENT is an example of the success of approved therapeutics. Since its approval for the treatment of AD in 2017, DUPIXENT has also been approved in asthma, CRSwNP, EoE and PN and is being clinically developed in allergic bronchopulmonary aspergillosis, allergic fungal rhinosinusitis, bullous pemphigoid, chronic pruritis of unknown origin, cold inducible urticaria, COPD, chronic rhinosinusitis sans nasal polyps and CSU, and is expected to reach peak sales of $21 billion in 2031 based on consensus estimates. Although our most advanced program APG777 targets the same mechanism of action as DUPIXENT, there is no assurance that our clinical trial results will achieve similar clinical trial results with respect to safety and/or efficacy or that APG777 will achieve FDA approval or commercial success.
AD Background and Current Treatment Limitations
AD, the most common subtype of eczema, is a chronic inflammatory skin disorder that affects individuals of all ages and races. AD affects individuals living in geographic regions worldwide. AD is characterized by pruritic (itchy), erythematous (red) and often excoriated (damaged) skin lesions, which are most often located on the neck, inner elbows and behind the knees. The specific cause of AD is unknown; however, research has shown that genetics, the immune system and the environment all play a role in the disease. AD can significantly impact quality of life, leading to sleep disturbance, psychological distress, elevated infection risk and chronic pain. AD is frequently associated with other atopic manifestations such as food allergy, allergic rhinitis (also known as hay fever) and asthma. AD is characterized by a Th2 response, which describes Th2 cells, a subset of white blood cells, that produce small proteins called cytokines, like IL-13, which regulate inflammation, immune response and tissue repair.
AD usually begins in childhood; however, anyone can become affected with this inflammatory disease at any age. It is estimated that 40 million adults and 18 million children in the United States, France, Germany, Italy, Japan, Spain and the United Kingdom are affected by AD. Approximately 40% of all patients have moderate-to-severe disease. The incidence of AD has increased two to three-fold in industrialized nations since the 1970s, with approximately 15% to 20% of children and 1% to 3% of adults affected worldwide.
There is no cure for AD and many people have difficulty controlling the disease. AD patients work with a dermatologist to determine treatment options that can bring their symptoms under control. For less extensive disease (i.e., mild-to-moderate AD), treatment is primarily topical corticosteroids and targeted topical treatments (e.g., a topical Janus kinase (JAK) inhibitor). For more extensive disease (i.e., moderate-to-severe AD), mAbs have emerged as the preferred frontline therapy in most adult and pediatric patients that is not controlled by topical therapies. Avoiding environmental and stress triggers, increased skin care regimen and dietary and lifestyle changes may also be part of the treatment recommendations.
There are two FDA-approved mAbs, Regeneron and Sanofi’s DUPIXENT (dupilumab), a mAb targeting IL-4Rα, and LEO Pharma’s ADBRY (tralokinumab-ldrm), a mAb targeting IL-13, labeled to treat moderate-to-severe AD.
Lebrikizumab is an investigational mAb targeting IL-13 being developed by Eli Lilly and Company and currently under regulatory review for approval in the United States and has been approved in the European Union and Japan.
Despite recent advancements in AD treatment, a significant number of patients continue to suffer from active disease. Today’s treatments are associated with many challenges, including a high frequency of injections that may lead to poor patient compliance. Based on a peer-reviewed third-party study of real world use published in the Journal of the American Academy of Dermatology, more than 20% of patients discontinue treatment with DUPIXENT within six months of starting therapy. The dosing schedule of biologics for AD is driven by the half-life for these agents, which provides a meaningful opportunity for a new treatment option with improved administration due to less frequent dosing.
12
COPD Background and Current Treatment Limitations
COPD is a heterogenous, progressive respiratory condition characterized by cough, dyspnea and airflow obstruction. It is estimated that approximately 10% of the global population 40 years of age and older have COPD, and in 2019 (prior to the COVID–19 pandemic), COPD was the third leading cause of death globally. In the United States, over 150,000 people die of COPD each year.
Three symptoms of COPD are dyspnea (difficulty breathing), cough and sputum (coughed-up phlegm) production. There are several possible linked risk factors to COPD including cigarette smoke, environmental factors (e.g., pollution and occupational exposures), airway responsiveness, atopy, asthma, infections and genetics.
COPD has historically been thought of as driven by Th1 immune responses, which are driven by IL-2, interferon-γ and lymphotoxin-α and associated with a neutrophilic response. However, more recent third-party data has demonstrated that Th2 immune responses, which are driven by IL-4, IL-5 and IL-13 and associated with an eosinophilic response, are prominent in a subset of COPD patients. Th2 immune responses have been shown to be associated with increased airway inflammation and appear to underlie COPD in a subset of patients and related cytokines have been shown to be upregulated during exacerbations.
For stable COPD, inhaled bronchodilators (drugs that increase the size of the airways) are the mainstay of treatment. These include short-and long-acting beta-agonists (e.g., albuterol, salmeterol and formoterol), muscarinic agonists (e.g., tiotropium and aclidinium), and inhaled glucocorticoids (e.g., fluticasone and budesonide). For patients with refractory COPD, treatment options include chronic antibiotic use and DALIRESP (roflumilast). DALIRESP is the only systemic therapy approved to reduce the risk of COPD exacerbations in patients with severe COPD and a history of frequent COPD exacerbations. However, the effect is modest. A pooled analysis from two Phase 3 trials of DALIRESP in COPD patients 40 years of age and older with severe airflow limitation, bronchitis symptoms and a history of exacerbations showed a 17% reduction in moderate or severe exacerbations.
Despite recent advancements in COPD treatment, 9.4 million patients in the United States, Japan, Germany, France, Italy, Spain and the United Kingdom with moderate-to-severe disease continue to suffer and die from the disease. No biologics are currently approved for the treatment of COPD, with ensifentrine, a nebulized PDE3/4 treatment under FDA review. Given the complexity of COPD, we believe biologics targeting Th2 immune response in patients with high peripheral eosinophils show the greatest promise, as supported by DUPIXENT’s 2023 positive Phase 3 data in COPD.
However, even if approved, biologics for the treatment of COPD will be associated with many challenges, including a high frequency of injections. The dosing schedule of current biologics in development for COPD is driven by the short half-life for these agents, which provides a meaningful opportunity for a new treatment option with improved administration due to less frequent dosing. Of the biologics in development for COPD, we are not aware of any programs that have the potential to reduce dosing frequency past four weeks and the related burden of administration on patients.
Asthma Background and Current Treatment Limitations
Asthma is one of the most common non-communicable diseases and, for a substantial number of patients, has an impact on quality of life. Asthma is estimated to affect 40 million adults and 12 million children in the United States, France, Germany, Italy, Japan, Spain and the United Kingdom, with prevalence rates of 5% to 8% in many countries. Currently, the asthma market is greater than $10 billion in these seven major markets.
Asthma is a complex multifactorial disease, attributed to interactions between genetic susceptibility, host factors and environmental exposures, which result in airway inflammation, control of airway tone and reactivity. The resulting clinical presentation can vary, but can result in shortness of breath, chest tightness or pain, coughing and wheezing. In the United States, asthma accounts for approximately five million physician visits, one million emergency room visits and thousands of deaths annually.
Treatment of asthma focuses on control of asthma symptoms and reduction of asthma exacerbations. Exact treatments are based on severity and can include short-acting inhalers (e.g., short-acting beta agonists) used as needed, long-acting inhalers (e.g., long-acting beta agonists, inhaled corticosteroids) given daily or systemic medications, such as biologics.
13
Biologics, specifically, have begun to play an important role in the treatment of the 15.2 million patients with moderate-to-severe disease, largely as an add-on to inhaled medication. XOLAIR was the first biologic approved for asthma in 2003 and subsequently, an additional five biologics have been approved since 2015 (NUCALA, CINQAIR, FASENRA, DUPIXENT and TEZSPIRE). All have shown reductions in annualized exacerbation rates of approximately 50% to 60% and are dosed every two to eight weeks.
Despite advances in care, including biologics, there is still high unmet medical need for patients suffering from asthma, both in terms of reduced injection burden as well as improved efficacy.
14
Our Pipeline
Our pipeline comprises four programs being developed initially for the treatment of I&I indications, as shown below. Our two most advanced programs, APG777 and APG808, which we are initially developing for the treatment of AD and COPD, respectively, target the same mechanism of action as lebrikizumab and DUPIXENT (dupilumab), respectively. Moreover, we are evaluating APG777 in additional I&I indications, including asthma, AA, CRSwNP, CSU, EoE and PN. Our earlier-stage programs, APG990 and APG222, utilize advanced antibody engineering to target OX40L and both IL-13 and OX40L, respectively. We recently added a new program that also utilizes advanced antibody engineering for an undisclosed target. Our programs incorporate advanced antibody engineering to optimize half-life and other properties designed to overcome limitations of existing therapies. We believe each of our programs has potential for broad application across multiple I&I indications.
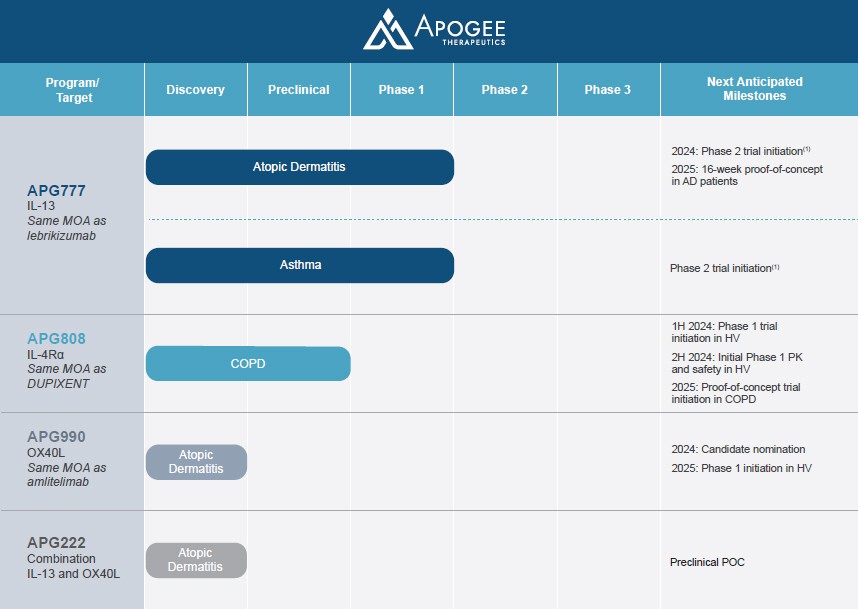
| (1) | Based on data from our Phase 1 trial of APG777 in healthy volunteers, we may initiate a Phase 2 trial in asthma and expect to further evaluate opportunities to develop APG777 for other I&I indications, including alopecia areata, chronic rhinosinusitis with nasal polyps, chronic spontaneous urticaria, eosinophilic esophagitis and prurigo nodularis. |
APG777
Our most advanced program, APG777, is an SQ mAb with YTE half-life extension technology targeting IL-13. In our head-to-head preclinical assays, our leads have demonstrated equivalent or better potency to lebrikizumab in the inhibition of IL-13 signaling. In our head-to-head studies of APG777 and lebrikizumab in non-human primates (NHPs) (cynomolgus monkeys), APG777 showed a significantly longer half-life than lebrikizumab. We expect APG777 to have a human half-life of approximately 80 to 110 days based on data from other YTE antibodies for soluble targets, which showed half-lives in humans that is three to four times greater than in NHPs, as shown in Figure 1 below.
15
Figure 1 — NHP and human half-life data of mAbs with and without the YTE amino acid modification
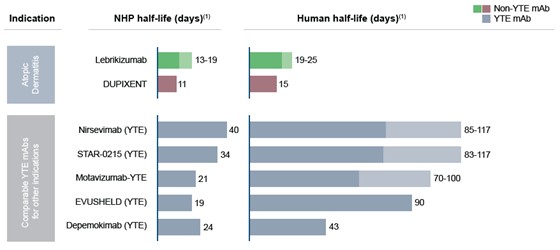
| (1) | As reported in studies conducted by the sponsor of each of these product candidates or in the label of approved products. |
Based on our PK modeling, with only a 33 day human half-life (which, to our knowledge, would be lower than the lowest half-life for a mAb with the YTE amino acid modifications reported to date), we believe we can achieve an every two-month maintenance dosing schedule at our target exposures, which are modeled based on lebrikizumab’s exposures. With only a 50 day half-life, we believe we can achieve an every three-month maintenance dosing schedule at our target exposures, which are modeled based on lebrikizumab’s exposures, each as shown in Figure 2 below.
Figure 2 — APG777 NHP half-life, predicted human half-life and predicted dosing interval
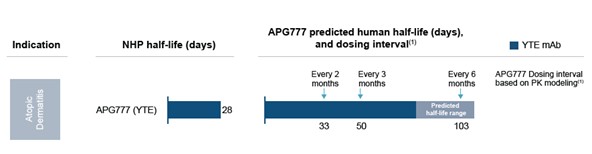
| (1) | Based on steady state PK simulations made with parameters for APG777 identical to lebrikizumab except changes in dose and kelimination. |
Compared to more frequent dosing schedules associated with existing AD therapies, every three or six month dosing, should our clinical trials be successful in demonstrating the requisite efficacy and safety profile, has the potential to be significantly more convenient for patients, enabling them to better adhere to their dosing schedule. Additionally, every three or six month dosing is expected to improve quality of life given that many patients experience “needle fatigue” and pediatric patients in particular often suffer from fear of needles.
16
In August 2023, we announced the dosing of our first participant in our first clinical trial for APG777 in Australia. The trial enrolled 40 healthy adult subjects into three SAD and two MAD cohorts. The primary endpoint is safety and a key secondary endpoint is PK. The Phase 1 trial is ongoing and we have announced initial safety and PK data from this trial. Generally, the half-life of mAbs is consistent between healthy volunteers and patients, since mAbs are degraded by endogenous catabolic processes that are not affected by disease. This gives us confidence that the PK parameters derived from the Phase 1 trial in healthy volunteers can be used effectively to model dosing regimens for subsequent Phase 2 and Phase 3 safety and efficacy trials in patients with AD and other indications. We have filed an IND in support of a Phase 1 trial in healthy volunteers in the United States for subjects of Japanese descent and have received a “study may proceed” letter from the FDA for the trial. We anticipate initiating a Phase 2 trial in AD in the United States and internationally in the first half of 2024. Pending data from the Phase 1 trial, we expect to enroll moderate-to-severe AD patients in a randomized, placebo-controlled Phase 2 trial. The primary data readout will be after 16 weeks on trial, which is common among other agents studied in AD. Primary efficacy outcomes will include, but will not be limited to, percent change from baseline in Eczema Area and Severity Index (EASI) and proportion of patients achieving an IGA scale 0/1 (assessment of clear or almost clear) and EASI-75 (change in EASI score from baseline of at least 75%). Based on our initial clinical data, we may initiate a Phase 2 trial in asthma, and expect to further evaluate opportunities to develop APG777 for other I&I indications, including AA, CRSwNP, CSU, EoE and PN.
APG808
Our second most advanced program, APG808, is an SQ extended half-life mAb targeting IL-4Rα, a target with clinical validation across eight Type 2 allergic diseases. In our head-to-head preclinical assays, our leads have demonstrated equivalent potency to DUPIXENT in the inhibition of IL-4Rα signaling. In addition, based on our preclinical studies, we believe APG808 can be dosed either every six weeks or every two months in maintenance, which, if our clinical trials are successful, would represent a significant improvement compared to first generation IL-4Rα antibodies that are dosed every two weeks. In November 2023, we finalized the nomination of a development candidate for APG808 and we have received regulatory approval to commence a first-in-human clinical trial in Australia. We anticipate that APG808 will enter the clinic in healthy volunteers in the first half of 2024 followed by a potential Phase 1b trial in asthma and/or a Phase 2 trial in COPD (pending data from the Phase 1 trial and following the submission of an IND or foreign equivalent to support such trials).
APG990
Our third program, APG990, is an SQ extended half-life mAb targeting OX40L for the treatment of AD. OX40L occurs higher up in the inflammatory pathway than IL-13 or IL4Rα and potentially broadens the impact on the inflammatory cascade. With current approved biologics only targeting two mechanisms of action (IL-13 and IL4Rα) in AD, OX40L could represent another therapeutic option for patients, especially the portion of patients who do not benefit from currently available treatments. We expect to nominate a development candidate in 2024 if we observe equivalent or better in vitro potency to other mAbs targeting OX40L in head-to-head preclinical studies, and an improved PK profile, including half-life extension, in head-to-head studies in NHPs.
APG222
Our fourth program, APG222, is one or more extended half-life SQ antibodies targeting both IL-13 and OX40L, which we believe has the potential to improve outcomes in AD over current standard of care biologic therapies. We believe that the mechanism of action of APG222, which combines blockage of OX40L and IL-13, could simultaneously decrease OX40L signaling, helping to rebalance the immune system and decrease immune cell differentiation and cytokine release, and further reduce IL-13, resulting even less immune signaling. This, in turn, could prevent certain disease-related signs and symptoms that are driven by IL-13 signaling and the downstream inflammatory cascade. We believe that blocking multiple targets, such as simultaneous inhibition of IL-13 and OX40L, could allow us to provide benefit to patients with AD and other I&I indications.
17
Additional Opportunities
We believe that each of our programs has the potential to impact multiple additional I&I indications beyond AD and COPD, including asthma, as well as AA, CRSwNP, CSU, EoE and PN. Initial structured indication prioritization has identified asthma as a leading expansion opportunity given the significant overlap with AD and the clinical unmet need for extended dosing biologics that do not sacrifice clinical benefit. Based on third-party claims data, 31% of AD patients also carry an asthma diagnosis. Based on feedback from dermatologists, we believe that there is significant value in having both indications on a label because of this overlap. Asthma is estimated to affect 40 million adults and 12 million children in the United States, France, Germany, Italy, Japan, Spain and the United Kingdom.
Our Team, Investors and Paragon Collaboration
We were founded in 2022 by leading healthcare investors Fairmount Funds and Venrock Healthcare Capital Partners and have since assembled a management team of drug developers with significant experience in clinical development. Our management team comprises industry veterans with extensive experience at biopharmaceuticals companies and proven track records in the discovery, development, manufacturing and commercialization of numerous approved therapeutics in I&I indications, including DALIRESP (Roflumilast), ILUMYA (tildrakizumab), KORSUVA (difelikafalin) and OTEZLA (apremilast), as well as more than a dozen other approved products. The team additionally has clinical and regulatory experience with late-stage I&I products currently under regulatory review, including etrasimod and lebrikizumab, manufacturing experience of biologics from IND through commercialization and financial, operational, legal and transactional experience across the biopharmaceutical industry.
Since our inception, we have raised approximately $484.4 million in net proceeds from the issuance of preferred units and sale of common stock in our initial public offering (IPO). In July 2023, we completed our IPO in which we issued and sold an aggregate of 20,297,500 shares of common stock (inclusive of 2,647,500 shares pursuant to the exercise in full of the underwriters’ option to purchase additional shares) at a public offering price of $17.00 per share, for aggregate net proceeds of $315.4 million after deducting underwriting discounts and commissions and other offering expenses.
We have exclusive development and commercialization rights to our programs through a strategic collaboration with Paragon Therapeutics, Inc. (Paragon). Together with Paragon, we intend to evaluate additional opportunities and can select additional targets as part of our discovery research collaboration. Paragon was founded by Fairmount Funds in 2021 as the firm’s discovery engine for biologics that potentially overcome limitations of existing therapies. Paragon leverages a dedicated in-house team of scientific experts in antibody development, as well as its partnership with FairJourney Biologics, to pursue unique therapeutic concepts and enable their rapid proof-of-concept validation. We consider Paragon to be a related party. See the section titled “Certain Relationships and Related Party Transactions — Our Relationship with Paragon” for additional information.
Our Strengths
We believe that our company and differentiated programs possess the following attributes that will help us successfully develop and commercialize new therapies:
| ● | Incorporate advanced antibody engineering to optimize half-life and other properties to potentially overcome limitations of existing therapies. We are focused on engineering therapies with potential for improved dosing, efficacy and safety profiles. We implement YTE or LS amino acid modifications, which have the potential to significantly improve PK profile and reduce injection burden compared to existing agents. Our antibody engineering programs are designed to improve antibody candidate attributes, including in vitro potency, bioavailability and decreased PK variability, as well as those attributes essential for manufacturability and high concentration formulation (i.e. viscosity, solubility and stability) to generate optimized antibodies. |
| ● | Leverage validated targets and mechanisms of action. Our antibody programs are designed to overcome limitations of existing therapies by targeting well-established mechanisms of action and incorporating advanced antibody engineering to optimize half-life and other properties. Our two most |
18
| advanced programs, APG777 and APG808, which we are initially developing for the treatment of AD and COPD, respectively, target IL-13 and IL-4Rα, respectively. |
| ● | Address a clear initial opportunity in AD driven by patient burden in a large addressable market. There is a large adult and pediatric patient population, with AD affecting over 40 million adults and 18 million children in the United States, France, Germany, Italy, Japan, Spain and the United Kingdom, and market penetration from existing biologics has been hindered in part due to the burden of frequent injections. Many patients experience “needle fatigue” and pediatric patients in particular often suffer from fear of needles. Estimates show that as many as two in three children and one in four adults have strong fears around needles. We believe there is clear unmet need for a new therapy that improves the clinical profile of existing agents and allows for less frequent dosing. |
| ● | Address a large unmet need in COPD, a leading cause of death with no approved biologics. COPD affects more than 32 million adults 40 years of age and older in the United States, France, Germany, Italy, Japan, Spain and the United Kingdom and is a leading cause of death worldwide. COPD patients are also much more likely to become severely ill when they are infected with other respiratory diseases, which further compounds the significant health care burden. While bronchodilators improve symptoms of COPD, they do not address the underlying inflammatory processes. There are no approved biologics available for the treatment of COPD. We believe there is a significant unmet need for a novel therapy that can effectively target an underlying source of inflammation that may be a root cause of COPD, in order to limit COPD events and improve lung capacity. |
| ● | Potential for expansion into a broad range of I&I indications, including asthma. We believe there is a path to indications beyond AD and COPD based on the common biology underlying multiple I&I indications. Based on current biologic understanding, we are evaluating APG777 in additional I&I indications, including asthma, as well as AA, CRSwNP, CSU, EoE and PN. Moreover, we believe that our programs beyond APG777 also have the potential to impact multiple additional I&I indications, including AA, CRSwNP, CSU, EoE and PN. |
| ● | Strong leadership in I&I discovery, development and commercialization, as well as manufacturing of biologics overall. We were founded in 2022 by leading healthcare investors, Fairmount Funds and Venrock Healthcare Capital Partners, and have since assembled a management team comprising industry veterans with extensive experience at biopharmaceuticals companies and with proven track records in the discovery, development, manufacturing and commercialization of numerous approved therapeutics, as well as clinical and regulatory experience with dermatologic products, including lebrikizumab. |
Our Strategy
Our goal is to become a leader in developing novel therapies for I&I indications. Our antibody programs are designed to overcome limitations of existing therapies by targeting well-established mechanisms of action and incorporating advanced antibody engineering to optimize half-life and other properties. The key elements of our strategy include:
| ● | Advancing APG777, our most advanced program, through clinical development and regulatory filings for AD. We are developing APG777 as a frontline treatment for patients with moderate-to-severe AD who have failed or have an inadequate response to topical corticosteroids. APG777 is an SQ extended half-life mAb targeting IL-13 that has been engineered to have differentiated attributes, including an extended half-life, which we expect will result in a more favorable dosing schedule, including either an every three or six months maintenance dosing schedule. In our head-to-head preclinical studies, APG777 was observed to be as potent as lebrikizumab in terms of IL-13 inhibition but with a significantly longer half-life. Based on these preclinical studies and our interim Phase 1 data we believe APG777 can be dosed either every three or six months in maintenance, which, if our clinical trials are successful, would represent a significant improvement compared to first generation IL-13 antibodies that are dosed every two to four weeks. In addition, we believe the low-volume SQ delivery |
19
| of APG777 and effector-silent backbone of the APG777 mAb will contribute to an optimized product. In August 2023, we announced the dosing of our first participant in our first clinical trial for APG777. The trial enrolled 40 healthy adult subjects into three SAD and two MAD cohorts. The primary endpoint is safety and a key secondary endpoint is PK. The Phase 1 trial is ongoing and we have announced initial safety and PK data from this trial. We anticipate initiating a Phase 2 trial in AD in the United States and internationally in the first half of 2024. We have completed GLP-compliant toxicology studies up to six months in duration, with no adverse findings at any dose level, including the highest tested dose, which was the maximum feasible dose. The completed toxicology studies were designed to facilitate moving from Phase 1 to Phase 2 clinical trials, pending regulatory approval. A primary readout at 16 weeks is common among AD agents and is recognized as an important time point for FDA approval of biologics for AD. |
| ● | Leveraging our approach of targeting known biologic drivers of I&I indications to advance APG808, our second most advanced program, into clinical development for COPD. APG808 is an SQ extended half-life mAb targeting IL-4Rα, a target with clinical validation across eight different Type 2 allergic diseases, that has been engineered to have an extended half-life as well as maintain similar potency as compared to DUPIXENT in our head-to-head in vitro assays. COPD is a heterogenous, progressive respiratory condition characterized by cough, dyspnea and airflow obstruction that affects approximately 32 million adults 40 years of age and older in the United States, France, Germany, Italy, Japan, Spain and the United Kingdom. Based on our preclinical studies, we believe APG808 can be dosed either every six weeks or every two months in maintenance, which would represent a significant improvement compared to first generation IL-4Rα antibodies, that are dosed every two weeks. In November 2023, we finalized the nomination of a development candidate for APG808 and we have received regulatory approval to commence a first-in-human clinical trial in Australia. We anticipate that APG808 will enter the clinic in healthy volunteers in the first half of 2024 followed by a potential Phase 1b trial in asthma and/or a Phase 2 trial in COPD (pending data from the Phase 1 trial and following the submission of an IND or foreign equivalent to support such trials). |
| ● | Advancing our programs targeting OX40L and the dual inhibition of OX40L and IL-13. Our third program, APG990, is a mAb targeting OX40L for the treatment of AD. OX40L occurs higher up in the inflammatory pathway than IL-13 or IL-4Rα and potentially broadens the impact on the inflammatory cascade. With current approved biologics only targeting two mechanisms of action (IL-13 and IL4Rα) in AD, OX40L could represent another therapeutic option for patients, especially the portion of patients who do not benefit from currently available treatments. We are engineering APG990 to have additional favorable properties compared to other mAbs targeting OX40L, including an extended half-life. We believe we are the only company applying half-life extension technology to the OX40L class. We plan on nominating a development candidate in this program in 2024. Our fourth program, APG222, is focused on the dual inhibition of OX40L and IL-13, which we believe could result in a more durable response than inhibition of either target alone across a broader range of I&I indications. We believe that blocking multiple targets, such as simultaneous inhibition of IL-13 and OX40L, could allow us to provide benefit to patients with AD and other I&I indications. |
| ● | Maximizing the potential of our programs through indication expansion beyond AD and COPD. We believe our APG777 and APG808 programs have the potential to treat I&I indications driven by Th2 immune response, such as asthma, as well as AA, CRSwNP, CSU, EoE and PN. In addition, we believe our APG990 and APG222 programs have the potential to treat I&I indications driven by both Th1 and Th2 immune responses. Other therapies with which our most advanced programs share a mechanism of action have demonstrated success in targeting indications driven by Th2 immune response. Leveraging different mechanisms of action for the same indications may allow us to treat a broader patient population. We have taken a systematic approach to prioritizing indications and plan on leveraging clinical data and knowledge from our Phase 1 trials in APG777 to launch proof-of-concept Phase 2 trials in indications with strong scientific rationale in large markets or areas of unmet need. Based on our initial clinical data, we may initiate a Phase 2 trial in asthma, and expect to further evaluate |
20
| opportunities to develop APG777 for other I&I indications, including AA, CRSwNP, CSU, EoE and PN. |
| ● | Expanding existing and evaluating new collaborations to broaden the impact we can have for patients living with I&I indications. Our strategic collaboration with Paragon has resulted in us obtaining exclusive development and commercialization rights for our initial programs. Together with Paragon, we intend to evaluate additional opportunities and can select additional targets as part of the discovery research collaboration. In addition, we plan to evaluate additional opportunities to enhance our capabilities and expand our development pipeline or provide development or commercialization capabilities that complement our own. We recently added a new program that also utilizes advanced antibody engineering for an undisclosed target. |
Biologics are Common Treatments for I&I Diseases
Over the last two decades, biologics have become more common for the treatment of a wide range of I&I indications and remain the core therapeutic modality today. New treatments for I&I indications have largely been driven by biologics, which accounted for nearly 90% of these I&I product revenues. Given the overlapping mechanistic drivers of many I&I indications, indication expansion remains a consistent hallmark of many I&I products. Broadly, mAbs have been developed to target both diseases driven by T helper type 1 (Th1) immune responses, which involve IL-2, interferon-γ and lymphotoxin-α and an associated neutrophilic response, and diseases driven by T helper type 2 (Th2) immune responses, which involve IL-4, IL-5 and IL-13 and an associated eosinophilic response.
As one example, psoriasis, with a moderate-to-severe population estimated to be approximately 9.2 million patients, had the first biologic approved in 2008 and an additional six biologics approved from that time to 2023. Only one other indication, psoriatic arthritis, has more approved biologics.
By contrast, the moderate-to-severe AD population, which is estimated to be approximately 25.1 million patients, has only two approved biologics, which leaves a large unmet need for patients with AD.
DUPIXENT is an example of the success of approved therapeutics. Since its approval for the treatment of AD in 2017, DUPIXENT has also been approved in asthma, CRSwNP, EoE and PN and is being clinically developed in allergic bronchopulmonary aspergillosis, allergic fungal rhinosinusitis, bullous pemphigoid, chronic pruritis of unknown origin, cold inducible urticaria, COPD, chronic rhinosinusitis sans nasal polyps and CSU. Although our most advanced program APG777 targets the same mechanism of action as DUPIXENT, there is no assurance that our clinical trial results will achieve similar clinical trial results with respect to safety and/or efficacy or that APG777 will achieve FDA approval or commercial success.
Overview of AD
Disease Overview
AD, the most common subtype of eczema, is a chronic inflammatory skin disorder that affects individuals of all ages and races. AD affects individuals living in geographic regions worldwide. AD is characterized by pruritic (itchy), erythematous (red) and often excoriated (damaged) skin lesions, which are most often located on the neck, inner elbows and behind the knees. The specific cause of AD is unknown; however, research has shown that genetics, the immune system and the environment all play a role in the disease. AD can significantly impact quality of life, leading to sleep disturbance, psychological distress, elevated infection risk and chronic pain. AD is frequently associated with other atopic manifestations such as food allergy, allergic rhinitis (also known as hay fever) and asthma. AD is characterized by a Th2 response, which describes Th2 cells that produce small proteins called cytokines, like IL-13, which regulate inflammation, immune response and tissue repair.
AD usually begins in childhood; however, patients can become affected with this inflammatory disease at any age. For some people, AD improves by adulthood, but for many, it can be a lifelong illness. It is estimated that 40 million adults and 18 million children in the United States, France, Germany, Italy, Japan, Spain and the United Kingdom are affected by AD. Approximately 40% of all patients have moderate-to-severe disease. The incidence of AD has increased two-to three-fold in industrialized nations since the 1970s, with approximately 15% to 20% of children and 1% to 3% of adults affected worldwide.
21
Overview of Current Treatment Options
There is no cure for AD and many people have difficulty controlling the disease. AD patients work with a dermatologist to determine treatment options that can bring their symptoms under control. For less extensive disease (i.e., mild-to-moderate AD), treatment is primarily topical corticosteroids and targeted topical treatments (e.g., a topical Janus kinase (JAK) inhibitor). For more extensive disease (i.e., moderate-to-severe AD), mAbs have emerged as the preferred frontline therapy in most adult and pediatric patients that is not controlled by topical therapies. Avoiding environmental and stress triggers, increased skin care regimen and dietary and lifestyle changes may also be part of the treatment recommendations.
Treatment of AD is specific to severity of disease. The primary goal of AD management is to control symptoms and prevent flares. Outcomes in AD are primarily reported using two measures: Eczema Area and Severity Index (EASI) and Investigator’s Global Assessment (IGA). Other measures are used as well to gain a comprehensive understanding of a treatment’s impact on AD patients.
EASI assesses key signs of eczema over four natural anatomic divisions of the body (the head and neck, the trunk, the upper extremities and the lower extremities) across the parameters of erythema (redness), induration (thickness), excoriation (scratching), lichenification (lined skin) and percentage of the region affected. The EASI score range is from 0 to 72 with 72 being the most severe. Zero is considered clear, 0.1 to 1.0 is considered almost clear, 1.1 to 7.0 is considered mild, 7.1 to 21.0 is considered moderate, 21.1 to 50.0 is considered severe and above 50.1 is considered very severe. Proportion of patients achieving EASI-75, an improvement of at least 75% from baseline on the EASI, or EASI-90, an improvement of at least 90% from baseline on the EASI, are key outcome measures in clinical trials of patients with moderate-to-severe AD. The extent and severity of AD as measured by the EASI is shown in Figure 3 below.
22
Figure 3 — Eczema Area and Severity Index
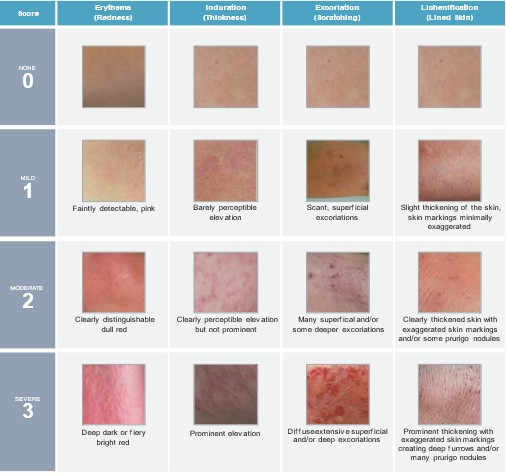
Source: Harmonising Outcome Measures for Eczema (HOME). EASI Guidance (presentation). Accessed April 28, 2023.
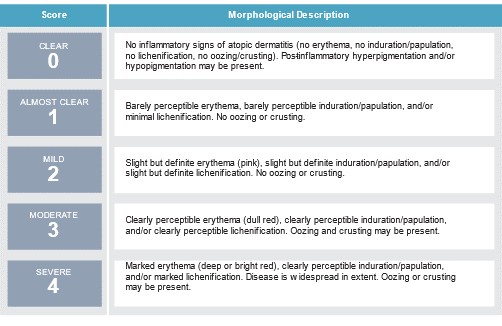
As shown in Figure 4 below, IGA is a five-point scale (scale 0 to 4) that uses clinical characteristics to assess overall disease severity at any given timepoint. Typical enrollment for clinical trials for moderate-to-severe AD patients requires an IGA score of three or four. As an outcome measure, IGA is looked at as the number of patients achieving an IGA score of 0 or 1 with at least a two point decrease in IGA from baseline, referred to as proportion of patients with IGA 0/1.
23
Figure 4 — Investigator’s Global Assessment
For patients with mild-to-moderate AD, topically applied corticosteroids and emollients are the mainstay of therapy with the exact regimen based on severity, body area involved and degree of skin inflammation. Options include topical corticosteroids, topical calcineurin inhibitors (tacrolimus or pimecrolimus), crisaborole or topical ruxolitinub.
AD patients with persistent moderate-to-severe disease may require systemic treatment. mAbs have emerged as the preferred frontline therapy in most adult and pediatric patients with moderate-to-severe AD that is not controlled by topical therapies. There are two FDA-approved mAbs, DUPIXENT and ADBRY, labeled to treat moderate-to-severe AD that is inadequately controlled by topical corticosteroids. Additionally, lebrikizumab is an investigational mAb being developed by Eli Lilly and Company designed to inhibit the IL-13 pathway and is currently under review for approval by the FDA and has been approved by the European Medicines Agency (EMA) and the Pharmaceuticals and Medical Devices Agency (PMDA), in Japan.
DUPIXENT is indicated for the treatment of adult and pediatric patients aged six months and older with moderate-to-severe AD whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. It can be used with or without topical corticosteroids. DUPIXENT is a fully human mAb that inhibits the signaling of the IL-4 and IL-13 pathways. For adults with AD, DUPIXENT is dosed via SQ injection with an initial loading dose requiring two injections, followed by one injection every two weeks for adults with AD. For pediatric patients, it is dosed as one or two injections every two to four weeks depending on age and weight. DUPIXENT was studied in over 2,800 patients across multiple pivotal trials and demonstrated clinically meaningful improvements at Week 16 in adult, adolescent and pediatric patients.
ADBRY is indicated for the treatment of moderate-to-severe AD in adult patients whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. It can be used with or without topical corticosteroids. ADBRY is a fully human, high-affinity mAb that targets IL-13. It selectively inhibits IL-13, preventing IL-13-induced immune responses in the skin. It is dosed via SQ injection with an initial loading dose requiring four injections, followed by two injections every two weeks for 16 weeks and then, for select patients, maintenance injections every month may be considered. ADBRY was evaluated in nearly 2,000 patients with AD in three pivotal trials. Across the three trials, ADBRY demonstrated improvements in both skin clearance and lesion extent and severity at Week 16.
24
Lebrikizumab is an emerging treatment with a similar mechanism of action to both DUPIXENT and ADBRY. It is an investigational mAb being developed by Eli Lilly and Company that is designed to inhibit the IL-13 pathway and currently under regulatory review for approval in the United States and has been approved in the European Union and Japan. In three Phase 3 clinical trials, SQ administration of lebrikizumab was dosed every two weeks in the induction phase (first 16 weeks of treatment) and every two or four weeks in the maintenance phase (from 16 weeks to 52 weeks). Lebrikizumab met all primary and key secondary endpoints at Week 16 in Phase 3 trials. The most commonly reported adverse events (AE) were conjunctivitis, common cold and headache.
For patients for which biologics such as DUPIXENT or ADBRY do not provide adequate control of moderate-to-severe AD, systemic JAK inhibitors may be recommended. RINVOQ (upadacitinib) or CIBINQO (abrocitinib) are both FDA-approved treatments for AD that may be prescribed to patients who do not respond to topical prescription treatments. Despite their effectiveness and convenient oral administration, these therapies are associated with serious risk of life-threatening side effects and carry boxed warnings. FDA labels for these therapies require patients to step-through (prove non-responsive or inability to tolerate) a biologic before systemic JAK inhibitors are indicated. Serious side effects can include infections, mortality, malignancies, cardiovascular events, thrombosis, hypersensitivity, gastrointestinal perforation, various lab abnormalities and embryo-fetal toxicity. These toxicity challenges have limited clinical use of systemic JAK inhibitors for AD where patients are generally healthy and young. Systemic JAK inhibitors represented just 7% of the AD market in 2022.
An emerging mechanism in treatments for AD is targeting OX40 or OX40L, which occur higher up in the inflammatory pathway than IL-13 or IL-4Rα and potentially broadens the impact on the inflammatory cascade. OX40L is the ligand for OX40. OX40L is expressed on antigen presenting cells and its interaction with OX40 causes the accumulation of T cells by providing a survival signal. OX40L, by playing a role in activating T cells and reprogramming them into inflammatory subsets, contributes to immune overactivation in AD and other inflammatory conditions. Additionally, OX40L activation of OX40 inhibits the expression of FOXP3 and the inhibitory function of regulatory T (Treg) cells. Treg cells suppress immune response, which leads to worse symptoms in inflammatory conditions. Therefore, OX40L blockade may lead to clinical benefit in AD and other inflammatory conditions by first suppressing inflammatory T cell activation, and next by increasing the proliferation of Treg cells, which can serve to further reduce inflammatory cells. Amlitelimab, which targets OX40L, and rocatinlimab, which targets OX40, have both demonstrated promising Phase 2 data in AD.
Addressing the Limitations of Current Biologics
Despite recent advancements in AD treatment, a significant number of patients continue to suffer from active disease. Today’s treatments are associated with many challenges, including a high frequency of injections that may lead to poor patient compliance. The dosing schedule of current biologics is driven by the short half-life for these agents, which provides a meaningful opportunity for a new treatment option with improved administration due to less frequent dosing.
High injection burden coupled with needle fatigue reported in adult patients has impacted the use of currently approved AD biologics. Based on a peer-reviewed third-party study of real world use published in the Journal of the American Academy of Dermatology, more than 20% of patients discontinue treatment with DUPIXENT within six months of starting therapy. Pediatric patients in particular often suffer from fear of needles, which limits the use of current biologics in a large and growing patient population.
In 2023, we conducted a single-blinded market research survey of 25 practicing dermatologists in 14 states in the United States, with the assistance of an expert search network.
Dermatologists were selected based on years of experience in the field (four or more years of practice post residency or fellowship training), number of AD patients treated (30 or more AD patients seen per month), experience prescribing biologic therapies in AD (10% or more of AD patients on biologics) and no previous contact with us. We conducted approximately 30-minute interviews using standardized questions to solicit sentiments towards a potential new product offering with every three month dosing in maintenance and the same efficacy and safety as DUPIXENT, which was presented as a blinded Target Product Profile (the TPP). The dermatologists selected for the survey have an average of 20 years in practice, treat an average of 88 AD patients per month and see a mix of both adult and pediatric patients.
25
In the interviews, dermatologists described how they would incorporate the TPP in treatment algorithms for biologic naïve patients (i.e., patients who have never taken a biologic treatment, but qualify based on failure to topical therapies) and biologic-experienced patients (i.e., patients who are either currently or have previously used a biologic therapy for AD). On average, dermatologists indicated they expect approximately 92% of their biologic patients would start a product with the TPP as frontline treatment. For patients currently or previously on biologic therapy, dermatologists estimated approximately 57% would switch to a product with the TPP.
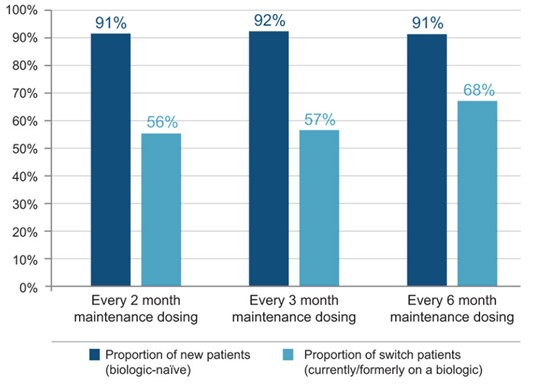
Dermatologists were then asked how their intent to use a product with the TPP would change if (i) it was dosed every two months in the maintenance setting, or (ii) it was dosed every six months in the maintenance setting. As shown in Figure 5 below, results for the every two month dosing were consistent with the every three month dosing. With every two month dosing, dermatologists on average indicated they would prescribe a product with the TPP to 91% of their biologic naïve patients and they estimated 56% of their patients currently or previously on biologic therapy would switch to a product with the TPP. As shown in Figure 5 below, results for the every six month dosing showed a greater proportion of patients would switch from a current biologic than for the every three month dosing. With every six month dosing, dermatologists on average indicated they would prescribe a product with the TPP to 91% of their biologic naïve patients and they estimated 68% of patients currently or previously on biologic therapy would switch to a product with the TPP.
Figure 5 — Intent to use a product with the APG777 Target Product Profile with every two, three or six month maintenance dosing and equivalent efficacy and safety to DUPIXENT
We are not aware of any programs in development in AD that have the potential to reduce dosing frequency past four weeks and the related burden of administration on patients. A more convenient dosing schedule is especially important for pediatric patients, which has the potential to expand the market significantly.
26
Overview of COPD
Disease Overview
COPD is a heterogenous, progressive respiratory condition characterized by cough, dyspnea and airflow obstruction. It is estimated that approximately 10% of the global population 40 years of age and older have COPD, and in 2019 (prior to the COVID–19 pandemic), COPD was the third leading cause of death globally. In the United States, over 150,000 people die of COPD each year.
Three symptoms of COPD are dyspnea (difficulty breathing), cough and sputum (coughed-up phlegm) production. There are several possible linked risk factors to COPD including cigarette smoke, environmental factors (e.g., pollution and occupational exposures), airway responsiveness, atopy, asthma, infections and genetics.
COPD has historically been thought of as driven by Th1 immune responses, which are driven by IL-2, interferon-γ and lymphotoxin-α and associated with a neutrophilic response. However, more recent third-party data has demonstrated that Th2 immune responses, which are driven by IL-4, IL-5 and IL-13 and associated with an eosinophilic response, are prominent in a subset of COPD patients. Th2 immune responses have been shown to be associated with increased airway inflammation and appear to underlie COPD in a subset of patients and related cytokines have been shown to be upregulated during exacerbations.
Overview of Current Treatment Options
For stable COPD, inhaled bronchodilators (drugs that increase the size of the airways) are the mainstay of treatment. These include short-and long-acting beta-agonists (e.g., albuterol, salmeterol and formoterol), muscarinic agonists (e.g., tiotropium and aclidinium), and inhaled glucocorticoids (e.g., fluticasone and budesonide). For patients with refractory COPD, treatment options include chronic antibiotic use and DALIRESP (roflumilast). DALIRESP is the only systemic therapy approved to reduce the risk of COPD exacerbations in patients with severe COPD and a history of frequent COPD exacerbations. However, the effect is modest. A pooled analysis from two Phase 3 trials of DALIRESP in COPD patients 40 years of age and older with severe airflow limitation, bronchitis symptoms and a history of exacerbations showed a 17% reduction in moderate or severe exacerbations.
Despite recent advancements in COPD treatment, a significant number of patients continue to suffer and die from the disease. No biologics are currently approved for the treatment of COPD, with ensifentrine, a nebulized PDE3/4 treatment under FDA review. Given the complexity of COPD, we believe biologics targeting Th2 immune response in patients with high peripheral eosinophils show the greatest promise, as supported by DUPIXENT’s recent positive Phase 3 data in COPD. Specifically, the topline data from DUPIXENT’s Phase 3 BOREAS trial, which enrolled COPD patients with elevated peripheral eosinophils (≥300 cell/μL), showed a significant reduction of 30% in moderate-to-severe acute exacerbations of COPD (p=0.0005), as well as improved lung function and quality of life. NOTUS, the second Phase 3 trial, confirmed the BOREAS findings with a 34% reduction in moderate-to-severe exacerbations at 52 weeks (p=0.0002).
Addressing the Limitations of Current Biologics
However, even if approved, biologics for the treatment of COPD will be associated with many challenges, including a high frequency of injections. The dosing schedule of current biologics in development for COPD is driven by the short half-life for these agents, which provides a meaningful opportunity for a new treatment option with improved administration due to less frequent dosing. Of the biologics in development for COPD, we are not aware of any programs that have the potential to reduce dosing frequency past four weeks and the related burden of administration on patients.
27
Overview of Asthma
Disease Overview
Asthma is one of the most common non-communicable diseases and, for a substantial number of patients, has an impact on quality of life. Asthma is estimated to affect 40 million adults and 12 million children in the United States, France, Germany, Italy, Japan, Spain and the United Kingdom, with prevalence rates of 5% to 8% in many countries. Currently, the asthma market is greater than $10 billion in these seven major markets. Asthma is a complex multifactorial disease, attributed to interactions between genetic susceptibility, host factors and environmental exposures, which result in airway inflammation, control of airway tone and reactivity. The resulting clinical presentation can vary, but can result in shortness of breath, chest tightness or pain, coughing and wheezing. In the United States, asthma accounts for approximately five million physician visits, one million emergency room visits and thousands of deaths annually.
Overview of Current Treatment Options
Treatment of asthma focuses on control of asthma symptoms and reduction of asthma exacerbations. Exact treatments are based on severity and can include short-acting inhalers (e.g., short-acting beta agonists) used as needed, long-acting inhalers (e.g., long-acting beta agonists, inhaled corticosteroids) given daily or systemic medications, such as biologics.
Biologics, specifically, have begun to play an important role in the treatment of moderate-to-severe asthma, largely as an add-on to inhaled medication. XOLAIR was the first biologic approved for asthma in 2003 and subsequently, an additional five biologics have been approved since 2015 (NUCALA, CINQAIR, FASENRA, DUPIXENT and TEZSPIRE). All have shown reductions in annualized exacerbation rates of approximately 50% to 60% and are dosed every two to eight weeks.
Despite advances in care, including biologics, there is still high unmet medical need for patients suffering from asthma, both in terms of reduced injection burden as well as improved efficacy
Our Solution: Building Differentiated Biologics
We are engineering therapies for AD, COPD, asthma and other related I&I indications. Our two most advanced programs, APG777 and APG808, target IL-13 and IL4Rα, respectively, and are designed to overcome limitations of frequent dosing associated with currently available treatments. With respect to our earlier-stage programs, APG990 utilizes advanced antibody engineering to target OX40L, a target with potentially broad application for inflammatory conditions, and APG222 utilizes advanced antibody engineering to target both IL-13 and OX40L. We recently added a new program that also utilizes advanced antibody engineering for an undisclosed target.
Our programs incorporate advanced antibody engineering approaches, and are designed to optimize for half-life extension, in vitro potency, bioavailability and decreased PK variability, as well as those attributes essential for manufacturability and high concentration formulation (i.e. viscosity, solubility and stability), potentially improving on each of those qualities over existing, non-optimized antibodies.
We utilize and test a number of half-life extension technologies, including YTE and LS, to identify the optimal candidate to advance against each target. YTE amino acid modifications are a triple modification (M252Y/S254T/T256E) introduced into the antibody, while LS amino acid modifications are a double modification (M428L/N434S).
Our most advanced program, APG777, leverages YTE amino acid modification half-life extension technology and is SQ mAb targeting IL-13. After regulatory approval, we initiated a Phase 1 clinical trial of APG777 in healthy volunteers in August 2023.
Our second most advanced program, APG808, leverages half-life extension technology and is an SQ mAb targeting IL-4Rα. In November 2023, we finalized the nomination of a development candidate for APG808 based on equivalent in vitro potency compared to DUPIXENT and other improved drug properties, including half-life extension in our head-to-head preclinical studies and we have received regulatory approval to commence a first-in-human clinical trial in Australia.
28
Our third program, APG990, leverages half-life extension technology and is an SQ mAb targeting OX40L. We expect to nominate a development candidate in 2024 if we observe equivalent or better in vitro potency compared to other mAbs targeting OX40L and other improved drug properties, including half-life extension in our head-to-head preclinical studies.
Our fourth program, APG222, targets both IL-13 and OX40L using one or more SQ mAbs that leverage half-life extension technology. We believe targeting both IL-13 and OX40L has the potential to improve clinical outcomes in AD over current standard of care biologic therapies.
Half-Life Extension and Antibody Engineering Technologies
Our antibody engineering programs are designed to improve antibody candidate attributes, including half-life extension, in vitro potency, bioavailability and decreased PK variability, as well as those attributes essential for manufacturability and high concentration formulation (i.e. viscosity, solubility and stability) to generate optimized antibodies. Each of our programs utilize YTE or LS amino acid modifications and are designed to significantly extend the half-life of antibodies by supercharging the body’s innate recycling mechanism for antibodies. Antibodies in circulation are naturally taken up by cells and degraded, which limits the half-life in circulation. Cells have evolved a mechanism to spare certain antibodies from degradation and return them to circulation, thus extending their half-life. This recycling mechanism works via the neonatal Fc receptor (FcRn). Antibodies are internalized into a cell via pinocytosis, the process of extracellular fluid and substances (including antibodies), being invaginated, or brought into, the cell resulting in an internalized vesicle. The process of pinocytosis is nonspecific, meaning uptake of fluid and substances is not regulated in any way. The internal vesical, or endosome, fuses with lysosomes, the specialized organelle or area in the cell that is able to break down and digest biomolecules. When antibodies are taken up by lysosomes, they can bind to FcRn on the membrane surface of the endosome in the acidic conditions within the lysosomes, which spares them from degradation. The antibody can then be returned to the cell surface with the membrane of the endosome and released back into circulation. This process is shown in Figure 6 below.
Figure 6 — Our half-life extended mAbs are designed to be recycled back into circulation more readily so drug exists at much higher levels for longer duration of effect
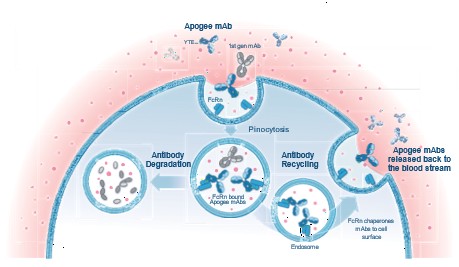
This natural mechanism of antibody recycling has been exploited by antibody engineers. Specifically, modifications to antibodies that increase the affinity for FcRn were developed in the early 2000s. One such modification was to the fragment crystallizable region (Fc region) of antibodies in the form of a triple modification:
29
M252Y/S254T/T256E. Referred to as “YTE amino acid modifications” due to the three amino acid changes, this triple modification has been observed to result in an approximately ten-fold increase in binding affinity of antibodies to FcRn compared to antibodies without YTE amino acid modifications in third-party studies. The increased affinity of antibodies with YTE amino acid modification for FcRn results in increased antibody recycling (i.e., less lysosomal degradation) and a prolonged half-life. LS is a double amino acid modification (M428L/N434S) that works similarly to YTE amino acid modifications and increases the antibodies affinity for FcRn, which leads to a prolonged half-life compared to wild type counterparts.
There is the potential for at least two significant benefits to antibodies that are engineered with a half-life extension amino acid modification:
| ● | Significantly increased half-life, leading to the potential for greater duration of effect. The typical half-life for an IgG antibody is typically 11 to 30 days. By contrast, IgG antibodies with half-life extension amino acid modifications, such as YTE, have the potential to increase human half-life three-to four-fold compared to non-YTE mAbs, with half-lives observed to often exceed 100 days in third-party trials. The half-life extension allows the drug to remain in the body for a longer period of time and therefore have additional action. The prolonged half-life results in more sustained concentrations, or levels of drug in the blood stream, often measured in area under the curve (AUC) between two time points. |
| ● | Decreased variability in drug exposure from person to person, leading to the potential for more consistent clinical outcomes. For example, the magnitude of half-life extension that YTE amino acid modification confers has been observed to be relatively consistent from person to person in third-party trials. For this reason, the typical factors that can vary amongst different people and give rise to variability in drug exposure from person to person have less of an impact for YTE antibodies. Decreased variability in exposure from one person to the next means the amount of drug in the body is more similar from one person to the next, which could help to better predict how people respond to the drug. |
Half-life extension amino acid modifications, such as YTE and LS amino acid modifications, have been introduced to monoclonal IgG1 in a wide variety of human therapeutics.
YTE amino acid modifications have been introduced in numerous mAbs in late-stage ongoing clinical trials (e.g., depemokimab) and completed trials (e.g., motavizumab-YTE and ziltivekimab), as well as one approved product, BEYFORTUS. The targets of these antibodies include cytokines (IL-5 for depemokimab and IL-6 for ziltvekimab) and viruses (RSV for motavizumab-YTE and BEYFORTUS).
Similarly, LS amino acid modifications have been introduced into numerous mAbs in early-and late-stage clinical trials (e.g., VIR-7831, VIR-2482 and VRC01LS) as well as approved products (e.g., ULTOMIRIS® and XEVUDY). The targets of these antibodies include complement (C5 for ULTOMIRIS) and viruses (SARS-CoV-2 for XEVUDY, HbsAg for VIR-2482 and HIV for VRC01LS).
30
The safety and immunogenicity profile of YTE-or LS-modified mAbs compares favorably to non-YTE or non-LS modified mAbs with identical targets
For example, in third-party clinical trials, the safety profile of motavizumab-YTE was comparable to that of the parent antibody, motavizumab, with no significant difference in the occurrence of self-limited AEs. Similarly, a Phase 1 trial of depemokimab, an anti-IL-5 with a YTE amino acid modifications for half-life extension, was notable for its overall benign safety profile and similar AE rate compared to mepolizumab (NUCALA), an anti-IL-5 without half-life extension. Finally, among infants with prematurity or other RSV risk factors, serious adverse event (SAE) frequency and type were comparable between nirsevimab (YTE) and palivizumab (non-YTE)-dosed infants.
In human subjects, we are not aware of administration of mAbs bearing YTE amino acid modifications being associated with greater immunogenicity than unmodified mAbs. For example, similar levels of anti-drug antibodies (ADAs) have been measured in motavizumab as compared to motavizumab-YTE. As another example, nirsevimab, a mAb with YTE amino acid modifications targeting RSV, exhibited lower levels of ADAs than an antibody for the same target without YTE amino acid modifications (palivizumab).
Similarly, administration of mAbs bearing LS amino acid modifications does not appear to confer any additional safety risk or immunogenicity risk. For example, ULTOMIRUS (ravulizumab) is an LS modified version of SOLIRIS (eculizumab). In third-party clinical trials, the AE profile of ULTOMIRUS and SOLIRIS were shown to be a similar in a head-to-head study and one ADA-positive sample was found in each treatment arm.
31
APG777
Our most advanced program, APG777, leverages YTE amino acid modifications half-life extension technology and is an SQ mAb targeting IL-13. We plan to evaluate APG777 in AD, as well as a number of expansion indications, including asthma.
In our head-to-head preclinical studies of APG777 and lebrikizumab in NHPs APG777 showed a significantly longer half-life than lebrikizumab. In these studies, APG777’s half-life was 27.6 days, as compared to 18.0 days for lebrikizumab based on cumulative fit models across SQ and IV groups for each compound and as shown in Figure 7 below.
Figure 7 — Head-to-head comparison of NHP PK for APG777 and lebrikizumab
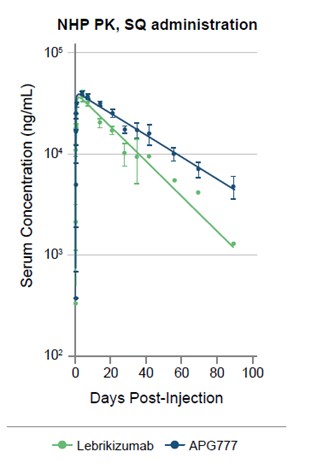
Note: N=3 per group. Two of three NHPs in the lebrikizumab arm developed ADAs by day 40 (datapoints associated with ADAs are excluded).
32
We expect APG777 to have a human half-life of approximately 80 to 110 days based on data from other YTE antibodies for soluble targets, which provided evidence that half-life in humans is three to four times greater than in NHPs. As shown in Figure 8 below, this is largely consistent with previous clinical observations of mAbs with YTE amino acid modification, however, there can be no assurance that APG777 will have similar or comparable results.
Figure 8 — YTE mAbs extended half-life in NHPs has consistently translated to significantly greater human half-life than non-YTE mAbs
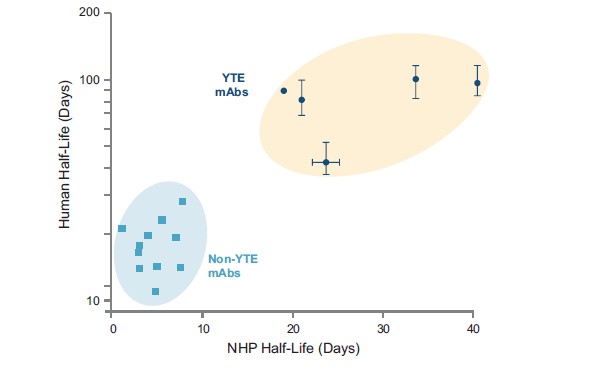
Based on our PK modeling, with only a 33-day human half-life (which, to our knowledge, would be lower than the lowest half-life for a mAb with the YTE amino acid modifications reported to date), we believe we can achieve an every two month maintenance dosing schedule at our target exposures, which are modeled based on lebrikizumab’s exposures. With only a 50-day half-life, we believe we can achieve an every three month maintenance dosing schedule at our target exposures, which are modeled based on lebrikizumab’s exposures. Compared to more frequent dosing schedules associated with existing AD therapies, every three or six month dosing, should our clinical trials be successful in demonstrating the requisite efficacy and safety profile, has the potential to be significantly more convenient for patients, enabling them to better adhere to their dosing schedule. Additionally, every three or six month dosing improves quality of life given that many patients experience “needle fatigue” and pediatric patients in particular often suffer from fear of needles.
In August 2023, we initiated a Phase 1 trial of APG777 in healthy volunteers in Australia. We have announced initial SQ PK and safety data from this trial. Generally, the half-life of mAbs is consistent between healthy volunteers and patients since mAbs are degraded by endogenous catabolic processes and are not subject to the same drug-drug interaction potential of many traditional small molecules. Consequently, this gives us confidence that the PK parameters derived from the Phase 1 trial in healthy volunteers can be used to effectively model dosing regimens in the subsequent Phase 2 and Phase 3 safety and efficacy trials in patients with AD and other I&I indications.
We plan to initiate a Phase 2 trial in patients with AD in the first half of 2024. We plan to enroll moderate-to-severe AD patients in a randomized, placebo-controlled Phase 2 trial. The primary data readout will be after 16 weeks on trial, which is common among other agents studied in AD. Primary outcomes will include, but will not be limited to, percent change from baseline in EASI and proportion of patients achieving an IGA scale 0/1 and EASI-75.
33
At the end of the primary 16-week trial, patients will rollover to continue treatment on either a maintenance or open-label extension trial. In addition, based on our initial clinical data, we may initiate a Phase 2 trial in asthma, and expect to further evaluate opportunities to develop APG777 for other I&I indications, including AA, CRSwNP, CSU, EoE and PN.
APG777’s target, IL-13, has no known non-disease function
APG777’s target, IL-13, is a cytokine with no known non-disease function such as growth or metabolism. IL-13 is a cytokine primarily produced by activated Th2 cells. Its primary role in normal physiology is to generate a Th2 response to parasitic infection. While increased IL-13 production has been implicated in a variety of indications, such as AD, asthma and certain types of cancer, the absence of IL-13 in animal models has not been tied to disease. In third-party studies, mice that lacked IL-13 (IL-13−/− knockout mice) were observed to be healthy and exhibited normal behavior under typical laboratory conditions.
IL-13 signaling begins with the binding of IL-13 to IL-13Rα1, forming an inactive complex that then binds to IL-4Rα to form the complete, active receptor heterodimer. The active receptor recruits members of the JAK family of enzymes, triggering a signaling cascade that results in the expression of pro-inflammatory cytokines and leads to an immune response by the body.
IL-13 is a known driver of AD pathogenesis and broader I&I indications
The pathogenesis, or underlying molecular cause of the disease, of AD involves both genetic and environmental factors that interact to produce a complex immune response. Genetic factors associated with AD include variations in genes that regulate the immune response, such as those encoding for IL-4, IL-13 and IL-31.
AD is characterized by a Th2 response, which describes Th2 cells, a subset of white blood cells, that produce small proteins called cytokines, like IL-13, which regulate inflammation, immune response and tissue repair. Overactivation of Th2 cells contributes to several allergic diseases, including AD, and chronic dysregulation of cytokine production and signaling leads to chronic inflammation and skin barrier dysfunction in AD.
34
More specifically, IL-4, IL-5 and IL-13 are all associated with Th2 response and IL-4 and IL-13 play a key role in the impairment of the skin barrier in AD, which leads to transepidermal water loss and susceptibility to irritants and allergens, creating an inflammatory positive feedback loop that is characteristic of AD. In third-party studies, IL-13 was observed to be elevated in skin lesions of patients with both acute and chronic AD compared to uninvolved skin and normal skin (see left panel of Figure 9 below) and was shown to be elevated to a greater extent than IL-4 in the skin of AD patients (see right panel of Figure 9 below).
Figure 9 — Cytokine expression in AD and Non-AD skin samples in third-party studies
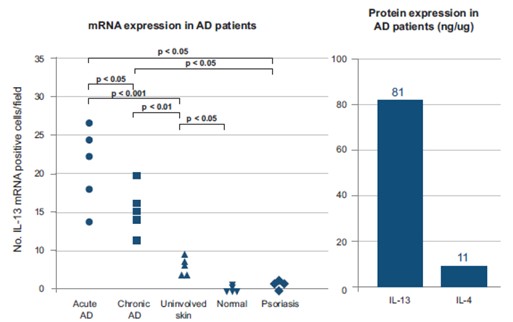
Sources: Hamid Q et al. J Allergy Clin Immunol. 1996 Jul;98(1). Koppes SA et al. Int Arch Allergy Immunol. 2016;170(3).
35
IL-13 signals through the formation of the IL-13Rα1IL4Rα heterodimer. In turn, the active IL-13Rα1IL4Rα heterodimer, through a signaling cascade, leads to skin barrier defects, immune cell recruitment, tissue inflammation, lichenification (skin thickening) and pruritis (skin itching). APG777 is designed to interrupt the heterodimer formation and thus disrupt IL-13 signaling as shown in Figure 10 below.
Figure 10 — APG777 is designed to disrupt IL-13 signaling by preventing the formation of the IL-13Rα1IL4Rα heterodimer
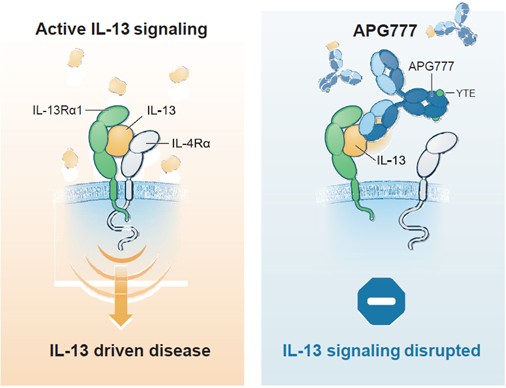
In addition to AD, elevated IL-13 has been observed in other inflammatory conditions such as asthma, CRSwNP and EoE.
Epitope, or binding site, is key in preventing the IL-13Rα1-IL-4Rα active heterodimer formation
As previously described, IL-13 signaling begins with the binding of IL-13 to IL-13Rα1, forming an inactive complex that then binds to IL-4Rα to form the complete, active receptor heterodimer. This active receptor heterodimer is key to the pathogenesis of AD. Therefore, we believe a therapeutic approach for AD needs to prevent the formation of this heterodimer.
36
As shown in Figure 11 below, a 3D rendering of human IL-13 generated from our head-to-head preclinical studies described below, the dark blue highlights the epitope, or binding site, of lebrikizumab, which overlaps with APG777’s epitope, also highlighted in blue. Importantly, these epitopes also overlap with the IL-4Rα epitope on IL-13. Thus, we believe mAb binding to this location is likely to prevent the formation of the IL-13Rα1-IL-4Rα active heterodimer, limiting the inflammatory signaling that is key to AD pathogenesis as well as the pathogenesis of other I&I conditions. This contrasts with the epitope of ADBRY, highlighted in gray, which does not overlap with the IL-4Rα epitope on IL-13 and therefore we believe may have a more limited ability to prevent heterodimerization.
Figure 11 — 3D rendering of human IL-13 and epitopes for antibodies and receptors that bind to IL-13
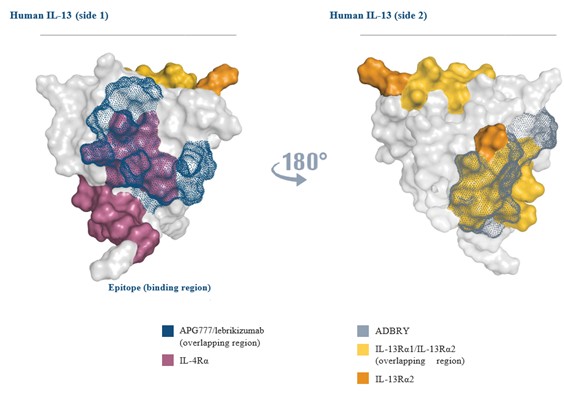
Furthermore, IL-13 also binds a second receptor, IL-13Rα2. Often described as a “decoy” receptor, IL-13Rα2 has a limited cytoplasmic domain and does not appear to mediate signal. IL-13Rα2 does, however, bind to IL-13 with very high affinity, effectively removing IL-13 from circulation. Third-party studies involving IL-13Rα2 knockout mice demonstrated worsened atopic features, including fibrosis and itch.
ADBRY, but not lebrikizumab or APG777, has an epitope that inhibits the binding of IL-13 to IL-13Rα2, which could lead to increased circulating IL-13 levels and, in a counterproductive fashion, worsen AD. However, there can be no assurance that our programs targeting IL-13 will not have similar or comparable results to other third-party agents based on epitope.
37
IL-13 is a soluble cytokine which exists at low concentrations in circulation, making it highly amenable to half-life extension
Half-life for antibodies is a product of degradation or elimination through three pathways: pinocytosis, target-mediated drug disposition (TMDD) and receptor-mediated endocytosis.
| ● | Pinocytosis is a non-specific process in which extracellular fluid and substances are brought into the cell, resulting in an internalized vesicle. This internal vesical then fuses with lysosomes. All antibodies are subject to this elimination pathway. |
| ● | TMDD is a receptor-mediated endocytosis process, meaning that the interactions of the antibody with the receptor on the cell surface results in the internalization of the antibody and subsequent degradation via lysosomes, specialized organelles, or areas within the cell that degrade molecules and other biomaterial. Only mAbs with receptor targets, such as APG808, which targets IL-4Rα, are subject to this elimination pathway. mAbs with soluble targets, such as APG777, which target the soluble cytokine IL-13, are not eliminated via TMDD. |
| ● | Receptor-mediated endocytosis is the binding of antibodies to Fc-gamma-receptors, which are present on many immune cells, can also trigger an elimination process similar to TMDD. However, third-party preclinical studies have demonstrated that this degradation pathway plays only a minor role in the elimination of antibodies, if at all. |
Importantly, antibody recycling through FcRn only impacts degradation via pinocytosis and has no impact on elimination via TMDD. Half-life extension through YTE amino acid modifications, which increases affinity for FcRn, therefore increasing recycling and antibody half-life, is more limited for receptor targets than soluble targets. This is because mAbs with receptor targets are subject to TMDD in addition to pinocytosis. Therefore, we believe soluble targets, like IL-13, which APG777 has been engineered to target, have potential for the longest half-life extension with YTE amino acid modifications. However, there can be no assurance that soluble targets will have such results.
APG777 and lebrikizumab have the same epitope on IL-13 in our head-to-head preclinical studies
Epitope binning describes a technique that characterizes whether two antibodies specific to the same target (in this case, IL-13) can each bind the target at the same time. mAb pairs are binned together if they block each other’s ability to bind to the target antigen. mAb pairs that are found to bin together typically bind to the same or similar epitopes on the antigen.
To characterize the binning of APG777 and lebrikizumab, we studied APG777 and lebrikizumab in head-to-head preclinical studies. Lebrikizumab was immobilized to a sensor chip surface capable of measuring mAb-antigen interactions. IL-13 was first injected into the flow channel, where binding of IL-13 to lebrikizumab generated a response. APG777 was then subsequently injected into the flow channel and the interaction response was recorded. In these studies, no response was observed after APG777 injection. This indicated that APG777 and lebrikizumab binned together and provided evidence to support that the two mAbs likely bind to a similar or the same epitope, or binding site, on IL-13.
In our similar head-to-head preclinical study, ADBRY was found to have a binding response, suggesting that it has a different epitope on IL-13 than lebrikizumab.
APG777 matched the in vitro potency of lebrikizumab and DUPIXENT across all relevant assays in our head-to-head preclinical studies
APG777 was engineered to demonstrate similar preclinical activity to available therapies in our head-to-head studies. Specifically, several assays were used to assess not only affinity for binding to IL-13, but downstream functional inhibition of the IL-13/IL-4 pathway, meaning after IL-13Rα1-IL-4Rα heterodimerization. Measuring downstream functional inhibition of the pathway is critical as this measures the mAb’s impact not only on IL-13, but also the impacts of the resulting inflammatory cascade that causes the features, signs and symptoms associated with AD. To measure these parameters, APG777 was tested in vitro across four assays: Human Affinity by SPR, Inhibition of pSTAT6 Induction, Inhibition of TF-1 Proliferation and Inhibition of TARC Secretion.
38
These assays are described in detail below and outputs are measured in IC90, the concentration or amount of drug it takes to cause a 90% inhibition in the assay.
Results from our head-to-head preclinical studies demonstrated that each of ADBRY, lebrikizumab and APG777 had similar affinity for IL-13 (see Figure 12 below). Notably, since DUPIXENT does not target IL-13, it cannot be compared in this assay, but can be tested in assays on pSTAT6, TF-1 proliferations and TARC release as these assays measure inhibition in the IL-13/IL-4 pathway downstream. On these assays, DUPIXENT, lebrikizumab and APG777 all showed similar inhibition, whereas ADBRY showed inferior downstream inhibition, as demonstrated by the higher IC90, which suggests greater drug concentrations are needed to obtain the same in vitro potency. This provides preclinical evidence of similar in vitro potency among DUPIXENT, lebrikizumab and APG777 across a variety of in vitro assays.
Figure 12 — Head-to-head studies of APG777, ADBRY, DUPIXENT and lebrikizumab in our preclinical assays
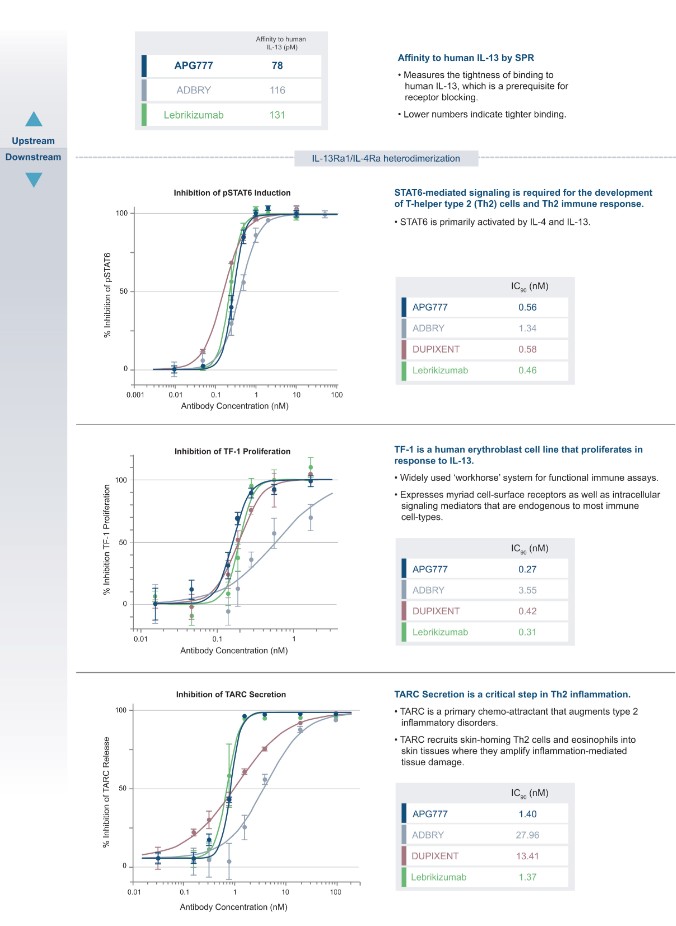
39
APG777 Dosing
APG777 has demonstrated significantly extended half-life in NHPs
To demonstrate APG777’s potential to improve dosing over current and anticipated standard of care mAbs in AD, among other diseases, we studied APG777 in female NHPs following a single bolus dose of 3 mg/kg, given SQ. Blood samples were collected serially starting with a sample pre-dose and subsequently at 0.167, 1, 4, 8, 24, 48, 96, 168, 336, 504, 674, 840, 1334, 1680 and 2160 hours post-dose. Data was analyzed to show mean serum concentration with standard deviation over time and a regression fit was performed.
In our head-to-head studies of APG777 and lebrikizumab in NHPs, APG777 showed a significantly longer half-life than lebrikizumab. In these studies, APG777’s half-life was 27.6 days, as compared to 18.0 days for lebrikizumab, based on cumulative fit models across SQ and IV groups for each compound as shown in Figure 13 below.
Figure 13 — Head-to-head comparison of NHP PK for APG777 and lebrikizumab
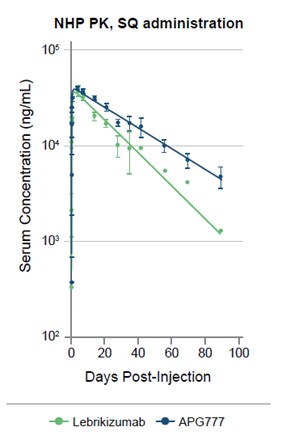
Note: N=3 per group. 2 of 3 animals in the lebrikizumab arm developed ADAs by day 40 (datapoints associated with ADAs are excluded).
40
In a non-head-to-head comparison against third-party NHP data, APG777 demonstrated the highest normalized AUC0-∞ (Cnorm*day), or area under the curve (AUC) from dosing to infinity, among antibodies with the YTE modification, as shown in Figure 14. We believe this showed that APG777’s PK profile provided the greatest sustained concentrations, or levels of drug in the blood stream, relative to other antibodies with the YTE modification.
Figure 14 — NHP PK and AUC for mAbs with YTE modification
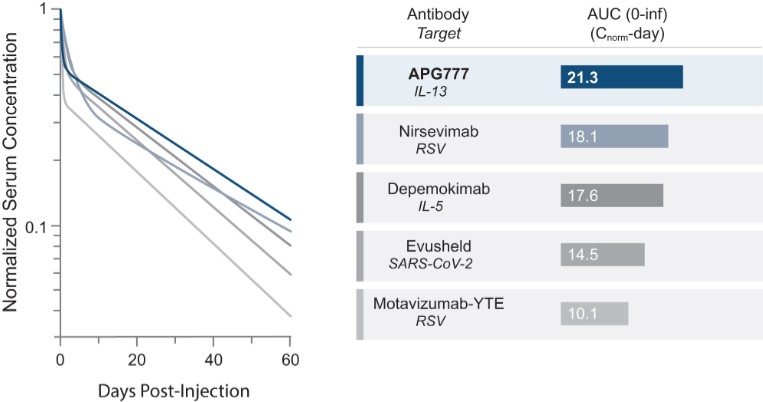
We expect this NHP half-life data to translate to a human half-life of approximately 80 to 110 days based on comparable mAbs with YTE amino acid modification
Given that half-life extension for mAbs with YTE amino acid modification is dependent on the type of target (receptor versus soluble), we examined the translation of NHP half-life data to human half-life data for mAbs with soluble targets and found that human half-life is approximately three to four times longer than NHP half-life (mean: 3.5x, median: 3.1x), as shown in Figure 15 below.
Figure 15 — NHP and human half-life data of mAbs with and without the YTE amino acid modification
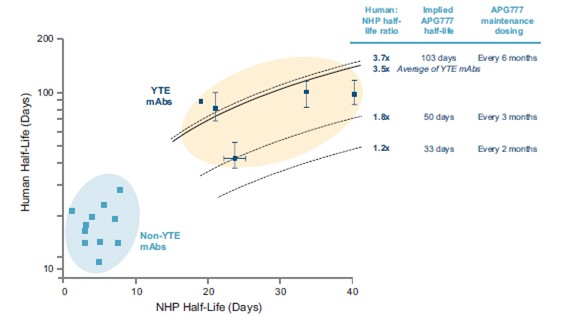
41
We expect APG777 to have a human half-life of approximately 80 to 110 days based on data from other YTE antibodies for soluble targets, which showed a half-life in humans that is three to four times greater than in NHPs, as shown in Figure 16 below, however, there can be no assurance that APG777 will have similar or comparable results.
Figure 16 — NHP and human half-life Data of mAbs with and without the YTE amino acid modification
| (1) | As reported in studies conducted by the sponsor of each of these product candidates or in the label of approved products. |
Based on our PK modeling, with only a 33-day human half-life (which, to our knowledge, would be lower than the lowest half-life for a mAb with the YTE amino acid modifications reported to date), we believe we can achieve an every two month maintenance dosing schedule at our target exposures, which are modeled based on lebrikizumab’s exposures. With only a 50-day half-life, we believe we can achieve an every three month maintenance dosing schedule at our target exposures, which are modeled based on lebrikizumab’s exposures, each as shown in Figure 17 below.
Figure 17 — APG777 NHP half-life, predicted human half-life and predicted dosing interval
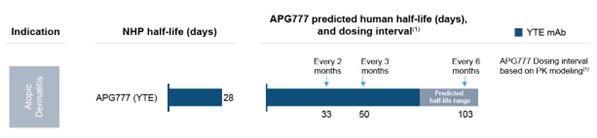
| (1) | Based on steady state PK simulations made with parameters for APG777 identical to lebrikizumab except changes in dose and kelimination. |
APG777 can achieve every two month dosing if it demonstrates a half-life of at least 33 days and every three month dosing if it demonstrates a half-life of at least 50 days
To understand the maintenance dosing schedule that APG777 may be able to achieve, we used known PK parameters for lebrikizumab. These PK parameters provide an understanding of how lebrikizumab is distributed throughout the body and cleared. Based on these known parameters, we built a two-compartment PK model with first-order absorption, which is standard for mAbs, to predict both lebrikizumab’s and APG777’s concentration, or drug levels, over time.
42
Key parameters included 0.156 L/day for clearance (CL), 4.10 L for central volume (Vc), 0.239 day-1 for absorption rate (ka) and 85.6% for bioavailability.
We believe that efficacy in inflammatory conditions, such as AD, is driven by Ctrough, or the minimal concentration of the mAb. Therefore, based on the model described above, we set APG777’s target Ctrough to be equal to lebrikizumab’s Ctrough in maintenance with every four weeks dosing, which was 31.3 mg/L. Given the overlapping epitopes of lebrikizumab and APG777, and similarity in potency across multiple in vitro assays, as described above, we believe this provides a reasonable target drug concentration for APG777. By modeling kelimination, the elimination rate constant or the fraction of drug eliminated in a given time, and half-life to maintain APG777 concentrations above 31.3 mg/L, we approximate at least a 33-day half-life would be required to dose APG777 every two months in maintenance and at least a 50-day half-life would be required to dose APG777 every three months in maintenance assuming a dose of 300 mg.
Thus, based on our PK modeling, with only a 33-day human half-life (which, to our knowledge, would be lower than the lowest half-life for a mAb with the YTE amino acid modifications reported to date), we believe we can achieve an every two month maintenance dosing schedule at our target exposures, which are modeled based on lebrikizumab’s exposures. In addition, with only a 50-day half-life, we believe we can achieve an every three month maintenance dosing schedule at our target exposures, which are modeled based on lebrikizumab’s exposures.
An Extensive Nonclinical Program Has Been Completed to Characterize the Toxicology, Toxicokinetics and ADA Profile of APG777 in NHPs
After evaluating APG777 across a broad range of species, NHPs represented the only pharmacologically relevant species for evaluation. Studies were conducted using an SQ route of administration, as this is the intended route of human administration. Three general toxicology studies with APG777 were designed to assess the toxicology, toxicokinetics and presence of ADAs in NHPs. These included a single-dose non-GLP dose-range finding study, as well as 29-day and six-month GLP toxicology studies.
Our single-dose, non-GLP study in NHPs was completed with no adverse findings in all cohorts, including the highest dose tested
Our single-dose non-GLP study in NHPs was conducted to select doses for the subsequent one-month and six-month studies in NHPs. No adverse findings were observed at doses up to the maximum feasible dose and the highest dose tested.
Our multi-dose, 29-day GLP study in NHPs was completed with no adverse findings in all cohorts, including the highest cohort tested, which was considered the NOAEL
We have conducted a 29-day repeat-dose, GLP-compliant toxicology study in NHPs, in support of our Phase 1 clinical trial in healthy volunteers. NHPs (three to five animals per sex per group) were administered APG777 weekly (five doses in total) at 0, 30, 75 or 150 mg/kg/dose via SC administration. No adverse findings were observed up to the highest dose tested (150 mg/kg), which was the maximum feasible dose and was considered the no observed adverse effect level (NOAEL) in this study.
Our multi-dose, 6-month GLP study in NHPs was completed with no adverse findings in all cohorts, including the highest cohort tested, which was considered the NOAEL
In support of dosing in clinical trials longer than one month in duration, we completed a six-month GLP-compliant toxicology study in NHPs. NHPs (three to five animals per sex per group) were administered APG777 weekly (27 doses in total) at 0, 30, 75 or 150 mg/kg/dose via SC administration. No adverse findings were observed up to the highest dose tested (150 mg/kg), which was the maximum feasible dose and was considered the NOAEL in this study. We believe the results of this study will support progression from Phase 1 to Phase 2 trials of extended duration.
43
Clinical Development of APG777
In August 2023, we initiated a Phase 1 trial of APG777 in healthy volunteers in Australia and we have announced initial SQ PK and safety data from this trial. The APG777 Phase 1 trial is a double-blind, placebo-controlled study in healthy volunteers and consists of a SAD component and a MAD component. Eight healthy volunteers, six treated with APG777 and two treated with placebo, will be enrolled in each cohort, and we enrolled a total of 40 healthy adult subjects in the trial. The primary endpoint is safety and a key secondary endpoint is PK. A schematic of the trial design is shown in Figure 18 below.
Figure 18 — Phase 1 trial design evaluating APG777 in healthy volunteers
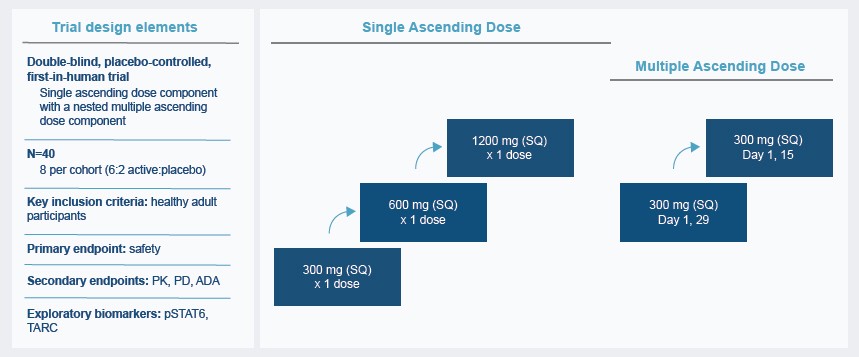
The Phase 1 trial is ongoing and we have announced initial safety and PK data from this trial. Generally, the half-life of mAbs is consistent between healthy volunteers and patients. Consequently, we believe that the PK parameters derived from the Phase 1 trial in healthy volunteers can be used to model dosing regimens in the subsequent Phase 2 and Phase 3 trials in patients with AD and other I&I indications.
We have filed an IND in support of a Phase 1 trial in healthy volunteers in the United States for subjects of Japanese descent and have received a “study may proceed” letter from the FDA for the trial. We anticipate initiating a Phase 2 trial in patients with AD in the first half of 2024. Broadly, the Phase 2 trial is planned to include moderate-to-severe AD patients in a randomized, placebo-controlled design. Primary data readout will be after 16 weeks of treatment, which is common among other agents studied in AD. Endpoints will include, but not be limited to, percent change from baseline in EASI and proportion of patients achieving IGA 0/1 and EASI-75. At the end of the primary 16-week trial, patients will rollover to continue treatment on either a maintenance or open-label extension trial.
Expansion opportunities for APG777
IL-13 has been found to be elevated in other inflammatory conditions. Based on our initial clinical data, we may initiate a Phase 2 trial in asthma, and expect to further evaluate opportunities to develop APG777 for other I&I indications, including AA, CRSwNP, CSU, EoE and PN.
Asthma
We believe asthma to be an important expansion opportunity for APG777 given the significant overlap with AD (31% according to third-party market research studies) and unmet need for extended dosing biologics that do not sacrifice clinical benefit. Patients with moderate-to-severe asthma who qualify and require biologic treatment have a serious condition that, when not treated appropriately, can lead to additional exacerbations and unnecessary emergency room and hospital visits.
44
Extended duration therapies may lead to increased adherence rates with better control and outcomes for these patients.
Eosinophilic asthma is a recognized subtype associated with increased severity and late-onset asthma. IL-13 can induce immune activation and eosinophilic response broadly, and in the case of asthma, contribute to inflammation, airway hyperreactivity and recruitment of eosinophils to lung tissues. Further, in third-party clinical studies, IL-13 and eosinophils have been shown to be positively correlated in airway lumen. Thus, we believe targeting IL-13 in eosinophilic asthma is a compelling approach.
Asthma is estimated to affect 40 million adults and 12 million children in the United States, France, Germany, Italy, Japan, Spain and the United Kingdom. Currently, the asthma market is greater than $10 billion in the seven major markets. Pending data from our Phase 1 trial in healthy volunteers, we plan to initiate a Phase 2 trial of APG777 in asthma to further explore this opportunity.
APG808
Our second most advanced program, APG808, is an SQ extended half-life mAb targeting IL-4Rα. We plan to evaluate APG808 in COPD with the potential to evaluate additional I&I indications at a later date.
Based on our head-to-head preclinical studies of APG808, we have demonstrated the potential to increase the half-life of IL-4Rα-targeting mAbs using half-life extension modifications. In our head-to-head studies of APG808 and DUPIXENT in NHPs, APG808 demonstrated half-life of 27 days versus 11 days for DUPIXENT, an increase of 145%, as shown in Figure 19 below. Moreover, in our head-to-head preclinical assay, APG808 demonstrated equivalent potency of IL-4Rα inhibition compared to DUPIXENT in a head-to-head in vitro assay.
Figure 19 — Head-to-head comparison of NHP PK for APG808 and DUPIXENT
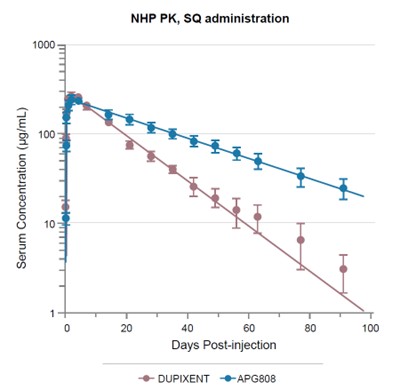
45
In November 2023, we finalized the nomination of a development candidate for APG808 and we received regulatory approval to commence a first-in-human clinical trial in Australia. We anticipate that APG808 will enter the clinic in healthy volunteers in the first half of 2024 followed by a potential Phase 1b trial in asthma and/or a Phase 2 trial in COPD (pending data from the Phase 1 trial and following the submission of an IND or foreign equivalent to support such trials).
IL-4Rα is a known driver of COPD pathogenesis and broader I&I indications
APG808’s target, IL-4Rα, is a known driver of pathogenesis for a number of diseases. By blocking IL-4Rα, we believe APG808 will prevent formation of the IL-13Rα1-IL-4Rα heterodimer, which is understood to be a key pathogenic step in multiple Th2-driven diseases such as AD, asthma, COPD and CRSwNP. As shown in Figure 20 below, blocking IL-4Rα can prevent signaling through both IL-4 and IL-13. Preventing the formation of the IL-13Rα1-IL-4Rα heterodimer in turn prevents recruitment of members of the JAK family of enzymes and prevents the signaling cascade that results in the expression of pro-inflammatory cytokines and leads to an immune response by the body in these diseases.
Figure 20 — APG808 is designed to disrupt IL-13 signaling by preventing the formation of the IL-13Rα1-IL-4Rα heterodimer
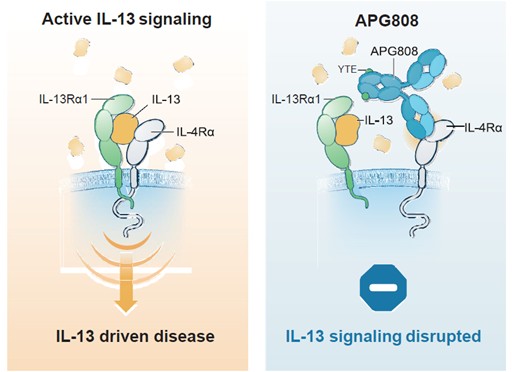
COPD has historically been thought of as driven by Th1 immune responses, which are driven by IL-2, interferon-γ and lymphotoxin-α and an associated neutrophilic response. However, more recent third-party data has demonstrated that Th2 immune responses, which are driven by IL-4, IL-5 and IL-13 and associated with an eosinophilic response, are prominent in a subset of COPD patients. Th2 immune responses have been shown to be associated with increased airway inflammation and appear to underlie COPD in a subset of patients and related cytokines have been shown to be upregulated during exacerbations.
The exact mechanism of Th2 immune response leading to airway inflammation is unknown, but is in part driven by allergens driving the adaptive immune response inducing differentiation toward Th2 cells, as well as pollutants, microbes and glycolipids activating ILC2s (Type 2 innate lymphoid cells) to produce Th2-associated cytokines IL-5 and IL-13. Eosinophils have been shown to contribute to bronchoconstriction, fibrosis and mucus production in animal models of COPD.
46
Further, overexpression of IL-13 has been shown in mice lungs to lead to emphysema (air-filled spaces in the lungs), elevated mucus production and inflammation reminiscent of human COPD. Therefore, while still not fully elucidated, Th2 immune response produces some of the hallmark pathologies of COPD.
Third-party clinical trials have demonstrated that up to 52% of patients with COPD have an increased eosinophil count, which is a marker of Th2 immune response. Studies have further demonstrated an association between eosinophilic airway inflammation and severe exacerbations of COPD. There is also epidemiological evidence of a correlation between eosinophils and mortality from COPD exacerbations. We do not yet have clinical data regarding patients with COPD and there can be no assurance that our trials will have similar or comparable results.
In our preclinical studies, APG808 binned with DUPIXENT
As described previously, epitope binning is a technique used to cluster different mAbs based on the specific region of the antigen (in this case IL-4Rα) that is recognized by the antibody. To characterize the binning of APG808 and DUPIXENT, we studied APG808 and DUPIXENT in head-to-head preclinical studies. In binning studies with immobilized DUPIXENT, no response was observed for APG808. This indicated that APG808 and DUPIXENT binned together and provided evidence that the two mAbs likely bind to a similar or the same epitope on IL-4Rα.
APG808 has demonstrated equivalent potency to DUPIXENT in head-to-head in vitro assays
APG808 was engineered to demonstrate similar preclinical activity to available therapies in our head-to-head studies. Specifically, an assay was performed to measure downstream functional inhibition of the IL-13/IL-4 pathway, meaning after IL-13Rα1 and IL-4Rα heterodimerization. Measuring downstream functional inhibition of the pathway is critical, as this measures the mAb’s impact on the inflammatory cascade that causes the features, signs, and symptoms associated with I&I indications, including COPD.
More specifically, three in vitro assays were performed showing inhibition of pSTAT6 induction, TF-1 proliferation and TARC Secretion. STAT6-mediated signaling is required for the development of Th2 cells and the Th2 immune response and is primarily activated by IL-4 and IL-13. TF-1 is a human erythroblast cell line that proliferates in response to IL-4 or IL-13. This cell line is a widely used “workhorse” system for several functional immune assays owing to its expression of a myriad of cell-surface receptors as well as intracellular signaling mediators that are endogenous to most immune cell-types. Lastly, TARC secretion is a critical step in Th2 inflammation, with TARC recruiting skim-homing Th2 cells and eosinophils into skin tissues where they amplify inflammation-mediated tissue damage. Outputs of these assays were measured in IC90, the concentration or amount of drug it takes to cause a 90% inhibition in the assay.
47
In our head-to-head preclinical study, DUPIXENT and APG808 showed similar binding, with femtomolar affinity for IL-4Rα, and similar inhibition across the three in vitro assays which measure downstream functional inhibition of the IL-13/IL-4 pathway (pSTAT6 induction, inhibition of TF-1 proliferation, and inhibition of TARC secretion). As shown in Figure 21 below, in the TF-1 assay for STAT-6 phosphorylation, the IC90 was 1.11 nM for APG808 compared to 1.93 nM for DUPIXENT and for TARC secretion the IC90 was 1.25 for APG808 and 1.67 for DUPIXENT. These results provide preclinical evidence of similar in vitro potency among DUPIXENT and APG808.
Figure 21 — Head-to-head comparison of APG808 versus DUPIXENT in the TF-1 proliferation assay
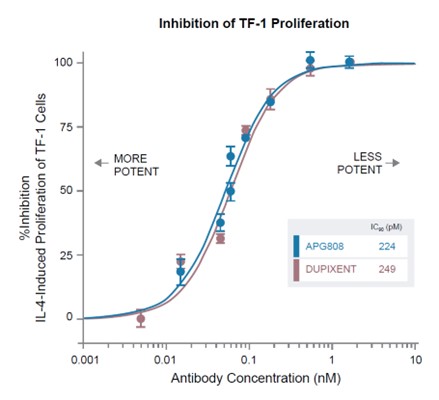
APG808 Dosing
We have demonstrated the potential to increase APG808’s half-life approximately two times over DUPIXENT’s half-life in NHPs
In our single-dose NHP studies, we have demonstrated the potential to increase the half-life of IL-4Rα-targeting mAbs using half-life extension modifications. In our head-to-head studies in NHPs, APG808 demonstrated half-life of 27 days versus 11 days for DUPIXENT, an increase of 145%.
48
Analogous antibodies with half-life extension modifications have shown half-lives extension over NHP data of approximately two to three times
We have incorporated half-life extension technology in APG808 based on antibody recycling, such as YTE or LS amino acid modifications, as was used in the tool compound data shown above. Antibody recycling through increased affinity for FcRn, as described in the sections above, impacts degradation via pinocytosis, but not elimination via TMDD. Therefore, to understand APG808’s potential half-life in the clinic, we concluded analogs with membrane-bound targets would be the most informative. Figure 22 below shows the NHP and human half-life data of mAbs for membrane-bound targets with and without the YTE amino acid modification.
Figure 22 — NHP and human half-life data of mAbs for membrane-bound targets with and without the YTE amino acid modification
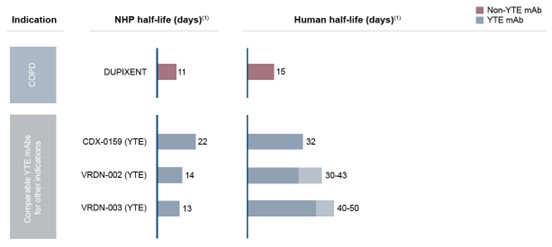
(1) |
As reported in studies conducted by the sponsor of each of these product candidates or in the label of approved products. |
As one example, CDX-0159 is an antibody targeting KIT (c-KIT/CD117) receptor tyrosine kinase with YTE amino acid modifications for half-life extension currently in clinical development. In NHPs, half-life was shown to be 22 days for CDX-0159 compared to 4.8 days for CDX-0158, a non-half-life extended antibody directed at the same target. Clinically, CDX-0159 showed a 32-day half-life, suggesting an approximately one-and-a-half times increase over NHP data. Further, CDX-0159 has shown a human half-life that is approximately five times greater than CDX-0158, the non-half-life extended antibody directed at the same target (half-life of CDX-0159 was 32 days versus 6 days for CDX-0158).
As another example, VRDN-002 is an antibody targeting anti-IGF-1 receptor with recycling-based FC modifications for half-life extension (i.e., YTE or LS or similar amino acid modifications) currently in clinical development. In NHPs, half-life was shown to be 14 days for VRDN-002 compared to 6.4 days for teprotumumab, a non-half-life extended antibody directed at the same target. Clinically, VRDN-002 showed an approximately 30-to 40-day half-life in an interim analysis, suggesting an approximately two to three times increase over NHP data. Further, VRDN-002 has shown a human half-life that is approximately three to four times greater than teprotumumab, the non-half-life extended antibody directed at the same target (half-life of VRDN-002 was approximately 30 to 40 days compared to approximately 10 to 11 days for teprotumumab).
As a third example, VRDN-003 is an antibody targeting anti-IGF-1 receptor with recycling-based Fc modifications for half-life extension (i.e. YTE or LS or similar amino acid modifications) currently in clinical development. In NHPs, half-life was shown to be 13 days. Clinically, VRDN-002 showed an approximately 40-to 50-day half-life, suggesting an increase of approximately three to four times over NHP data.
49
Therefore, as shown in Figure 23 below, we expect that APG808 would have a human half-life of approximately 39 to 104 days based on two estimation methods. Via the first method, we estimate APG808’s human half-life to be approximately 41 to 103 days based on APG808’s 27 day NHP half-life and a one-and-a-half to approximately four times factor going from NHPs to humans as observed for other membrane-bound half-life extended mAbs.
Via the second method, we estimate APG808’s human half-life to be approximately 45 to 75 days based on DUPIXENT’s 15-day human half-life and a three to five times factor going from non-half-life extended antibodies to half-life extended antibodies directed at the same receptor target.
Figure 23 — APG808 NHP half-life, predicted human half-life and predicted dosing interval
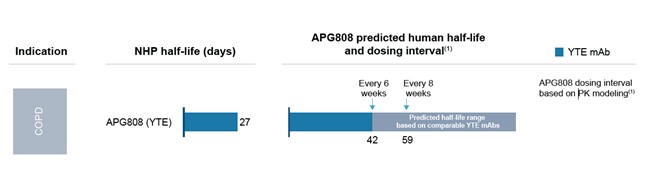
(1) |
Based on steady state PK simulations made with parameters for APG808 identical to DUPIXENT except changes in dose and kelimination. |
APG808 can achieve every six weeks dosing if it demonstrates a half-life of at least 42 days and every two month dosing if it demonstrates a half-life of at least 59 days
To understand the maintenance dosing schedule that APG808 may be able to achieve, we used known PK parameters for DUPIXENT. These PK parameters provide an understanding of how DUPIXENT is distributed throughout the body and cleared. Based on these known parameters, we built a two-compartment model with first-order absorption and parallel linear and Michaelis-Menten elimination, the latter corresponding to TMDD effects associated with targeting membrane-bound IL-4Rα, to predict both DUPIXENT’s and APG808’s concentration, or drug levels, over time. Key parameters included 0.0447 day-1 for elimination rate (ke), 2.74 L for central volume (Vc), 0.306 day-1 for absorption rate (ka) and 64.2% for bioavailability.
We believe that efficacy in inflammatory conditions, such as COPD, is driven by Ctrough, or the minimal concentration of the mAb. Therefore, based on the model described above, we set APG808’s target Ctrough to be equal to DUPIXENT’s Ctrough with every two weeks dosing, which was approximately 75 mg/L. Given the planned overlapping epitopes of DUPIXENT and APG808 and similarity in potency across multiple in vitro assays, we believe this provides a reasonable target drug concentration for APG808. By modeling kelimination and half-life to maintain APG808 concentrations above approximately 75 mg/L, we approximate at least a 42 day half-life would be required to dose APG808 every six weeks and at least a 59-day half-life would be required to dose APG808 every two months based on our planned dose and formulation.
Thus, with a minimum of 42-or 59-day half-life, which is in range for most mAbs with half-life extension targeting receptors, we believe we can achieve either an every six week or an every two month dosing schedule, respectively, at our target exposures, which are modeled based on DUPIXENT’s exposures.
50
Development Plan for APG808
In November 2023, we finalized the nomination of a development candidate for APG808 and we received regulatory approval to commence a first-in-human clinical trial in Australia. The APG808 Phase 1 trial is designed as a double-blind, placebo-controlled study in healthy volunteers with single ascending doses. Eight healthy volunteers, six treated with APG808 and two treated with placebo, will be enrolled in each cohort, and we expect to enroll a total of approximately 32 healthy adult subjects in the trial. The primary endpoint is safety and a key secondary endpoint is PK. Pending data from our Phase 1 trial in healthy volunteers and following the submission of an IND or foreign equivalent to support a Phase 2 trial in COPD, we plan to initiate a Phase 2 trial in patients with COPD.
Expansion opportunities for APG808
IL-4Rα biology has been implicated in a number of different indications, including AD, asthma, CRSwNP, EoE, PN and CSU. We intend to evaluate additional expansion opportunities in one or more of such indications.
Asthma
We believe that APG808 could potentially benefit patients with eosinophilic asthma. DUPIXENT, which also targets IL-4Rα but is dosed every other week, is approved in asthma in patients six years of age or older with moderate-to-severe-asthma with eosinophilic phenotype or oral corticosteroids dependent regardless of phenotype and has shown a 46% reduction in the rate of annualized exacerbations in pivotal studies, which we believe validates targeting IL-4Rα as an approach to treating asthma.
Pending data from our Phase 1 trial in healthy volunteers, we may initiate a Phase 1b trial of APG808 in a small cohort of asthma patients to further explore this opportunity.
APG990
Our third program, APG990, is an SQ extended half-life mAb targeting OX40L. We expect to nominate a development candidate in 2024 if we observe equivalent or better in vitro potency compared to other mAbs targeting OX40L and an improved PK profile, including half-life extension, in head-to-head studies.
OX40L is the ligand for OX40 expressed on antigen presenting cells. Its interaction with OX40 causes the accumulation of T cells by providing a survival signal. T cells are important types of white blood cells of the immune system that play a central role in the immune response. OX40L, by playing a role in activating T cells and reprogramming them into inflammatory subsets, contributes to immune overactivation in AD and other inflammatory conditions. OX40-OX40L interaction has been implicated in a broad range of inflammatory and autoimmune diseases, including Inflammatory Bowel Disease (IBD), asthma, diabetes, arthritis, atherosclerosis, transplant rejection, GVHD and Systemic Lupus Erythematosus. Additionally, OX40L activation of OX40 inhibits the expression of FOXP3 and the inhibitory function of regulatory T (Treg) cells. Treg cells can suppress the immune response that leads to worsening symptoms in inflammatory conditions.
OX40L blockade therefore has two mechanisms by which it might have impact on the pathology associated with inflammatory conditions, first by suppressing inflammatory T cell activation, and second by increasing the proliferation of Treg cells, which can serve to further reduce effector T cell function. The mechanism of action of APG990 is shown in Figure 24 below.
51
Figure 24 — Mechanism of action of APG990
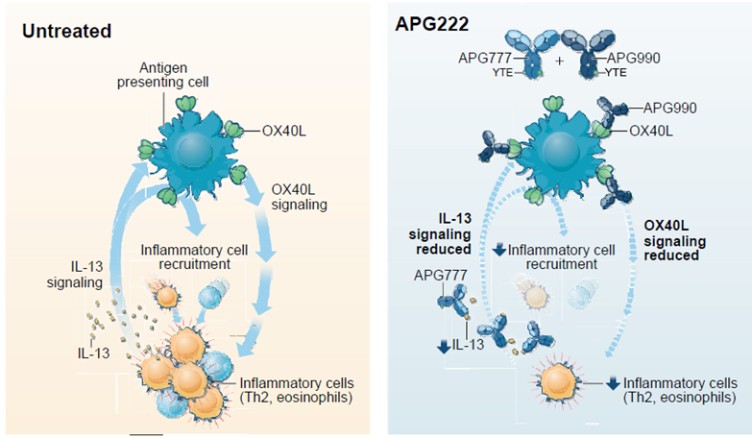
Currently, there are only two MOAs targeted by approved biologic agents in atopic dermatitis, IL-13 and IL-4Rα. Targeting OX40L could represent a third MOA. OX40L occurs higher up in the inflammatory pathway than IL-13 or IL-4Rα and potentially broadens the impact on the inflammatory cascade, which may have benefits for certain patients. Specifically, OX40L could represent another therapeutic option for the portion of patients who do not benefit from currently available treatments.
Development plan for APG990
We intend to nominate a development candidate in 2024 if we observe equivalent or better in vitro potency compared to other mAbs targeting OX40L and an improved PK profile, including half-life extension, in head-to-head studies. Following nomination of a development candidate, we plan to conduct the appropriate nonclinical toxicology studies to support initiation of a Phase 1 clinical trial in healthy volunteers and file an IND or foreign equivalent required to initiate such trial.
APG222
Our fourth program, APG222, is one or more extended half-life SQ antibodies targeting both IL-13 and OX40L, which we believe has the potential to improve outcomes in AD over current standard of care biologic therapies.
Potential clinical benefit of targeting both IL-13 and OX40L
We believe that blocking multiple targets, such as simultaneous inhibition of IL-13 and OX40L, could allow us to provide benefit to patients with AD and other I&I indications. Data from a third-party Phase 2a trial of amlitelimab, an antibody targeting OX40L, demonstrated a decrease in circulating IL-13 with treatment, but not a complete obliteration of IL-13. OX40L signaling promotes immune cells to differentiate and produce cytokines, including IL-13. Thus, we hypothesize that blocking IL-13 will lead to less immune cell differentiation leading to lower levels of IL-13 production. We believe that the mechanism of action of APG222, which combines blockage of OX40L and IL-13 (as shown in Figure 25 below), could simultaneously decrease OX40L signaling, helping to rebalance the immune system and decrease immune cell differentiation and cytokine release, and further reduce IL-13, resulting even less immune signaling. This, in turn, could prevent certain disease-related signs and symptoms that are driven by IL-13 signaling and the downstream inflammatory cascade.
52
Figure 25 — Mechanism of action of APG222
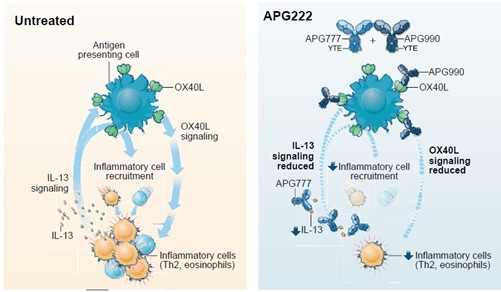
Development plan for APG222
We are generating preclinical data to support our approach to targeting both IL-13 and OX40L. If such preclinical data supports our approach, subject to completion of the Phase 1 healthy volunteer trials for each of APG777 and APG990, we intend to file an IND or foreign equivalent and initiate a trial targeting both IL-13 and OX40L in AD thereafter.
Additional Expansion Opportunities
In addition to the currently planned expansion opportunities for APG777 and APG808, we are evaluating opportunities to develop our programs for other I&I indications, including AA, CRSwNP, CSU, EoE and PN. We do not yet have clinical data showing the ability of our programs to treat other indications and there can be no assurance that our programs will have similar or comparable results to any products or later-stage product candidates for these indications.
Alopecia Areata
Patients with AA represent a population with high unmet need, given there are no approved targeted biologic therapies. Recent third-party Phase 2a data for DUPIXENT demonstrated clinical benefit in patients with AA, which we believe provides support for the IL-4/IL-13 pathway blockade as a potential treatment for AA.
Chronic Rhinosinusitis with Nasal Polyps
CRSwNP is commonly comorbid with asthma and the two diseases have overlapping biology. IL-4 and IL-13 have been shown to play important roles in the pathophysiology of CRSwNP. Further, DUPIXENT is approved for this indication, which we believe demonstrates the potential for IL-13 and/or IL-4Rα targeting.
Chronic Spontaneous Urticaria
CSU is a disease where mast cells are believed to be the key effector cells, although data has also demonstrated that IL-4 and IL-13 may be key in the development and maintenance of CSU. Further, we believe the positive Phase 3 data for DUPIXENT in patients with CSU that is not adequately controlled with the current standard of care suggests the role of the IL-4/IL-13 heterodimer signaling complex’s involvement in CSU.
53
Eosinophilic Esophagitis
EoE is a chronic inflammatory condition of the esophagus, with the hallmark histological finding being eosinophilic infiltrates (i.e., presences of eosinophils in the tissue). When not treated appropriately, EoE progresses to cause scarring and strictures of the esophagus, which gives patients significant trouble with eating and drinking and potential nutritional compromise. The only available biologic for the treatment of EoE is DUPIXENT, which was approved for this indication in 2022, and requires weekly dosing. DUPIXENT’s approval in EoE further supports the scientific rationale for IL-13/IL-4Rα targeting agents in treating EoE.
Prurigo Nodularis
PN is a chronic inflammatory condition of the skin where lesions have shown Th2-associated cytokines such as IL-4, IL-13 and IL-31. DUPIXENT is approved for this indication, which we believe demonstrates the potential for IL-13 and/or IL-4Rα targeting.
Additional I&I Indications
We may expand into additional I&I indications, such as Crohn disease, lupus, rheumatoid arthritis, psoriasis and ulcerative colitis, that are implicated in the disease pathways targeted by our current or future programs.
Our Collaboration, License and Services Agreements
Paragon Option Agreements
In February 2022, we entered into an antibody discovery and option agreement with Paragon, which was subsequently amended in November 2022 (as amended, the 2022 Option Agreement). Under the terms of the 2022 Option Agreement, Paragon identifies, evaluates and develops antibodies directed against certain mutually agreed therapeutic targets of interest to us. The 2022 Option Agreement initially included two selected targets, IL-13 and IL-4Rα, and was subsequently amended in November 2022 to include an additional selected target, OX40L. Under the 2022 Option Agreement, we have the exclusive option to, on a research program-by-research program basis, be granted an exclusive, worldwide license to all of Paragon’s right, title and interest in and to the intellectual property resulting from the applicable research program to develop, manufacture and commercialize the antibodies and products directed to the selected targets (each, an Option). From time to time, we can choose to add additional targets to the collaboration by mutual agreement with Paragon.
Pursuant to the terms of the 2022 Option Agreement, the parties will initiate certain research programs that will generally be focused on a particular target (each, a Research Program). Each Research Program is aimed at discovering, generating, identifying and/or characterizing antibodies directed to the respective target. For each Research Program, the parties established a research plan that sets forth the activities that will be conducted, and the associated research budget (each, a Research Plan). Upon execution of the 2022 Option Agreement, we agreed with Paragon on an initial Research Plan that outlined the services that will be performed commencing at inception of the arrangement related to IL-13 and IL-4Rα. The Research Plan for OX40L was agreed to prior to December 31, 2022. Our exclusive option with respect to any future Research Program is exercisable at our sole discretion at any time during the period beginning on the initiation of activities under the associated Research Program and ending a specified number of days following the delivery of the data package from Paragon related to the results of the Research Plan activities (the Option Period). There is no payment due upon exercise of an Option pursuant to the 2022 Option Agreement.
In consideration for the exclusive options granted under the 2022 Option Agreement, we paid an upfront cash amount of $1.3 million and issued 1,250,000 common units to Paragon. Paragon was also entitled to up to an additional 3,750,000 of common units in exchange for the rights granted under the 2022 Option Agreement, which were issued in connection with the closings of the additional tranches of the Series A Preferred Unit financing. Under the 2022 Option Agreement, on a Research Program-by-Research Program basis following the finalization of the Research Plan for each respective Research Program, we are required to pay Paragon a nonrefundable fee in cash of $0.5 million. We are also obligated to compensate Paragon on a quarterly basis for its services performed under each Research Program based on the actual costs incurred.
54
In November 2023, we entered into an additional antibody discovery and option agreement with Paragon (the 2023 Option Agreement and together with the 2022 Option Agreement, collectively, the Option Agreements). Under the terms of the 2023 Option Agreement, Paragon identifies, evaluates and develops antibodies directed against certain mutually agreed therapeutic targets of interest to us. The 2023 Option Agreement initially includes one undisclosed target. Under the 2023 Option Agreement, we have the exclusive option to, on a research program-by-research program basis, be granted an exclusive, worldwide license to all of Paragon’s right, title and interest in and to the intellectual property resulting from the applicable research program to develop, manufacture and commercialize the antibodies and products directed to the selected targets. From time to time, we can choose to add additional targets to the collaboration by mutual agreement with Paragon.
Pursuant to the terms of the 2023 Option Agreement, the parties may initiate Research Programs. Each Research Program is aimed at discovering, generating, identifying and/or characterizing antibodies directed to the respective target. For each Research Program, the parties must establish a Research Plan. We and Paragon will agree on an initial Research Plan that outlines the services that will be performed commencing at inception of the arrangement related to the undisclosed target. Our exclusive option with respect to each Research Program is exercisable at our sole discretion at any time during the period beginning on the initiation of activities under the associated Research Program and ending a specified number of days following the delivery of the data package from Paragon related to the results of the Research Plan activities. There is no payment due upon exercise of an Option pursuant to the 2023 Option Agreement. Following entry into the 2023 Option Agreement, we and Paragon will negotiate a form of License Agreement to be entered into in the event that we exercise our exclusive option with respect to each Research Program, which License Agreement will include certain pre-agreed economic and other business terms.
Under the 2023 Option Agreement, on a Research Program-by-Research Program basis following the finalization of the Research Plan for each respective Research Program, we are required to pay Paragon a nonrefundable fee in cash of $2.0 million. In the first quarter of 2024, we paid Paragon $2.0 million fee for a Research Program for an undisclosed target. We are also obligated to compensate Paragon on a quarterly basis for its services performed under each Research Program based on the actual costs incurred. We expense the service fees as the associated costs are incurred when the underlying services are rendered.
Unless terminated earlier, the Option Agreements shall continue in force on a Research Program-by-Research Program basis until the earlier of: (i) the end of the Option Period for such Research Program, as applicable, if such Option is not exercised by us; and (ii) the effective date of the license agreement for such Research Program if we exercise our Option with respect to such Research Program (the Term). Upon the expiration of the Term for all then-existing Research Programs, the applicable Option Agreement will automatically expire in its entirety. We may terminate either Option Agreement or any Research Program at any time for any or no reason upon 30 days’ prior written notice to Paragon, provided that we must pay certain unpaid fees due to Paragon upon such termination, as well as any non-cancellable obligations reasonably incurred by Paragon in connection with its activities under any terminated Research Program. Each party has the right to terminate either Option Agreement or any Research Program upon (i) 30 days’ prior written notice of the other party’s material breach that remains uncured for the 30 day period and (ii) the other party’s bankruptcy.
Paragon IL-13 License Agreement
In November 2022, we exercised our option available under the 2022 Option Agreement with respect to the IL-13 Research Program. Upon such exercise, we entered into an associated license agreement with Paragon (the IL-13 License Agreement). Under the terms of the IL-13 License Agreement, Paragon granted to us an exclusive, worldwide, royalty-bearing, sublicensable right and license with respect to certain information, patent rights and sequence information related to antibodies directed at the IL-13 target to use, make, sell, import, export and otherwise exploit the antibodies directed at the IL-13 target. Pursuant to the IL-13 License Agreement, we granted to Paragon a similar license (except that such license we granted to Paragon is non-exclusive) to the IL-13 license with respect to multispecific antibodies that are directed at the IL-13 target and one or more other antibodies. We were also granted a right of first negotiation with Paragon concerning the development, license and grant of rights to certain multispecific antibodies.
55
We are solely responsible for the continued development, manufacture and commercialization of products at our own cost and expense.
We are obligated to pay Paragon up to $3.0 million upon the achievement of specific development and clinical milestones for the first product under the IL-13 License Agreement that achieves such specified milestones. Upon execution of the IL-13 License Agreement, we paid Paragon a $1.0 million fee for nomination of a development candidate. In August 2023, we announced the dosing of our first participant in the Phase 1 trial of APG777 and incurred a milestone payment of $2.0 million to Paragon in the third quarter of 2023.
We are also obligated to pay royalties to Paragon equal to a low-single digit percentage of net sales of any products under the IL-13 License Agreement, and Paragon has a similar obligation to pay royalties to us with respect to the IL-13 multispecific license. Royalties are due on a product-by-product and country-by-country basis beginning upon the first commercial sale of each product and ending on the later of (i) 12 years after the first commercial sale of such product in such country and (ii) expiration of the last valid claim of a patent covering such product in such country (Royalty Term). No royalty payments had become due to Paragon through December 31, 2023.
Unless earlier terminated, the IL-13 License Agreement remains in effect until the expiration of the last-to-expire Royalty Term for any and all products. We may terminate the agreement in its entirety or on a country-by-country or product-by-product at any time for any or no reason upon 60 days advance written notice to Paragon, and either party may terminate for (i) the other party’s material breach that remains uncured for 90 days (or 30 days with respect to any failure to make payments) following notice of such breach and (ii) the other party’s bankruptcy. Upon any termination prior to the expiration of an agreement, all licenses and rights granted pursuant to the agreement will automatically terminate and revert to the granting party and all other rights and obligations of the parties will terminate.
Paragon IL-4Rα License Agreement
In April 2023, we exercised our option available under the 2022 Option Agreement with respect to the IL-4Rα Research Program. Upon such exercise, we entered into an associated license agreement with Paragon (the IL-4Rα License Agreement). Under the terms of the IL-4Rα License Agreement, Paragon granted to us an exclusive, worldwide, royalty-bearing, sublicensable right and license with respect to certain information, patent rights and sequence information related to antibodies directed at the IL-4Rα target to use, make, sell, import, export and otherwise exploit the antibodies directed at the IL-4Rα target. Pursuant to the IL-4Rα License Agreement, we granted to Paragon a similar license (except that such license we granted to Paragon is non-exclusive) to the IL-4Rα license with respect to multispecific antibodies that are directed at the IL-4Rα target and one or more other antibodies. We also granted a right of first negotiation with Paragon concerning the development, license and grant of rights to certain multispecific antibodies. We are solely responsible for the continued development, manufacture and commercialization of products at our own cost and expense.
We are obligated to pay Paragon up to $3.0 million upon the achievement of specific development and clinical milestones for the first product under the IL-4Rα License Agreement that achieves such specified milestones.
In November 2023, the Company finalized the nomination of a development candidate under the IL-4Rα License Agreement and made a milestone payment of $1.0 million to Paragon in the fourth quarter of 2023. Thereafter, we are obligated to make a further milestone payment of $2.0 million upon the first dosing of a human patient in a Phase 1 trial.
We are also obligated to pay royalties to Paragon equal to a low-single digit percentage of net sales of any products under the IL-4Rα License Agreement, and Paragon has a similar obligation to pay royalties to us with respect to the IL-4Rα multispecific license. Royalties are due on a product-by-product and country-by-country basis beginning upon the first commercial sale of each product and ending on the later of (i) 12 years after the first commercial sale of such product in such country and (ii) expiration of the last valid claim of a patent covering such product in such country.
Unless earlier terminated, the IL-4Rα License Agreement remains in effect until the expiration of the last-to-expire Royalty Term for any and all products. We may terminate the agreement in its entirety or on a country-by-country or product-by-product at any time for any or no reason upon 60 days advance written notice to Paragon, and either party may terminate for (i) the other party’s material breach that remains uncured for 90 days (or 30 days with respect to any failure to make payments) following notice of such breach and (ii) the other party’s bankruptcy.
56
Upon any termination prior to the expiration of an agreement, all licenses and rights granted pursuant to the agreement will automatically terminate and revert to the granting party and all other rights and obligations of the parties will terminate.
Paragon OX40L License Agreement
In April 2023, we exercised our option available under the 2022 Option Agreement with respect to the OX40L Research Program. Upon such exercise, we entered into an associated license agreement with Paragon (the OX40L License Agreement). Under the terms of the OX40L License Agreement, Paragon granted to us an exclusive, worldwide, royalty-bearing, sublicensable right and license with respect to certain information, patent rights and sequence information related to antibodies directed at the OX40L target to use, make, sell, import, export and otherwise exploit the antibodies directed at the OX40L target. Pursuant to the OX40L License Agreement, we granted to Paragon a similar license (except that such license we granted to Paragon is non-exclusive) to the OX40L license with respect to multispecific antibodies that are directed at the OX40L target and one or more other antibodies. We also granted a right of first negotiation with Paragon concerning the development, license and grant of rights to certain multispecific antibodies. We are solely responsible for the continued development, manufacture and commercialization of products at our own cost and expense.
We are obligated to pay Paragon up to $3.0 million upon the achievement of specific development and clinical milestones for the first product under the OX40L License Agreement that achieves such specified milestones. The first specified milestone payment of $1.0 million under the agreement is due upon the nomination of a development candidate, which has not yet occurred. Thereafter, we are obligated to make a further milestone payment of $2.0 million upon the first dosing of a human patient in a Phase 1 trial.
We are also obligated to pay royalties to Paragon equal to a low-single digit percentage of net sales of any products under the OX40L License Agreement, and Paragon has a similar obligation to pay royalties to us with respect to the OX40L multispecific license. Royalties are due on a product-by-product and country-by-country basis beginning upon the first commercial sale of each product and ending on the later of (i) 12 years after the first commercial sale of such product in such country and (ii) expiration of the last valid claim of a patent covering such product in such country.
Unless earlier terminated, the OX40L License Agreement remains in effect until the expiration of the last-to-expire Royalty Term for any and all products. We may terminate each agreement in its entirety or on a country-by-country or product-by-product at any time for any or no reason upon 60 days advance written notice to Paragon, and either party may terminate for (i) the other party’s material breach that remains uncured for 90 days (or 30 days with respect to any failure to make payments) following notice of such breach and (ii) the other party’s bankruptcy. Upon any termination prior to the expiration of an agreement, all licenses and rights granted pursuant to the agreement will automatically terminate and revert to the granting party and all other rights and obligations of the parties will terminate.
Biologics Master Services Agreement — WuXi Biologics (Hong Kong) Limited
In June 2022, Paragon and WuXi Biologics (Hong Kong) Limited (WuXi Biologics) entered into a biologics master services agreement (the WuXi Biologics MSA), which was subsequently novated to us by Paragon in the second quarter of 2023. The WuXi Biologics MSA governs all development activities and GMP manufacturing and testing for our APG777, APG808 and APG990 programs, as well as potential future programs, on a work order basis. Under the WuXi Biologics MSA, we are obligated to pay WuXi Biologics a service fee and all non-cancellable obligations in the amount specified in each work order associated with the agreement for the provision of services.
The WuXi Biologics MSA terminates on the later of (i) June 20, 2027 or (ii) the completion of services under all work orders executed by the parties prior to June 20, 2027, unless terminated earlier. The term of each work order terminates upon completion of the services under such work order, unless terminated earlier. We can terminate the WuXi Biologics MSA or any work order at any time upon 30 days’ prior written notice and immediately upon written notice if WuXi Biologics fails to obtain or maintain required material governmental licenses or approvals. Either party may terminate a work order (i) at any time upon six months’ prior notice with reasonable cause, provided however that if WuXi Biologics terminates a work order in such manner, no termination or cancellation fees shall be paid by us and (ii) immediately for cause upon (a) the other party’s material breach that remains uncured for 30 days after notice of such breach, (b) the other party’s bankruptcy or (c) a force majeure event that prevents performance for a period of at least 90 days.
57
Cell Line License Agreement — WuXi Biologics (Hong Kong) Limited
In June 2022, Paragon and WuXi Biologics entered into a cell line license agreement (the Cell Line License Agreement), which was subsequently novated to us by Paragon in the second quarter of 2023. Under the Cell Line License Agreement, we received a non-exclusive, worldwide, sublicensable license to certain of WuXi Biologics’ know-how, cell line, biological materials (the WuXi Biologics Licensed Technology) and media and feeds to make, have made, use, sell and import certain therapeutic products produced through the use of the cell line licensed by WuXi Biologics under the Cell Line License Agreement (the WuXi Biologics Licensed Products). Specifically, the WuXi Biologics Licensed Technology is used to manufacture a component of our APG777 and APG808 product candidates.
In consideration for the license, we agreed to pay WuXi Biologics a non-refundable license fee of $150,000. Additionally, if we manufacture all of our commercial supplies of bulk drug product with a manufacturer other than WuXi Biologics or its affiliates, we are required to make royalty payments to WuXi Biologics in an amount equal to a fraction of a single digit percentage of global net sales of WuXi Biologics Licensed Products manufactured by a third-party manufacturer (the Royalty). If we manufacture part of our commercial supplies of the WuXi Biologics Licensed Products with WuXi Biologics or its affiliates, then the Royalty will be reduced accordingly on a pro rata basis.
The Cell Line License Agreement will continue indefinitely unless terminated (i) by us upon six months’ prior written notice and our payment of all undisputed amounts due to WuXi Biologics through the effective date of termination, (ii) by WuXi Biologics for a material breach by us that remains uncured for 60 days after written notice, (iii) by WuXi Biologics if we fail to make a payment and such failure continues for 30 days after receiving notice of such failure, or (iv) by either party upon the other party’s bankruptcy.
Competition
The biotechnology and biopharmaceutical industries are characterized by continuing technological advancement and significant competition. While we believe that our programs, technology, development experience and scientific knowledge provide us with competitive advantages, we face competition from major pharmaceutical and biotechnology companies, academic institutions, governmental agencies and public and private research institutions, among others. Any product candidates that we successfully develop and commercialize will compete with existing therapies and new therapies that may become available in the future. Many of the companies with which we are currently competing or will complete against in the future have significantly greater financial resources and expertise in research and development, manufacturing, preclinical testing, conducting clinical trials, obtaining regulatory approvals and marketing approved products than we do. Mergers and acquisitions in the pharmaceutical and biotechnology industry may result in even more resources being concentrated among a smaller number of our competitors. Smaller or early-stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies. These competitors also compete with us in recruiting and retaining qualified scientific and management personnel, establishing clinical trial sites, patient enrollment for clinical trials as well as in acquiring technologies complementary to, or necessary for, our programs. Key competitive factors affecting the success of all our product candidates that we develop, if approved, are likely to be efficacy, safety, convenience, presentation, price, the level of generic competition and the availability of reimbursement from government and other third-party payors. Our competitors may also obtain FDA or other regulatory approval for their products more rapidly than we may obtain approval for ours, which could result in our competitors establishing a strong market position before we are able to enter the market.
Specifically, there are several companies developing or marketing treatments that may be approved for the same indications and/or disease as our two most advanced programs, APG777 and APG808, and third and fourth programs, APG990 and APG222, including major pharmaceutical companies. We do not yet have clinical data for any of our programs and there can be no assurance that our programs will have similar or comparable results.
Over time, I&I markets have developed with a general increasing number of competitors, improved efficacy and improved dosing intervals (i.e. less frequent dosing). Psoriasis is one example of how an I&I market has developed.
58
ENBREL was first approved for psoriasis in 2004 with an every week maintenance dosing schedule. Four years after ENBREL’s approval for psoriasis, HUMIRA was approved in 2008 for psoriasis with an every other week dosing schedule. STELARA was approved a year later with similar Phase 3 data, as measured by the percentage of patients achieving PASI-75 (change in psoriasis area and severity index (PASI) score from baseline of at least 75%), but with a significantly improved dosing schedule of every twelve weeks. A number of psoriasis drugs have been approved since 2009 that demonstrated higher PASI-75 or PASI-90 scores in their pivotal studies as compared to STELARA, but have a more burdensome dosing schedule and have not been able to attain the same level of estimated psoriasis annual sales. Among those drugs are COSENTYX and TALTZ, which have dosing schedules of every four weeks. The only drug in the psoriasis market that is projected to achieve similar estimated psoriasis annual sales to STELARA is SKYRIZI, which has a similar dosing schedule of every twelve weeks, but also provided modest improvements in outcomes, as evidenced by higher PASI-75 scores in clinical trials. While the AD market has shown similarities to the psoriasis market to date, there can be no assurance that the AD market will develop in a similar or comparable manner to psoriasis.
There are several approved products for moderate-to-severe AD, such as dupilumab, an IL-4Rα mAb marketed as DUPIXENT by Sanofi/Regeneron, tralokinumab-ldrm, an IL-13 mAb marketed as ADBRY by LEO Pharmaceuticals, and nemolizumab, an anti-IL-31 mAb marketed in Japan as MITCHGA by Maruho Co., Ltd. There are several approved treatments that target JAK1 and/or JAK2 to treat AD, including abrocitinib, marketed as CIBINQO by Pfizer, and upadacitinib, marketed as RINVOQ by AbbVie.
Change in EASI score at 16 weeks is a common endpoint in AD. For example, the percentage of patients achieving EASI-75 on a placebo-adjusted basis in Phase 2 and average of Phase 3 monotherapy trials in AD were 59% and 62%, respectively, for upadacitinib at 30 mg dosed daily, 42% and 51%, respectively, for upadacitinib at 15 mg dosed daily, 36% and 38%, respectively, for lebrikizumab at 250 mg dosed every two weeks, 40% and 34%, respectively, for DUPIXENT at 300 mg dosed every two weeks, 49% and 51%, respectively, for abrocitinib at 200 mg dosed daily, and 25% and 21%, respectively, for abrocitinib at 100 mg dosed daily.
With respect to biologics with global Phase 3 data in AD, DUPIXENT, ADBRY, and lebrikizumab have all demonstrated statistically significant results.
In two Phase 3 trials of DUPIXENT dosed every two weeks in patients with AD, at 16 weeks, DUPIXENT showed 38.0% and 36.1% of treated patients achieved IGA 0/1 compared to 10.3% and 8.5% on placebo, respectively. Further, 51.3% and 44.2% of patients treated with DUPIXENT achieved EASI-75, compared to 14.7% and 11.9% on placebo, respectively. All differences were statistically significant. Of the 16-week responders who received DUPIXENT every two weeks during the induction period, 44% of patients dosed every four weeks and 54% of patients dosed every two weeks in the maintenance period achieved IGA 0/1 and 58% of patients dosed every four weeks and 72% of patients dosed every two weeks in the maintenance period achieved EASI-75 at 52 weeks.
In two Phase 3 trials of lebrikizumab dosed every two weeks in patients with AD, at 16 weeks, lebrikizumab showed 43.1% and 33.2% of treated patients achieved IGA 0/1 compared to 12.7% and 10.8% on placebo, respectively. Further, 58.8% and 52.1% of patients treated with lebrikizumab achieved EASI-75, compared to 16.2% and 18.1% of patients on placebo, respectively. All differences were statistically significant. Of the 16-week responders who received lebrikizumab every two weeks during the induction period, 78% of patients dosed every four weeks and 71% of patients dosed every two weeks in the maintenance period achieved IGA 0/1 and 82% of patients dosed every four weeks and 78% of patients dosed every two weeks in the maintenance period achieved EASI-75 at 52 weeks.
In two Phase 3 trials of ADBRY dosed every two weeks in patients with AD, at 16 weeks, ADBRY showed 15.8% and 22.2% of treated patients achieved IGA 0/1 compared to 7.1% and 10.9% on placebo, respectively. Further, 25.0% and 33.2% of patients treated with ADBRY achieved EASI-75, compared to 12.7% and 11.4% of patients on placebo, respectively. All differences were statistically significant.
We do not yet have clinical data in patients for our programs targeting IL-13 or IL-4Rα and there can be no assurance that our programs will have similar or comparable results.
59
We are also aware of several product candidates in clinical development for AD. Lebrikizumab is an IL-13 mAb from Eli Lilly and Company and Almirall, which is under review for potential approval by the FDA and, in 2023, received approval from the EMA. Nemolizumab is an IL-31R mAb from Galderma which had positive topline results in two Phase 3 trials showing 35.6% and 37.7% IGA 0/1 compared to 24.6% and 26.0% in the placebo group. For EASI-75, 43.5% and 42.1% of treated patients achieved the endpoint compared to 29.0% and 30.2% in the placebo group. Amlitelimab is an OX40L mAb, which is currently being evaluated in a Phase 3 trial by Sanofi and has demonstrated EASI-75 of 61.5% compared to 29.4% in the placebo group at week 16 when dosed every four weeks at 250 mg with a 500 mg loading dose (LD) in a Phase 2b trial.
22.1% of patients treated with amlitelimab 250 mg with LD achieved IGA0/1 at Week 16 compared to 5.1% of placebo patients. CBP-201 is an IL-4Rα mAb, which is currently being evaluated in a Phase 3 trial by Connect Biopharma and has demonstrated EASI-75 of 47% compared to 14% for placebo when dosed every two weeks in a Phase 2b trial. Rocatinlimab is an OX40 mAb, which is currently being evaluated in a Phase 3 trial by Amgen and Kyowa Kirin Co., Ltd. and has demonstrated EASI-75 of 54% compared to 11% for placebo in a Phase 2 trial. Eblasakimab, an IL-13Rα1 mAb being developed by ASLAN Pharmaceuticals, showed positive Phase 2b data with 600 mg Q4W leading to 52% of treated patients achieving EASI-75 versus 24.4% in the placebo group. For IGA 0/1, 31.2% of treated patients achieved the endpoint versus 15.1% in the placebo group. Other agents include ANB032, a BTLA antagonist, which is currently being evaluated in a Phase 2b trial by AnaptysBio; Rezpeg, a rIL-2 in Phase 2 trials by NEKTAR, and RAPT193, a CCR4 antagonist in Phase 2b trials by RAPT Therapeutics.
Advanced therapy penetration in AD is currently expected to ramp up from 8% in 2022 to approximately 25% by 2032. With more convenient and patient-friendly dosing, and potentially better efficacy, we believe that the market for future penetration of biologics could expand even beyond the projected 25%.
There are several approved products for COPD, however, there are no approved biologics. We are aware of several biologics in development, including DUPIXENT, for which Sanofi released positive data from two Phase 3 trials; itepekimab, an IL-33 mAb from Sanofi/Regeneron, which is currently being evaluated in a Phase 3 trial; tozorakimab, an IL-33 mAb from AstraZeneca, which is currently being evaluated in Phase 3 trials; benralizumab, an IL-5R mAb, from AstraZeneca, which is currently being evaluated in a Phase 3 trial; mepolizumab, an IL-5 mAb from GSK, which is currently being evaluated in a Phase 3 trial; tezepelumab, a TSLP mAb from AstraZeneca/Amgen, which is currently being evaluated in a Phase 2 trial; astegolimab, an ST2 mAb from Roche, which is currently being evaluated in Phase 2/3 trials; and ensifentrine, a PDE3/PDE4 inhibitor from Verona Pharma, which met the primary endpoint in two Phase 3 trials and has had an NDA accepted by the FDA.
Manufacturing and Supply
We do not own or operate, and currently have no plans to establish, any manufacturing facilities. All of our preclinical and clinical drug supply development, manufacturing, storage, distribution and testing are outsourced to third-party manufacturers and facilities. Our manufacturing strategy enables us to more efficiently direct financial resources to the research, development and commercialization of programs rather than diverting resources to internally develop and maintain manufacturing facilities. As our programs advance through development, we expect to enter into longer-term commercial supply agreements with key suppliers and manufacturers to fulfill and secure our supply needs.
With our contract development and manufacturing organizations, we have developed, or expect to develop, high yield, industry standard mAb drug manufacturing processes suitable for preclinical supply, as well as clinical and commercial scale manufacturing. We expect to use industry standard sterile liquid drug product manufacturing processes and to develop formulations and presentations that enable SQ delivery of all of our planned clinical development candidates. APG777 drug substance and drug product have been successfully manufactured at clinical scale with acceptable yields for near-term, planned clinical trials. Our initial formulation for APG777 is suitable for SQ injection. By the time of commercialization, we expect APG777 to be administrated via a pre-filled autoinjector. We use a similar approach to development and supply for our APG808 program. APG808 drug substance and drug product have been successfully manufactured at clinical scale with acceptable yields for use in our initial planned clinical trials.
60
While we expect to continue to devote significant resources to process development, scale-up and registration-enabling validation activities for APG777, we believe the manufacturing processes for mAbs such as APG777 are well established and should not create meaningful impediments to either clinical development or commercial launch. However, we will continue to identify additional second source drug substance and drug product contract manufacturers to ensure that we will have sufficient capacity as well as redundancy within our supply chain to avoid product shortages in the future. We will also continue to invest in development activities to ensure an acceptable cost of goods. We will also continue to apply mitigation strategies to ensure minimal disruption to our manufacturing supply due to any future global raw material supply chain shortages. We believe there are multiple sources for the raw materials required for the manufacture of our programs. While any reduction or halt in the supply of raw materials, drug substance or drug product could limit our ability to develop our programs until a replacement supplier or contract manufacturer is found and qualified, we believe that we have or will be able to manufacture sufficient clinical supply of APG777 and APG808, as well as future pipeline products, to support our near-term planned clinical trials, and have access to sufficient manufacturing capacity to support our planned clinical development program.
In light of the recently introduced BIOSECURE Act, which would prohibit federal agencies from entering into procurement contracts with an entity that uses biotechnology equipment or services from a biotechnology company of concern, we continue to take risk mitigation measures to reduce our supply chain risk in the event that WuXi Biologics or one of our other manufacturers or other supply chain vendors is impacted. We intend to continue to identify and select second source suppliers, including those based in the US and EU, for our contract development, manufacturing, testing, and storage needs. We will also continue to closely monitor geopolitical risk and implement additional mitigations and supply chain redundancies, as needed. See the section titled, Risk Factor - Risks Related to Our Reliance on Third Parties - “We currently rely, and plan to rely in the future, on third parties to conduct and support our preclinical studies and clinical trials. If these third parties do not properly and successfully carry out their contractual duties or meet expected deadlines, we may not be able to obtain regulatory approval of or commercialize our programs.”
For APG990 and APG222, we plan to follow a similar approach to APG777 and APG808 for the development and supply of preclinical, clinical and commercial material.
Intellectual Property
Overview
We strive to protect the proprietary programs and technologies that we believe are important to our business, including seeking and maintaining patent protection intended to cover the composition of matter of our programs, their methods of use, related technologies, diagnostics, and other inventions.
Patent Rights Relating to Our IL-13 Program
As of March 1, 2024, we own four patent families directed to antibodies that target IL-13, including APG777, pharmaceutical formulations, and methods of using those antibodies. The first patent family is directed to compositions of matter and includes an international (PCT) patent application and patent applications in Argentina and Taiwan. If issued, we would expect these patents to expire in 2043, absent any applicable patent term extensions. The second patent family is directed to methods of using APG777 and includes seven provisional applications. If the provisional patent applications are pursued non-provisionally and mature into one or more issued patents, we would expect those patents to expire in 2044, absent any applicable patent term extensions. The third patent family is directed to pharmaceutical formulations containing APG777 and includes one provisional application. If the provisional patent application is pursued non-provisionally and matures into one or more issued patents, we would expect those patents to expire in 2044, absent any applicable patent term extensions. The fourth patent family is directed to other APG777 compositions and includes one provisional application. If the provisional patent application is pursued non-provisionally and matures into one or more issued patents, we would expect those patents to expire in 2044, absent any applicable patent term extensions.
61
Patent Rights Relating to Our IL-4Ra Program
We have licensed one patent family from Paragon directed to antibodies that target IL-4Ra, including APG808, and methods of using those antibodies. As of March 1, 2024, this family includes an international (PCT) patent application and patent applications in Argentina and Taiwan. If these applications mature into one or more issued patents, we would expect those patents to expire in 2044, absent any applicable patent term extensions.
Patent Rights Relating to Our OX40L Program
We have licensed one patent family from Paragon directed to antibodies that target OX40L, including APG990, and methods of using those antibodies. As of March 1, 2024, this family includes two pending provisional patent applications. Any patents that grant from this family would be expected to expire in 2044, absent any applicable patent term extensions.
As indicated above, some of our owned and licensed patent applications are provisional patent applications. Provisional patent applications are not eligible to become issued patents until, among other things, we file a non-provisional patent application within 12 months of filing of one or more of our related provisional patent applications. If we do not timely file any non-provisional patent applications, we may lose our priority date with respect to our provisional patent applications and any patent protection on the inventions disclosed in our provisional patent applications. While we intend to timely file non-provisional patent applications relating to our provisional patent applications, we cannot predict whether any such patent applications will result in the issuance of patents that provide us with any competitive advantage. Moreover, the patent application and approval processes are expensive and time-consuming. We may not be able to file and prosecute all necessary or desirable patent applications at a reasonable cost or in a timely manner.
The term of individual patents depends upon the legal term for patents in the countries in which they are obtained. In most countries in which we have filed, including the United States, the patent term is 20 years from the earliest filing date of a non-provisional patent application. In the United States, a patent’s term may be lengthened by patent term adjustment, which compensates a patentee for administrative delays by the USPTO in examining and granting a patent, or may be shortened if a patent is terminally disclaimed over an earlier-filed patent. The term of a patent that covers a drug or biological product may also be eligible for patent term extension when FDA approval is granted for a portion of the term effectively lost as a result of the FDA regulatory review period, subject to certain limitations and provided statutory and regulatory requirements are met. Any such patent term extension can be for no more than five years, only one patent per approved product can be extended, the extension cannot extend the total patent term beyond 14 years from approval, and only those claims covering the approved drug, a method for using it or a method for manufacturing it may be extended. We may not receive an extension if we fail to exercise due diligence during the testing phase or regulatory review process, fail to apply within applicable deadlines, fail to apply prior to expiration of relevant patents, or otherwise fail to satisfy applicable requirements. Moreover, the length of the extension could be less than we request. In the future, if and when our product candidates receive approval from the FDA or foreign regulatory authorities, we expect to apply for patent term extensions on issued patents we may obtain in the future covering those products, depending upon the length of the clinical trials for each product and other factors. There can be no assurance that any of our pending patent applications will issue or that we will benefit from any patent term extension or favorable adjustment to the term of any of our patents.
As with other biotechnology and pharmaceutical companies, our ability to maintain and solidify our proprietary and intellectual property position for our product candidates will depend on our success in obtaining effective patent claims and enforcing those claims if granted. However, our owned and licensed pending patent applications, and any patent applications that we may in the future file or license from third parties, may not result in the issuance of patents. We also cannot predict the breadth of claims that may be allowed or enforced in our patents. Any issued patents that we may receive in the future may be challenged, invalidated, infringed or circumvented. In addition, because of the extensive time required for clinical development and regulatory review of a product candidate we may develop, it is possible that, before any of our product candidates can be commercialized, any related patent may expire or remain in force for only a short period following commercialization, thereby limiting the protection such patent would afford the respective product and any competitive advantage such patent may provide. For more information, see the section titled “Risk Factors — Risks Related to Intellectual Property”.
62
Other IP Rights
In addition to patents, we rely upon unpatented trade secrets, know-how and continuing technological innovation to develop and maintain our competitive position. However, trade secrets and know-how can be difficult to protect. We seek to protect our proprietary information, in part by executing confidentiality agreements with our collaborators and scientific advisors, and non-competition, non-solicitation, confidentiality and invention assignment agreements with our employees and consultants. We have also executed agreements requiring assignment of inventions with selected scientific advisors and collaborators. The confidentiality agreements we enter into are designed to protect our proprietary information and the agreements or clauses requiring assignment of inventions to us are designed to grant us ownership of technologies that are developed through our relationship with the respective counterparty. We cannot guarantee, however, that we have executed such agreements with all applicable counterparties, that such agreements will not be breached, or that these agreements will afford us adequate protection of our intellectual property and proprietary rights. For more information, see the section entitled “Risk Factors — Risks Related to Intellectual Property”.
Employees and Human Capital Resources
As of March 1, 2024, we had 91 full-time employees, 22 of whom have Ph.D. or M.D. degrees. Of these full-time employees, 62 employees are engaged in research and development. We also retain independent contractors as needed to support our organization’s needs. None of our employees are represented by labor unions or covered under collective bargaining agreements. We consider our relationship with our employees to be good.
We believe our employees are critical to our success and ability to achieve our business objectives. To that end, we are focused on retaining, developing and engaging our existing employees, and attracting high performing talent to join our team. Our rewards package (cash and equity-based compensation and 401(k) and health and welfare benefits plans) is a key tool in retaining, engaging and rewarding our team. We are also committed to the continued learning and development of our employees, which we believe will enable us to do our best work for patients. We encourage our team members to attend conferences and seminars and take continuing education courses to further their development.
We expect to continue to build our team to ensure we can effectively execute against our clinical plans. As we grow, we strive to retain the fast-paced, psychologically safe and entrepreneurial culture that embodies our four C.O.R.E. values: Caring, Original, Resilient and Egoless.
Government Regulation
The FDA and other regulatory authorities at federal, state and local levels, as well as in foreign countries, extensively regulate, among other things, the research, development, testing, manufacture, quality control, import, export, safety, effectiveness, labeling, packaging, storage, distribution, record keeping, approval, advertising, promotion, marketing, post-approval monitoring and post-approval reporting of biologics such as those we are developing. We, along with third-party contractors, will be required to navigate the various preclinical, clinical and commercial approval requirements of the governing regulatory agencies of the countries in which we wish to conduct studies or seek approval or licensure of our product candidates.
U.S. Biologics Regulation
In the United States, biological products are subject to regulation under the Federal Food, Drug, and Cosmetic Act (FDCA), the Public Health Service Act (PHSA) and other federal, state, local, and foreign statutes and regulations. The process of obtaining regulatory approvals and the subsequent compliance with appropriate federal, state, and local statutes and regulations requires the expenditure of substantial time and financial resources. Failure to comply with the applicable U.S. requirements at any time during the product development process, approval process or following approval may subject an applicant to administrative action and judicial sanctions. The process required by the FDA before biologic product candidates may be marketed in the United States generally involves the following:
| ● | completion of preclinical laboratory tests and animal studies performed in accordance with the FDA’s current Good Laboratory Practices (GLP) regulation; |
63
| ● | submission to the FDA of an IND, which must become effective before clinical trials may begin and must be updated annually or when significant changes are made; |
| ● | approval by an independent institutional review board (IRB), or ethics committee at each clinical site before the trial is commenced; |
| ● | manufacture of the proposed biologic candidate in accordance with cGMPs; |
| ● | performance of adequate and well-controlled human clinical trials in accordance with GCP requirements to establish the safety, purity and potency of the proposed biologic product candidate for its intended purpose; |
| ● | preparation of and submission to the FDA of a BLA, after completion of all pivotal clinical trials; |
| ● | satisfactory completion of an FDA Advisory Committee review, if applicable; |
| ● | a determination by the FDA within 60 days of its receipt of a BLA to file the application for review; |
| ● | satisfactory completion of an FDA pre-approval inspection of the manufacturing facility or facilities at which the proposed product is produced to assess compliance with cGMPs, and to assure that the facilities, methods and controls are adequate to preserve the biological product’s continued safety, purity and potency, and of selected clinical investigation sites to assess compliance with GCPs; and |
| ● | FDA review and approval of a BLA to permit commercial marketing of the product for particular indications for use in the United States. |
Preclinical and Clinical Development
Prior to beginning any clinical trial with a product candidate in the United States, we must submit an IND to the FDA. An IND is a request for authorization from the FDA to administer an investigational new drug product to humans. The central focus of an IND submission is on the general investigational plan and the protocol or protocols for preclinical studies and clinical trials. The IND also includes results of animal and in vitro studies assessing the toxicology, pharmacokinetics, pharmacology and pharmacodynamic characteristics of the product, chemistry, manufacturing and controls information, and any available human data or literature to support the use of the investigational product. An IND must become effective before human clinical trials may begin. The IND automatically becomes effective 30 days after receipt by the FDA, unless the FDA, within the 30-day period, raises safety concerns or questions about the proposed clinical trial. In such a case, the IND may be placed on clinical hold and the IND sponsor and the FDA must resolve any outstanding concerns or questions before the clinical trial can begin. Submission of an IND therefore may or may not result in FDA authorization to begin a clinical trial.
In addition to the IND submission process, supervision of human gene transfer trials includes evaluation and assessment by an institutional biosafety committee (IBC), a local institutional committee that reviews and oversees research utilizing recombinant or synthetic nucleic acid molecules at that institution. The IBC assesses the safety of the research and identifies any potential risk to public health or the environment and such review may result in some delay before initiation of a clinical trial.
Clinical trials involve the administration of the investigational product to human subjects under the supervision of qualified investigators in accordance with GCPs, which include the requirement that all research subjects provide their informed consent for their participation in any clinical study. Clinical trials are conducted under protocols detailing, among other things, the objectives of the study, the parameters to be used in monitoring safety and the effectiveness criteria to be evaluated. A separate submission to the existing IND must be made for each successive clinical trial conducted during product development and for any subsequent protocol amendments. Furthermore, an independent IRB for each site proposing to conduct the clinical trial must review and approve the plan for any clinical trial and its informed consent form before the clinical trial begins at that site, and must monitor the study until completed.
64
Regulatory authorities, the IRB or the sponsor may suspend a clinical trial at any time on various grounds, including a finding that the subjects are being exposed to an unacceptable health risk or that the trial is unlikely to meet its stated objectives. Some studies also include oversight by an independent group of qualified experts organized by the clinical study sponsor, known as a data safety monitoring board, which provides authorization for whether or not a study may move forward at designated check points based on access to certain data from the study and may halt the clinical trial if it determines that there is an unacceptable safety risk for subjects or other grounds, such as no demonstration of efficacy. There are also requirements governing the reporting of ongoing preclinical studies and clinical trials and clinical study results to public registries.
For purposes of BLA approval, human clinical trials are typically conducted in three sequential phases that may overlap.
| ● | Phase 1. The investigational product is initially introduced into healthy human subjects or patients with the target disease or condition. These studies are designed to test the safety, dosage tolerance, absorption, metabolism and distribution of the investigational product in humans, the side effects associated with increasing doses, and, if possible, to gain early evidence on effectiveness. |
| ● | Phase 2. The investigational product is administered to a limited patient population with a specified disease or condition to evaluate the preliminary efficacy, optimal dosages and dosing schedule and to identify possible adverse side effects and safety risks. Multiple Phase 2 clinical trials may be conducted to obtain information prior to beginning larger and more expensive Phase 3 clinical trials. |
| ● | Phase 3. The investigational product is administered to an expanded patient population to further evaluate dosage, to provide statistically significant evidence of clinical efficacy and to further test for safety, generally at multiple geographically dispersed clinical trial sites. These clinical trials are intended to establish the overall risk/benefit ratio of the investigational product and to provide an adequate basis for product approval. |
In some cases, the FDA may require, or companies may voluntarily pursue, additional clinical trials after a product is approved to gain more information about the product. These so-called Phase 4 studies may be made a condition to approval of the BLA. Concurrent with clinical trials, companies may complete additional animal studies and develop additional information about the biological characteristics of the product candidate, and must finalize a process for manufacturing the product in commercial quantities in accordance with cGMP requirements. The manufacturing process must be capable of consistently producing quality batches of the product candidate and, among other things, must develop methods for testing the identity, strength, quality and purity of the final product, or for biologics, the safety, purity and potency. Additionally, appropriate packaging must be selected and tested and stability studies must be conducted to demonstrate that the product candidate does not undergo unacceptable deterioration over its shelf life.
A sponsor may choose, but is not required, to conduct a foreign clinical study under an IND. When a foreign clinical study is conducted under an IND, all IND requirements must be met unless waived. When the foreign clinical study is not conducted under an IND, the sponsor must ensure that the study complies with certain FDA regulatory requirements in order to use the study as support for an IND or application for marketing approval or licensure, including that the study was conducted in accordance with GCP, including review and approval by an independent ethics committee and use of proper procedures for obtaining informed consent from subjects, and the FDA is able to validate the data from the study through an onsite inspection if the FDA deems such inspection necessary. The GCP requirements encompass both ethical and data integrity standards for clinical studies.
BLA Submission and Review
Assuming successful completion of all required testing in accordance with all applicable regulatory requirements, the results of product development, nonclinical studies and clinical trials are submitted to the FDA as part of a BLA requesting approval to market the product for one or more indications. The BLA must include all relevant data available from pertinent preclinical studies and clinical trials, including negative or ambiguous results as well as positive findings, together with detailed information relating to the product’s chemistry, manufacturing, controls, and proposed labeling, among other things.
65
Data can come from company-sponsored clinical studies intended to test the safety and effectiveness of the product, or from a number of alternative sources, including studies initiated and sponsored by investigators. The submission of a BLA requires payment of a substantial application user fee to the FDA, unless a waiver or exemption applies.
In addition, under the Pediatric Research Equity Act (PREA), a BLA or supplement to a BLA must contain data to assess the safety and effectiveness of the biological product candidate for the claimed indications in all relevant pediatric subpopulations and to support dosing and administration for each pediatric subpopulation for which the product is safe and effective. The Food and Drug Administration Safety and Innovation Act requires that a sponsor who is planning to submit a marketing application for a biological product that includes a new active ingredient, new indication, new dosage form, new dosing regimen or new route of administration submit an initial pediatric study plan (PSP) within sixty days after an end-of-Phase 2 meeting or as may be agreed between the sponsor and FDA. Unless otherwise required by regulation, PREA does not apply to any biological product for an indication for which orphan designation has been granted.
Within 60 days following submission of the application, the FDA reviews a BLA submitted to determine if it is substantially complete before the agency accepts it for filing. The FDA may refuse to file any BLA that it deems incomplete or not properly reviewable at the time of submission and may request additional information. In this event, the BLA must be resubmitted with the additional information. Once a BLA has been accepted for filing, the FDA’s goal is to review standard applications within ten months after the filing date, or, if the application qualifies for priority review, six months after the FDA accepts the application for filing. In both standard and priority reviews, the review process may also be extended by FDA requests for additional information or clarification. The FDA reviews a BLA to determine, among other things, whether a product is safe, pure and potent and the facility in which it is manufactured, processed, packed or held meets standards designed to assure the product’s continued safety, purity and potency. The FDA may convene an advisory committee to provide clinical insight on application review questions. The FDA is not bound by the recommendations of an advisory committee, but it considers such recommendations carefully when making decisions. Before approving a BLA, the FDA will typically inspect the facility or facilities where the product is manufactured. The FDA will not approve an application unless it determines that the manufacturing processes and facilities are in compliance with cGMP requirements and adequate to assure consistent production of the product within required specifications. Additionally, before approving a BLA, the FDA will typically inspect one or more clinical sites to assure compliance with GCPs. If the FDA determines that the application, manufacturing process or manufacturing facilities are not acceptable, it will outline the deficiencies in the submission and often will request additional testing or information. Notwithstanding the submission of any requested additional information, the FDA ultimately may decide that the application does not satisfy the regulatory criteria for approval.
After the FDA evaluates a BLA and conducts inspections of manufacturing facilities where the investigational product and/or its drug substance will be produced, the FDA may issue an approval letter or a Complete Response letter. An approval letter authorizes commercial marketing of the product with specific prescribing information for specific indications. A Complete Response letter will describe all of the deficiencies that the FDA has identified in the BLA, except that where the FDA determines that the data supporting the application are inadequate to support approval, the FDA may issue the Complete Response letter without first conducting required inspections, testing submitted product lots and/or reviewing proposed labeling. In issuing the Complete Response letter, the FDA may recommend actions that the applicant might take to place the BLA in condition for approval, including requests for additional information or clarification. The FDA may delay or refuse approval of a BLA if applicable regulatory criteria are not satisfied, require additional testing or information and/or require post-marketing testing and surveillance to monitor safety or efficacy of a product.
If regulatory approval of a product is granted, such approval will be granted for particular indications and may entail limitations on the indicated uses for which such product may be marketed. For example, the FDA may approve the BLA with a REMS to ensure the benefits of the product outweigh its risks. A REMS is a safety strategy to manage a known or potential serious risk associated with a product and to enable patients to have continued access to such medicines by managing their safe use, and could include medication guides, physician communication plans, or elements to assure safe use, such as restricted distribution methods, patient registries and other risk minimization tools. The FDA also may condition approval on, among other things, changes to proposed labeling or the development of adequate controls and specifications. Once approved, the FDA may withdraw the product approval if compliance with pre-and post-marketing requirements is not maintained or if problems occur after the product reaches the marketplace.
66
The FDA may require one or more Phase 4 post-market studies and surveillance to further assess and monitor the product’s safety and effectiveness after commercialization, and may limit further marketing of the product based on the results of these post-marketing studies.
Expedited Development and Review Programs
The FDA offers a number of expedited development and review programs for qualifying product candidates. The fast track program is intended to expedite or facilitate the process for reviewing new products that meet certain criteria. Specifically, new products are eligible for fast track designation if they are intended to treat a serious or life-threatening disease or condition and data demonstrate the potential to address unmet medical needs for the disease or condition. Fast track designation applies to the combination of the product and the specific indication for which it is being studied. The sponsor of a fast track product has opportunities for more frequent interactions with the review team during product development and, once a BLA is submitted, the product may be eligible for priority review. A fast track product may also be eligible for rolling review, where the FDA may consider for review sections of the BLA on a rolling basis before the complete application is submitted, if the sponsor provides a schedule for the submission of the sections of the BLA, the FDA agrees to accept sections of the BLA and determines that the schedule is acceptable, and the sponsor pays any required user fees upon submission of the first section of the BLA.
A product intended to treat a serious or life-threatening disease or condition may also be eligible for breakthrough therapy designation to expedite its development and review. A product can receive breakthrough therapy designation if preliminary clinical evidence indicates that the product, alone or in combination with one or more other drugs or biologics, may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints, such as substantial treatment effects observed early in clinical development. The designation includes all of the fast track program features, as well as more intensive FDA interaction and guidance beginning as early as Phase 1 and an organizational commitment to expedite the development and review of the product, including involvement of senior managers.
Any marketing application for a biologic submitted to the FDA for approval, including a product with a fast track designation and/or breakthrough therapy designation, may be eligible for other types of FDA programs intended to expedite the FDA review and approval process, such as priority review and accelerated approval. A product is eligible for priority review if there is evidence it has the potential to provide a significant improvement in the treatment, diagnosis or prevention of a serious disease or condition. For original BLAs, priority review designation means the FDA’s goal is to take action on the marketing application within six months of the 60-day filing date (as compared to ten months under standard review).
Additionally, products studied for their safety and effectiveness in treating serious or life-threatening diseases or conditions may receive accelerated approval upon a determination that the product has an effect on a surrogate endpoint that is reasonably likely to predict clinical benefit, or on a clinical endpoint that can be measured earlier than irreversible morbidity or mortality, that is reasonably likely to predict an effect on irreversible morbidity or mortality or other clinical benefit, taking into account the severity, rarity, or prevalence of the condition and the availability or lack of alternative treatments. As a condition of accelerated approval, the FDA will generally require the sponsor to perform adequate and well-controlled post-marketing clinical studies to verify and describe the anticipated effect on irreversible morbidity or mortality or other clinical benefit. Under the Food and Drug Omnibus Reform Act of 2022, the FDA may require, as appropriate, that such studies be underway prior to approval or within a specific time period after the date of approval for a product granted accelerated approval. Products receiving accelerated approval may be subject to expedited withdrawal procedures if the sponsor fails to conduct the required post-marketing studies or if such studies fail to verify the predicted clinical benefit. In addition, the FDA currently requires as a condition for accelerated approval pre-approval of promotional materials, which could adversely impact the timing of the commercial launch of the product.
Fast track designation, breakthrough therapy designation and priority review do not change the standards for approval but may expedite the development or approval process. Even if a product qualifies for one or more of these programs, the FDA may later decide that the product no longer meets the conditions for qualification or decide that the time period for FDA review or approval will not be shortened.
67
Post-Approval Requirements
Any products manufactured or distributed by us pursuant to FDA approvals are subject to pervasive and continuing regulation by the FDA, including, among other things, requirements relating to record-keeping, reporting of adverse experiences, periodic reporting, product sampling and distribution, and advertising and promotion of the product. After approval, most changes to the approved product, such as adding new indications or other labeling claims, are subject to prior FDA review and approval. There also are continuing user fee requirements, under which the FDA assesses an annual program fee for each product identified in an approved BLA. Biologic manufacturers and their subcontractors are required to register their establishments with the FDA and certain state agencies, and are subject to periodic unannounced inspections by the FDA and certain state agencies for compliance with cGMPs, which impose certain procedural and documentation requirements upon us and our third-party manufacturers. Changes to the manufacturing process are strictly regulated, and, depending on the significance of the change, may require prior FDA approval before being implemented.
FDA regulations also require investigation and correction of any deviations from cGMPs and impose reporting requirements upon us and any third-party manufacturers that we may decide to use. Accordingly, manufacturers must continue to expend time, money and effort in the area of production and quality control to maintain compliance with cGMPs and other aspects of regulatory compliance.
The FDA may withdraw approval if compliance with regulatory requirements and standards is not maintained or if problems occur after the product reaches the market. Later discovery of previously unknown problems with a product, including adverse events of unanticipated severity or frequency, or with manufacturing processes, or failure to comply with regulatory requirements, may result in revisions to the approved labeling to add new safety information; imposition of post-market studies or clinical studies to assess new safety risks; or imposition of distribution restrictions or other restrictions under a REMS program. Other potential consequences include, among other things:
| ● | restrictions on the marketing or manufacturing of a product, complete withdrawal of the product from the market or product recalls; |
| ● | fines, warning letters or holds on post-approval clinical studies; |
| ● | refusal of the FDA to approve pending applications or supplements to approved applications, or suspension or revocation of existing product approvals; |
| ● | product seizure or detention, or refusal of the FDA to permit the import or export of products; |
| ● | consent decrees, corporate integrity agreements, debarment or exclusion from federal healthcare programs; |
| ● | mandated modification of promotional materials and labeling and the issuance of corrective information; |
| ● | the issuance of safety alerts, Dear Healthcare Provider letters, press releases and other communications containing warnings or other safety information about the product; or |
| ● | injunctions or the imposition of civil or criminal penalties. |
The FDA closely regulates the marketing, labeling, advertising and promotion of biologics. A company can make only those claims relating to safety and efficacy, purity and potency that are approved by the FDA and in accordance with the provisions of the approved label. The FDA and other agencies actively enforce the laws and regulations prohibiting the promotion of off-label uses. Failure to comply with these requirements can result in, among other things, adverse publicity, warning letters, corrective advertising and potential civil and criminal penalties. Physicians may prescribe legally available products for uses that are not described in the product’s labeling and that differ from those tested by us and approved by the FDA. Such off-label uses are common across medical specialties. Physicians may believe that such off-label uses are the best treatment for many patients in varied circumstances. The FDA does not regulate the behavior of physicians in their choice of treatments.
68
The FDA does, however, restrict manufacturer’s communications on the subject of off-label use of their products.
Biosimilars and Reference Product Exclusivity
The ACA includes a subtitle called the BPCIA, which created an abbreviated approval pathway for biological products that are highly similar, or “biosimilar,” to or interchangeable with an FDA-approved reference biological product. The FDA has issued several guidance documents outlining an approach to review and approval of biosimilars.
Biosimilarity, which requires that there be no clinically meaningful differences between the biological product and the reference product in terms of safety, purity, and potency, is generally shown through analytical studies, animal studies, and a clinical study or studies. Interchangeability requires that a product is biosimilar to the reference product and the product must demonstrate that it can be expected to produce the same clinical results as the reference product in any given patient and, for products that are administered multiple times to an individual, the biologic and the reference biologic may be alternated or switched after one has been previously administered without increasing safety risks or risks of diminished efficacy relative to exclusive use of the reference biologic. A product shown to be biosimilar or interchangeable with an FDA-approved reference biological product may rely in part on the FDA’s previous determination of safety and effectiveness for the reference product for approval, which can potentially reduce the cost and time required to obtain approval to market the product. Complexities associated with the larger, and often more complex, structures of biological products, as well as the processes by which such products are manufactured, pose significant hurdles to implementation of the abbreviated approval pathway that are still being worked out by the FDA.
In September 2021, the FDA issued two guidance documents intended to inform prospective applicants and facilitate the development of proposed biosimilars and interchangeable biosimilars, as well as to describe the FDA’s interpretation of certain statutory requirements added by the BPCIA.
Under the BPCIA, an application for a biosimilar product may not be submitted to the FDA until four years following the date that the reference product was first licensed by the FDA. In addition, the approval of a biosimilar product may not be made effective by the FDA until 12 years from the date on which the reference product was first licensed. During this 12-year period of exclusivity, another company may still market a competing version of the reference product if the FDA approves a full BLA for the competing product containing that applicant’s own preclinical data and data from adequate and well-controlled clinical trials to demonstrate the safety, purity and potency of its product. The BPCIA also created certain exclusivity periods for biosimilars approved as interchangeable products. At this juncture, it is unclear whether products deemed “interchangeable” by the FDA will, in fact, be readily substituted by pharmacies, which are governed by state pharmacy law.
A reference biologic is granted twelve years of exclusivity from the time of first licensure of the reference product. The first biologic product submitted under the abbreviated approval pathway that is determined to be interchangeable with the reference product has exclusivity against other biologics submitted under the abbreviated approval pathway for the lesser of (i) one year after the first commercial marketing, (ii) 18 months after approval if there is no legal challenge, (iii) 18 months after the resolution in the applicant’s favor of a lawsuit challenging the biologics’ patents if an application has been submitted, or (iv) 42 months after the application has been approved if a lawsuit is ongoing within the 42-month period.
A biological product can also obtain pediatric market exclusivity in the United States. Pediatric exclusivity, if granted, adds six months to existing exclusivity periods and patent terms. This six-month exclusivity, which runs from the end of other exclusivity protection or patent term, may be granted based on the voluntary completion of a pediatric study in accordance with an FDA-issued “Written Request” for such a study.
The BPCIA is complex and continues to be interpreted and implemented by the FDA. In July 2018, the FDA announced an action plan to encourage the development and efficient review of biosimilars, including the establishment of a new office within the agency that will focus on therapeutic biologics and biosimilars. On December 20, 2020, Congress amended the PHSA as part of the COVID-19 relief bill to further simplify the biosimilar review process by making it optional to show that conditions of use proposed in labeling have been previously approved for the reference product, which used to be a requirement of the application.
69
In addition, government proposals have sought to reduce the 12-year reference product exclusivity period. Other aspects of the BPCIA, some of which may impact the BPCIA exclusivity provisions, have also been the subject of recent litigation. As a result, the ultimate impact, implementation, and impact of the BPCIA is subject to significant uncertainty.
As discussed below, the Inflation Reduction Act of 2022 (IRA) is a significant new law that intends to foster generic and biosimilar competition and to lower drug and biologic costs.
Other Healthcare Laws and Compliance Requirements
Pharmaceutical companies are subject to additional healthcare regulation and enforcement by the federal government and by authorities in the states and foreign jurisdictions in which they conduct their business. Such laws include, without limitation: the federal Anti-Kickback Statute (AKS); the federal False Claims Act (FCA); the Health Insurance Portability and Accountability Act of 1996 (HIPAA) and similar foreign, federal and state fraud, abuse and transparency laws.
The AKS prohibits, among other things, persons and entities from knowingly and willfully soliciting, receiving, offering or paying remuneration, to induce, or in return for, either the referral of an individual, or the purchase or recommendation of an item or service for which payment may be made under any federal healthcare program. The term remuneration has been interpreted broadly to include anything of value. The AKS has been interpreted to apply to arrangements between pharmaceutical manufacturers on one hand, and prescribers and purchasers on the other. The government often takes the position that to violate the AKS, only one purpose of the remuneration need be to induce referrals, even if there are other legitimate purposes for the remuneration. There are a number of statutory exceptions and regulatory safe harbors protecting some common activities from AKS prosecution, but they are drawn narrowly and practices that involve remuneration, such as consulting agreements, that may be alleged to be intended to induce prescribing, purchasing or recommending may be subject to scrutiny if they do not qualify for an exception or safe harbor. Our practices may not in all cases meet all of the criteria for protection under a statutory exception or regulatory safe harbor. Failure to meet all of the requirements of a particular applicable statutory exception or regulatory safe harbor does not make the conduct per se illegal under the AKS. Instead, the legality of the arrangement will be evaluated on a case-by-case basis based on a cumulative review of all of its facts and circumstances. A person or entity does not need to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation.
Civil and criminal false claims laws, including the FCA, and civil monetary penalty laws, which can be enforced through civil whistleblower or qui tam actions, prohibit, among other things, individuals or entities from knowingly presenting, or causing to be presented, claims for payment of federal government funds, including in federal healthcare programs, that are false or fraudulent. Pharmaceutical and other healthcare companies have been prosecuted under these laws for engaging in a variety of different types of conduct that caused the submission of false claims to federal healthcare programs. Under the AKS, for example, a claim resulting from a violation of the AKS is deemed to be a false or fraudulent claim for purposes of the FCA.
HIPAA created additional federal criminal statutes that prohibit, among other things, executing a scheme to defraud any healthcare benefit program, including private third-party payors, and making false statements relating to healthcare matters. A person or entity does not need to have actual knowledge of the healthcare fraud statute implemented under HIPAA or specific intent to violate the statute in order to have committed a violation.
The FDCA addresses, among other things, the design, production, labeling, promotion, manufacturing, and testing of drugs, biologics and medical devices, and prohibits such acts as the introduction into interstate commerce of adulterated or misbranded drugs or devices. The PHSA also prohibits the introduction into interstate commerce of unlicensed or mislabeled biological products.
The U.S. federal Physician Payments Sunshine Act requires certain manufacturers of drugs, devices, biologics and medical supplies for which payment is available under Medicare, Medicaid or the Children’s Health Insurance Program, with specific exceptions, to annually report to the Centers for Medicaid & Medicare Services (CMS) information related to payments or other transfers of value to various healthcare professionals including physicians, physician assistants, nurse practitioners, clinical nurse specialists, certified nurse anesthetists, certified nurse-midwives, and teaching hospitals, as well as ownership and investment interests held by physicians and their immediate family members.
70
Beginning on January 1, 2023, California Assembly Bill 1278 requires California physicians and surgeons to notify patients of the Open Payments database established under the federal Physician Payments Sunshine Act.
We are also subject to additional similar U.S. state and foreign law equivalents of each of the above federal laws, which, in some cases, differ from each other in significant ways, and may not have the same effect, thus complicating compliance efforts. If our operations are found to be in violation of any of such laws or any other governmental regulations that apply, we may be subject to penalties, including, without limitation, civil, criminal and administrative penalties, damages, fines, exclusion from government-funded healthcare programs, such as Medicare and Medicaid or similar programs in other countries or jurisdictions, integrity oversight and reporting obligations to resolve allegations of non-compliance, disgorgement, individual imprisonment, contractual damages, reputational harm, diminished profits and the curtailment or restructuring of our operations.
Data Privacy and Security
Numerous state, federal, and foreign laws govern the collection, dissemination, use, access to, confidentiality, and security of personal information, including health-related information. In the United States, numerous federal and state laws and regulations, including state data breach notification laws, state health information privacy laws, and federal and state consumer protection laws and regulations, govern the collection, use, disclosure, and protection of health-related and other personal information could apply to our operations or the operations of our partners.
For example, HIPAA, as amended by the Health Information Technology for Economic and Clinical Health (HITECH), and their respective implementing regulations imposes data privacy, security, and breach notification obligations on certain health care providers, health plans, and health care clearinghouses, known as covered entities, as well as their business associates and their covered subcontractors that perform certain services that involve using, disclosing, creating, receiving, maintaining, or transmitting individually identifiable protected health information (PHI) for or on behalf of such covered entities. These requirements imposed by HIPAA and the HITECH Act on covered entities and business associates include entering into agreements that require business associates protect PHI provided by the covered entity against improper use or disclosure, among other things; following certain standards for the privacy of PHI, which limit the disclosure of a patient’s past, present, or future physical or mental health or condition or information about a patient’s receipt of health care if the information identifies, or could reasonably be used to identify, the individual; ensuring the confidentiality, integrity, and availability of all PHI created, received, maintained, or transmitted in electronic form, to identify and protect against reasonably anticipated threats or impermissible uses or disclosures to the security and integrity of such PHI; and reporting of breaches of PHI to individuals and regulators.
Entities that are found to be in violation of HIPAA may be subject to significant civil, criminal, and administrative fines and penalties and/or additional reporting and oversight obligations if required to enter into a resolution agreement and corrective action plan with HHS to settle allegations of HIPAA non-compliance. A covered entity or business associate is also liable for civil money penalties for a violation that is based on an act or omission of any of its agents, which may include a downstream business associate, as determined according to the federal common law of agency. HITECH also increased the civil and criminal penalties applicable to covered entities and business associates and gave state attorneys general new authority to file civil actions for damages or injunctions in federal courts to enforce HIPAA and seek attorneys’ fees and costs associated with pursuing federal civil actions. To the extent that we submit electronic healthcare claims and payment transactions that do not comply with the electronic data transmission standards established under HIPAA and HITECH, payments to us may be delayed or denied.
Even when HIPAA does not apply, according to the FTC, violating consumers’ privacy rights or failing to take appropriate steps to keep consumers’ personal information secure may constitute unfair acts or practices in or affecting commerce in violation of Section 5(a) of the Federal Trade Commission Act.
In addition, certain state laws, such as the California Consumer Privacy Act of 2018 (CCPA), as amended by the California Privacy Rights Act of 2020 (CPRA), govern the privacy and security of personal information, including health-related information in certain circumstances, some of which are more stringent than HIPAA and many of which differ from each other in significant ways and may not have the same effect, thus complicating compliance efforts.
71
The CCPA/CPRA applies to personal data of consumers, business representatives, and employees, and imposes obligations on certain businesses that do business in California, including to provide specific disclosures in privacy notices, rights to California residents in relation to their personal information. Health information falls under the CCPA/CPRA’s definition of personal information where it identifies, relates to, describes, or is reasonably capable of being associated with or could reasonably be linked with a particular consumer or household — unless it is subject to HIPAA — and is included under a new category of personal information, “sensitive personal information,” which is offered greater protection.
Failure to comply with these laws, where applicable, can result in the imposition of significant civil and/or criminal penalties and private litigation. Privacy and security laws, regulations, and other obligations are constantly evolving, may conflict with each other to complicate compliance efforts, and can result in investigations, proceedings, or actions that lead to significant civil and/or criminal penalties and restrictions on data processing. Additionally, our use of artificial intelligence and machine learning may be subject to laws and evolving regulations regarding the use of artificial intelligence/machine learning, controlling for data bias, and antidiscrimination.
In addition, the CPRA expands the CCPA’s requirements, including by adding a new right for individuals to correct their personal information and establishing a new regulatory agency to implement and enforce the law.
Other states, such as Virginia, Colorado, Connecticut and Utah, have also passed comprehensive privacy laws, and similar laws are being considered in several other states, as well as at the federal and local levels.
While the laws in these states, like the CCPA, also exempt some data processed in the context of clinical trials, such developments further complicate compliance efforts, and increase legal risk and compliance costs for us and the third parties upon whom we rely.
Coverage and Reimbursement
Significant uncertainty exists as to the coverage and reimbursement status of any pharmaceutical or biological product for which we obtain regulatory approval. Sales of any product, if approved, depend, in part, on the extent to which such product will be covered by third-party payors, such as federal, state, and foreign government healthcare programs, commercial insurance and managed healthcare organizations, and the level of reimbursement, if any, for such product by third-party payors. Decisions regarding whether to cover any of our product candidates, if approved, the extent of coverage and amount of reimbursement to be provided are made on a plan-by-plan basis. Further, no uniform policy for coverage and reimbursement exists in the United States, and coverage and reimbursement can differ significantly from payor to payor. Third-party payors often rely upon Medicare coverage policy and payment limitations in setting their own reimbursement rates, but also have their own methods and approval process apart from Medicare determinations. As a result, the coverage determination process is often a time-consuming and costly process that will require us to provide scientific and clinical support for the use of our product candidates to each payor separately, with no assurance that coverage and adequate reimbursement will be applied consistently or obtained in the first instance.
Third-party payors are increasingly challenging the prices charged for medical products and services, examining the medical necessity and reviewing the cost effectiveness of pharmaceutical or biological products, medical devices and medical services, in addition to questioning safety and efficacy. Adoption of price controls and cost-containment measures, and adoption of more restrictive policies in jurisdictions with existing controls and measures, could further limit sales of any product that receives approval. Decreases in third-party reimbursement for any product or a decision by a third-party not to cover a product could reduce physician usage and patient demand for the product.
For products administered under the supervision of a physician, obtaining coverage and adequate reimbursement may be particularly difficult because of the higher prices often associated with such drugs. Additionally, separate reimbursement for the product itself or the treatment or procedure in which the product is used may not be available, which may impact physician utilization. In addition, companion diagnostic tests require coverage and reimbursement separate and apart from the coverage and reimbursement for their companion pharmaceutical or biological products. Similar challenges to obtaining coverage and reimbursement, applicable to pharmaceutical or biological products, will apply to companion diagnostics.
72
In addition, the U.S. government, state legislatures and foreign governments have continued implementing cost-containment programs, including price controls, restrictions on coverage and reimbursement and requirements for substitution of generic products. The IRA provides CMS with significant new authorities intended to curb drug costs and to encourage market competition. For the first time, CMS will be able to directly negotiate prescription drug prices and to cap out-of-pocket costs. Each year, CMS will select and negotiate a preset number of high-spend drugs and biologics that are covered under Medicare Part B and Part D that do not have generic or biosimilar competition. On August 29, 2023, HHS announced the list of the first ten drugs that will be subject to price negotiations. These price negotiations will begin in 2023, although the Medicare drug price negotiation program is currently subject to legal challenges. The IRA also provides a new “inflation rebate” covering Medicare patients that will take effect in 2023 and is intended to counter certain price increases in prescriptions drugs. The inflation rebate provision will require drug manufacturers to pay a rebate to the federal government if the price for a drug or biologic under Medicare Part B and Part D increases faster than the rate of inflation. To support biosimilar competition, beginning in October 2022, qualifying biosimilars may receive a Medicare Part B payment increase for a period of five years. Separately, if a biologic drug for which no biosimilar exists delays a biosimilar’s market entry beyond two years, CMS will be authorized to subject the biologics manufacturer to price negotiations intended to ensure fair competition. Notwithstanding these provisions, the IRA’s impact on commercialization and competition remains largely uncertain.
Healthcare Reform
The United States and some foreign jurisdictions are considering or have enacted a number of reform proposals to change the healthcare system. There is significant interest in promoting changes in healthcare systems with the stated goals of containing healthcare costs, improving quality or expanding access. In the United States, the pharmaceutical industry has been a particular focus of these efforts and has been significantly affected by federal and state legislative initiatives, including those designed to limit the pricing, coverage, and reimbursement of pharmaceutical and biopharmaceutical products, especially under government-funded health care programs, and increased governmental control of drug pricing.
The ACA, which was enacted in March 2010, substantially changed the way healthcare is financed by both governmental and private insurers in the United States, and significantly affected the pharmaceutical industry. The ACA contains a number of provisions of particular import to the pharmaceutical and biotechnology industries, including, but not limited to, those governing enrollment in federal healthcare programs, a new methodology by which rebates owed by manufacturers under the Medicaid Drug Rebate Program are calculated for drugs that are inhaled, infused, instilled, implanted or injected, and annual fees based on pharmaceutical companies’ share of sales to federal health care programs. Since its enactment, there have been judicial and Congressional challenges to certain aspects of the ACA, and we expect there will be additional challenges and amendments to the ACA in the future. For example, the IRA, among other things, extends enhanced subsidies for individuals purchasing health insurance coverage in ACA marketplaces through plan year 2025. The IRA also eliminates the “donut hole” under the Medicare Part D program beginning in 2025 by significantly lowering the beneficiary maximum out-of-pocket cost and creating a new manufacturer discount program.
Other legislative changes have been proposed and adopted since the ACA was enacted, including automatic aggregate reductions of Medicare payments to providers of on average 2% per fiscal year as part of the federal budget sequestration under the Budget Control Act of 2011. These reductions went into effect in April 2013 and, due to subsequent legislative amendments, will remain in effect until 2032 unless additional action is taken by Congress. In addition, the Bipartisan Budget Act of 2018, among other things, amended the Medicare Act (as amended by the ACA) to increase the point-of-sale discounts that manufacturers must agree to offer under the Medicare Part D coverage discount program from 50% to 70% off negotiated prices of applicable brand drugs to eligible beneficiaries during their coverage gap period, as a condition for the manufacturer’s outpatient drugs being covered under Medicare Part D.
Moreover, there has recently been heightened governmental scrutiny over the manner in which manufacturers set prices for their marketed products, which has resulted in several Congressional inquiries and proposed and enacted federal and state measures designed to, among other things, reduce the cost of prescription drugs, bring more transparency to product pricing, review the relationship between pricing and manufacturer patient programs, and reform government program reimbursement methodologies for drug products. For example, in May 2019, CMS adopted a final rule allowing Medicare Advantage Plans the option to use step therapy for Part B drugs, permitting Medicare Part D plans to apply certain utilization controls to new starts of five of the six protected class drugs, and requiring the Explanation of Benefits for Part D beneficiaries to disclose drug price increases and lower cost therapeutic alternatives, which went into effect on January 1, 2021.
73
In response to the Biden administration’s October 2022 executive order, on February 14, 2023, HHS released a report outlining three new models for testing by the CMS Innovation Center which will be evaluated on their ability to lower the cost of drugs, promote accessibility, and improve quality of care. It is unclear whether the models will be utilized in any health reform measures in the future. Further, on December 7, 2023, the Biden administration announced an initiative to control the price of prescription drugs through the use of march-in rights under the Bayh-Dole Act. On December 8, 2023, the National Institute of Standards and Technology published for comment a Draft Interagency Guidance Framework for Considering the Exercise of March-In Rights which for the first time includes the price of a product as one factor an agency can use when deciding to exercise march-in rights. While march-in rights have not previously been exercised, it is uncertain if that will continue under the new framework.
Notwithstanding the IRA, continued legislative and enforcement interest exists in the United States with respect to specialty drug pricing practices. Specifically, we expect regulators to continue pushing for transparency to drug pricing, reducing the cost of prescription drugs under Medicare, reviewing the relationship between pricing and manufacturer patient programs, and reforming government program reimbursement methodologies for drugs.
Other Government Regulation Outside of the United States
In addition to regulations in the United States, we are subject to a variety of regulations in other jurisdictions governing, among other things, research and development, clinical trials, testing, manufacturing, safety, efficacy, quality control, labeling, packaging, storage, record keeping, distribution, reporting, export and import, advertising, marketing and other promotional practices involving biological products as well as authorization, approval as well as post-approval monitoring and reporting of our products. Because biologically sourced raw materials are subject to unique contamination risks, their use may be restricted in some countries.
Whether or not we obtain FDA approval for a product, we must obtain the requisite approvals from regulatory authorities in foreign countries prior to the commencement of clinical trials or marketing of the product in those countries. Certain countries outside of the United States have a similar process that requires the submission of a clinical trial application much like the IND prior to the commencement of human clinical trials.
The requirements and process governing the conduct of clinical trials, including requirements to conduct additional clinical trials, product licensing, safety reporting, post-authorization requirements, marketing and promotion, interactions with healthcare professionals, pricing and reimbursement may vary widely from country to country. No action can be taken to market any product in a country until an appropriate approval application has been approved by the regulatory authorities in that country. The current approval process varies from country to country, and the time spent in gaining approval varies from that required for FDA approval. In certain countries, the sales price of a product must also be approved. The pricing review period often begins after market approval is granted. Even if a product is approved by a regulatory authority, satisfactory prices may not be approved for such product, which would make launch of such products commercially unfeasible in such countries.
Regulation in the European Union
European Data Laws
The collection and use of personal health data and other personal data in the EU is governed by the provisions of the European General Data Protection Regulation (EU) 2016/679 (GDPR), which came into force in May 2018, and related data protection laws in individual EU Member States. The GDPR imposes a number of strict obligations and restrictions on the ability to process, including collecting, analyzing and transferring, personal data of individuals, in particular with respect to health data from clinical trials and adverse event reporting. The GDPR includes requirements relating to the legal basis of the processing (such as consent of the individuals to whom the personal data relates), the information provided to the individuals prior to processing their personal data, the notification obligations to the national data protection authorities, and the security and confidentiality of the personal data. EU Member States may also impose additional requirements in relation to health, genetic and biometric data through their national legislation.
74
In addition, the GDPR imposes specific restrictions on the transfer of personal data to countries outside of the European Economic Area (EEA) that are not considered by the European Commission (EC) to provide an adequate level of data protection. Appropriate safeguards are required to enable such transfers. Among the appropriate safeguards that can be used, the data exporter may use the standard contractual clauses (SCCs). With regard to the transfer of data from the EEA to the United States, on July 10, 2023, the EC adopted its adequacy decision for the EU-US Data Privacy Framework. On the basis of the new adequacy decision, personal data can flow from the EEA to U.S. companies participating in the framework.
Failure to comply with the requirements of the GDPR and the related national data protection laws of the EU Member States may result in significant monetary fines for noncompliance of up to €20 million or 4% of the annual global revenues of the noncompliant company, whichever is greater, other administrative penalties and a number of criminal offenses (punishable by uncapped fines) for organizations and, in certain cases, their directors and officers, as well as civil liability claims from individuals whose personal data was processed.
Data protection authorities from the different EU Member States may still implement certain variations, enforce the GDPR and national data protection laws differently, and introduce additional national regulations and guidelines, which adds to the complexity of processing personal data in the EU. Guidance developed at both the EU level and at the national level in individual EU Member States concerning implementation and compliance practices are often updated or otherwise revised.
Furthermore, there is a growing trend towards the required public disclosure of clinical trial data in the EU, which adds to the complexity of obligations relating to processing health data from clinical trials. Such public disclosure obligations are provided in the new EU Clinical Trials Regulation No. 536/2014 (CTR), EMA disclosure initiatives and voluntary commitments by industry. Failure to comply with these obligations could lead to government enforcement actions and significant penalties against us, harm to our reputation, and adversely impact our business and operating results. The uncertainty regarding the interplay between different regulatory frameworks, such as the CTR and the GDPR, further adds to the complexity that we face with regard to data protection regulation.
With regard to the transfer of personal data from the EEA to the United Kingdom (UK), personal data may now freely flow from the EEA to the UK since the UK is deemed to have an adequate data protection level.
However, the adequacy decisions include a ‘sunset clause’ which entails that the decisions will automatically expire four years after their entry into force. Additionally, following the UK’s withdrawal from the EU and the EEA, companies also have to comply with the UK’s data protection laws (including the UK GDPR (as defined in section 3(10) (as supplemented by section 205(4)) of the Data Protection Act 2018 (the DPA 2018)), the DPA 2018, and related data protection laws in the UK). Separate from the fines that can be imposed by the GDPR, the UK regime has the ability to fine up to the greater of £17.5 million or 4% of global turnover.
Following the UK’s withdrawal from the EU and the EEA, companies are subject to specific transfer rules under the UK regime; personal data may flow freely from the UK to the EEA, since the EEA is deemed to have an adequate data protection level for purposes of the UK regime. These UK international transfer rules broadly mirror the GDPR rules. On February 2, 2022, the UK Secretary of State laid before the UK Parliament the international data transfer agreement (IDTA) and the international data transfer addendum to the EC’s standard contractual clauses for international data transfers (Addendum) and a document setting out transitional provisions. The IDTA and Addendum came into force on March 21, 2022 and replaced the old SCCs for the purposes of the UK regime. However, the transitional provisions, adopted with the IDTA and the Addendum, provide that contracts concluded on or before September 21, 2022 on the basis of any old SCCs continue to provide appropriate safeguards for the purpose of the UK regime until March 21, 2024, provided that the processing operations that are the subject matter of the contract remain unchanged and reliance on those clauses ensures that the transfer of personal data is subject to appropriate safeguards.
With regard to the transfer of personal data from the UK to the United States, the UK government has adopted an adequacy decision for the United States, the UK-US Data Bridge, which came into force on October 12, 2023. The UK-US Data Bridge recognizes the United States as offering an adequate level of data protection where the transfer is to a U.S. company participating in the EU-US Data Privacy Framework and the UK Extension.
75
Drug and Biologic Development Process
Regardless of where they are conducted, all clinical trials included in applications for marketing authorization (MA) for human medicines in the European EU/EEA must have been carried out in accordance with EU regulations. This means that clinical trials conducted in the EU/EEA have to comply with EU clinical trial legislation but also that clinical trials conducted outside the EU/EEA have to comply with ethical principles equivalent to those set out in the EEA, including adhering to international good clinical practice and the Declaration of Helsinki. The conduct of clinical trials in the EU is governed by the CTR, which entered into force on January 31, 2022. The CTR replaced the Clinical Trials Directive 2001/20/EC, (Clinical Trials Directive) and introduced a complete overhaul of the existing regulation of clinical trials for medicinal products in the EU.
Under the former regime, which will expire after a transition period of three years, as outlined below in more detail, before a clinical trial can be initiated it must be approved in each EU member state where there is a site at which the clinical trial is to be conducted. The approval must be obtained from two separate entities: the National Competent Authority (NCA) and one or more Ethics Committees. The NCA of the EU Member States in which the clinical trial will be conducted must authorize the conduct of the trial, and the independent Ethics Committee must grant a positive opinion in relation to the conduct of the clinical trial in the relevant EU member state before the commencement of the trial. Any substantial changes to the trial protocol or other information submitted with the clinical trial applications must be submitted to or approved by the relevant NCA and Ethics Committees. Under the current regime all suspected unexpected serious adverse reactions to the investigated drug that occur during the clinical trial must be reported to the NCA and to the Ethics Committees of the EU member state where they occur.
A more unified procedure will apply under the new CTR. A sponsor will be able to submit a single application for approval of a clinical trial through a centralized EU clinical trials portal. One national regulatory authority (the reporting EU member state proposed by the applicant) will take the lead in validating and evaluating the application consult and coordinate with the other concerned EU Member States. If an application is rejected, it may be amended and resubmitted through the EU clinical trials portal. If an approval is issued, the sponsor may start the clinical trial in all concerned EU Member States. However, a concerned EU member state may in limited circumstances declare an “opt-out” from an approval and prevent the clinical trial from being conducted in such member state. The CTR also aims to streamline and simplify the rules on safety reporting, and introduces enhanced transparency requirements such as mandatory submission of a summary of the clinical trial results to the EU Database. The CTR foresees a three-year transition period. EU Member States will work in CTIS immediately after the system has gone live. Since January 31, 2023, submission of initial clinical trial applications via CTIS is mandatory, and by January 31, 2025, all ongoing trials approved under the former Clinical Trials Directive will need to comply with the CTR and have to be transitioned to CTIS. On July 19, 2023, the EC published guidance concerning the steps to be taken in this transition. This guidance provides, among other things, that (i) documentation which was previously assessed will not be reassessed, (ii) templates that were developed and endorsed by the EU Clinical Trials Expert Group to provide compliance with the CTR do not need to be updated and (iii) there is no need to retrospectively create a site suitability form, which are only necessary for new trial sites.
Under both the former regime and the new CTR, national laws, regulations, and the applicable GCP and Good Laboratory Practice standards must also be respected during the conduct of the trials, including the International Council for Harmonization of Technical Requirements for Pharmaceuticals for Human Use (ICH) guidelines on Good Clinical Practice and the ethical principles that have their origin in the Declaration of Helsinki.
During the development of a medicinal product, the EMA and national regulators within the EU provide the opportunity for dialogue and guidance on the development program. At the EMA level, this is usually done in the form of scientific advice, which is given by the Committee for Medicinal Products for Human Use (CHMP) on the recommendation of the Scientific Advice Working Party (SAWP). A fee is incurred with each scientific advice procedure, but is significantly reduced for designated orphan medicines. Advice from the EMA is typically provided based on questions concerning, for example, quality (chemistry, manufacturing and controls testing), nonclinical testing and clinical studies, and pharmacovigilance plans and risk-management programs. Advice is not legally binding with regard to any future Marketing Authorization Application (MAA) of the product concerned.
76
Drug Marketing Authorization
In the EEA, after completion of all required clinical testing, pharmaceutical products may only be placed on the market after obtaining a MA. To obtain an MA of a drug under European Union regulatory systems, an applicant can submit an MAA through, amongst others, a centralized or decentralized procedure.
To be used or sold in the UK, a drug must have an effective MA obtained by a centralized application through EMA or a national application. National applications are governed by the Human Medicines Regulations (SI 2012/1916). Applications are made electronically through the Medicines and Healthcare products Regulatory Agency (MHRA) Submissions Portal. The process from application to authorizations generally takes up to 210 days, excluding time taken to provide any additional information or data required by the MHRA.
On August 30, 2023, the MHRA published detailed guidance on its recently announced new International Reliance Procedure (IRP) for MAAs. The IRP applies since January 1, 2024 and replaces existing EU reliance procedures to apply for authorizations from seven international regulators (e.g. Health Canada, Swiss Medic, FDA, EMA, among others). The IRP allows medicinal products approved in other jurisdictions that meet certain criteria to undergo a fast-tracked MHRA review to obtain and/or update a MA in the UK or Great Britain. Applicants can submit initial MAAs to the IRP but the procedure can also be used throughout the lifecycle of a product for post-authorization procedures including line extensions, variations and renewals.
Centralized Authorization Procedure
The centralized procedure provides for the grant of a single MA that is issued by the EC following the scientific assessment of the application by the European Medicines Agency (EMA) that is valid for all EU Member States as well as in the three additional EEA Member States. The centralized procedure is compulsory for specific medicinal products, including for medicines developed by means of certain biotechnological processes, products designated as orphan medicinal products, advanced therapy medicinal products (ATMP) and medicinal products with a new active substance indicated for the treatment of certain diseases (AIDS, cancer, neurodegenerative disorders, diabetes, auto-immune and viral diseases). For medicinal products containing a new active substance not yet authorized in the EEA before May 20, 2004 and indicated for the treatment of other diseases, medicinal products that constitute significant therapeutic, scientific or technical innovations or for which the grant of a MA through the centralized procedure would be in the interest of public health at EU level, an applicant may voluntarily submit an application for a MA through the centralized procedure.
Under the centralized procedure, the Committee for Medicinal Products for Human Use (CHMP) established at the EMA, is responsible for conducting the initial assessment of a drug. The CHMP is also responsible for several post-authorization and maintenance activities, such as the assessment of modifications or extensions to an existing MA. Under the centralized procedure, the timeframe for the evaluation of an MAA by the EMA’s CHMP is, in principle, 210 days from receipt of a valid MAA. However, this timeline excludes clock stops, when additional written or oral information is to be provided by the applicant in response to questions asked by the CHMP, so the overall process typically takes a year or more, unless the application is eligible for an accelerated assessment. Accelerated evaluation might be granted by the CHMP in exceptional cases, when a medicinal product is expected to be of a major public health interest, particularly from the point of view of therapeutic innovation. Upon request, the CHMP can reduce the time frame to 150 days if the applicant provides sufficient justification for an accelerated assessment. The CHMP will provide a positive opinion regarding the application only if it meets certain quality, safety and efficacy requirements. This opinion is then transmitted to the EC, which has the ultimate authority for granting MA within 67 days after receipt of the CHMP opinion.
Decentralized Authorization Procedure
Medicines that fall outside the mandatory scope of the centralized procedure have three routes to authorization:
(i) they can be authorized under the centralized procedure if they concern a significant therapeutic, scientific or technical innovation, or if their authorization would be in the interest of public health; (ii) they can be authorized under a decentralized procedure where an applicant applies for simultaneous authorization in more than one EU member state; or (iii) they can be authorized in an EU member state in accordance with that state’s national procedures and then be authorized in other EU countries by a procedure whereby the countries concerned agree to recognize the validity of the original, national MA (mutual recognition procedure).
77
The decentralized procedure permits companies to file identical MA applications for a medicinal product to the competent authorities in various EU Member States simultaneously if such medicinal product has not received marketing approval in any EU Member State before. This procedure is available for pharmaceutical products not falling within the mandatory scope of the centralized procedure. The competent authority of a single EU Member State, the reference member state, is appointed to review the application and provide an assessment report. The competent authorities of the other EU Member States, the concerned member states, are subsequently required to grant a MA for their territories on the basis of this assessment. The only exception to this is where the competent authority of an EU Member State considers that there are concerns of potential serious risk to public health, the disputed points are subject to a dispute resolution mechanism and may eventually be referred to the EC, whose decision is binding for all EU Member States.
Risk Management Plan
All new MAAs must include a Risk Management Plan (RMP) describing the risk management system that the company will put in place and documenting measures to prevent or minimize the risks associated with the product. RMPs are continually modified and updated throughout the lifetime of the medicine as new information becomes available. An updated RMP must be submitted: (i) at the request of EMA or a national competent authority, or (ii) whenever the risk-management system is modified, especially as the result of new information being received that may lead to a significant change to the benefit-risk profile or as a result of an important pharmacovigilance or risk-minimization milestone being reached. The regulatory authorities may also impose specific obligations as a condition of the MA. Since October 20, 2023, all RMPs for centrally authorized products are published by the EMA, subject only to limited redactions.
MA Validity Period
MAs have an initial duration of five years. After these five years, the authorization may subsequently be renewed on the basis of a reevaluation of the risk-benefit balance. Once renewed, the MA is valid for an unlimited period unless the EC or the national competent authority decides, on justified grounds relating to pharmacovigilance, to proceed with only one additional five-year renewal. Applications for renewal must be made to the EMA at least nine months before the five-year period expires.
Additionally, the holder of a MA for an ATMP must put in place and maintain a system to ensure that each individual product and its starting and raw materials, including all substances coming into contact with the cells or tissues it may contain, can be traced through the sourcing, manufacturing, packaging, storage, transport and delivery to the relevant healthcare institution where the product is used.
Any authorization which is not followed by the actual placing of the drug on the EU market (in case of centralized procedure) or on the market of the authorizing member state within three years after authorization ceases to be valid.
For the UK, the period of three years during which the drug has not been marketed in Great Britain will be restarted from the date of conversion to a Great Britain MA. Conversion refers to the procedure by which, as of January 1, 2021, MAs granted on the basis of a centralized procedure in the EU are only valid in Norther Ireland but not in Great Britain, whereas, prior EU authorizations have all been automatically converted into UK MAs effective in Great Britain only.
On the other hand, for the EU, in the case the drug has been marketed in the UK, the placing on the UK market before the end of the period starting when the UK left the EU on January 31, 2020 and ending on December 31, 2020 (the Brexit Transition Period) will be taken into account. If, after the end of the Brexit Transition Period, the drug is not placed on any other market of the remaining member states of the EU, the three year period will start running from the last date the drug was placed on the UK market before the end of the Brexit Transition Period.
78
Advanced Therapy Medicinal Products
In the EU, medicinal products, including ATMPs are subject to extensive pre-and post-market regulation by regulatory authorities at both the EU and national levels. ATMPs comprise gene therapy products, somatic cell therapy products and tissue engineered products, which are genes, cells or tissues that have undergone substantial manipulation and that are administered to human beings in order to cure, diagnose or prevent diseases or regenerate, repair or replace a human tissue. Pursuant to the ATMP Regulation, the Committee on Advanced Therapies (CAT) is responsible in conjunction with the CHMP for the evaluation of ATMPs. The CHMP and CAT are also responsible for providing guidelines on ATMPs. These guidelines provide additional guidance on the factors that the EMA will consider in relation to the development and evaluation of ATMPs and include, among other things, the preclinical studies required to characterize ATMPs. Although such guidelines are not legally binding, compliance with them is often necessary to gain and maintain approval for product candidates.
In addition to the mandatory RMP, the holder of a MA for an ATMP must put in place and maintain a system to ensure that each individual product and its starting and raw materials, including all substances coming into contact with the cells or tissues it may contain, can be traced through the sourcing, manufacturing, packaging, storage, transport and delivery to the relevant healthcare institution where the product is used.
Exceptional Circumstances/Conditional Approval
Similar to accelerated approval regulations in the United States, conditional MAs can be granted in the EU in exceptional circumstances. A conditional MA can be granted for medicinal products where, although comprehensive clinical data referring to the safety and efficacy of the medicinal product have not been supplied, a number of criteria are fulfilled: (i) the benefit/risk balance of the product is positive, (ii) it is likely that the applicant will be in a position to provide the comprehensive clinical data, (iii) unmet medical needs will be fulfilled by the grant of the MA and (iv) the benefit to public health of the immediate availability on the market of the medicinal product concerned outweighs the risk inherent in the fact that additional data are still required. A conditional MA must be renewed annually.
Data and Market Exclusivity
As in the United States, it may be possible to obtain a period of market and / or data exclusivity in the EU that would have the effect of postponing the entry into the marketplace of a competitor’s generic, hybrid or biosimilar product (even if the pharmaceutical product has already received a MA) and prohibiting another applicant from relying on the MA holder’s pharmacological, toxicological and clinical data in support of another MA for the purposes of submitting an application, obtaining MA or placing the product on the market. New Chemical Entities (NCE) approved in the EU qualify for eight years of data exclusivity and 10 years of marketing exclusivity.
An additional non-cumulative one-year period of marketing exclusivity is possible if during the data exclusivity period (the first eight years of the 10-year marketing exclusivity period), the MA holder obtains an authorization for one or more new therapeutic indications that are deemed to bring a significant clinical benefit compared to existing therapies.
The data exclusivity period begins on the date of the product’s first MA in the EU. After eight years, a generic product application may be submitted and generic companies may rely on the MA holder’s data. However, a generic product cannot launch until two years later (or a total of 10 years after the first MA in the EU of the innovator product), or three years later (or a total of 11 years after the first MA in the EU of the innovator product) if the MA holder obtains MA for a new indication with significant clinical benefit within the eight-year data exclusivity period. Additionally, another noncumulative one-year period of data exclusivity can be added to the eight years of data exclusivity where an application is made for a new indication for a well-established substance, provided that significant pre-clinical or clinical studies were carried out in relation to the new indication. Another year of data exclusivity may be added to the eight years, where a change of classification of a pharmaceutical product has been authorized on the basis of significant pre-trial tests or clinical trials (when examining an application by another applicant for or holder of market authorization for a change of classification of the same substance the competent authority will not refer to the results of those tests or trials for one year after the initial change was authorized).
79
Products may not be granted data exclusivity since there is no guarantee that a product will be considered by the European Union’s regulatory authorities to include a NCE. Even if a compound is considered to be a NCE and the MA applicant is able to gain the prescribed period of data exclusivity, another company nevertheless could also market another version of the medicinal product if such company can complete a full MAA with their own complete database of pharmaceutical tests, preclinical studies and clinical trials and obtain MA of its product.
On April 26, 2023, the EC submitted a proposal for the reform of the European pharmaceutical legislation. The current draft envisages e.g., a shortening of the periods of data exclusivity, however, there is currently neither a final version of this draft nor a date for its entry into force.
Orphan Designation and Exclusivity
The criteria for designating an orphan medicinal product in the European Union are similar in principle to those in the United States. The EMA grants orphan drug designation if the medicinal product is intended for the diagnosis, prevention or treatment of a life-threatening or chronically debilitating condition affecting no more than five in 10,000 persons in the European Union (prevalence criterion). In addition, Orphan Drug Designation can be granted if, for economic reasons, the medicinal product would be unlikely to be developed without incentives and if there is no other satisfactory method approved in the European Union of diagnosing, preventing, or treating the condition, or if such a method exists, the proposed medicinal product is a significant benefit to patients affected by the condition. An application for orphan drug designation (which is not a MA, as not all orphan-designated medicines reach the authorization application stage) must be submitted first before an application for MA of the medicinal product is submitted. The applicant will receive a fee reduction for the MAA if the orphan drug designation has been granted, but not if the designation is still pending at the time the MA is submitted, and sponsors must submit an annual report to EMA summarizing the status of development of the medicine. Orphan drug designation does not convey any advantage in, or shorten the duration of, the regulatory review and approval process. Designated orphan medicines are eligible for conditional MA.
The EMA’s Committee for Orphan Medicinal Products (COMP) reassesses the orphan drug designation of a product in parallel with the review for a MA; for a product to benefit from market exclusivity it must maintain its orphan drug designation at the time of MA review by the EMA and approval by the EC. Additionally, any MA granted for an orphan medicinal product must only cover the therapeutic indication(s) that are covered by the orphan drug designation. Upon the grant of a MA, orphan drug designation provides up to ten years of market exclusivity in the orphan indication.
During the 10-year period of market exclusivity, with a limited number of exceptions, the regulatory authorities of the EU Member States and the EMA may not accept applications for MA, accept an application to extend an existing MA or grant a MA for other similar medicinal products for the same therapeutic indication. A similar medicinal product is defined as a medicinal product containing a similar active substance or substances as contained in a currently authorized orphan medicinal product, and which is intended for the same therapeutic indication. An orphan medicinal product can also obtain an additional two years of market exclusivity for an orphan-designated condition when the results of specific studies are reflected in the Summary of Product Characteristics (SmPC) addressing the pediatric population and completed in accordance with a fully compliant Pediatric Investigation Plan (PIP). No extension to any supplementary protection certificate can be granted on the basis of pediatric studies for orphan indications.
The 10-year market exclusivity may be reduced to six years if, at the end of the fifth year, it is established that the product no longer meets the criteria for orphan designation, i.e. the condition prevalence or financial returns criteria under Article 3 of Regulation (EC) No. 141/2000 on orphan medicinal products. When the period of orphan market exclusivity for an indication ends, the orphan drug designation for that indication expires as well. Orphan exclusivity runs in parallel with normal rules on data exclusivity and market protection. Additionally, a MA may be granted to a similar medicinal product (orphan or not) for the same or overlapping indication subject to certain requirements.
In the UK, following the post-Brexit transition period, a system for incentivizing the development of orphan medicines was introduced. Overall, the requirements for orphan designation largely replicate the requirements in the EU and the benefit of market exclusivity has been retained. Products with an orphan designation in the EU can be considered for an orphan MA in Great Britain, but a UK-wide orphan MA can only be considered in the absence of an active EU orphan designation. The MHRA will review applications for orphan designation at the time of a MA, and will offer incentives, such as market exclusivity and full or partial refunds for MA fees to encourage the development of medicines in rare diseases.
80
Pediatric Development
In the EU, companies developing a new medicinal product are obligated to study their product in children and must therefore submit a PIP together with a request for agreement to the EMA. The EMA issues a decision on the PIP based on an opinion of the EMA’s Pediatric Committee (PDCO). Companies must conduct pediatric clinical trials in accordance with the PIP approved by the EMA, unless a deferral (e.g. until enough information to demonstrate its effectiveness and safety in adults is available) or waiver (e.g. because the relevant disease or condition occurs only in adults) has been granted by the EMA. The MAA for the medicinal product must include the results of all pediatric clinical trials performed and details of all information collected in compliance with the approved PIP, unless a waiver or a deferral has been granted, in which case the pediatric clinical trials may be completed at a later date. Medicinal products that are granted a MA on the basis of the pediatric clinical trials conducted in accordance with the approved PIP are eligible for a six month extension of the protection under a supplementary protection certificate (if any is in effect at the time of approval) or, in the case of orphan medicinal products, a two year extension of the orphan market exclusivity. This pediatric reward is subject to specific conditions and is not automatically available when data in compliance with the approved PIP are developed and submitted. An approved PIP is also required when a MA holder wants to add a new indication, medicinal form or route of administration for a medicine that is already authorized and covered by intellectual property rights.
In the UK, the MHRA has published guidance on the procedures for UK Paediatric Investigation Plans (PIPs) which, where possible, mirror the submission format and requirements of the EU system. EU PIPs remain applicable for Northern Ireland and EU PIPs agreed by the EMA prior to January 1, 2021 have been adopted as UK PIPs.
PRIME Designation
In March 2016, the EMA launched an initiative to facilitate development of product candidates in indications, often rare, for which few or no therapies currently exist. The Priority Medicines (PRIME) scheme is intended to encourage drug development in areas of unmet medical need and provides accelerated assessment of products representing substantial innovation reviewed under the centralized procedure. Products from small-and medium-sized enterprises may qualify for earlier entry into the PRIME scheme than larger companies on the basis of compelling non-clinical data and tolerability data from initial clinical trials. Many benefits accrue to sponsors of product candidates with PRIME designation, including but not limited to, early and proactive regulatory dialogue with the EMA, frequent discussions on clinical trial designs and other development program elements, and potentially accelerated MAA assessment once a dossier has been submitted. Importantly, once a candidate medicine has been selected for the PRIME scheme, a dedicated contact point and rapporteur from the CHMP or from CAT are appointed facilitating increased understanding of the product at EMA’s Committee level. A kick-off meeting with the CHMP/CAT rapporteur initiates these relationships and includes a team of multidisciplinary experts to provide guidance on the overall development plan and regulatory strategy. PRIME eligibility does not change the standards for product approval, and there is no assurance that any such designation or eligibility will result in expedited review or approval.
Post-Approval Regulation
Similar to the United States, both MA holders and manufacturers of medicinal products are subject to comprehensive regulatory oversight by the EMA, the EC and/or the competent regulatory authorities of the EU Member States. This oversight applies both before and after grant of manufacturing licenses and MAs. It includes control of compliance with EU good manufacturing practices rules, manufacturing authorizations, pharmacovigilance rules and requirements governing advertising, promotion, sale, and distribution, recordkeeping, importing and exporting of medicinal products.
Failure by us or by any of our third-party partners, including suppliers, manufacturers and distributors to comply with EU laws and the related national laws of individual EU Member States governing the conduct of clinical trials, manufacturing approval, MA of medicinal products and marketing of such products, both before and after grant of MA, statutory health insurance, bribery and anti-corruption or other applicable regulatory requirements may result in administrative, civil or criminal penalties.
81
These penalties could include delays or refusal to authorize the conduct of clinical trials or to grant MA, product withdrawals and recalls, product seizures, suspension, withdrawal or variation of the MA, total or partial suspension of production, distribution, manufacturing or clinical trials, operating restrictions, injunctions, suspension of licenses, fines and criminal penalties.
The holder of a MA for a medicinal product must also comply with EU pharmacovigilance legislation and its related regulations and guidelines, which entail many requirements for conducting pharmacovigilance, or the assessment and monitoring of the safety of medicinal products.
These pharmacovigilance rules can impose on holders of MAs the obligation to conduct a labor intensive collection of data regarding the risks and benefits of marketed medicinal products and to engage in ongoing assessments of those risks and benefits, including the possible requirement to conduct additional clinical studies or post-authorization safety studies to obtain further information on a medicine’s safety, or to measure the effectiveness of risk-management measures, which may be time consuming and expensive and could impact our profitability. MA holders must establish and maintain a pharmacovigilance system and appoint an individual qualified person for pharmacovigilance, who is responsible for oversight of that system. Key obligations include expedited reporting of suspected serious adverse reactions and submission of PSURs in relation to medicinal products for which they hold MAs. The EMA reviews PSURs for medicinal products authorized through the centralized procedure. If the EMA has concerns that the risk benefit profile of a product has varied, it can adopt an opinion advising that the existing MA for the product be suspended, withdrawn or varied. The agency can advise that the MA holder be obliged to conduct post-authorization Phase IV safety studies. If the EC agrees with the opinion, it can adopt a decision varying the existing MA. Failure by the MA holder to fulfill the obligations for which the EC’s decision provides can undermine the ongoing validity of the MA.
More generally, non-compliance with pharmacovigilance obligations can lead to the variation, suspension or withdrawal of the MA for the product or imposition of financial penalties or other enforcement measures.
The manufacturing process for pharmaceutical products in the European Union is highly regulated and regulators may shut down manufacturing facilities that they believe do not comply with regulations.
Manufacturing requires a manufacturing authorization, and the manufacturing authorization holder must comply with various requirements set out in the applicable EU laws, regulations and guidance, including Directive 2001/83/EC, Directive 2003/94/EC, Regulation (EC) No 726/2004 and the European Commission Guidelines for Good Manufacturing Practice (GMP). These requirements include compliance with EU GMP standards when manufacturing pharmaceutical products and active pharmaceutical ingredients, including the manufacture of active pharmaceutical ingredients outside of the European Union with the intention to import the active pharmaceutical ingredients into the European Union. Similarly, the distribution of pharmaceutical products into and within the European Union is subject to compliance with the applicable EU laws, regulations and guidelines, including the requirement to hold appropriate authorizations for distribution granted by the competent authorities of the EU Member States. The manufacturer or importer must have a qualified person who is responsible for certifying that each batch of product has been manufactured in accordance with GMP, before releasing the product for commercial distribution in the European Union or for use in a clinical trial. Manufacturing facilities are subject to periodic inspections by the competent authorities for compliance with GMP.
Sales and Marketing Regulations
The advertising and promotion of our products is also subject to EU laws concerning promotion of medicinal products, interactions with physicians, misleading and comparative advertising and unfair commercial practices. In addition, other national legislation of individual EU Member States may apply to the advertising and promotion of medicinal products and may differ from one country to another. These laws require that promotional materials and advertising in relation to medicinal products comply with the product’s SmPC as approved by the competent regulatory authorities. The SmPC is the document that provides information to physicians concerning the safe and effective use of the medicinal product. It forms an intrinsic and integral part of the MA granted for the medicinal product. Promotion of a medicinal product that does not comply with the SmPC is considered to constitute off-label promotion. All advertising and promotional activities for the product must be consistent with the approved SmPC and therefore all off-label promotion is prohibited. Direct-to-consumer advertising of prescription-only medicines is also prohibited in the EU. Violations of the rules governing the promotion of medicinal products in the European Union could be penalized by administrative measures, fines and imprisonment.
82
These laws may further limit or restrict the advertising and promotion of our products to the general public and may also impose limitations on its promotional activities with healthcare professionals. EU regulation with regards to dispensing, sale and purchase of medicines has generally been preserved in the UK following Brexit, through the HMRs. However, organizations wishing to sell medicines online need to register with the MHRA. Following Brexit, the requirements to display the common logo no longer apply to UK-based online sellers, except for those established in Northern Ireland.
Anti-Corruption Legislation
In the EU, interactions between pharmaceutical companies and physicians are also governed by strict laws, regulations, industry self-regulation codes of conduct and physicians’ codes of professional conduct both at EU level and in the individual EU Member States. The provision of benefits or advantages to physicians to induce or encourage the prescription, recommendation, endorsement, purchase, supply, order or use of medicinal products is prohibited in the European Union. The provision of benefits or advantages to physicians is also governed by the national anti-bribery laws of the EU Member States. Violation of these laws could result in substantial fines and imprisonment.
Payments made to physicians in certain EU Member States also must be publicly disclosed. Moreover, agreements with physicians must often be the subject of prior notification and approval by the physician’s employer, his/her regulatory professional organization, and/or the competent authorities of the individual EU Member States. These requirements are provided in the national laws, industry codes, or professional codes of conduct, applicable in the individual EU Member States. Failure to comply with these requirements could result in reputational risk, public reprimands, administrative penalties, fines or imprisonment.
In the UK, the pharmaceutical sector is recognized as being particularly vulnerable to corrupt practices, some of which fall within the scope of the Bribery Act 2010. Due to the Bribery Act 2010’s far-reaching territorial application, the potential penalized act does not have to occur in the UK to become within its scope. If the act or omission does not take place in the UK, but the person’s act or omission would constitute an offense if carried out there and the person has a close connection with the UK, an offense will still have been committed.
The Bribery Act 2010 is comprised of four offenses that cover (i) individuals, companies and partnerships that give, promise or offer bribes, (ii) individuals, companies and partnerships that request, agree to receive or accept bribes, (iii) individuals, companies and partnerships that bribe foreign public officials and (iv) companies and partnerships that fail to prevent persons acting on their behalf from paying bribes. The penalties imposed under the Bribery Act 2010 depend on the offence committed, harm and culpability and penalties range from unlimited fines to imprisonment for a maximum term of ten years and in some cases both.
Regulations in the UK and Other Markets
The UK formally left the EU on January 31, 2020 and EU laws now only apply to the UK in respect of Northern Ireland as laid out in the Protocol on Ireland and Northern Ireland and as amended by the Windsor Framework sets out a long-term set of arrangements for the supply of medicines into Northern Ireland. The EU and the UK agreed on a trade and cooperation agreement, which includes provisions affecting the life sciences sector (including on customs and tariffs). There are some specific provisions concerning pharmaceuticals, including the mutual recognition of GMP, inspections of manufacturing facilities for medicinal products and GMP issued documents. The TCA does not, however, contain wholesale mutual recognition of UK and EU pharmaceutical regulations and product standards.
The UK government has adopted the Medicines and Medical Devices Act 2021 to enable the UK’s regulatory frameworks to be updated following the UK’s departure from the EU. The MMDA introduces regulation-making, delegated powers covering the fields of human medicines, clinical trials of human medicines, veterinary medicines and medical devices. The MHRA has since been consulting on future regulations for medicines and medical devices in the UK.
83
For other countries outside of the European Union, such as countries in Eastern Europe, Latin America or Asia, the requirements governing the conduct of clinical trials, product licensing, pricing and reimbursement vary from country to country. In all cases, again, the clinical trials must be conducted in accordance with GCP and the applicable regulatory requirements and the ethical principles that have their origin in the Declaration of Helsinki.
If we fail to comply with applicable foreign regulatory requirements, we may be subject to, among other things, fines, suspension of clinical trials, suspension or withdrawal of regulatory approvals, product recalls, seizure of products, operating restrictions and criminal prosecution.
Item 1A. Risk Factors
Investing in our common stock involves a high degree of risk. Before you decide to invest in our common stock, you should consider carefully the risks described below, together with the other information contained in this Annual Report, including “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and our audited consolidated financial statements and related notes. We believe the risks described below are the risks that are material to us as of the date of this Annual Report. If any of the following risks actually occur, our business, financial condition, results of operations and future growth prospects could be materially and adversely affected. In these circumstances, the market price of our common stock could decline, and you may lose all or part of your investment.
Risk Factor Summary
Below is a summary of the material risks to our business, our operations and an investment in our common stock. This summary does not address all of the risks that we face. Risks and uncertainties not presently known to us or that we presently deem less significant may also impair our business operations. Additional discussion of the risks summarized in this risk factor summary, and other risks that we face, can be found below and should be carefully considered, together with other information in this Annual Report in its entirety before making investment decisions regarding our common stock.
| ● | We are a clinical stage biotechnology company with a limited operating history, we have not completed any clinical trials, and we have no products approved for commercial sale, which may make it difficult for you to evaluate our current business and likelihood of success and viability. |
| ● | We will require substantial additional capital to finance our operations in the future. If we are unable to raise such capital when needed, or on acceptable terms, we may be forced to delay, reduce and/or eliminate one or more of our development programs or future commercialization efforts. |
| ● | We have incurred significant losses since inception, and we expect to incur significant losses for the foreseeable future and may not be able to achieve or sustain profitability in the future. We have no products approved for sale, have not generated any revenue from our programs and may never generate revenue or become profitable. |
| ● | We face competition from entities that have developed or may develop programs for the diseases addressed by our programs. |
| ● | Our programs are in clinical and preclinical stages of development and may fail in development or suffer delays that materially and adversely affect their commercial viability. |
| ● | We are substantially dependent on the success of our two most advanced programs, APG777 and APG808, and our anticipated clinical trials of such programs may not be successful. |
| ● | Our approach to the discovery and development of our programs is unproven, and we may not be successful in our efforts to build a pipeline of programs with commercial value. |
84
| ● | Preclinical and clinical development involves a lengthy and expensive process that is subject to delays and with uncertain outcomes, and results of earlier studies and trials may not be predictive of future clinical trial results. |
| ● | If we encounter difficulties enrolling patients in our future clinical trials, our clinical development activities could be delayed or otherwise adversely affected. |
| ● | We rely on collaborations and licensing arrangements with third parties. If we are unable to maintain these collaborations or licensing arrangements, or if these collaborations or licensing arrangements are not successful, our business could be negatively impacted. |
| ● | We currently rely, and plan to rely in the future, on third parties to conduct and support our preclinical studies and clinical trials. If these third parties do not properly and successfully carry out their contractual duties or meet expected deadlines, we may not be able to obtain regulatory approval of or commercialize our programs. |
| ● | We currently rely, and expect to rely in the future, on the use of manufacturing suites in third-party facilities or on third parties to manufacture our products, and we may rely on third parties to produce and process our products, if approved. Our business could be adversely affected if we are unable to use third-party manufacturing suites or if the third-party manufacturers encounter difficulties in production. |
| ● | Our ability to protect our patents and other proprietary rights is uncertain, exposing us to the possible loss of competitive advantage. |
| ● | We may be subject to patent infringement claims or may need to file claims to protect our intellectual property, which could result in substantial costs and liability and prevent us from commercializing our potential products. |
| ● | The regulatory approval processes of the FDA and other comparable foreign regulatory authorities are lengthy, time-consuming and inherently unpredictable. |
Risks Related to Our Limited Operating History, Financial Position and Capital Requirements
We are a clinical stage biotechnology company with a limited operating history, we have not completed any clinical trials, and we have no products approved for commercial sale, which may make it difficult for you to evaluate our current business and likelihood of success and viability.
We are a clinical stage biotechnology company with limited operating history. Since our inception in 2022, we have incurred significant operating losses and have utilized substantially all of our resources to date in-licensing and developing our programs, organizing and staffing our company and providing other general and administrative support for our operations. We have no significant experience as a company in initiating, conducting or completing clinical trials. In part because of this lack of experience, we cannot be certain that our planned clinical trials will begin or be completed on time, if at all, or that our ongoing clinical trial will be completed on time, if at all. In addition, we have not yet demonstrated an ability to obtain marketing approvals, manufacture a commercial-scale product or arrange for a third party to do so on our behalf, or conduct sales, marketing and distribution activities necessary for successful product commercialization. Consequently, any predictions you make about our future success or viability may not be as accurate as they could be if we had a longer operating history.
In addition, as our business grows, we may encounter unforeseen expenses, restrictions, difficulties, complications, delays and other known and unknown factors. We will need to transition at some point from a company with an early research and development focus to a company capable of supporting larger scale clinical trials and eventually commercial activities. We may not be successful in such a transition.
85
We will require substantial additional capital to finance our operations in the future. If we are unable to raise such capital when needed, or on acceptable terms, we may be forced to delay, reduce and/or eliminate one or more of our development programs or future commercialization efforts.
Developing biotechnology products is a very long, time-consuming, expensive and uncertain process that takes years to complete. We expect our expenses to increase in connection with our ongoing activities, particularly as we conduct clinical trials of, and seek marketing approval for our most advanced programs, APG777 and APG808, and advance our other programs and any future programs and product candidates. Even if one or more of the programs that we develop is approved for commercial sale, we anticipate incurring significant costs associated with sales, marketing, manufacturing and distribution activities to launch any such product. Our expenses could increase beyond expectations if we are required by the U.S. Food and Drug Administration (FDA) or other regulatory agencies to perform preclinical studies or clinical trials in addition to those that we are currently conducting or anticipate.
Because the design of our planned and anticipated clinical trials, as well as the outcome of our ongoing, planned and anticipated clinical trials are highly uncertain, we cannot reasonably estimate the actual amount of funding that will be necessary to successfully complete the development and commercialization of any program we develop. Our future capital requirements depend on many factors, including but not limited to:
| ● | the scope, progress, results and costs of discovery, preclinical and clinical development for our programs; |
| ● | the cost and timing of completion of commercial-scale manufacturing activities; |
| ● | the costs and timing of preparing, filing and prosecuting patent applications, maintaining and enforcing our intellectual property and proprietary rights, and defending intellectual property-related claims, including claims of infringement, misappropriation or other violation of third-party intellectual property; |
| ● | the costs, timing and outcome of regulatory review of our programs; |
| ● | the costs of future commercialization activities, either by ourselves or in collaboration with others, including product sales, marketing, manufacturing, and distribution for any program for which we receive marketing approval; |
| ● | the revenue, if any, received from commercial sales of programs for which we receive marketing approval; |
| ● | the success of our current or future collaborations; |
| ● | our ability to establish and maintain additional collaborations on favorable terms, if at all; |
| ● | the extent to which we acquire or in-license products, intellectual property and technologies; |
| ● | the costs of operational, financial and management information systems and associated personnel; and |
| ● | the costs of operating as a public company. |
Accordingly, we will require substantial additional funding to continue our operations. Based on our current operating plan, we estimate that our existing cash, cash equivalents, and marketable securities will be sufficient to enable us to fund our operating expenses and capital expenditure requirements into the fourth quarter of 2026. We have based this estimate on assumptions that may prove to be incorrect, and we could use our available capital resources sooner than we currently anticipate.
86
We do not have any committed external sources of funds and adequate additional financing may not be available to us on acceptable terms, or at all. We may be required to seek additional funds sooner than planned through public or private equity offerings, debt financings, collaborations and licensing arrangements or other sources. Such financing may dilute our stockholders or the failure to obtain such financing may restrict our operating activities. Any additional fundraising efforts may divert our management from their day-to-day activities, which may adversely affect our business. To the extent that we raise additional capital through the sale of equity or convertible debt securities, your ownership interest will be diluted, and the terms may include liquidation or other preferences and anti-dilution protections that adversely affect your rights as a stockholder. Debt financing may result in imposition of debt covenants, increased fixed payment obligations or other restrictions that may affect our business. If we raise additional funds through upfront payments or milestone payments pursuant to future collaborations with third parties, we may have to relinquish valuable rights to our programs, or grant licenses on terms that are not favorable to us. Our ability to raise additional capital may be adversely impacted by global macroeconomic conditions and volatility in the credit and financial markets in the United States and worldwide. Our failure to raise capital as and when needed or on acceptable terms would have a negative impact on our financial condition and our ability to pursue our business strategy, and we may have to delay, reduce the scope of, suspend or eliminate one or more of our programs, clinical trials or future commercialization efforts.
We have incurred significant losses since inception, and we expect to incur significant losses for the foreseeable future and may not be able to achieve or sustain profitability in the future. We have no products approved for sale, have not generated any revenue from our programs and may never generate revenue or become profitable.
Investment in biotechnology product development is a highly speculative undertaking and entails substantial upfront capital expenditures and significant risks that any program will fail to demonstrate adequate efficacy or an acceptable safety profile, gain regulatory approval and become commercially viable. We have no products approved for commercial sale, we have not generated any revenue from product sales to date, and we continue to incur significant research and development and other expenses related to our ongoing operations. We do not expect to generate product revenue unless or until we successfully complete preclinical and clinical development and obtain regulatory approval of, and then successfully commercialize, at least one of our programs. We may never succeed in these activities and, even if we do, may never generate revenues that are significant or large enough to achieve profitability. If we are unable to generate sufficient revenue through the sale of any approved products, we may be unable to continue operations without additional funding.
We have incurred significant net losses in each period since we commenced operations in February 2022. We generated net losses of $39.8 million and $84.0 million for the period from February 4, 2022 (inception) to December 31, 2022 and the year ended December 31, 2023, respectively. As of December 31, 2023, we had an accumulated deficit of $123.8 million. We expect to continue to incur significant losses for the foreseeable future. Our operating expenses and net losses may fluctuate significantly from quarter to quarter and year to year. We anticipate that our expenses will increase substantially if and as we:
| ● | advance our existing and future programs through preclinical and clinical development, including expansion into additional indications; |
| ● | seek to identify additional programs and additional product candidates; |
| ● | maintain, expand, enforce, defend and protect our intellectual property portfolio; |
| ● | seek regulatory and marketing approvals for our programs; |
| ● | seek to identify, establish and maintain additional collaborations and license agreements; |
| ● | make milestone payments to Paragon under the Option Agreements and licensing and royalty payments to WuXi Biologics under the Cell Line License Agreement and under any additional future collaboration or license agreements that we enter into; |
87
| ● | ultimately establish a sales, marketing and distribution infrastructure to commercialize any drug products for which we may obtain marketing approval, either by ourselves or in collaboration with others; |
| ● | generate revenue from commercial sales of programs for which we receive marketing approval; |
| ● | hire additional personnel including research and development, clinical and commercial personnel; |
| ● | add operational, financial and management information systems and personnel, including personnel to support our product development; |
| ● | acquire or in-license products, intellectual property and technologies; |
| ● | develop and manufacture our clinical supplies and access commercial-scale current good manufacturing practices (“cGMP”) capacity and capabilities through third parties or our own manufacturing facility; and |
| ● | continue to operate as a public company. |
In addition, our expenses will increase if, among other things, we are required by the FDA or other regulatory authorities to perform trials or studies in addition to, or different than, those that we currently anticipate, there are any delays in completing our clinical trials or the development of any of our programs, or there are any third-party challenges to our intellectual property or we need to defend against any intellectual property-related claim.
Even if we obtain marketing approval for, and are successful in commercializing, one or more of our programs, we expect to incur substantial additional research and development and other expenditures to develop and market additional programs and/or to expand the approved indications of any marketed product. We may encounter unforeseen expenses, difficulties, complications, delays and other unknown factors that may adversely affect our business. The size of our future net losses will depend, in part, on the rate of future growth of our expenses and our ability to generate revenue.
Our failure to become profitable would decrease the value of our company and could impair our ability to raise capital, maintain our research and development efforts, expand our business and/or continue our operations. A decline in the value of our company could also cause you to lose all or part of your investment.
Risks Related to Discovery, Development and Commercialization
We face competition from entities that have developed or may develop programs for the diseases addressed by our programs.
The development and commercialization of drugs is highly competitive. Our programs, if approved, will face significant competition and our failure to effectively compete may prevent us from achieving significant market penetration. We compete with a variety of multinational biopharmaceutical companies, specialized biotechnology companies and emerging biotechnology companies, as well as academic institutions, governmental agencies, and public and private research institutions, among others. Many of the companies with which we are currently competing or will complete against in the future have significantly greater financial resources and expertise in research and development, manufacturing, preclinical testing, conducting clinical trials, obtaining regulatory approvals, and marketing approved products than we do. Mergers and acquisitions in the pharmaceutical and biotechnology industry may result in even more resources being concentrated among a smaller number of our competitors. Smaller or early-stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies. These competitors also compete with us in recruiting and retaining qualified scientific and management personnel, establishing clinical trial sites, patient registration for clinical trials, as well as in acquiring technologies complementary to, or necessary for, our programs.
88
Our competitors have developed, are developing or will develop programs and processes competitive with our programs and processes. Competitive therapeutic treatments include those that have already been approved and accepted by the medical community and any new treatments. Our success will depend partially on our ability to develop and commercialize products that have a competitive safety, efficacy, dosing and/or presentation profile. Our commercial opportunity and success will be reduced or eliminated if competing products are safer, more effective, have a more attractive dosing profile or presentation or are less expensive than the products we develop, or if our competitors develop competing products or if biosimilars enter the market more quickly than we do and are able to gain market acceptance. See the section titled “Business—Competition” for a more detailed description of our competitors and the factors that may affect the success of our programs.
In addition, because of the competitive landscape for I&I indications, we may also face competition for clinical trial enrollment. Patient enrollment will depend on many factors, including if potential clinical trial patients choose to undergo treatment with approved products or enroll in competitors’ ongoing clinical trials for programs that are under development for the same indications as our programs. An increase in the number of approved products for the indications we are targeting with our programs may further exacerbate this competition. Our inability to enroll a sufficient number of patients could, among other things, delay our development timeline, which may further harm our competitive position.
Our programs are in clinical and preclinical stages of development and may fail in development or suffer delays that materially and adversely affect their commercial viability. If we or our current or future collaborators are unable to complete development of, or commercialize our programs, or experience significant delays in doing so, our business will be materially harmed.
We have no products on the market and we have not completed any clinical trials. As a result, we expect it will be many years before we commercialize any program, if ever. Our ability to achieve and sustain profitability depends on obtaining regulatory approvals for, and successfully commercializing, our programs, either alone or with third parties, and we cannot guarantee you that we will ever obtain regulatory approval for any of our programs. We have not yet demonstrated our ability to complete any clinical trials, obtain regulatory approvals, manufacture a commercial scale product or arrange for a third party to do so on our behalf, or conduct sales and marketing activities necessary for successful product commercialization. Before obtaining regulatory approval for the commercial distribution of our programs, we or an existing or future collaborator must conduct extensive preclinical tests and clinical trials to demonstrate the safety and efficacy in humans of our programs and future product candidates.
We or our collaborators may experience delays in initiating or completing clinical trials. We or our collaborators also may experience numerous unforeseen events during, or as a result of, any current or future clinical trials that we could conduct that could delay or prevent our ability to receive marketing approval or commercialize our programs or any future programs, including:
| ● | regulators or institutional review boards (“IRBs”), the FDA or ethics committees may not authorize us or our investigators to commence a clinical trial or conduct a clinical trial at a prospective trial site; |
| ● | we may experience delays in reaching, or fail to reach, agreement on acceptable terms with prospective trial sites and prospective CROs, the terms of which can be subject to extensive negotiation and may vary significantly among different CROs and trial sites; |
| ● | clinical trial sites deviating from trial protocol or dropping out of a trial; |
| ● | clinical trials of any programs may fail to show safety or efficacy, produce negative or inconclusive results and we may decide, or regulators may require us, to conduct additional preclinical studies or clinical trials or we may decide to abandon product development programs; |
| ● | the number of subjects required for clinical trials of any programs may be larger than we anticipate, especially if regulatory bodies require completion of non-inferiority or superiority trials, enrollment in these clinical trials may be slower than we anticipate or subjects may drop out of these clinical trials or fail to return for post-treatment follow-up at a higher rate than we anticipate; |
89
| ● | our third-party contractors may fail to comply with regulatory requirements or meet their contractual obligations to us in a timely manner, or at all, or may deviate from the clinical trial protocol or drop out of the trial, which may require that we add new clinical trial sites or investigators; |
| ● | we may elect to, or regulators, IRBs or ethics committees may require that we or our investigators, suspend or terminate clinical research or trials for various reasons, including noncompliance with regulatory requirements or a finding that the participants in our trials are being exposed to unacceptable health risks; |
| ● | the cost of clinical trials of any of our programs may be greater than we anticipate; |
| ● | the quality of our programs or other materials necessary to conduct clinical trials of our programs may be inadequate to initiate or complete a given clinical trial; |
| ● | our inability to manufacture sufficient quantities of our programs for use in clinical trials, or delays in manufacturing or distribution; |
| ● | reports from clinical testing of other therapies may raise safety or efficacy concerns about our programs; |
| ● | our failure to establish an appropriate safety profile for a program based on clinical or preclinical data for such programs as well as data emerging from other therapies in the same class as our programs; and |
| ● | the FDA or other regulatory authorities may require us to submit additional data such as additional toxicology studies, or impose other requirements before permitting us to initiate a clinical trial. |
Commencing clinical trials in the United States is subject to acceptance by the FDA of an IND, biologics license application (“BLA”) or similar application and finalizing the trial design based on discussions with the FDA and other regulatory authorities. In the event that the FDA requires us to complete additional preclinical studies or we are required to satisfy other FDA requests prior to commencing future clinical trials, the start of such clinical trials may be delayed. Even after we receive and incorporate guidance from these regulatory authorities, the FDA or other regulatory authorities could disagree that we have satisfied their requirements to commence any future clinical trial or change their position on the acceptability of our trial design or the clinical endpoints selected, which may require us to complete additional preclinical studies or clinical trials, delay the enrollment of our clinical trials or impose stricter approval conditions than we currently expect. There are equivalent processes and risks applicable to clinical trial applications in other countries, including countries in the European Union (“EU”).
We may not have the financial resources to continue development of, or to modify existing or enter into new collaborations for, a program if we experience any issues that delay or prevent regulatory approval of, or our ability to commercialize, our programs. We or our current or future collaborators’ inability to complete development of, or commercialize our programs, or significant delays in doing so, could have a material and adverse effect on our business, financial condition, results of operations and prospects.
We are substantially dependent on the success of our two most advanced programs, APG777 and APG808, and our ongoing and anticipated trials of APG777 and anticipated clinical trial of APG808 may not be successful.
Our future success is substantially dependent on our ability to timely obtain marketing approval for, and then successfully commercialize, our two most advanced programs, APG777 and APG808. We are investing a majority of our efforts and financial resources into the research and development of these programs. We initiated our Phase 1 clinical trial for APG777 in healthy volunteers and announced the dosing of our first participant in August 2023. We finalized the nomination of a development candidate for APG808 in the fourth quarter of 2023 and plan to initiate a Phase 1 clinical trial in the first half of 2024 in healthy volunteers in Australia. The success of our programs is dependent on observing a longer half-life of our programs in humans than other monoclonal antibodies currently marketed and in development as we believe this longer half-life has the potential to result in a more favorable dosing schedule for our programs, assuming they successfully complete clinical development and obtain marketing approval.
90
This is based in part on the assumption that the longer half-life we have observed in non-human primates (“NHPs”) will translate into an extended half-life of our programs in humans. To the extent we do not observe this extended half-life when we dose humans with our programs, it would significantly and adversely affect the clinical and commercial potential of our programs.
Our programs will require additional clinical development, evaluation of clinical, preclinical and manufacturing activities, marketing approval in multiple jurisdictions, substantial investment and significant marketing efforts before we generate any revenues from product sales. We are not permitted to market or promote these programs, or any other programs, before we receive marketing approval from the FDA and comparable foreign regulatory authorities, and we may never receive such marketing approvals.
The success of our programs will depend on a variety of factors. We do not have complete control over many of these factors, including certain aspects of clinical development and the regulatory submission process, potential threats to our intellectual property rights and the manufacturing, marketing, distribution and sales efforts of any future collaborator. Accordingly, we cannot assure you that we will ever be able to generate revenue through the sale of these programs, even if approved. If we are not successful in commercializing APG777 or APG808, or are significantly delayed in doing so, our business will be materially harmed.
If we do not achieve our projected development goals in the time frames we announce and expect, the commercialization of our programs may be delayed and our expenses may increase and, as a result, our stock price may decline.
From time to time, we estimate the timing of the anticipated accomplishment of various scientific, clinical, regulatory and other product development goals, which we sometimes refer to as milestones. These milestones may include the commencement or completion of scientific studies and clinical trials, such as the expected timing for the completion of our Phase 1 clinical trial in AD and expected initiation of and topline data from our planned Phase 2 clinical trial in AD, as well as the submission of regulatory filings. From time to time, we may publicly announce the expected timing of some of these milestones. All of these milestones are and will be based on numerous assumptions. The actual timing of these milestones can vary dramatically compared to our estimates, in some cases for reasons beyond our control. If we do not meet these milestones as publicly announced, or at all, the commercialization of our programs may be delayed or never achieved and, as a result, our stock price may decline. Additionally, delays relative to our projected timelines are likely to cause overall expenses to increase, which may require us to raise additional capital sooner than expected and prior to achieving targeted development milestones.
Our approach to the discovery and development of our programs is unproven, and we may not be successful in our efforts to build a pipeline of programs with commercial value.
Our approach to the discovery and development of our programs leverages clinically validated mechanisms of action and incorporates advanced antibody engineering to optimize half-life and other properties designed to overcome limitations of existing therapies. Our programs are purposefully designed to improve upon existing product candidates and products while maintaining the same, well-established mechanisms of action. However, the scientific research that forms the basis of our efforts to develop programs using half-life extension technologies, including YTE and LS amino acid modification, is ongoing and may not result in viable programs. We have limited clinical data on product candidates utilizing YTE and LS half-life extension technologies, especially in I&I indications, demonstrating whether they are safe or effective for long-term treatment in humans. The long-term safety and efficacy of these technologies and the extended half-life and exposure profile of our programs compared to currently approved products is unknown.
We may ultimately discover that utilizing half-life extension technologies for our specific targets and indications and any programs resulting therefrom do not possess certain properties required for therapeutic effectiveness. We currently have only preclinical data regarding the increased half-life properties of our programs and the same results may not be seen in humans. In addition, programs using half-life extension technologies may demonstrate different chemical and pharmacological properties in patients than they do in laboratory studies. This technology and any programs resulting therefrom may not demonstrate the same chemical and pharmacological properties in humans and may interact with human biological systems in unforeseen, ineffective or harmful ways.
91
In addition, we may in the future seek to discover and develop programs that are based on novel targets and technologies that are unproven. If our discovery activities fail to identify novel targets or technologies for drug discovery, or such targets prove to be unsuitable for treating human disease, we may not be able to develop viable additional programs. We and our existing or future collaborators may never receive approval to market and commercialize any program. Even if we or an existing or future collaborator obtains regulatory approval, the approval may be for targets, disease indications or patient populations that are not as broad as we intended or desired or may require labeling that includes significant use or distribution restrictions or safety warnings. If the products resulting from our programs prove to be ineffective, unsafe or commercially unviable, our programs and pipeline would have little, if any, value, which would have a material and adverse effect on our business, financial condition, results of operations and prospects.
Preclinical and clinical development involves a lengthy and expensive process that is subject to delays and with uncertain outcomes, and results of earlier studies and trials may not be predictive of future clinical trial results. If our preclinical studies and clinical trials are not sufficient to support regulatory approval of any of our programs, we may incur additional costs or experience delays in completing, or ultimately be unable to complete, the development of such program.
Before obtaining marketing approval from regulatory authorities for the sale of any program, we must complete preclinical studies and conduct extensive clinical trials to demonstrate the safety and efficacy of our program in humans. Our clinical trials may not be conducted as planned or completed on schedule, if at all, and failure can occur at any time during the preclinical study or clinical trial process. For example, we depend on the availability of NHPs to conduct certain preclinical studies that we are required to complete prior to submitting an IND or foreign equivalent and initiating clinical development. There is currently a global shortage of NHPs available for drug development. This could cause the cost of obtaining NHPs for our future preclinical studies to increase significantly and, if the shortage continues, could also result in delays to our development timelines.
Furthermore, a failure of one or more clinical trials can occur at any stage of testing. The outcome of preclinical studies and early-stage clinical trials may not be predictive of the success of later clinical trials. Moreover, preclinical and clinical data are often susceptible to varying interpretations and analyses, and many companies that have believed their programs performed satisfactorily in preclinical studies and clinical trials have nonetheless failed to obtain marketing approval of their programs. In addition, we expect to rely on patients to provide feedback on measures such as itch and quality of life, which are subjective and inherently difficult to evaluate. These measures can be influenced by factors outside of our control, and can vary widely from day to day for a particular patient, and from patient to patient and from site to site within a clinical trial.
We cannot be sure that the FDA will agree with our clinical development plan. We plan to use the data from our ongoing Phase 1 trial of APG777 in healthy volunteers to support Phase 2 trials in AD and other I&I indications. If the FDA requires us to conduct additional trials or enroll additional patients, our development timelines may be delayed. We cannot be sure that submission of an IND, BLA or similar application will result in the FDA or comparable foreign regulatory authorities, as applicable, allowing clinical trials to begin in a timely manner, if at all. Moreover, even if these trials begin, issues may arise that could cause regulatory authorities to suspend or terminate such clinical trials. Events that may prevent successful or timely initiation or completion of clinical trials include: inability to generate sufficient preclinical, toxicology or other in vivo or in vitro data to support the initiation or continuation of clinical trials; delays in reaching a consensus with regulatory authorities on study design or implementation of the clinical trials; delays or failure in obtaining regulatory authorization to commence a trial; delays in reaching agreement on acceptable terms with prospective CROs and clinical trial sites, the terms of which can be subject to extensive negotiation and may vary significantly among different CROs and clinical trial sites; delays in identifying, recruiting and training suitable clinical investigators; delays in obtaining required IRB approval at each clinical trial site; delays in manufacturing, testing, releasing, validating or importing/exporting sufficient stable quantities of our programs for use in clinical trials or the inability to do any of the foregoing; failure by our CROs, other third parties or us to adhere to clinical trial protocols; failure to perform in accordance with the FDA’s or any other regulatory authority’s good clinical practice requirements (“GCPs”) or applicable regulatory guidelines in other countries; changes to the clinical trial protocols; clinical sites deviating from trial protocol or dropping out of a trial; changes in regulatory requirements and guidance that require amending or submitting new clinical protocols; selection of clinical endpoints that require prolonged periods of observation or analyses of resulting data; transfer of manufacturing processes to larger-scale facilities operated by a CMO and delays or failure by our CMOs or us to make any necessary changes to such manufacturing process; and third parties being unwilling or unable to satisfy their contractual obligations to us.
92
We could also encounter delays if a clinical trial is suspended or terminated by us, by the IRBs of the institutions in which such clinical trials are being conducted, by the Data Safety Monitoring Board, if any, for such clinical trial or by the FDA or comparable foreign regulatory authorities. Such authorities may suspend or terminate a clinical trial due to a number of factors, including failure to conduct the clinical trial in accordance with regulatory requirements or our clinical trial protocols, inspection of the clinical trial operations or trial site by the FDA or comparable foreign regulatory authorities resulting in the imposition of a clinical hold, unforeseen safety issues or adverse side effects, failure to demonstrate a benefit from the programs, changes in governmental regulations or administrative actions or lack of adequate funding to continue the clinical trial. If we are required to conduct additional clinical trials or other testing of our programs beyond those that we currently contemplate, if we are unable to successfully complete clinical trials of our programs, if the results of these trials are not positive or are only moderately positive or if there are safety concerns, our business and results of operations may be adversely affected and we may incur significant additional costs.
If we encounter difficulties enrolling patients in our current and future clinical trials, our clinical development activities could be delayed or otherwise adversely affected.
We may experience difficulties in patient enrollment in our current and future clinical trials for a variety of reasons. The timely completion of clinical trials in accordance with their protocols depends, among other things, on our ability to enroll a sufficient number of patients who remain in the trial until its conclusion. The enrollment of patients in current or future trials for any of our programs will depend on many factors, including if patients choose to enroll in clinical trials, rather than using approved products, or if our competitors have ongoing clinical trials for programs that are under development for the same indications as our programs, and patients instead enroll in such clinical trials. Additionally, the number of patients required for clinical trials of our programs may be larger than we anticipate, especially if regulatory bodies require the completion of non-inferiority or superiority trials. Even if we are able to enroll a sufficient number of patients for our current or future clinical trials, we may have difficulty maintaining patients in our clinical trials. Our inability to enroll or maintain a sufficient number of patients would result in significant delays in completing clinical trials or receipt of marketing approvals and increased development costs or may require us to abandon one or more clinical trials altogether.
Preliminary, “topline” or interim data from our clinical trials that we announce or publish from time to time may change as more patient data become available and are subject to audit and verification procedures.
From time to time, we may publicly disclose preliminary or topline data from our preclinical studies and clinical trials, which are based on a preliminary analysis of then-available data, and the results and related findings and conclusions are subject to change following a more comprehensive review of the data. We also make assumptions, estimations, calculations and conclusions as part of our analyses of these data without the opportunity to fully and carefully evaluate complete data. As a result, the preliminary or topline results that we report may differ from future results of the same studies, or different conclusions or considerations may qualify such results, once additional data have been received and fully evaluated or subsequently made subject to audit and verification procedures.
Any preliminary or topline data should be viewed with caution until the final data are available. From time to time, we may also disclose interim data from our preclinical studies and clinical trials. Interim data are subject to the risk that one or more of the clinical outcomes may materially change as patient enrollment continues and more patient data become available or as patients from our clinical trials continue other treatments. Further, others, including regulatory agencies, may not accept or agree with our assumptions, estimates, calculations, conclusions or analyses or may interpret or weigh the importance of data differently, which could impact the value of the particular program, the approvability or commercialization of the particular program and our company in general. In addition, the information we choose to publicly disclose regarding a particular preclinical study or clinical trial is based on what is typically extensive information, and you or others may not agree with what we determine is material or otherwise appropriate information to include in our disclosure. If the preliminary, topline or interim data that we report differ from actual results, or if others, including regulatory authorities, disagree with the conclusions reached, our ability to obtain approval for, and commercialize, our programs may be harmed, which could harm our business, operating results, prospects or financial condition.
93
Our current and future clinical trials or those of our future collaborators may reveal significant adverse events or undesirable side effects not seen in our preclinical studies and may result in a safety profile that could halt clinical development, inhibit regulatory approval or limit commercial potential or market acceptance of any of our programs.
Results of our clinical trials could reveal a high and unacceptable severity and prevalence of side effects, adverse events or unexpected characteristics. While our preclinical studies in NHPs have not shown any such characteristics to date, we cannot assure you that the results of our clinical trials will not reveal such characteristics. If significant adverse events or other side effects are observed in any of our current or future clinical trials, we may have difficulty recruiting patients to such trials, patients may drop out of our trials, or we may be required to abandon the trials or our development efforts of one or more programs altogether. For example, certain drugs targeting IL-13 have previously demonstrated increased conjunctivitis in patients with AD. We, the FDA or other applicable regulatory authorities, or an IRB, may suspend any clinical trials of any program at any time for various reasons, including a belief that subjects or patients in such trials are being exposed to unacceptable health risks or adverse side effects. Some potential products developed in the biotechnology industry that initially showed therapeutic promise in early-stage studies and trials have later been found to cause side effects that prevented their further development. Other potential products have shown side effects in preclinical studies, which side effects do not present themselves in clinical trials in humans. Even if the side effects do not preclude the program from obtaining or maintaining marketing approval, undesirable side effects may inhibit market acceptance of the approved product due to its tolerability versus other therapies. In addition, an extended half-life could prolong the duration of undesirable side effects, which could also inhibit market acceptance. Treatment-emergent adverse events could also affect patient recruitment or the ability of enrolled subjects to complete our clinical trials or could result in potential product liability claims. Potential side effects associated with our programs may not be appropriately recognized or managed by the treating medical staff, as toxicities resulting from our programs may not be normally encountered in the general patient population and by medical personnel. Any of these occurrences could harm our business, financial condition, results of operations and prospects significantly.
In addition, even if we successfully advance our programs or any future program through clinical trials, such trials will only include a limited number of patients and limited duration of exposure to our programs. As a result, we cannot be assured that adverse effects of our programs will not be uncovered when a significantly larger number of patients are exposed to the program after approval. Further, any clinical trials may not be sufficient to determine the effect and safety consequences of using our programs over a multi-year period.
If any of the foregoing events occur or if one or more of our programs prove to be unsafe, our entire pipeline could be affected, which would have a material adverse effect on our business, financial condition, results of operations and prospects.
We may expend our limited resources to pursue a particular program and fail to capitalize on programs that may be more profitable or for which there is a greater likelihood of success.
Because we have limited financial and managerial resources, we focus our research and development efforts on certain selected programs.
For example, we are initially focused on our most advanced programs, APG777 and APG808. As a result, we may forgo or delay pursuit of opportunities with other programs that later prove to have greater commercial potential. Our resource allocation decisions may cause us to fail to capitalize on viable commercial products or profitable market opportunities. Our spending on current and future research and development programs for specific indications may not yield any commercially viable programs. If we do not accurately evaluate the commercial potential or target market for a particular program, we may relinquish valuable rights to that program through collaboration, licensing or other royalty arrangements in cases in which it would have been more advantageous for us to retain sole development and commercialization rights to such program.
94
Any approved products resulting from our current programs or any future program may not achieve adequate market acceptance among clinicians, patients, healthcare third-party payors and others in the medical community necessary for commercial success and we may not generate any future revenue from the sale or licensing of such products.
Even if regulatory approval is obtained for a product candidate resulting from one of our current or future programs, they may not gain market acceptance among physicians, patients, healthcare payors or the medical community. We may not generate or sustain revenue from sales of the product due to factors such as whether the product can be sold at a competitive cost and whether it will otherwise be accepted in the market.
There are several approved products and product candidates in later stages of development for the treatment of AD, including DUPIXENT, a well-established treatment for moderate-to-severe AD. However, our programs incorporate advanced antibody engineering to optimize half-life of antibodies targeting IL-13, IL-4Ra and OX40L; to date, no such antibody has been approved by the FDA for the treatment of AD. Market participants with significant influence over acceptance of new treatments, such as clinicians and third-party payors, may not adopt a biologic that incorporates half-life extension for our targeted indications, and we may not be able to convince the medical community and third-party payors to accept and use, or to provide favorable reimbursement for, any programs developed by us or our existing or future collaborators. An extended half-life may make it more difficult for patients to change treatments and there is a perception that half-life extension could exacerbate side effects, each of which may adversely affect our ability to gain market acceptance. Market acceptance of our programs will depend on many factors, including factors that are not within our control.
Sales of medical products also depend on the willingness of clinicians to prescribe the treatment. We cannot predict whether clinicians, clinicians’ organizations, hospitals, other healthcare providers, government agencies or private insurers will determine that our product is safe, therapeutically effective, cost effective or less burdensome as compared with competing treatments. If any current or future program is approved but does not achieve an adequate level of acceptance by such parties, we may not generate or derive sufficient revenue from that program and may not become or remain profitable.
Certain of our programs may compete with our other programs, which could negatively impact our business and reduce our future revenue.
We are developing APG777, APG990 and APG222 for the same indication: atopic dermatitis, and may in the future develop our programs for other I&I indications. Each such program targets a different mechanism of action. Based on the differing mechanisms of action, we are developing APG777 as a frontline treatment for patients with moderate-to-severe AD who have failed or have an inadequate response to topical corticosteroids. APG990 and APG222 may serve as alternative treatments for either frontline patients or patients who have failed or have inadequate responses to other treatment options. However, developing multiple programs for a single indication may negatively impact our business if the programs compete with each other. For example, if multiple programs are conducting clinical trials at the same time, they could compete for the enrollment of patients. In addition, if multiple programs are approved for the same indication, they may compete for market share, which could limit our future revenue.
We are conducting and may conduct future clinical trials for our programs at sites outside the United States, and the FDA may not accept data from trials conducted in such locations.
We are conducting our Phase 1 clinical trial for APG777 in Australia, are planning to conduct our Phase 1 clinical trial for APG808 in Australia, and we may choose to conduct one or more of our future clinical trials outside the United States. Although the FDA may accept data from clinical trials conducted outside the United States, acceptance of this data is subject to conditions imposed by the FDA. For example, the clinical trial must be well designed and conducted and performed by qualified investigators in accordance with ethical principles. The trial population must also adequately represent the U.S. population, and the data must be applicable to the U.S. population and U.S. medical practice in ways that the FDA deems clinically meaningful. In addition, while these clinical trials are subject to the applicable local laws, FDA acceptance of the data will depend on its determination that the trials also complied with all applicable U.S. laws and regulations. If the FDA does not accept the data from any trial that we conduct outside the United States, it would likely result in the need for additional trials, which would be costly and time-consuming and would delay or permanently halt our development of the applicable product candidates.
95
Even if the FDA accepted such data, it could require us to modify our planned clinical trials to receive clearance to initiate such trials in the United States or to continue such trials once initiated.
Further, conducting international clinical trials presents additional risks that may delay completion of our clinical trials. These risks include the failure of enrolled patients in foreign countries to adhere to clinical protocol as a result of differences in healthcare services or cultural customs that could restrict or limit our ability to conduct our clinical trials, the administrative burdens of conducting clinical trials under multiple sets of foreign regulations, foreign exchange fluctuations, diminished protection of intellectual property in some countries, as well as political and economic risks relevant to foreign countries.
Risks Related to Our Reliance on Third Parties
We rely on collaborations and licensing arrangements with third parties, including our collaboration with Paragon. If we are unable to maintain these collaborations or licensing arrangements, or if these collaborations or licensing arrangements are not successful, our business could be negatively impacted.
We currently rely on our collaborations and licensing arrangements with third parties, including Paragon, for a substantial portion of our discovery capabilities and in-licenses. We consider Paragon to be a related party because Paragon beneficially owns more than 5% of our capital stock and Fairmount Funds Management LLC, which beneficially owns more than 5% of Paragon, beneficially owns more than 5% of our capital stock and has two seats on our Board of Directors (the Board).
Collaborations or licensing arrangements that we enter into may not be successful, and any success will depend heavily on the efforts and activities of such collaborators or licensors. If any of our collaborators or licensors experiences delays in performance of, or fails to perform its obligations under their agreement with us, disagrees with our interpretation of the terms of such agreement or terminates their agreement with us, our pipeline and programs and development timeline could be adversely affected. If we fail to comply with any of the obligations under our collaborations or license agreements, including payment terms and diligence terms, our collaborators or licensors may have the right to terminate such agreements, in which event we may lose intellectual property rights and may not be able to develop, manufacture, market or sell the products covered by our agreements or may face other penalties under our agreements. Our collaborators and licensors may also fail to properly maintain or defend the intellectual property we have licensed from them, if required by our agreement with them, or even infringe upon, our intellectual property rights, leading to the potential invalidation of our intellectual property or subjecting us to litigation or arbitration, any of which would be time-consuming and expensive and could harm our ability to commercialize our programs. In addition, collaborators could independently develop, or develop with third parties, products that compete directly or indirectly with our programs and products if the collaborators believe that the competitive products are more likely to be successfully developed or can be commercialized under terms that are more economically attractive than ours.
As part of our strategy, we plan to evaluate additional opportunities to enhance our capabilities and expand our development pipeline or provide development or commercialization capabilities that complement our own. We may not realize the benefits of such collaborations, alliances or licensing arrangements. Any of these relationships may require us to incur non-recurring and other charges, increase our near and long-term expenditures, issue securities that dilute our existing stockholders or disrupt our management and business.
We may face significant competition in attracting appropriate collaborators, and more established companies may also be pursuing strategies to license or acquire third-party intellectual property rights that we consider attractive. These companies may have a competitive advantage over us due to their size, financial resources and greater clinical development and commercialization capabilities. In addition, companies that perceive us to be a competitor may be unwilling to assign or license rights to us. Whether we reach a definitive agreement for a collaboration will depend, among other things, upon our assessment of the collaborator’s resources and expertise, the terms and conditions of the proposed collaboration and the proposed collaborator’s evaluation of a number of factors. Collaborations are complex and time-consuming to negotiate, document and execute. In addition, consolidation among large pharmaceutical and biotechnology companies has reduced the number of potential future collaborators. We may not be able to negotiate additional collaborations on a timely basis, on acceptable terms or at all.
96
If we fail to enter into collaborations and do not have sufficient funds or expertise to undertake the necessary development and commercialization activities, we may not be able to further develop our programs or bring them to market.
We currently rely, and plan to rely in the future, on third parties to conduct and support our preclinical studies and clinical trials. If these third parties do not properly and successfully carry out their contractual duties or meet expected deadlines, we may not be able to obtain regulatory approval of or commercialize our programs.
We have utilized and plan to continue to utilize and depend upon independent investigators and collaborators, such as medical institutions, CROs, contract testing labs and strategic partners, to conduct and support our preclinical studies and clinical trials under agreements with us. We will rely heavily on these third parties over the course of our preclinical studies and clinical trials, and we control only certain aspects of their activities. As a result, we will have less direct control over the conduct, timing and completion of these preclinical studies and clinical trials and the management of data developed through preclinical studies and clinical trials than would be the case if we were relying entirely upon our own staff. Nevertheless, we are responsible for ensuring that each of our studies and trials is conducted in accordance with the applicable protocol, legal, regulatory and scientific standards, and our reliance on these third parties does not relieve us of our regulatory responsibilities. We and our third-party contractors and CROs are required to comply with GCP regulations, which are regulations and guidelines enforced by the FDA and comparable foreign regulatory authorities for all of our programs in clinical development. If we or any of these third parties fail to comply with applicable GCP regulations, the clinical data generated in our clinical trials may be deemed unreliable and the FDA or comparable foreign regulatory authorities may require us to perform additional clinical trials before approving our marketing applications. We cannot assure you that upon inspection by a given regulatory authority, such regulatory authority will determine that any of our clinical trials comply with GCP regulations. In addition, our clinical trials must be conducted with products produced under cGMP regulations. Our failure to comply with these regulations may require us to repeat clinical trials, which would delay the regulatory approval process. Moreover, our business may be implicated if any of these third parties violates federal or state fraud and abuse or false claims laws and regulations or healthcare privacy and security laws.
Any third parties conducting our clinical trials will not be our employees and, except for remedies available to us under our agreements with such third parties, we cannot control whether they devote sufficient time and resources to our programs. These third parties may be involved in mergers, acquisitions or similar transactions and may have relationships with other commercial entities, including our competitors, for whom they may also be conducting clinical trials or other product development activities, which could negatively affect their performance on our behalf and the timing thereof and could lead to products that compete directly or indirectly with our current or future programs. If these third parties do not successfully carry out their contractual duties or obligations or meet expected deadlines, if they need to be replaced or if the quality or accuracy of the clinical data they obtain is compromised due to the failure to adhere to our clinical protocols or regulatory requirements or for other reasons, our clinical trials may be extended, delayed or terminated and we may not be able to complete development of, obtain regulatory approval of or successfully commercialize our programs.
In addition, we currently rely on foreign CROs and CMOs, including WuXi Biologics, and will likely continue to rely on foreign CROs and CMOs in the future. Foreign CMOs may be subject to U.S. legislation, including the proposed BIOSECURE Act, sanctions, trade restrictions and other foreign regulatory requirements which could increase the cost or reduce the supply of material available to us, delay the procurement or supply of such material or have an adverse effect on our ability to secure significant commitments from governments to purchase our potential therapies.
For example, the biopharmaceutical industry in China is strictly regulated by the Chinese government. Changes to Chinese regulations or government policies affecting biopharmaceutical companies are unpredictable and may have a material adverse effect on our collaborators in China which could have an adverse effect on our business, financial condition, results of operations and prospects. Evolving changes in China’s public health, economic, political, and social conditions and the uncertainty around China’s relationship with other governments, such as the United States and the U.K., could also negatively impact our ability to manufacture our product candidates for our planned clinical trials or have an adverse effect on our ability to secure government funding, which could adversely affect our financial condition and cause us to delay our clinical development programs.
97
We currently rely and expect to rely in the future on the use of manufacturing suites in third-party facilities or on third parties to manufacture our programs, and we may rely on third parties to produce and process our products, if approved. Our business could be adversely affected if we are unable to use third-party manufacturing suites or if the third-party manufacturers encounter difficulties in production.
We do not currently own any facility that may be used as our clinical-scale manufacturing and processing facility and must currently rely on CMOs for developing and manufacturing our programs and product candidates. We have not yet caused our programs or product candidates to be manufactured on a commercial scale and may not be able to do so for any of our programs or product candidates, if approved. We currently have a sole source relationship for our preclinical and clinical supply of APG777 and APG808 and preclinical supply of APG990. If there should be any disruption in such supply arrangement, including any adverse events affecting our sole supplier, it could have a negative effect on the clinical development of our programs and other operations while we work to identify and qualify an alternate supply source. We may not control the manufacturing process of, and may be completely dependent on, our contract manufacturing partners for compliance with cGMP requirements and any other regulatory requirements of the FDA or comparable foreign regulatory authorities for the manufacture of our programs. Beyond periodic audits, we have no control over the ability of our CMOs to maintain adequate quality control, quality assurance and other qualified personnel. If the FDA or a comparable foreign regulatory authority does not approve these facilities for the manufacture of our programs or if it withdraws any approval in the future, we may need to find alternative manufacturing facilities, which would require the incurrence of significant additional costs and materially adversely affect our ability to develop, obtain regulatory approval for or market our programs, if approved. Similarly, our failure, or the failure of our CMOs, to comply with applicable regulations could result in sanctions being imposed on us, including fines, injunctions, civil penalties, delays, suspension or withdrawal of approvals, license revocation, seizures or recalls of programs or drugs, operating restrictions and criminal prosecutions, any of which could significantly and adversely affect supplies of our programs or drugs and harm our business and results of operations.
Moreover, our CMOs may experience manufacturing difficulties due to resource constraints, supply chain issues, or as a result of labor disputes or unstable political environments. If any CMOs on which we will rely fail to manufacture quantities of our programs at quality levels necessary to meet regulatory requirements and at a scale sufficient to meet anticipated demand at a cost that allows us to achieve profitability, our business, financial condition and prospects could be materially and adversely affected. In addition, our CMOs and other vendors are responsible for transporting temperature-controlled materials that can be inadvertently degraded during transport due to several factors, rendering certain batches unsuitable for trial use for failure to meet, among others, our integrity and purity specifications. We and any of our CMOs may also face product seizure or detention or refusal to permit the import or export of products. Our business could be materially adversely affected by business disruptions to our third-party providers that could materially adversely affect our anticipated timelines, potential future revenue and financial condition and increase our costs and expenses. Each of these risks could delay or prevent the completion of our preclinical studies and clinical trials or the approval of any of our programs by the FDA, resulting in higher costs or adversely impacting commercialization of our programs. See the section titled “Business-Manufacturing and Supply” for a more detailed description of our manufacturing and supply plans and assumptions and the factors that may affect the success of our programs.
Risks Related to Our Business and Operations
In order to successfully implement our plans and strategies, we will need to grow the size of our organization and we may experience difficulties in managing this growth.
We expect to experience significant growth in the number of our employees and the scope of our operations, particularly in the areas of preclinical and clinical drug development, technical operations, clinical operations, regulatory affairs and, potentially, sales and marketing. To manage our anticipated future growth, we must continue to implement and improve our managerial, operational and financial personnel and systems, expand our facilities and continue to recruit and train additional qualified personnel. We are dependent on the experience of our management team, who have only worked together for a limited time in managing a public company with such anticipated growth, and we may not be able to effectively manage the expansion of our operations or recruit and train additional qualified personnel.
98
We are highly dependent on our key personnel and anticipate hiring new key personnel. If we are not successful in attracting and retaining highly qualified personnel, we may not be able to successfully implement our business strategy.
Our ability to compete in the highly competitive biotechnology and pharmaceutical industries depends upon our ability to attract and retain highly qualified managerial, scientific and medical personnel. We are highly dependent on our managerial, scientific and medical personnel, including our Chief Executive Officer, Chief Medical Officer, Chief Financial Officer and other key members of our leadership team. Although we have entered into employment agreements with our executive officers, each of them may terminate their employment with us at any time. We do not maintain “key person” insurance for any of our executives or other employees.
The loss of the services of our executive officers or other key employees could impede the achievement of our research, development and commercialization objectives and seriously harm our ability to successfully implement our business strategy. Furthermore, replacing executive officers and key personnel may be difficult and may take an extended period of time. If we do not succeed in attracting and retaining qualified personnel, it could materially adversely affect our business, financial condition and results of operations. We could in the future have difficulty attracting and retaining experienced personnel and may be required to expend significant financial resources in our employee recruitment and retention efforts.
Our future growth may depend, in part, on our ability to operate in foreign markets, where we would be subject to additional regulatory burdens and other risks and uncertainties.
Our future growth may depend, in part, on our ability to develop and commercialize our programs in foreign markets for which we may rely on collaboration with third parties. We are not permitted to market or promote any of our programs before we receive regulatory approval from the applicable foreign regulatory authority, and may never receive such regulatory approval for any of our programs. To obtain separate regulatory approval in many other countries, we must comply with numerous and varying regulatory requirements of such countries regarding safety and efficacy and governing, among other things, clinical trials and commercial sales, pricing and distribution of our programs, and we cannot predict success in these jurisdictions. If we fail to comply with the regulatory requirements in international markets and receive applicable marketing approvals, our target market will be reduced and our ability to realize the full market potential of our programs will be harmed and our business will be adversely affected. Moreover, even if we obtain approval of our programs and ultimately commercialize our programs in foreign markets, we would be subject to the risks and uncertainties, including the burden of complying with complex and changing foreign regulatory, tax, accounting and legal requirements and reduced protection of intellectual property rights in some foreign countries.
Our employees, independent contractors, consultants, commercial collaborators, principal investigators, CROs, CMOs, suppliers and vendors may engage in misconduct or other improper activities, including noncompliance with regulatory standards and requirements.
We are exposed to the risk that our employees, independent contractors, consultants, commercial collaborators, principal investigators, CROs, CMOs, suppliers and vendors acting for or on our behalf may engage in misconduct or other improper activities. While we have adopted a code of conduct, it is not always possible to identify and deter misconduct by these parties and the precautions we take to detect and prevent this activity may not be effective in controlling unknown or unmanaged risks or losses or in protecting us from governmental investigations or other actions or lawsuits stemming from a failure to comply with these laws or regulations.
Our internal information technology systems, or those of any of our CROs, manufacturers, other contractors or consultants, third party service providers, or potential future collaborators, may fail or suffer security or data privacy breaches or other unauthorized or improper access to, use of, or destruction of our proprietary or confidential data, employee data or personal data, which could result in additional costs, loss of revenue, significant liabilities, harm to our brand and material disruption of our operations.
In the ordinary course of our business, we and the third parties upon which we rely collect, receive, store, process, generate, use, transfer, disclose, make accessible, protect, secure, dispose of, transmit, and share (collectively, process)
99
proprietary, confidential, and sensitive data, including personal data, intellectual property, trade secrets, and other sensitive data (collectively, sensitive information).
We may implement a variety of security measures designed to protect systems that store our information, given their size and complexity and the increasing amounts of information maintained on our internal information technology systems and those of our third-party CROs, other contractors (including sites performing our clinical trials), third party service providers and supply chain companies, and consultants, these systems are potentially vulnerable to breakdown or other damage or interruption from service interruptions, system malfunction, natural disasters, terrorism, war and telecommunication and electrical failures, as well as security breaches from inadvertent or intentional actions by our employees, contractors, consultants, business partners and/or other third parties, or from cyber-attacks by malicious third parties, which may compromise our system infrastructure or lead to the loss, destruction, alteration or dissemination of, or damage to, our data.
Some actors now engage and are expected to continue to engage in cyber-attacks, including without limitation nation-state actors for geopolitical reasons and in conjunction with military conflicts and defense activities. During times of war and other major conflicts, we, and the third parties upon which we rely, may be vulnerable to a heightened risk of these attacks, including retaliatory cyber-attacks, that could materially disrupt our systems and operations, supply chain, and ability to produce, sell and distribute our goods and services. In particular, severe ransomware attacks are becoming increasingly prevalent and can lead to significant interruptions in our operations, ability to provide our products or services, loss of sensitive data and income, reputational harm, and diversion of funds. Extortion payments may alleviate the negative impact of a ransomware attack, but we may be unwilling or unable to make such payments due to, for example, applicable laws or regulations prohibiting such payments.
To the extent that any disruption or security breach were to result in loss, destruction, unavailability, alteration or dissemination of, or damage to, our data or applications, or for it to be believed or reported that any of these occurred, we could incur liability and reputational damage and the development and commercialization of our programs could be delayed. Further, our insurance policies may not be adequate to compensate us for the potential losses arising from any such disruption in, or failure or security breach of, our systems or third-party systems where information important to our business operations or commercial development is stored.
Our remote workforce may create additional risks for our information technology systems and data because a majority of our employees work remotely and utilize network connections, computers, and devices working at home, while in transit and in public locations. Additionally, business transactions (such as acquisitions or integrations) could expose us to additional cybersecurity risks and vulnerabilities, as our systems could be negatively affected by vulnerabilities present in acquired or integrated entities’ systems and technologies.
While we have implemented security measures designed to protect against security incidents, there can be no assurance that these measures will be effective. We may be unable in the future to detect vulnerabilities in our information technology systems because such threats and techniques change frequently, are often sophisticated in nature, and may not be detected until after a security incident has occurred. Further, we may experience delays in developing and deploying remedial measures designed to address any such identified vulnerabilities. Applicable data privacy and security obligations may require us to notify relevant stakeholders of security incidents. Such disclosures are costly, and the disclosure or the failure to comply with such requirements could lead to adverse consequences.
We rely on third-party service providers and technologies to operate critical business systems to process sensitive information in a variety of contexts. Our ability to monitor these third parties’ information security practices is limited, and these third parties may not have adequate information security measures in place. If our third-party service providers experience a security incident or other interruption, we could experience adverse consequences. While we may be entitled to damages if our third-party service providers fail to satisfy their privacy or security-related obligations to us, any award may be insufficient to cover our damages, or we may be unable to recover such award. In addition, supply-chain attacks have increased in frequency and severity, and we cannot guarantee that third parties’ infrastructure in our supply chain or our third-party partners’ supply chains have not been compromised.
100
If we (or a third party upon whom we rely) experience a security incident or are perceived to have experienced a security incident, we may experience adverse consequences, such as government enforcement actions (for example, investigations, fines, penalties, audits, and inspections); additional reporting requirements and/or oversight; restrictions on processing sensitive information (including personal data); litigation (including class claims); indemnification obligations; negative publicity; reputational harm; monetary fund diversions; interruptions in our operations (including availability of data); financial loss; and other similar harms. Security incidents and attendant consequences may cause stakeholders (including investors and potential customers) to stop supporting our platform, deter new customers from products, and negatively impact our ability to grow and operate our business.
Our contracts may not contain limitations of liability, and even where they do, there can be no assurance that limitations of liability in our contracts are sufficient to protect us from liabilities, damages, or claims related to our data privacy and security obligations. We cannot be sure that our insurance coverage will be adequate or sufficient to protect us from or to mitigate liabilities arising out of our privacy and security practices, that such coverage will continue to be available on commercially reasonable terms or at all, or that such coverage will pay future claims.
We are subject to stringent and changing laws, regulations and standards, and contractual obligations relating to privacy, data protection, and data security. The actual or perceived failure to comply with such obligations could lead to government enforcement actions (which could include civil or criminal penalties), fines and sanctions, private litigation and/or adverse publicity and could negatively affect our operating results and business.
We, and third parties who we work with are or may become subject to numerous domestic and foreign laws, regulations, and standards relating to privacy, data protection, and data security, the scope of which is changing, subject to differing applications and interpretations, and may be inconsistent among countries, or conflict with other rules. We are or may become subject to the terms of contractual obligations related to privacy, data protection, and data security. Our obligations may also change or expand as our business grows. The actual or perceived failure by us or third parties related to us to comply with such laws, regulations and obligations could increase our compliance and operational costs, expose us to regulatory scrutiny, actions, fines and penalties, result in reputational harm, lead to a loss of customers, result in litigation and liability, and otherwise cause a material adverse effect on our business, financial condition, and results of operations. See the section titled “Business— Government Regulation—Data Privacy and Security” for a more detailed description of the laws that may affect our ability to operate.
If we fail to comply with environmental, health and safety laws and regulations, we could become subject to fines or penalties or incur costs that could have a material adverse effect on the success of our business.
We are subject to numerous environmental, health and safety laws and regulations, including those governing laboratory procedures and the handling, use, storage, treatment and disposal of hazardous materials and wastes. Our operations may involve the use of hazardous and flammable materials, including chemicals and biological and radioactive materials. In addition, we may incur substantial costs in order to comply with current or future environmental, health and safety laws and regulations. These current or future laws and regulations may impair our research, development or commercialization efforts. Failure to comply with these laws and regulations also may result in substantial fines, penalties or other sanctions.
We may be subject to adverse legislative or regulatory tax changes that could negatively impact our financial condition.
The rules dealing with U.S. federal, state and local income taxation are constantly under review by persons involved in the legislative process and by the Internal Revenue Service and the U.S. Treasury Department. Changes to tax laws (which changes may have retroactive application) could adversely affect our stockholders or us. We assess the impact of various tax reform proposals and modifications to existing tax treaties in all jurisdictions where we have operations to determine the potential effect on our business and any assumptions we have made about our future taxable income. We cannot predict whether any specific proposals will be enacted, the terms of any such proposals or what effect, if any, such proposals would have on our business if they were to be enacted. For example, the United States enacted the Inflation Reduction Act of 2022, which implements, among other changes, a 1% excise tax on certain stock buybacks. In addition, beginning in 2022, the Tax Cuts and Jobs Act eliminated the previously available option to deduct research and development expenditures and requires taxpayers to amortize them generally over five years for research activities conducted in the United States and over 15 years for research activities conducted outside the United States.
101
The U.S. Congress is considering legislation that would restore the current deductibility of research and development expenditures; however, we have no assurance that the provision will be repealed or otherwise modified. Such changes, among others, may adversely affect our effective tax rate, results of operation and general business condition.
We may acquire businesses or products, or form strategic alliances, in the future, and may not realize the benefits of such acquisitions.
We may acquire additional businesses or products, form strategic alliances, or create joint ventures with third parties that we believe will complement or augment our existing business. If we acquire businesses with promising markets or technologies, we may not be able to realize the benefit of acquiring such businesses if we are unable to successfully integrate them with our existing operations and company culture. We may encounter numerous difficulties in developing, manufacturing and marketing any new programs or products resulting from a strategic alliance or acquisition that delay or prevent us from realizing their expected benefits or enhancing our business. There is no assurance that, following any such acquisition, we will achieve the synergies expected in order to justify the transaction, which could result in a material adverse effect on our business and prospects.
We maintain our cash at financial institutions, often in balances that exceed federally-insured limits. The failure of financial institutions could adversely affect our ability to pay our operational expenses or make other payments.
Our cash held in non-interest-bearing and interest-bearing accounts exceeds the Federal Deposit Insurance Corporation (“FDIC”) insurance limits. If such banking institutions were to fail, we could lose all or a portion of those amounts held in excess of such insurance limitations. For example, the FDIC took control of Silicon Valley Bank on March 10, 2023. The Federal Reserve subsequently announced that account holders would be made whole. However, the FDIC may not make all account holders whole in the event of future bank failures. In addition, even if account holders are ultimately made whole with respect to a future bank failure, account holders’ access to their accounts and assets held in their accounts may be substantially delayed. Any material loss that we may experience in the future or inability for a material time period to access our cash and cash equivalents could have an adverse effect on our ability to pay our operational expenses or make other payments, which could adversely affect our business.
Risks Related to Intellectual Property
Our ability to protect our patents and other proprietary rights is uncertain, exposing us to the possible loss of competitive advantage.
We rely upon a combination of patents, trademarks, trade secret protection and confidentiality agreements to protect the intellectual property related to our programs and technologies and to prevent third parties from competing with us. Our success depends in large part on our ability to obtain and maintain patent protection for our platform technologies, programs and their uses, as well as our ability to operate without infringing on or violating the proprietary rights of others. We own and have licensed rights to pending patent applications and expect to continue to file patent applications in the United States and abroad related to our novel discoveries and technologies that are important to our business.
However, we may not be able to protect our intellectual property rights throughout the world and the legal systems in certain countries may not favor enforcement or protection of patents, trade secrets and other intellectual property. Filing, prosecuting and defending patents on programs worldwide would be prohibitively expensive and our intellectual property rights in some foreign jurisdictions can be less extensive than those in the United States. As such, we may not have patents in all countries or all major markets and may not be able to obtain patents in all jurisdictions even if we apply for them. Our competitors may operate in countries where we do not have patent protection and can freely use our technologies and discoveries in such countries to the extent such technologies and discoveries are publicly known or disclosed in countries where we do have patent protection or pending patent applications.
Our intellectual property portfolio is at an early stage and we do not currently own or in-license any issued patents. Our pending and future patent applications may not result in patents being issued. Any issued patents may not afford sufficient protection of our programs or their intended uses against competitors, nor can there be any assurance that the patents issued will not be infringed, designed around, invalidated by third parties, or effectively prevent others from commercializing competitive technologies, products or programs.
102
Even if these patents are granted, they may be difficult to enforce. Further, any issued patents that we may license or own covering our programs could be narrowed or found invalid or unenforceable if challenged in court or before administrative bodies in the United States or abroad, including the United States Patent and Trademark Office (“USPTO”). Further, if we encounter delays in our clinical trials or delays in obtaining regulatory approval, the period of time during which we could market our programs under patent protection would be reduced. Thus, the patents that we own and license may not afford us any meaningful competitive advantage.
In addition to seeking patents for some of our technology and programs, we may also rely on trade secrets, including unpatented know-how, technology and other proprietary information, to maintain our competitive position. Any disclosure, either intentional or unintentional, by our employees, the employees of third parties with whom we share our facilities or third-party consultants and vendors that we engage to perform research, clinical trials or manufacturing activities, or misappropriation by third parties (such as through a cybersecurity breach) of our trade secrets or proprietary information could enable competitors to duplicate or surpass our technological achievements, thus eroding our competitive position in our market. In order to protect our proprietary technology and processes, we rely in part on confidentiality agreements with our collaborators, employees, consultants, outside scientific collaborators and sponsored researchers and other advisors.
These agreements may not effectively prevent disclosure of confidential information and may not provide an adequate remedy in the event of unauthorized disclosure of confidential information. We may need to share our proprietary information, including trade secrets, with future business partners, collaborators, contractors and others located in countries at heightened risk of theft of trade secrets, including through direct intrusion by private parties or foreign actors and those affiliated with or controlled by state actors. In addition, while we undertake efforts to protect our trade secrets and other confidential information from disclosure, others may independently discover trade secrets and proprietary information, and in such cases, we may not be able to assert any trade secret rights against such party. Costly and time-consuming litigation could be necessary to enforce and determine the scope of our proprietary rights and failure to obtain or maintain trade secret protection could adversely affect our competitive business position.
Lastly, if our trademarks and trade names are not registered or adequately protected, then we may not be able to build name recognition in our markets of interest and our business may be adversely affected.
We may not be successful in obtaining or maintaining necessary rights to our programs through acquisitions and in-licenses.
Because our development programs currently do and may in the future require the use of proprietary rights held by third parties, the growth of our business may depend in part on our ability to acquire, in-license, or use these third-party proprietary rights. We may be unable to acquire or in-license any compositions, methods of use, processes or other third-party intellectual property rights from third parties that we identify as necessary for our programs. The licensing and acquisition of third-party intellectual property rights is a competitive area, and a number of more established companies may pursue strategies to license or acquire third-party intellectual property rights that we may consider attractive or necessary. These established companies may have a competitive advantage over us due to their size, capital resources and greater clinical development and commercialization capabilities. In addition, companies that perceive us to be a competitor may be unwilling to assign or license rights to us. We also may be unable to license or acquire third-party intellectual property rights on terms that would allow us to make an appropriate return on our investment or at all. If we are unable to successfully obtain rights to required third-party intellectual property rights or maintain the existing intellectual property rights we have, we may have to abandon development of the relevant program, which could have a material adverse effect on our business, financial condition, results of operations, and prospects.
While we normally seek to obtain the right to control prosecution, maintenance and enforcement of the patents relating to our programs, there may be times when the filing and prosecution activities for patents and patent applications relating to our programs are controlled by our future licensors or collaboration partners. If any of our future licensors or collaboration partners fail to prosecute, maintain and enforce such patents and patent applications in a manner consistent with the best interests of our business, including by payment of all applicable fees for patents covering our programs, we could lose our rights to the intellectual property or our exclusivity with respect to those rights, our ability to develop and commercialize those programs may be adversely affected and we may not be able to prevent competitors from making, using and selling competing products.
103
In addition, even where we have the right to control patent prosecution of patents and patent applications we have licensed to and from third parties, we may still be adversely affected or prejudiced by actions or inactions of our licensees, our future licensors and their counsel that took place prior to the date upon which we assumed control over patent prosecution.
Our future licensors may rely on third-party consultants or collaborators or on funds from third parties such that our future licensors are not the sole and exclusive owners of the patents we in-license. If other third parties have ownership rights to our future in-licensed patents, they may be able to license such patents to our competitors, and our competitors could market competing products and technology. This could have a material adverse effect on our competitive position, business, financial conditions, results of operations, and prospects.
It is possible that we may be unable to obtain licenses at a reasonable cost or on reasonable terms, if at all. Even if we are able to obtain a license, it may be non-exclusive, thereby giving our competitors access to the same technologies licensed to us. In that event, we may be required to expend significant time and resources to redesign our technology, programs, or the methods for manufacturing them or to develop or license replacement technology, all of which may not be feasible on a technical or commercial basis. If we are unable to do so, we may be unable to develop or commercialize the affected programs, which could harm our business, financial condition, results of operations, and prospects significantly. We cannot provide any assurances that third-party patents do not exist which might be enforced against our current technology, manufacturing methods, programs, or future methods or products resulting in either an injunction prohibiting our manufacture or future sales, or, with respect to our future sales, an obligation on our part to pay royalties and/or other forms of compensation to third parties, which could be significant.
Disputes may arise between us and our future licensors regarding intellectual property subject to a license agreement, including: the scope of rights granted under the license agreement and other interpretation-related issues; whether and the extent to which our technology and processes infringe on intellectual property of the licensor that is not subject to the licensing agreement; our right to sublicense patents and other rights to third parties; our right to transfer or assign the license; the inventorship and ownership of inventions and know-how resulting from the joint creation or use of intellectual property by our future licensors and us and our partners; and the priority of invention of patented technology.
We may be subject to patent infringement claims or may need to file claims to protect our intellectual property, which could result in substantial costs and liability and prevent us from commercializing our potential products.
Because the intellectual property landscape in the biotechnology industry is rapidly evolving and interdisciplinary, it is difficult to conclusively assess our freedom to operate and guarantee that we can operate without infringing on or violating third party rights. If certain of our programs are ultimately granted regulatory approval, patent rights held by third parties, if found to be valid and enforceable, could be alleged to render one or more of our programs infringing. If a third party successfully brings a claim against us, we may be required to pay substantial damages, be forced to abandon any affected program and/or seek a license from the patent holder. In addition, any intellectual property claims (e.g. patent infringement or trade secret theft) brought against us, whether or not successful, may cause us to incur significant legal expenses and divert the attention of our management and key personnel from other business concerns. We cannot be certain that patents owned or licensed by us will not be challenged by others in the course of litigation. Some of our competitors may be able to sustain the costs of complex intellectual property litigation more effectively than we can because they have substantially greater resources. In addition, any uncertainties resulting from the initiation and continuation of any litigation could have a material adverse effect on our ability to raise funds and on the market price of our common stock.
Competitors may infringe or otherwise violate our patents, trademarks, copyrights or other intellectual property. To counter infringement or other violations, we may be required to file claims, which can be expensive and time-consuming. Any such claims could provoke these parties to assert counterclaims against us, including claims alleging that we infringe their patents or other intellectual property rights. In addition, in a patent infringement proceeding, a court or administrative body may decide that one or more of the patents we assert is invalid or unenforceable, in whole or in part, construe the patent’s claims narrowly or refuse to prevent the other party from using the technology at issue on the grounds that our patents do not cover the technology. Similarly, if we assert trademark infringement claims, a court or administrative body may determine that the marks we have asserted are invalid or unenforceable or that the party against whom we have asserted trademark infringement has superior rights to the marks in question.
104
In such a case, we could ultimately be forced to cease use of such marks. In any intellectual property litigation, even if we are successful, any award of monetary damages or other remedy we receive may not be commercially valuable.
Further, we may be required to protect our patents through procedures created to attack the validity of a patent at the USPTO. An adverse determination in any such submission or proceeding could reduce the scope or enforceability of, or invalidate, our patent rights, which could adversely affect our competitive position. Because of a lower evidentiary standard in USPTO proceedings compared to the evidentiary standard in United States federal courts necessary to invalidate a patent claim, a third party could potentially provide evidence in a USPTO proceeding sufficient for the USPTO to hold a claim invalid even though the same evidence would be insufficient to invalidate the claim if first presented in a district court action.
In addition, if our programs are found to infringe the intellectual property rights of third parties, these third parties may assert infringement claims against our future licensees and other parties with whom we have business relationships and we may be required to indemnify those parties for any damages they suffer as a result of these claims, which may require us to initiate or defend protracted and costly litigation on behalf of licensees and other parties regardless of the merits of such claims. If any of these claims succeed, we may be forced to pay damages on behalf of those parties or may be required to obtain licenses for the products they use.
Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation or other legal proceedings relating to our intellectual property rights, there is a risk that some of our confidential information could be compromised by disclosure during this type of litigation or other proceedings.
We may be subject to claims that we have wrongfully hired an employee from a competitor or that our employees, consultants or independent contractors have wrongfully used or disclosed confidential information of third parties.
As is common in the biotechnology industry, in addition to our employees, we engage the services of consultants to assist us in the development of our programs. Many of these consultants, and many of our employees, were previously employed at, or may have previously provided or may be currently providing consulting services to, other biotechnology or pharmaceutical companies including our competitors or potential competitors. We could in the future be subject to claims that we or our employees have inadvertently or otherwise used or disclosed alleged trade secrets or other confidential information of former employers or competitors. Although we try to ensure that our employees and consultants do not use the intellectual property, proprietary information, know-how or trade secrets of others in their work for us, we may become subject to claims that we caused an employee to breach the terms of his or her non-competition or non-solicitation agreement, or that we or these individuals have, inadvertently or otherwise, used or disclosed the alleged trade secrets or other proprietary information of a former employer or competitor.
While we may litigate to defend ourselves against these claims, even if we are successful, litigation could result in substantial costs and could be a distraction to management. If our defenses to these claims fail, in addition to requiring us to pay monetary damages, a court could prohibit us from using technologies or features that are essential to our programs, if such technologies or features are found to incorporate or be derived from the trade secrets or other proprietary information of the former employers. Moreover, any such litigation or the threat thereof may adversely affect our reputation, our ability to form strategic alliances or sublicense our rights to collaborators, engage with scientific advisors or hire employees or consultants, each of which would have an adverse effect on our business, results of operations and financial condition. Even if we are successful in defending against such claims, litigation could result in substantial costs and be a distraction to management.
Changes to patent laws in the United States and other jurisdictions could diminish the value of patents in general, thereby impairing our ability to protect our products.
Changes in either the patent laws or interpretation of patent laws in the United States, including patent reform legislation such as the Leahy-Smith America Invents Act (the “Leahy-Smith Act”) could increase the uncertainties and costs surrounding the prosecution of our owned and in-licensed patent applications and the maintenance, enforcement or defense of our owned and in-licensed issued patents.
105
The Leahy-Smith Act includes a number of significant changes to United States patent law. These changes include provisions that affect the way patent applications are prosecuted, redefine prior art, provide more efficient and cost-effective avenues for competitors to challenge the validity of patents, and enable third-party submission of prior art to the USPTO during patent prosecution and additional procedures to attack the validity of a patent at USPTO-administered post-grant proceedings, including post-grant review, inter partes review, and derivation proceedings. Assuming that other requirements for patentability are met, prior to March 2013, in the United States, the first to invent the claimed invention was entitled to the patent, while outside the United States, the first to file a patent application was entitled to the patent. After March 2013, under the Leahy-Smith Act, the United States transitioned to a first-to-file system in which, assuming that the other statutory requirements for patentability are met, the first inventor to file a patent application will be entitled to the patent on an invention regardless of whether a third party was the first to invent the claimed invention. As such, the Leahy-Smith Act and its implementation could increase the uncertainties and costs surrounding the prosecution of our patent applications and the enforcement or defense of our issued patents, all of which could have a material adverse effect on our business, financial condition, results of operations and prospects.
In addition, the patent positions of companies in the development and commercialization of biologics and pharmaceuticals are particularly uncertain. U.S. Supreme Court and U.S. Court of Appeals for the Federal Circuit rulings have narrowed the scope of patent protection available in certain circumstances and weakened the rights of patent owners in certain situations, including in the antibody arts. For example, the United States Supreme Court in Amgen, Inc. v. Sanofi (Amgen) recently held that Amgen’s patent claims to a class of antibodies functionally defined by their ability to bind a particular antigen were invalid for lack of enablement where the patent specification provided twenty-six exemplary antibodies, but the claimed class of antibodies covered a “vast number” of additional antibodies not disclosed in the specification. The Court stated that if patent claims are directed to an entire class of compositions of matter, then the patent specification must enable a person skilled in the art to make and use the entire class of compositions. This decision makes it unlikely that we will be granted U.S. patents with composition of matter claims directed to antibodies functionally defined by their ability to bind a particular antigen. Even if we are granted claims directed to functionally defined antibodies, it is possible that a third party may challenge our patents, when issued, relying on the reasoning in Amgen or other recent precedential court decisions. Additionally, there have been proposals for additional changes to the patent laws of the United States and other countries that, if adopted, could impact our ability to enforce our proprietary technology. Depending on future actions by the Congress, the United States courts, the USPTO and the relevant law-making bodies in other countries, the laws and regulations governing patents could change in ways that could have a material adverse effect on our patent rights and weaken our ability to protect, defend and enforce our patent rights in the future.
Geopolitical actions in the United States and in foreign countries could increase the uncertainties and costs surrounding the prosecution or maintenance of patent applications and the maintenance, enforcement or defense of issued patents. For example, the United States and foreign government actions related to Russia’s invasion of Ukraine may limit or prevent filing, prosecution and maintenance of patent applications in Russia. Government actions may also prevent maintenance of issued patents in Russia. These actions could result in abandonment or lapse of patents or patent applications, resulting in partial or complete loss of patent rights in Russia. If such an event were to occur, it could have a material adverse effect on our business. In addition, a decree was adopted by the Russian government in March 2022, allowing Russian companies and individuals to exploit inventions owned by patentees that have citizenship or nationality in, are registered in, or have predominately primary place of business or profit-making activities in the United States and other countries that Russia has deemed unfriendly without consent or compensation. Consequently, we would not be able to prevent third parties from practicing our inventions in Russia or from selling or importing products made using our inventions in and into Russia. Accordingly, our competitive position may be impaired, and our business, financial condition, results of operations and prospects may be adversely affected.
In addition, a European Unified Patent Court (“UPC”) entered into force on June 1, 2023. The UPC is a common patent court to hear patent infringement and revocation proceedings effective for member states of the European Union. This enables third parties to seek revocation of a European patent in a single proceeding at the UPC rather than through multiple proceedings in each of the jurisdictions in which the European patent is validated. Although we do not currently own any European patents or applications, if we obtain such patents and applications in the future, any such revocation and loss of patent protection could have a material adverse impact on our business and our ability to commercialize or license our technology and products. Moreover, the controlling laws and regulations of the UPC will develop over time, and may adversely affect our ability to enforce or defend the validity of any European patents we may obtain. We may decide to opt out from the UPC any future European patent applications that we may file and any patents we may obtain.
106
If certain formalities and requirements are not met, however, such European patents and patent applications could be challenged for non-compliance and brought under the jurisdiction of the UPC. We cannot be certain that future European patents and patent applications will avoid falling under the jurisdiction of the UPC, if we decide to opt out of the UPC.
Obtaining and maintaining patent protection depends on compliance with various procedural, document submissions, fee payment and other requirements imposed by governmental patent agencies, and our patent protection could be reduced or eliminated for non-compliance with these requirements.
Periodic maintenance fees, renewal fees, annuities fees and various other governmental fees on patents and/or patent applications are due to be paid to the USPTO and foreign patent agencies in several stages over the lifetime of the patent and/or patent application. The USPTO and various foreign governmental patent agencies also require compliance with a number of procedural, documentary, fee payment and other similar provisions during the patent application process. While an inadvertent lapse can in many cases be cured by payment of a late fee or by other means in accordance with the applicable rules, there are situations in which noncompliance can result in abandonment or lapse of the patent or patent application, resulting in partial or complete loss of patent rights in the relevant jurisdiction. Non-compliance events that could result in abandonment or lapse of a patent or patent application include, but are not limited to, failure to respond to official actions within prescribed time limits, non-payment of fees and failure to properly legalize and submit formal documents. If we fail to maintain the patents and patent applications covering our programs, our competitive position would be adversely affected.
We may not identify relevant third-party patents or may incorrectly interpret the relevance, scope or expiration of a third-party patent, which might adversely affect our ability to develop and market our products.
We cannot guarantee that any of our patent searches or analyses, including the identification of relevant patents, the scope of patent claims or the expiration of relevant patents, are complete or thorough, nor can we be certain that we have identified each and every third-party patent and pending application in the United States and abroad that is relevant to or necessary for the commercialization of our programs in any jurisdiction. The scope of a patent claim is determined by an interpretation of the law, the written disclosure in a patent and the patent’s prosecution history. Our interpretation of the relevance or the scope of a patent or a pending application may be incorrect. For example, we may incorrectly determine that our products are not covered by a third-party patent or may incorrectly predict whether a third-party’s pending application will issue with claims of relevant scope. Our determination of the expiration date of any patent in the United States or abroad that we consider relevant may be incorrect. Our failure to identify and correctly interpret relevant patents may negatively impact our ability to develop and market our products.
In addition, because some patent applications in the United States may be maintained in secrecy until the patents are issued, patent applications in the United States and many foreign jurisdictions are typically not published until 18 months after filing, and publications in the scientific literature often lag behind actual discoveries, we cannot be certain that others have not filed patent applications for technology covered by our issued patents or our pending applications, or that we were the first to invent the technology. Our competitors may have filed, and may in the future file, patent applications covering our products or technology similar to ours. Any such patent application may have priority over our patent applications or patents, which could require us to obtain rights to issued patents covering such technologies.
We may become subject to claims challenging the inventorship or ownership of our patents and other intellectual property.
We may be subject to claims that former employees, collaborators or other third parties have an interest in our patents or other intellectual property as an inventor or co-inventor. The failure to name the proper inventors on a patent application can result in the patents issuing thereon being unenforceable. Inventorship disputes may arise from conflicting views regarding the contributions of different individuals named as inventors, the effects of foreign laws where foreign nationals are involved in the development of the subject matter of the patent, conflicting obligations of third parties involved in developing our programs or as a result of questions regarding co-ownership of potential joint inventions.
107
Litigation may be necessary to resolve these and other claims challenging inventorship and/or ownership. Alternatively, or additionally, we may enter into agreements to clarify the scope of our rights in such intellectual property. If we fail in defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights, such as exclusive ownership of, or right to use, valuable intellectual property. Such an outcome could have a material adverse effect on our business. Even if we are successful in defending against such claims, litigation could result in substantial costs and be a distraction to management and other employees.
Our current or future licensors may have relied on third-party consultants or collaborators or on funds from third parties, such as the U.S. government, such that our licensors are not the sole and exclusive owners of the patents we in-licensed. If other third parties have ownership rights or other rights to our in-licensed patents, they may be able to license such patents to our competitors, and our competitors could market competing products and technology. This could have a material adverse effect on our competitive position, business, financial conditions, results of operations, and prospects.
Patent terms may be inadequate to protect our competitive position on our programs for an adequate amount of time.
Patents have a limited lifespan. In the United States, if all maintenance fees are timely paid, the natural expiration of a patent is generally 20 years from its earliest U.S. non-provisional filing date. Various extensions may be available, but the life of a patent, and the protection it affords, is limited. Even if patents covering our programs are obtained, once the patent life has expired, we may be open to competition from competitive products, including generics or biosimilars. Given the amount of time required for the development, testing and regulatory review of new programs, patents protecting such programs might expire before or shortly after such programs are commercialized. As a result, our owned and licensed patent portfolio may not provide us with sufficient rights to exclude others from commercializing products similar or identical to ours.
Our technology licensed from various third parties may be subject to retained rights.
Our future licensors may retain certain rights under the relevant agreements with us, including the right to use the underlying technology for noncommercial academic and research use, to publish general scientific findings from research related to the technology, and to make customary scientific and scholarly disclosures of information relating to the technology. It is difficult to monitor whether our licensors limit their use of the technology to these uses, and we could incur substantial expenses to enforce our rights to our licensed technology in the event of misuse.
Risks Related to Government Regulation
The regulatory approval processes of the FDA and other comparable foreign regulatory authorities are lengthy, time-consuming and inherently unpredictable. If we are not able to obtain, or if there are delays in obtaining, required regulatory approvals for our programs, we will not be able to commercialize, or will be delayed in commercializing, our programs, and our ability to generate revenue will be materially impaired.
The process of obtaining regulatory approvals, both in the United States and abroad, is unpredictable, expensive and typically takes many years following commencement of clinical trials, if approval is obtained at all, and can vary substantially based upon a variety of factors, including the type, complexity and novelty of the programs involved. We cannot commercialize programs in the United States without first obtaining regulatory approval from the FDA. Similarly, we cannot commercialize programs outside of the United States without obtaining regulatory approval from comparable foreign regulatory authorities. Before obtaining regulatory approvals for the commercial sale of our programs, including our most advanced programs, APG777 and APG808, we must demonstrate through lengthy, complex and expensive preclinical studies and clinical trials that our programs are both safe and effective for each targeted indication. Securing regulatory approval also requires the submission of information about the drug manufacturing process to, and inspection of manufacturing facilities by, the relevant regulatory authority. Further, our programs may not be effective, may be only moderately effective or may prove to have undesirable or unintended side effects, toxicities or other characteristics that may preclude our obtaining marketing approval. The FDA and comparable foreign regulatory authorities have substantial discretion in the approval process and may refuse to accept any application or may decide that our data are insufficient for approval and require additional preclinical, clinical or other data.
108
Our programs could be delayed in receiving, or fail to receive, regulatory approval for many reasons, including: the FDA or comparable foreign regulatory authorities may disagree with the design or implementation of our clinical trials; we may be unable to demonstrate to the satisfaction of the FDA or comparable foreign regulatory authorities that a program is safe and effective for its proposed indication; the results of clinical trials may not meet the level of statistical significance required by the FDA or comparable foreign regulatory authorities for approval; serious and unexpected drug-related side effects may be experienced by participants in our clinical trials or by individuals using drugs similar to our programs; we may be unable to demonstrate that a program’s clinical and other benefits outweigh its safety risks; the FDA or comparable foreign regulatory authorities may disagree with our interpretation of data from preclinical studies or clinical trials; the data collected from clinical trials of our programs may not be acceptable or sufficient to support the submission of an NDA or other submission or to obtain regulatory approval in the United States or elsewhere, and we may be required to conduct additional clinical trials; the FDA or the applicable foreign regulatory authority may disagree regarding the formulation, labeling and/or the specifications of our programs; the FDA or comparable foreign regulatory authorities may fail to approve the manufacturing processes or facilities of third-party manufacturers with which we contract for clinical and commercial supplies; and the approval policies or regulations of the FDA or comparable foreign regulatory authorities may significantly change in a manner rendering our clinical data insufficient for approval.
Of the large number of drugs in development, only a small percentage successfully complete the FDA or foreign regulatory approval processes and are commercialized. The lengthy approval process as well as the unpredictability of future clinical trial results may result in our failing to obtain regulatory approval to market our programs, which would significantly harm our business, results of operations and prospects.
If we were to obtain approval, regulatory authorities may approve any of our programs for fewer or more limited indications than we request, including failing to approve the most commercially promising indications, may grant approval contingent on the performance of costly post-marketing clinical trials, or may approve a program with a label that does not include the labeling claims necessary or desirable for the successful commercialization of that program. If we are not able to obtain, or if there are delays in obtaining, required regulatory approvals for our programs, we will not be able to commercialize, or will be delayed in commercializing, our programs and our ability to generate revenue will be materially impaired.
We may not be able to meet requirements for the chemistry, manufacturing and control of our programs.
In order to receive approval of our products by the FDA and comparable foreign regulatory authorities, we must show that we and our contract manufacturing partners are able to characterize, control and manufacture our drug products safely and in accordance with regulatory requirements. This includes manufacturing the active ingredient, developing an acceptable formulation, performing tests to adequately characterize the product, documenting a repeatable manufacturing process, meeting facility, process and testing validation requirements, and demonstrating that our drug products meet standards for parenteral administration as well as stability requirements. Meeting these chemistry, manufacturing and control requirements is a complex task that requires specialized expertise. If we are not able to meet the chemistry, manufacturing and control requirements, we may not be successful in getting our products approved.
Our programs for which we intend to seek approval as biologics may face competition sooner than anticipated.
The Patient Protection and Affordable Care Act, as amended by the Healthcare and Education Reconciliation Act, includes a subtitle called the Biologics Price Competition and Innovation Act of 2009 (“BPCIA”), which created an abbreviated approval pathway for biological products that are biosimilar to or interchangeable with an FDA-licensed reference biological product. Under the BPCIA, an application for a highly similar or “biosimilar” product may not be submitted to the FDA until four years following the date that the reference product was first approved by the FDA. In addition, the approval of a biosimilar product may not be made effective by the FDA until 12 years from the date on which the reference product was first approved. During this 12-year period of exclusivity, another company may still market a competing version of the reference product if the FDA approves a full BLA for the competing product containing the sponsor’s own preclinical data and data from adequate and well-controlled clinical trials to demonstrate the safety, purity and potency of their product.
We believe that any of our programs approved as biologics under a BLA should qualify for the 12-year period of exclusivity. However, there is a risk that this exclusivity could be shortened due to congressional action or otherwise, or that the FDA will not consider our programs to be reference products for competing products, potentially creating the opportunity for competition sooner than anticipated.
109
Other aspects of the BPCIA, some of which may impact the BPCIA exclusivity provisions, have also been the subject of recent litigation. Moreover, the extent to which a biosimilar, once approved, will be substituted for any reference products in a way that is similar to traditional generic substitution for non-biological products is not yet clear, and will depend on a number of marketplace and regulatory factors that are still developing.
Even if we receive regulatory approval of our programs, we will be subject to extensive ongoing regulatory obligations and continued regulatory review, which may result in significant additional expense and we may be subject to penalties if we fail to comply with regulatory requirements or experience unanticipated problems with our programs.
Any regulatory approvals that we may receive for our programs will require the submission of reports to regulatory authorities and surveillance to monitor the safety and efficacy of the program, may contain significant limitations related to use restrictions for specified age groups, warnings, precautions or contraindications, and may include burdensome post-approval study or risk management requirements. For example, the FDA may require a risk evaluation and mitigation strategy (“REMS”) in order to approve our programs, which could entail requirements for a medication guide, physician training and communication plans or additional elements to ensure safe use, such as restricted distribution methods, patient registries and other risk minimization tools. In addition, if the FDA or comparable foreign regulatory authorities approve our programs, our programs and the activities associated with their development and commercialization, including their design, testing, manufacture, safety, efficacy, recordkeeping, labeling, storage, approval, advertising, promotion, sale, distribution, import and export will be subject to comprehensive regulation by the FDA and other regulatory agencies in the United States and by comparable foreign regulatory authorities. These requirements include submissions of safety and other post-marketing information and reports, registration, as well as on-going compliance with current cGMPs and GCPs for any clinical trials that we conduct following approval. In addition, manufacturers of drug products and their facilities are subject to continual review and periodic, unannounced inspections by the FDA and other regulatory authorities for compliance with cGMPs.
If we or a regulatory authority discover previously unknown problems with a product, such as adverse events of unanticipated severity or frequency, or problems with the facilities where the product is manufactured, a regulatory authority may impose restrictions on that product, the manufacturing facility or us, including requiring recall or withdrawal of the product from the market or suspension of manufacturing, restrictions on our ability to conduct clinical trials, including full or partial clinical holds on ongoing or planned trials, restrictions on the manufacturing process, warning or untitled letters, civil and criminal penalties, injunctions, product seizures, detentions or import bans, voluntary or mandatory publicity requirements and imposition of restrictions on operations, including costly new manufacturing requirements. The occurrence of any event or penalty described above may inhibit our ability to commercialize our programs and generate revenue and could require us to expend significant time and resources in response and could generate negative publicity.
We may face difficulties from healthcare legislative reform measures.
Existing regulatory policies may change, and additional government regulations may be enacted that could prevent, limit or delay regulatory approval of our programs. We cannot predict the likelihood, nature or extent of government regulation that may arise from future legislation or administrative action, either in the United States or abroad. If we are slow or unable to adapt to changes in existing requirements or the adoption of new requirements or policies, or if we are not able to maintain regulatory compliance, we may lose any marketing approval that we may have obtained and we may not achieve or sustain profitability. See the section titled “Business—Government Regulation—Healthcare Reform” for a more detailed description of healthcare reforms measures that may prevent us from being able to generate revenue, attain profitability, or commercialize our programs.
110
Our business operations and current and future arrangements with investigators, healthcare professionals, consultants, third-party payors, patient organizations and customers will be subject to applicable healthcare regulatory laws, which could expose us to penalties.
Our business operations and current and future arrangements with investigators, healthcare professionals, consultants, third-party payors, patient organizations and customers may expose us to broadly applicable fraud and abuse and other healthcare laws and regulations. These laws may constrain the business or financial arrangements and relationships through which we conduct our operations, including how we research, market, sell and distribute our programs, if approved. See the section titled “Business—Government Regulation— Other Healthcare Laws and Compliance Requirements” for a more detailed description of the laws that may affect our ability to operate.
Ensuring that our internal operations and future business arrangements with third parties comply with applicable healthcare laws and regulations will involve substantial costs. If our operations are found to be in violation of any of these laws or any other governmental laws and regulations that may apply to us, we may be subject to significant penalties, including civil, criminal and administrative penalties, damages, fines, exclusion from government-funded healthcare programs, integrity oversight and reporting obligations to resolve allegations of non-compliance, disgorgement, individual imprisonment, contractual damages, reputational harm, diminished profits and the curtailment or restructuring of our operations. Further, defending against any such actions can be costly and time-consuming and may require significant personnel resources. Therefore, even if we are successful in defending against any such actions that may be brought against us, our business may be impaired.
Even if we are able to commercialize any programs, due to unfavorable pricing regulations and/or third-party coverage and reimbursement policies, we may not be able to offer such programs at competitive prices which would seriously harm our business.
We intend to seek approval to market our programs in both the United States and in selected foreign jurisdictions. If we obtain approval in one or more foreign jurisdictions for our programs, we will be subject to rules and regulations in those jurisdictions. Our ability to successfully commercialize any programs that we may develop will depend in part on the extent to which reimbursement for these programs and related treatments will be available from government health administration authorities, private health insurers and other organizations. Government authorities and other third-party payors, such as private health insurers and health maintenance organizations, decide which medications they will pay for and establish reimbursement levels.
Government authorities and other third-party payors have attempted to control costs by limiting coverage and the amount of reimbursement for particular medications. These entities may create preferential access policies for a competitor’s product, including a branded or generic/biosimilar product, over our products in an attempt to reduce their costs, which may reduce our commercial opportunity. Additionally, if any of our programs are approved and we are found to have improperly promoted off-label uses of those programs, we may become subject to significant liability, which would materially adversely affect our business and financial condition. See the sections titled “Business—Government Regulation—Coverage and Reimbursement” and “Business— Other Government Regulation Outside of the United States—Regulation in the European Union” for a more detailed description of the government regulations and third-party payor practices that may affect our ability to commercialize our programs.
We are subject to U.S. and certain foreign export and import controls, sanctions, embargoes, anti-corruption laws, and anti-money laundering laws and regulations. We can face criminal liability and other serious consequences for violations, which can harm our business.
We are subject to export control and import laws and regulations, including the U.S. Export Administration Regulations, U.S. Customs regulations, various economic and trade sanctions regulations administered by the U.S. Treasury Department’s Office of Foreign Assets Controls, the U.S. Foreign Corrupt Practices Act of 1977, as amended, the U.S. domestic bribery statute contained in 18 U.S.C. § 201, the U.S. Travel Act, the USA PATRIOT Act, and other state and national anti-bribery and anti-money laundering laws in the countries in which we conduct activities. Anti-corruption laws are interpreted broadly and prohibit companies and their employees, agents, contractors, and other collaborators from authorizing, promising, offering, or providing, directly or indirectly, improper payments or anything else of value to or from recipients in the public or private sector.
111
We may engage third parties to sell our products outside the United States, to conduct clinical trials, and/or to obtain necessary permits, licenses, patent registrations, and other regulatory approvals. We have direct or indirect interactions with officials and employees of government agencies or government-affiliated hospitals, universities, and other organizations. We can be held liable for the corrupt or other illegal activities of our employees, agents, contractors, and other collaborators, even if we do not explicitly authorize or have actual knowledge of such activities. Any violations of the laws and regulations described above may result in substantial civil and criminal fines and penalties, imprisonment, the loss of export or import privileges, debarment, tax reassessments, breach of contract and fraud litigation, reputational harm, and other consequences.
Governments outside the United States tend to impose strict price controls, which may adversely affect our revenue, if any.
In some countries, particularly member states of the European Union, the pricing of prescription drugs is subject to governmental control.
In these countries, pricing negotiations with governmental authorities can take considerable time after receipt of marketing approval for a therapeutic. In addition, there can be considerable pressure by governments and other stakeholders on prices and reimbursement levels, including as part of cost containment measures. Political, economic and regulatory developments may further complicate pricing negotiations, and pricing negotiations may continue after reimbursement has been obtained. Reference pricing used by various EU member states and parallel distribution, or arbitrage between low-priced and high-priced member states, can further reduce prices. To obtain coverage and reimbursement or pricing approvals in some countries, we or current or future collaborators may be required to conduct a clinical trial or other studies that compare the cost-effectiveness of our programs to other available therapies in order to obtain or maintain reimbursement or pricing approval. Publication of discounts by third-party payors or authorities may lead to further pressure on the prices or reimbursement levels within the country of publication and other countries. If reimbursement of any program approved for marketing is unavailable or limited in scope or amount, or if pricing is set at unsatisfactory levels, our business, financial condition, results of operations or prospects could be materially and adversely affected. Brexit could lead to legal uncertainty and potentially divergent national laws and regulations, including those related to the pricing of prescription pharmaceuticals, as the UK determines which EU laws to replicate or replace. If the UK were to significantly alter its regulations affecting the pricing of prescription pharmaceuticals, we could face significant new costs.
If we decide to pursue a Fast Track Designation by the FDA, it may not lead to a faster development or regulatory review or approval process.
We may seek Fast Track Designation for one or more of our programs. If a drug is intended for the treatment of a serious or life-threatening condition and the drug demonstrates the potential to address unmet medical needs for this condition, the product sponsor may apply for FDA Fast Track Designation. The FDA has broad discretion whether or not to grant this designation, so even if we believe a particular program is eligible for this designation, we cannot assure you that the FDA would decide to grant it. Even if we do receive Fast Track Designation, we may not experience a faster development process, review or approval compared to conventional FDA procedures. The FDA may withdraw Fast Track Designation if it believes that the designation is no longer supported by data from our clinical development program. See the section titled “Business—Government Regulation—Expedited Development and Review Programs” for a more detailed description of the process for seeking Fast Track Designation.
Risks Related to Our Common Stock
Our quarterly and annual operating results may fluctuate significantly or may fall below the expectations of investors or securities analysts, each of which may cause our stock price to fluctuate or decline.
We expect our operating results to be subject to quarterly fluctuations. Our net loss and other operating results will be affected by numerous factors, including the factors discussed in this “Risk Factors” section and elsewhere in this Annual Report. If our quarterly or annual operating results fall below the expectations of investors or securities analysts, the price of our common stock could decline substantially. Furthermore, any quarterly or annual fluctuations in our operating results may, in turn, cause the price of our common stock to fluctuate substantially.
112
We believe that quarterly comparisons of our financial results are not necessarily meaningful and should not be relied upon as an indication of our future performance.
The price of our stock may be volatile, and you could lose all or part of your investment.
The trading price of our common stock has fluctuated, and is likely to continue to fluctuate substantially in response to various factors, some of which are beyond our control, including the factors discussed in this “Risk Factors” section and elsewhere in this Annual Report. The realization of any of these factors could have a dramatic and adverse impact on the market price of our common stock.
In addition, the stock market in general, and the market for biotechnology and biopharmaceutical companies in particular, have historically been particularly volatile and experienced extreme price and volume fluctuations that have often been unrelated or disproportionate to the operating performance of these companies. Broad market and industry factors may negatively affect the market price of our common stock, regardless of our actual operating performance. If the market price of our common stock does not exceed the price at which you purchase your shares, you may not realize any return on your investment in us and may lose some or all of your investment. In the past, securities class action litigation has often been instituted against companies following periods of volatility in the market price of a company’s securities. This type of litigation, if instituted, could result in substantial costs and a diversion of management’s attention and resources, which would materially adversely affect our business, financial condition and results of operation.
A sale of a substantial number of shares of our common stock may cause the price of our common stock to decline.
We cannot predict what effect, if any, future sales of our shares in the public market or the availability of shares for sale will have on the market price of our common stock. However, future sales of substantial amounts of our common stock in the public market, including shares issued upon exercise of outstanding options, or the perception that such sales may occur, could adversely affect the market price of our common stock. We also expect that significant additional capital may be needed in the future to continue our planned operations. To raise capital, we may sell common stock, convertible securities, or other equity securities in one or more transactions at prices and in a manner we determine from time to time. These sales, or the perception in the market that the holders of a large number of shares intend to sell shares, could reduce the market price of our common stock.
Our principal stockholders and management own a significant percentage of our stock and will be able to exert significant influence over matters subject to stockholder approval.
Our executive officers, directors, holders of 5% or more of our capital stock and their respective affiliates beneficially own a significant percentage of our outstanding voting common stock and all of our outstanding non-voting common stock. These stockholders, acting together, may be able to impact matters requiring stockholder approval. For example, they may be able to entrench management or impact elections of directors, amendments of our organizational documents or approval of any merger, sale of assets or other major corporate transaction. This may prevent or discourage unsolicited acquisition proposals or offers for our common stock that you may feel are in your best interest as one of our stockholders. The interests of this group of stockholders may not always coincide with your interests or the interests of other stockholders and they may act in a manner that advances their best interests and not necessarily those of other stockholders, including seeking a premium value for their common stock, and might affect the prevailing market price for our common stock.
A sale of a substantial number of shares of our common stock may cause the market price of our common stock to drop significantly, even if our business is doing well.
We cannot predict what effect, if any, sales of our shares in the public market or the availability of shares for sale will have on the market price of our common stock. However, future sales of a substantial number of shares of our common stock in the public market, including shares issued upon exercise of outstanding options or other equity awards, could reduce the market price of our common stock. We also expect that significant additional capital may be needed in the future to continue our planned operations. To raise capital, we may sell common stock, convertible securities, or other equity securities in one or more transactions at prices and in a manner we determine from time to time.
113
These sales, or the perception in the market that the holders of a large number of shares intend to sell shares, could reduce the market price of our common stock.
In addition, certain holders of our shares of our common stock have rights, subject to specified conditions, to require us to file registration statements covering their shares or to include their shares in registration statements that we may file for ourselves or other stockholders. We have filed a registration statement under the Securities Act to register the shares of our common stock reserved for issuance under our equity compensation plans. These shares can be freely sold in the public market upon issuance, subject to volume limitations applicable to affiliates.
We are an “emerging growth company” and a “smaller reporting company” and the reduced disclosure requirements applicable to emerging growth companies and smaller reporting companies may make our common stock less attractive to investors.
We are an “emerging growth company” as defined in Section 2(a) of the Securities Act, as modified by the JOBS Act. As an emerging growth company, we are only required to provide two years of audited financial statements (in addition to any required unaudited interim financial statements) and correspondingly reduced management discussion and analysis of financial condition and results of operations disclosure. In addition, we are not required to obtain auditor attestation of reporting on internal control over financial reporting, we have reduced disclosure obligations regarding executive compensation and we are not required to hold non-binding advisory votes on executive compensation or obtain stockholder approval of any golden parachute payments not previously approved. We may choose to take advantage of some, but not all, of the available exemptions. We have taken advantage of reduced reporting obligations in this Annual Report. In addition, the JOBS Act provides that an emerging growth company can take advantage of an extended transition period for complying with new or revised accounting standards. These provisions allow an emerging growth company to delay the adoption of these accounting standards until they would otherwise apply to private companies. We have elected to take advantage of such extended transition period. We cannot predict whether investors will find our common stock less attractive as a result of its reliance on these exemptions. If some investors find our common stock to be less attractive as a result, there may be a less active trading market for our common stock and the price of our common stock may be more volatile than the current trading market and price of our common stock.
Further, there is no guarantee that the exemptions available under the JOBS Act will result in significant savings. To the extent that we choose not to use exemptions from various reporting requirements under the JOBS Act, we will incur additional compliance costs, which may impact our financial condition.
We will remain an emerging growth company until the earliest of: (i) the end of the fiscal year in which we have a total annual gross revenue of $1.235 billion; (ii) the last day of our fiscal year following the fifth anniversary of the closing of our IPO; (iii) the date on which we have, during the previous three-year period, issued more than $1.0 billion in non-convertible debt; or (iv) the end of the fiscal year in which the market value of common stock held by non-affiliates exceeds $700 million as of the prior June 30. Even after we no longer qualify as an emerging growth company, we may continue to qualify as a smaller reporting company, which would allow us to take advantage of many of the same exemptions from disclosure requirements, including reduced disclosure obligations regarding executive compensation. In addition, for so long as we are a smaller reporting company with less than $100 million in annual revenue, we would not be required to comply with the auditor attestation requirements of Section 404 of the Sarbanes-Oxley Act.
Provisions in our amended and restated certificate of incorporation and amended and restated bylaws and Delaware law might discourage, delay or prevent a change in control of our company or changes in our management and, therefore, depress the market price of our common stock.
Our amended and restated certificate of incorporation and amended and restated bylaws contain provisions that could delay or prevent a change of control of our company or changes in our Board that our stockholders might consider favorable. At any time while at least 6,061,821 shares of non-voting common stock remain issued and outstanding, we may not consummate a Fundamental Transaction (as defined in our amended and restated certificate of incorporation) or any merger or consolidation of the Company with or into another entity or any stock sale to, or other business combination in which the stockholders of the Company immediately before such transaction do not hold at least a majority of the capital stock of the Company immediately after such transaction, without the affirmative vote of the holders of a majority of the then outstanding shares of non-voting common stock.
114
All of the outstanding shares of non-voting common stock are held by entities affiliated with two stockholders. This provision of our amended and restated certificate of incorporation may make it more difficult for us to enter into any of the aforementioned transactions. In addition, Section 203 of the General Corporation Law of the State of Delaware (“DGCL”) prohibits a publicly-held Delaware corporation from engaging in a business combination with an interested stockholder for a period of three years after the date of the transaction in which the person became an interested stockholder, unless the business combination is approved in a prescribed manner. Any provision of our amended and restated certificate of incorporation, amended and restated bylaws or Delaware law that has the effect of delaying or preventing a change in control could limit the opportunity for our stockholders to receive a premium for their shares of our capital stock and could also affect the price that some investors are willing to pay for our common stock. See the section titled “Description of Capital Stock—Anti-Takeover Effects of Our Amended and Restated Certificate of Incorporation, Amended and Restated Bylaws and Delaware Law” for a more detailed description of these provisions.
Our amended and restated certificate of incorporation provides that the Court of Chancery of the State of Delaware and the federal district courts of the United States will be the exclusive forums for substantially all disputes between us and our stockholders, which could limit our stockholders’ ability to obtain a favorable judicial forum for disputes.
Our amended and restated certificate of incorporation provides that the Court of Chancery of the State of Delaware (or, if the Court of Chancery does not have jurisdiction, another State court in Delaware or the federal district court for the District of Delaware) is the exclusive forum for certain actions, in all cases subject to the court’s having jurisdiction over indispensable parties named as defendants. In addition, our amended and restated certificate of incorporation provides that the federal district courts of the United States will be the exclusive forum for resolving any complaint asserting a cause of action arising under the Securities Act but that the forum selection provision will not apply to claims brought to enforce a duty or liability created by the Exchange Act. These exclusive forum provisions may impose additional costs on stockholders in pursuing any such claims or limit a stockholder’s ability to bring a claim in a judicial forum that it finds favorable for disputes, which may discourage lawsuits. There is uncertainty as to whether a court would enforce such provisions. If a court were to find these types of provisions to be inapplicable or unenforceable, and if a court were to find the exclusive forum provision in our amended and restated bylaws to be inapplicable or unenforceable in an action, we may incur additional costs associated with resolving the dispute in other jurisdictions, which could materially adversely affect our business. See the section titled “Description of Capital Stock—Anti-Takeover Effects of Our Amended and Restated Certificate of Incorporation, Amended and Restated Bylaws and Delaware Law—Exclusive Forum Selection Clause” for a more detailed description of these choice of forums provisions.
Because we do not anticipate paying any dividends on our capital stock in the foreseeable future, capital appreciation, if any, will be your sole source of gain.
We have never declared or paid dividends on our capital stock. We currently intend to retain all of our future earnings, if any, to finance the growth and development, operation and expansion of our business and do not anticipate declaring or paying any dividends for the foreseeable future. As a result, capital appreciation, if any, of our common stock will be your sole source of gain for the foreseeable future.
Our estimates of market opportunity and forecasts of market growth may prove to be inaccurate, and even if the markets in which we compete achieve the forecasted growth, our business may not grow at similar rates, or at all.
Our market opportunity estimates and growth forecasts are subject to significant uncertainty and are based on assumptions and estimates which may not prove to be accurate. Our estimates and forecasts relating to size and expected growth of our target market may prove to be inaccurate. Even if the markets in which we compete meet our size estimates and growth forecasts, our business may not grow at similar rates, or at all. Our growth is subject to many factors, including our success in implementing our business strategy, which is subject to many risks and uncertainties.
Our revenue will be dependent, in part, upon the size of the markets in the territories for which we gain regulatory approval, the accepted price for the product, the ability to obtain coverage and reimbursement and whether we own the commercial rights for that territory. If the number of our addressable patients is not as significant as we estimate, the indication approved by regulatory authorities is narrower than we expect or the treatment population is narrowed by competition, physician choice or treatment guidelines, we may not generate significant revenue from sales of such products, even if approved.
115
The dual class structure of our common stock may limit your ability to influence corporate matters and may limit your visibility with respect to certain transactions.
The dual class structure of our common stock may limit your ability to influence corporate matters. Holders of our common stock are entitled to one vote per share, while holders of our non-voting common stock are not entitled to any votes. Nonetheless, each share of our non-voting common stock may be converted at any time into one share of our common stock at the option of its holder by providing written notice to us, subject to the limitations provided for in our amended and restated certificate of incorporation. Consequently, if holders of our non-voting common stock exercise their option to make this conversion, this will have the effect of increasing the relative voting power of those prior holders of our non-voting common stock, and correspondingly decreasing the voting power of the holders of our common stock, which may limit your ability to influence corporate matters. Additionally, stockholders who hold, in the aggregate, more than 10% of our common stock and non-voting common stock, but 10% or less of our common stock, and are not otherwise an insider, may not be required to report changes in their ownership due to transactions in our non-voting common stock pursuant to Section 16(a) of the Exchange Act, and may not be subject to the short-swing profit provisions of Section 16(b) of the Exchange Act.
General Risk Factors
We may become exposed to costly and damaging liability claims, either when testing our programs in the clinic or at the commercial stage, and our product liability insurance may not cover all damages from such claims.
We are exposed to potential product liability and professional indemnity risks that are inherent in the research, development, manufacturing, marketing and use of pharmaceutical products. While we currently have no products that have been approved for commercial sale, the use of our programs in clinical trials, and the sale of any approved products in the future, may expose us to liability claims. These claims may be made by patients that use the product, healthcare providers, pharmaceutical companies, or others selling such products. Any claims against us, regardless of their merit, could be difficult and costly to defend and could materially and adversely affect the market for our products or any prospects for commercialization of our products. Although we currently maintain adequate product liability insurance for our programs, it is possible that our liabilities could exceed our insurance coverage or that in the future we may not be able to maintain insurance coverage at a reasonable cost or obtain insurance coverage that will be adequate to satisfy any liability that may arise. If a successful product liability claim or series of claims is brought against us for uninsured liabilities or in excess of insured liabilities, our assets may not be sufficient to cover such claims and our business operations could be impaired.
Litigation costs and the outcome of litigation could have a material adverse effect on our business.
From time to time we may be subject to litigation claims through the ordinary course of our business operations regarding, but not limited to, securities litigation, employment matters, security of patient and employee personal information, contractual relations with collaborators and licensors and intellectual property rights. Litigation to defend ourselves against claims by third parties, or to enforce any rights that we may have against third parties, could result in substantial costs and diversion of our resources, causing a material adverse effect on our business, financial condition, results of operations or cash flows.
If securities or industry analysts do not publish research or reports, or if they publish adverse or misleading research or reports, regarding us or our business, our stock price and trading volume could decline.
The trading market for our common stock depends, in part, on the research and reports that securities or industry analysts publish about us or our business. If no or few securities or industry analysts continue coverage of us or if one or more of these analysts cease coverage of us or fail to publish reports on us regularly, our stock price could be negatively impacted. If any of the analysts who cover us issue adverse or misleading research or reports regarding us, our business model, our intellectual property, our stock performance or our market, or if our clinical trials or operating results fail to meet the expectations of analysts, our stock price would likely decline.
116
If one or more of these analysts cease to cover our stock, we could lose visibility in the market for our stock, which in turn could cause our stock price and trading volume to decline.
We will continue to incur increased costs as a result of operating as a public company, and our management will continue to be required to devote substantial time to new compliance initiatives and corporate governance practices.
As a public company, and particularly after we are no longer an “emerging growth company” or a “smaller reporting company,” we will continue to incur significant legal, accounting and other expenses that we did not incur as a private company. The Sarbanes-Oxley Act, the Dodd-Frank Wall Street Reform and Consumer Protection Act, the listing requirements of the Nasdaq Global Market and other applicable securities rules and regulations impose various requirements on public companies, including establishment and maintenance of effective disclosure and financial controls and corporate governance practices. In addition, changing laws, regulations, and standards relating to corporate governance and public disclosure, including those related to climate change and other environmental, social and governance focused disclosures, are creating uncertainty for public companies, increasing legal and financial compliance costs, and making some activities more time consuming. Our management and other personnel will continue to devote a substantial amount of time to these compliance initiatives, and we will continue to incur increased legal and financial compliance costs. For example, maintaining customary public company director and officer liability insurance requires substantial expenditures. The impact of these legal and financial requirements could make it more difficult for us to attract and retain qualified persons to serve on our Board, our Board committees or as executive officers. The increased costs may require us to reduce costs in other areas of our business or increase the prices of our programs, once commercialized. Moreover, these rules and regulations are often subject to varying interpretations, in many cases due to their lack of specificity, and, as a result, their application in practice may evolve over time as new guidance is provided by regulatory and governing bodies. This could result in continuing uncertainty regarding compliance matters and higher costs necessitated by ongoing revisions to disclosure and governance practices.
If we fail to maintain proper and effective internal controls over financial reporting our ability to produce accurate and timely financial statements could be impaired.
Pursuant to Section 404 of the Sarbanes-Oxley Act, our management will be required to report upon the effectiveness of our internal control over financial reporting beginning with annual report for our fiscal year ending December 31, 2024. When we lose our status as an “emerging growth company” and become an “accelerated filer” or a “large accelerated filer,” we will be required to have an audit of the effectiveness of our internal control over financial reporting. The rules governing the standards that must be met for management to assess our internal control over financial reporting are complex and require significant documentation, testing, and possible remediation. To achieve compliance with Section 404 within the prescribed period, we are engaged in a process to document and evaluate our internal control over financial reporting, which is both costly and challenging. In this regard, we will need to continue to dedicate internal resources, engage outside consultants and adopt a detailed work plan to assess and document the adequacy of internal control over financial reporting, continue steps to improve control processes as appropriate, validate through testing that controls are functioning as documented and implement a continuous reporting and improvement process for internal control over financial reporting. This process will be time-consuming, costly and complicated.
Any failure to maintain internal control over financial reporting could severely inhibit our ability to accurately report our financial condition, results of operations, or cash flows. If we are unable to conclude that our internal control over financial reporting is effective, or if our independent registered public accounting firm determines we have a material weakness or significant deficiency in our internal control over financial reporting, investors may lose confidence in the accuracy and completeness of our financial reports, the market price of our common stock could decline, and we could be subject to sanctions or investigations by Nasdaq, the SEC, or other regulatory authorities. Failure to remedy any material weakness in our internal control over financial reporting, or to implement or maintain other effective control systems required of public companies, could also restrict our future access to the capital markets.
117
Our disclosure controls and procedures may not prevent or detect all errors or acts of fraud.
We are subject to the periodic reporting requirements of the Exchange Act. We designed our disclosure controls and procedures to reasonably assure that information we must disclose in reports we file or submit under the Exchange Act is accumulated and communicated to management, and recorded, processed, summarized and reported within the time periods specified in the rules and forms of the SEC. We believe that any disclosure controls and procedures or internal controls and procedures, no matter how well-conceived and operated, can provide only reasonable, not absolute, assurance that the objectives of the control system are met.
These inherent limitations include the realities that judgments in decision-making can be faulty, and that breakdowns can occur because of simple error or mistake. For example, our directors or executive officers could inadvertently fail to disclose a new relationship or arrangement causing us to fail to make any related party transaction disclosures. Additionally, controls can be circumvented by the individual acts of some persons, by collusion of two or more people or by an unauthorized override of the controls. Accordingly, because of the inherent limitations in our control system, misstatements due to error or fraud may occur and not be detected. In addition, we do not have a formal risk management program for identifying and addressing risks to our business in other areas.
Our business could be adversely affected by economic downturns, inflation, increases in interest rates, natural disasters, public health crises such as the COVID-19 pandemic, political crises, geopolitical events, such as the conflict between Russia and Ukraine, and Israel and Hamas or other macroeconomic conditions, which could have a material and adverse effect on our results of operations and financial condition.
The global economy, including credit and financial markets, has experienced extreme volatility and disruptions, including, among other things, diminished liquidity and credit availability, declines in consumer confidence, declines in economic growth, supply chain shortages, increases in inflation rates, higher interest rates, and uncertainty about economic stability. For example, the COVID-19 pandemic resulted in widespread unemployment, economic slowdown and extreme volatility in the capital markets. The Federal Reserve has raised interest rates multiple times in response to concerns about inflation and it may raise them again. Higher interest rates, coupled with reduced government spending and volatility in financial markets, may increase economic uncertainty and affect consumer spending. Similarly, geopolitical uncertainties and international conflicts, including the ongoing military conflicts between Russia and Ukraine, and Israel and Hamas, and rising tensions with China, have created extreme volatility in the global capital markets and may have further global economic consequences, including disruptions of the global supply chain. Any such volatility and disruptions may adversely affect our business or the third parties on whom we rely. If the equity and credit markets deteriorate, including as a result of political unrest or war, it may make any necessary debt or equity financing more costly, more dilutive, or more difficult to obtain in a timely manner or on favorable terms, if at all. Increased inflation rates can adversely affect us by increasing our costs, including labor and employee benefit costs.
We may in the future experience disruptions as a result of such macroeconomic conditions, including delays or difficulties in initiating or expanding clinical trials and manufacturing sufficient quantities of materials. Any one or a combination of these events could have a material and adverse effect on our results of operations and financial condition.
Item 1B. Unresolved Staff Comments.
None.
Item 1C. Cybersecurity
We operate in the biotechnology sector, which is subject to various cybersecurity risks that could adversely affect our business, financial condition, and results of operations, including intellectual property theft; fraud; extortion; harm to employees or customers; violation of privacy laws and other litigation and legal risk; and reputational risk. We have implemented and utilize a risk-based approach that incorporates various information security processes designed to assess, identify and manage risks from potential unauthorized occurrences on or through our information technology systems that may result in adverse effects on the confidentiality, integrity and availability of information technology systems and the data residing therein. The critical data contained on our information systems include intellectual property, confidential information that is proprietary, strategic or competitive in nature, and sensitive, personal information that we collect, use, store and transmit digitally in the ordinary course of our business.
118
These processes are managed and monitored by a dedicated information technology team, which is led by our Senior Vice President of Information Technology, and include mechanisms, controls, technologies, systems, and other processes designed to monitor and evaluate our threat environment, prevent or mitigate data loss, theft, misuse, or other security incidents or vulnerabilities affecting the data and maintain a stable information technology environment. Our cybersecurity program is informed by certain industry standards and best practices as outlined by the National Institute of Standards and Technology (“NIST”) Cybersecurity Framework. We use various tools and methodologies to manage cybersecurity risk that are tested on a regular cadence. We use email security tools, managed detection and response, third party managed security services, regular vulnerability scans and threat intelligence feeds. We also have an incident response plan designed to mitigate and remediate identified cybersecurity incidents and escalate certain incidents as appropriate to management and the Audit Committee. We assess third-party service providers with a cyber security questionnaire and a follow up meeting or audit based upon the risk profile of the third party with access to personal, confidential or proprietary information to implement and maintain cybersecurity practices intended to be consistent with applicable legal standards and industry best practices.
Our business depends on the availability, reliability, and security of our information systems, networks, data, and intellectual property. Any disruption, compromise, or breach of our systems or data due to a cybersecurity threat or incident could adversely affect our operations, customer service, product development, and competitive position. They may also result in a breach of our contractual obligations or legal duties to protect the privacy and confidentiality of our stakeholders. Such a breach could expose us to business interruption, lost revenue, ransom payments, remediation costs, liabilities to affected parties, cybersecurity protection costs, lost assets, litigation, regulatory scrutiny and actions, reputational harm, customer dissatisfaction, harm to our vendor relationships, or loss of market share. To mitigate the aforementioned consequences of cybersecurity incidents, we carry cyber attack insurance. In the last fiscal year, we have not identified risks from known cybersecurity threats, including as a result of any prior cybersecurity incidents, that have materially affected us, but we face certain ongoing cybersecurity risks threats that, if realized, are reasonably likely to materially affect us. Additional information on cybersecurity risks we face is discussed in Part I, Item 1A, “Risk Factors,” under the heading “Our internal information technology systems, or those of any of our CROs, manufacturers, other contractors or consultants, third party service providers, or potential future collaborators, may fail or suffer security or data privacy breaches or other unauthorized or improper access to, use of, or destruction of our proprietary or confidential data, employee data or personal data, which could result in additional costs, loss of revenue, significant liabilities, harm to our brand and material disruption of our operations.”
Our Senior Vice President of Information Technology, a certified CISSP, who reports directly to the Chief Financial Officer and has over twenty years of experience managing information technology and cybersecurity, is responsible for assessing and managing cybersecurity risks. We consider cybersecurity, along with other significant risks that we face, within our overall enterprise risk management framework. The Board of Directors, as a whole and at the committee level, has oversight for the most significant risks facing us and for our processes to identify, prioritize, assess, manage, and mitigate those risks. The Audit Committee, which is comprised solely of independent directors, has been designated by our Board to oversee cybersecurity risks. The Audit Committee receives regular updates on cybersecurity and information technology matters and related risk exposures from our Senior Vice President of Information Technology. The Board also receives updates from management and the Audit Committee on cybersecurity risks on at least an annual basis.
119
Item 2.Properties.
We maintain a corporate headquarters in Waltham, Massachusetts, laboratory space in Boston, Massachusetts and otherwise operate virtually in the United States. In September 2023, we entered into a one-year lease for 1,087 square feet of office space in Waltham, Massachusetts. In November 2023, we entered into a two-year lease agreement for a 1,740 square foot laboratory facility in Boston, Massachusetts, which consists of two R&D laboratories and office space. We believe these arrangements support our current needs. If we require additional space, we believe that we will be able to obtain such space on acceptable, commercially reasonable terms.
Item 3.Legal Proceedings.
We are not party to any material legal proceedings at this time. From time to time, we may become involved in various legal proceedings that arise in the ordinary course of our business. Regardless of outcome, litigation can have an adverse impact on us due to defense and settlement costs, diversion of management resources, negative publicity, reputational harm and other factors, and there can be no assurances that favorable outcomes will be obtained.
Item 4.Mine Safety Disclosures.
Not applicable.
120
PART II
Item 5.Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer
Purchases of Equity Securities.
Market Information
Our common stock trades on the Nasdaq Global Market under the symbol “APGE.” Trading of our common stock commenced on July 14, 2023 in connection with our initial public offering. Prior to that time, there was no established public trading market for our common stock.
Holders
As of February 23, 2024, we had approximately eight holders of record of our common stock. This number does not include beneficial owners whose shares were held in street name.
Dividend Policy
We have never declared or paid any cash dividend on our capital stock. We currently intend to retain all available funds and future earnings, if any, to fund the operations and the further development and expansion of our business. We have no present intention to pay cash dividends on our common stock or non-voting common stock. Any determination to pay dividends to holders of our common stock or non-voting common stock will be at the discretion of our Board and will depend on many factors, including our financial condition, results of operations, liquidity, earnings, projected capital and other cash requirements, legal requirements, restrictions in the agreements governing any indebtedness we may enter into, our business prospects and other factors that our Board deems relevant.
Recent Sales of Unregistered Securities
None.
Use of Proceeds from the Initial Public Offering of Common Stock
On July 18, 2023, we completed our IPO in which we issued and sold an aggregate of 20,297,500 shares of our common stock, including the full exercise of the underwriters’ option to purchase up 2,647,500 additional shares of our common stock, at the IPO price of $17.00 per share.
The offer and sale of all of the shares of our common stock in the IPO were registered under the Securities Act pursuant to our Registration Statement on Form S-1, as amended (File Nos. 333-272831 and 333-273236), which was declared effective on July 13, 2023. Jefferies, TD Cowen, Stifel and Guggenheim Securities acted as joint book-running managers for the IPO. Wedbush PacGrow acted as lead manager for the IPO.
121
We received gross proceeds from our IPO of approximately $345.1 million, and net proceeds of approximately $315.4 million, after deducting underwriting discounts and commissions and other offering expenses. None of the underwriting discounts and commissions or other offering expenses were incurred or paid, directly or indirectly, to any of our directors or officers or their associates or to persons owning 10% or more of our common stock or to any of our affiliates.
The net proceeds from the IPO have been used and are expected to be used, primarily to fund our clinical trials, including a potential Phase 2 trial, and manufacturing of our APG777 product candidate, fund our preclinical studies, clinical trials and manufacturing of our APG808 program, fund our preclinical studies, clinical trials and manufacturing of our APG990 program and fund our preclinical studies of our APG222 program. We intend to use the remainder for our additional research and development activities, as well as for capital expenditures, working capital and general corporate purposes. There has been no material change in our intended use of proceeds from our IPO as described in the final prospectus for our IPO filed with the Securities and Exchange Commission (“SEC”) pursuant to Rule 424(b) under the on July 17, 2023.
Issuer Purchases of Equity Securities
None.
Item 6.Reserved.
122
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations
You should read the following discussion of our financial condition and results of operations in conjunction with the consolidated financial statements and related notes included elsewhere in this Annual Report on Form 10-K (this “Annual Report”). The following discussion contains forward-looking statements that reflect our current plans, forecasts, estimates and beliefs and involve risks and uncertainties. Our historical results are not necessarily indicative of the results that may be expected for any period in the future. Our actual results, outcomes and the timing of events could differ materially from those discussed in the forward-looking statements. Factors that could cause or contribute to these differences include those discussed below and elsewhere in this Annual Report, particularly in the sections titled “Special Note Regarding Forward-Looking Statements” and “Risk Factors”. We urge you to consider these factors carefully in evaluating the forward-looking statements contained in this Annual Report. Forward-looking statements are not historical facts, reflect our current views with respect to future events, and apply only as of the date made. We do not intend, and undertake no obligation, to update these forward-looking statements, except as required by law.
Overview
We are a clinical stage biotechnology company seeking to develop differentiated biologics for the treatment of AD, asthma, COPD, and related I&I indications with high unmet need. Our antibody programs are designed to overcome limitations of existing therapies by targeting well-established mechanisms of action and incorporating advanced antibody engineering to optimize half-life and other properties. We commenced our operations in February 2022 as a Delaware limited liability company named Apogee Therapeutics, LLC. We were founded by leading healthcare investors, Fairmount Funds and Venrock Healthcare Capital Partners, and has since assembled a management team of drug developers and an executive team with significant experience in clinical development, manufacturing of biologics and leading public biopharmaceutical company operations, financing and transactions. Apogee Therapeutics, Inc., a successor to Apogee Therapeutics, LLC, was formed as a Delaware corporation in June 2023 in preparation for our IPO. We maintain a corporate headquarters in Waltham, Massachusetts, laboratory space in Boston, Massachusetts and otherwise operate virtually in the United States. In addition, we engage significantly with third parties, including Paragon, who is also a related party, to perform ongoing research and development activities and other services on our behalf.
Our pipeline comprises four programs being developed initially for the treatment of I&I indications. Our two most advanced programs, APG777 and APG808, which we are initially developing for the treatment of AD and COPD, respectively, target the same mechanism of action as lebrikizumab and DUPIXENT (dupilumab), respectively. Moreover, we are evaluating APG777 in additional I&I indications, including asthma, alopecia areata, chronic rhinosinusitis with nasal polyps, chronic spontaneous urticaria, eosinophilic esophagitis and prurigo nodularis. Our earlier-stage programs, APG990 and APG222, utilize advanced antibody engineering to target OX40L and both IL-13 and OX40L, respectively. We recently added a new program that also utilizes advanced antibody engineering for an undisclosed target. Our programs incorporate advanced antibody engineering to optimize half-life and other properties designed to overcome limitations of existing therapies. We believe each of our programs has potential for broad application across multiple I&I indications.
In August 2023, we announced the dosing of our first participant in our first clinical trial for APG777 in Australia. The APG777 Phase 1 trial is a double-blind, placebo-controlled study in healthy volunteers and consists of a SAD component and a MAD component. The trial enrolled 40 healthy adult subjects into three SAD and two MAD cohorts. The primary endpoint is safety and a key secondary endpoint is PK. The Phase 1 trial is ongoing and we have announced initial safety and PK data from this trial. We filed an IND in support of a Phase 1 trial in healthy volunteers in the United States for subjects of Japanese descent and have received a “safe to proceed” notification from the FDA for the trial. We anticipate initiating a Phase 2 trial in AD in the United States and internationally in the first half of 2024.
In November 2023, we finalized the nomination of a development candidate for APG808 and we have received regulatory approval to commence a first-in-human clinical trial in Australia. APG808 is an SQ extended half-life mAb targeting IL-4Rα, a target with clinical validation across eight different Type 2 allergic diseases. APG808 has similar binding as a first generation mAb, DUPIXENT, with femtomolar affinity for IL-4Rα and has demonstrated similar inhibition to DUPIXENT across three in vitro assays which measure downstream functional inhibition of the IL-13/IL-4 pathway (pSTAT6 induction, inhibition of TF-1 proliferation, and inhibition of TARC secretion). Additionally, in our head-to-head studies of APG808 and DUPIXENT in non-human primates, APG808 showed a significantly longer half-life than DUPIXENT.
123
In these preclinical studies, APG808’s half-life was up to 27 days, as compared to 11 days for DUPIXENT. Based on these preclinical studies, we believe that the longer half-life could support dosing either every 6 weeks or every 2 months in the clinic, which, if future clinical trials are successful, would represent a significant improvement compared to DUPIXENT which is currently being investigated with every 2-week dosing in COPD. We anticipate that APG808 will enter the clinic in healthy volunteers in the first half of 2024 followed by a potential Phase 1b trial in asthma and/or a Phase 2 trial in COPD (pending data from the Phase 1 trial and following the submission of an IND or foreign equivalent to support such trials).
Since our inception in February 2022, we have devoted substantially all of our resources to raising capital, organizing and staffing our company, business and scientific planning, conducting discovery and research activities, acquiring product programs, establishing and protecting our intellectual property portfolio, developing and progressing our pipeline, establishing arrangements with third parties for the manufacture of our programs and component materials, and providing general and administrative support for these operations. We do not have any programs approved for sale and have not generated any revenue from product sales. To date, we have funded our operations primarily with proceeds from the issuance of preferred units and sale of common stock. Through December 31, 2023, we received gross proceeds of $169.0 million from sales of our preferred units. On July 13, 2023, our Registration Statement on Form S 1, as amended (File Nos. 333 272831 and 333 273236) (the Registration Statement), relating to our IPO was declared effective by the SEC. Pursuant to the Registration Statement, we issued and sold an aggregate of 20,297,500 shares of common stock (inclusive of 2,647,500 shares pursuant to the exercise in full of the underwriters’ option to purchase additional shares) at a public offering price of $17.00 per share, for aggregate net proceeds of $315.4 million after deducting underwriting discounts and commissions and other offering expenses.
We have incurred significant operating losses since inception. Our ability to generate product revenue sufficient to achieve profitability will depend heavily on the successful development and eventual commercialization of any programs we may develop. We generated net losses of $84.0 million for the year ended December 31, 2023. As of December 31, 2023, we had an accumulated deficit of $123.8 million. We expect to continue to incur significantly increased expenses for the foreseeable future if and as we:
| ● | advance our most advanced programs, APG777 and APG808, through clinical trials and regulatory approval prior to commercialization; |
| ● | continue our research and development and preclinical development of our other programs, including APG990 and APG222; |
| ● | seek and identify additional research programs and product candidates and initiate preclinical studies for those programs; |
| ● | maintain, expand, enforce, defend and protect our intellectual property portfolio and provide reimbursement of third-party expenses related to our patent portfolio; |
| ● | hire additional research and development and clinical personnel; |
| ● | experience any delays, challenges, or other issues associated with the clinical development of our programs, including with respect to our regulatory strategies; |
| ● | seek marketing approvals for any programs for which we successfully complete clinical trials; |
| ● | develop, maintain and enhance a sustainable, scalable, reproducible and transferable manufacturing process for the programs we may develop; |
| ● | ultimately establish a sales, marketing and distribution infrastructure to commercialize any programs for which we may obtain marketing approval; |
124
| ● | add operational, financial and management information systems and personnel, including personnel to support our product development; |
| ● | acquire or in-license product candidates or programs, intellectual property and technologies; |
| ● | establish and maintain our current and any future collaborations, including making royalty, milestone or other payments thereunder; and |
| ● | operate as a public company. |
We will not generate revenue from product sales unless and until we successfully initiate and complete clinical development and obtain regulatory approval for any product candidates. If we obtain regulatory approval for any of our programs and do not enter into a commercialization partnership, we expect to incur significant expenses related to developing our commercialization capability to support product sales, manufacturing, marketing, and distribution. Further, we expect to incur additional costs associated with operating as a public company, including increased costs of accounting, audit, legal, regulatory and tax-related services associated with compliance with exchange listing and SEC requirements, director and officer insurance costs and investor and public relations costs.
As a result, we will need substantial additional funding to support our continued operations and growth strategy. Until such a time as we can generate significant revenue from product sales, if ever, we expect to finance our operations through the sale of equity, debt financings or other capital sources, including collaborations with other companies or other strategic transactions. We may be unable to raise additional funds or enter into such other agreements on favorable terms, or at all. If we fail to raise capital or enter into such agreements as, and when, needed, we may have to significantly delay, scale back or discontinue the development and commercialization of one or more of our programs.
Because of the numerous risks associated with product development, we are unable to accurately predict the timing or amount of increased expenses or when or if we will be able to achieve or maintain profitability. Even if we are able to generate product sales, we may not become profitable. If we fail to become profitable or are unable to sustain profitability on a continuing basis, then we may be unable to continue our operations at planned levels and be forced to reduce or terminate our operations.
We expect that our existing cash and cash equivalents of $118.3 million, and marketable securities of $277.1 million as of December 31, 2023 will enable us to fund our operating expenses and capital expenditure requirements into the fourth quarter of 2026. We have based this estimate on assumptions that may prove to be wrong, and we could use our capital resources sooner than we currently expect. See “Liquidity and Capital Resources” for further information.
Reorganization
Apogee Therapeutics, LLC was formed as a limited liability company under the laws of the State of Delaware in February 2022. Apogee Therapeutics, Inc. was incorporated in June 2023, in connection with our IPO to serve as a holding company that would wholly own the assets of Apogee Therapeutics, LLC. Prior to July 13, 2023, our business was conducted by Apogee Therapeutics, LLC and its subsidiary, Apogee Biologics, Inc. In July 2023, in connection with our IPO, we completed a series of transactions which are referred to, collectively, as the “Reorganization,” and pursuant to which Apogee Therapeutics, Inc., became the parent and holding company that wholly owns the assets of Apogee Therapeutics, LLC, including stock of its subsidiary, Apogee Biologics, Inc. In connection with our Reorganization:
| ● | holders of Series A preferred units of Apogee Therapeutics, LLC received 7,678,000 shares of non-voting common stock of Apogee Therapeutics, Inc.; |
| ● | holders of Series B preferred units of Apogee Therapeutics, LLC received 11,501,108 shares of common stock and 5,808,642 shares of non-voting common stock of Apogee Therapeutics, Inc.; |
125
| ● | holders of common units of Apogee Therapeutics, LLC received 1,919,500 shares of common stock of Apogee Therapeutics, Inc.; |
| ● | holders of vested incentive units of Apogee Therapeutics, LLC received 690,188 shares of common stock of Apogee Therapeutics, Inc.; and |
| ● | holders of unvested incentive units of Apogee Therapeutics, LLC received 2,779,358 shares of restricted common stock of Apogee Therapeutics, Inc. |
Our Collaboration, License and Services Agreements
Paragon Option Agreements
In February 2022, we entered into the, 2022 Option Agreement. Under the terms of the 2022 Option Agreement, Paragon identifies, evaluates and develops antibodies directed against certain mutually agreed therapeutic targets of interest to us. The 2022 Option Agreement initially included two selected targets, IL-13 and IL-4Rα, and was subsequently amended in November 2022 to include an additional selected target, OX40L. Under the 2022 Option Agreement, we have the exclusive option to, on a research program-by-research program basis, be granted an exclusive, worldwide license to all of Paragon’s right, title and interest in and to the intellectual property resulting from the applicable research program to develop, manufacture and commercialize the antibodies and products directed to the selected targets. From time to time, we can choose to add additional targets to the collaboration by mutual agreement with Paragon.
Pursuant to the terms of the 2022 Option Agreement, the parties will initiate certain research programs that will generally be focused on a particular target. Each Research Program will be aimed at discovering, generating, identifying and/or characterizing antibodies directed to the respective target. For each Research Program, the parties established a research plan that sets forth the activities that will be conducted, and the associated research budget. Upon execution of the 2022 Option Agreement, we agreed with Paragon on an initial Research Plan that outlined the services that will be performed commencing at inception of the arrangement related to IL-13 and IL-4Rα. The Research Plan for OX40L was agreed to prior to December 31, 2022. Our exclusive option with respect to any future Research Program is exercisable at our sole discretion, at any time during the period beginning on the initiation of activities under the associated Research Program and ending a specified number of days following the delivery of the data package from Paragon related to the results of the Research Plan activities. There is no payment due upon exercise of an Option pursuant to the 2022 Option Agreement.
In consideration for the exclusive options granted under the 2022 Option Agreement, we paid an upfront cash amount of $1.3 million and issued 1,250,000 common units to Paragon. Paragon was also entitled to up to an additional 3,750,000 of common units in exchange for the rights granted under the 2022 Option Agreement, which were issued in connection with the closings of the additional tranches of the Series A Preferred Unit financing. As of December 31, 2023, we had issued a total of 5,000,000 common units to Paragon with an aggregate fair value of $2.2 million on the grant date, which subsequently were exchanged for common stock following the IPO. Under the 2022 Option Agreement, on a Research Program-by-Research Program basis following the finalization of the Research Plan for each respective Research Program, we are required to pay Paragon a nonrefundable fee in cash of $0.5 million. We are also obligated to compensate Paragon on a quarterly basis for its services performed under each Research Program based on the actual costs incurred. We expense the service fees as the associated costs are incurred when the underlying services are rendered. Such amounts are classified within research and development expenses in our consolidated statement of operations and comprehensive loss.
In November 2023, we entered into the 2023 Option Agreement. Under the terms of the 2023 Option Agreement, Paragon identifies, evaluates and develops antibodies directed against certain mutually agreed therapeutic targets of interest to us. The 2023 Option Agreement initially includes one undisclosed target. Under the 2023 Option Agreement, we have the exclusive option to, on a research program-by-research program basis, be granted an exclusive, worldwide license to all of Paragon’s right, title and interest in and to the intellectual property resulting from the applicable research program to develop, manufacture and commercialize the antibodies and products directed to the selected targets. From time to time, we can choose to add additional targets to the collaboration by mutual agreement with Paragon.
126
Pursuant to the terms of the 2023 Option Agreement, the parties may initiate Research Programs. Each Research Program is aimed at discovering, generating, identifying and/or characterizing antibodies directed to the respective target. For each Research Program, the parties must establish a Research Plan. In January 2024, we agreed on an initial Research Plan with Paragon that outlines the services that will be performed commencing at inception of the arrangement related to the undisclosed target. Our exclusive option with respect to each Research Program is exercisable at our sole discretion at any time during the period beginning on the initiation of activities under the associated Research Program and ending a specified number of days following the delivery of the data package from Paragon related to the results of the Research Plan activities. There is no payment due upon exercise of an Option pursuant to the 2023 Option Agreement. Following entry into the 2023 Option Agreement, we and Paragon will negotiate a form of License Agreement to be entered into in the event that we exercise our exclusive option with respect to each Research Program, which License Agreement will include certain pre-agreed economic and other business terms.
Under the 2023 Option Agreement, on a Research Program-by-Research Program basis following the finalization of the Research Plan for each respective Research Program, we are required to pay Paragon a nonrefundable fee in cash of $2.0 million. In the first quarter of 2024, we paid Paragon a $2.0 million fee for a Research Program for an undisclosed target. We are also obligated to compensate Paragon on a quarterly basis for its services performed under each Research Program based on the actual costs incurred. We expense the service fees as the associated costs are incurred when the underlying services are rendered.
Unless terminated earlier, the Option Agreement shall continue in force on a Research Program-by-Research Program basis until the earlier of: (i) the end of the Option Period for such Research Program, as applicable, if such Option is not exercised by us; and (ii) the effective date of the license agreement for such Research Program if we exercise our Option with respect to such Research Program. Upon the expiration of the Term for all then-existing Research Programs, the applicable Option Agreement will automatically expire in its entirety. We may terminate either Option Agreement or any Research Program at any time for any or no reason upon 30 days’ prior written notice to Paragon, provided that we must pay certain unpaid fees due to Paragon upon such termination, as well as any non-cancellable obligations reasonably incurred by Paragon in connection with its activities under any terminated Research Program. Each party has the right to terminate either Option Agreement or any Research Program upon (i) 30 days’ prior written notice of the other party’s material breach that remains uncured for the 30 day period and (ii) the other party’s bankruptcy.
Paragon License Agreements
In November 2022, we exercised our option available under the 2022 Option Agreement with respect to the IL-13 Research Program. Upon such exercise, the parties entered into the IL-13 License Agreement. In April 2023, we exercised our option available under the 2022 Option Agreement with respect to the IL-4Rα Research Program and OX40L Research Program. Upon such exercise, the parties entered into the IL-4Rα License Agreement and the OX40L License Agreement. Under the terms of the License Agreements, Paragon granted to us an exclusive, worldwide, royalty-bearing, sublicensable right and license with respect to certain information, patent rights and sequence information related to antibodies directed at the respective target to use, make, sell, import, export and otherwise exploit the antibodies directed at the respective target. Pursuant to the License Agreements, we granted to Paragon a similar license (except that such license we granted to Paragon is non-exclusive) to the respective licenses with respect to multispecific antibodies that are directed at the respective targets and one or more other antibodies. We were also granted a right of first negotiation with Paragon concerning the development, license and grant of rights to certain multispecific antibodies associated with each respective license. We are solely responsible for the continued development, manufacture and commercialization of products at our own cost and expense for each licensed target.
We are obligated to pay Paragon up to $3.0 million upon the achievement of specific development and clinical milestones for the first product under each of the License Agreements that achieves such specified milestones, including a payment of $1.0 million upon the nomination of a development candidate and $2.0 million upon the first dosing of a human patient in a Phase 1 trial. Upon execution of the IL-13 License Agreement, we paid Paragon a $1.0 million fee for the nomination of a development candidate. In August 2023, we announced the dosing of our first participant in the Phase 1 trial of APG777 and accordingly have recorded research and development expense for the milestone payment of $2.0 million to Paragon in the year ended December 31, 2023. In November 2023, we finalized the nomination of a development candidate under the IL-4Rα License Agreement and made a milestone payment of $1.0 million to Paragon in the fourth quarter of 2023.
127
The nomination of a development candidate under the OX40L License Agreement had not yet occurred as of December 31, 2023.
We are also obligated to pay royalties to Paragon equal to a low-single digit percentage of net sales of any products under each of the respective License Agreements, and Paragon has a similar obligation to pay royalties to us with respect to each of the multispecific licenses. Royalties are due on a product-by-product and country-by-country basis beginning upon the first commercial sale of each product and ending on the later of (i) 12 years after the first commercial sale of such product in such country and (ii) expiration of the last valid claim of a patent covering such product in such country.
Biologics Master Services Agreement-WuXi Biologics (Hong Kong) Limited
In June 2022, Paragon and WuXi Biologics entered into the WuXi Biologics MSA, which was subsequently novated to us by Paragon in the second quarter of 2023. The WuXi Biologics MSA governs all development activities and GMP manufacturing and testing for APG777, APG808 and APG990 programs, as well as potential future programs, on a work order basis. Under the WuXi Biologics MSA, we are obligated to pay WuXi Biologics a service fee and all non-cancellable obligations in the amount specified in each work order associated with the agreement for the provision of services.
The WuXi Biologics MSA terminates on the later of (i) June 20, 2027 or (ii) the completion of services under all work orders executed by the parties prior to June 20, 2027, unless terminated earlier. The term of each work order terminates upon completion of the services under such work order, unless terminated earlier. We can terminate the WuXi Biologics MSA or any work order at any time upon 30 days’ prior written notice and immediately upon written notice if WuXi Biologics fails to obtain or maintain required material governmental licenses or approvals. Either party may terminate a work order (i) at any time upon six months’ prior notice with reasonable cause, provided however that if WuXi Biologics terminates a work order in such manner, no termination or cancellation fees shall be paid by us and (ii) immediately for cause upon (a) the other party’s material breach that remains uncured for 30 days after notice of such breach, (b) the other party’s bankruptcy or (c) a force majeure event that prevents performance for a period of at least 90 days.
Cell Line License Agreement — WuXi Biologics (Hong Kong) Limited
In June 2022, Paragon and WuXi Biologics entered into the Cell Line License Agreement, which was subsequently novated to us by Paragon in the second quarter of 2023. Under the Cell Line License Agreement, we received a non-exclusive, worldwide, sublicensable license to the WuXi Biologics Licensed Technology and media and feeds to make, have made, use, sell and import the WuXi Biologics Licensed Products. Specifically, the WuXi Biologics Licensed Technology is used to manufacture a component of the APG777 and APG808 programs.
In consideration for the license, we agreed to pay WuXi Biologics a non-refundable license fee of $150,000. Additionally, if we manufacture all of our commercial supplies of bulk drug product with a manufacturer other than WuXi Biologics or its affiliates, we are required to make the Royalty payments to WuXi Biologics. If we manufacture part of our commercial supplies of the WuXi Biologics Licensed Products with WuXi Biologics or its affiliates, then the Royalty will be reduced accordingly on a pro rata basis.
The Cell Line License Agreement will continue indefinitely unless terminated (i) by us upon six months’ prior written notice and our payment of all undisputed amounts due to WuXi Biologics through the effective date of termination, (ii) by WuXi Biologics for a material breach by us that remains uncured for 60 days after written notice, (iii) by WuXi Biologics if we fail to make a payment and such failure continues for 30 days after receiving notice of such failure, or (iv) by either party upon the other party’s bankruptcy.
For additional detail regarding the agreements described above, see the section titled “Notes to Consolidated Financial Statements—Other Significant Agreements” included elsewhere in this Annual Report.
128
Overview of Financial Results
Revenue
We have not generated any revenue from product sales and do not expect to generate any revenue from the sale of products for several years, if at all. If our development efforts for our programs are successful and result in regulatory approval or collaboration or license agreements with third parties, we may generate revenue in the future from product sales or payments from collaboration or license agreements that we may enter into with third parties, or any combination thereof.
Operating Expenses
Our operating expenses consist of (i) research and development expenses and (ii) general and administrative expenses.
Research and Development
Research and development expenses consist primarily of costs incurred in connection with the development and research of our programs.
These expenses include:
| ● | costs of funding research performed by third parties, including Paragon, that conduct research and development and preclinical or clinical activities on our behalf; |
| ● | the cost to acquire in-process research and development, with no alternative future use associated with asset acquisitions, such as the Option Agreements and License Agreements; |
| ● | expenses incurred in connection with continuing our current research programs and preclinical development of any programs we may identify, including under agreements with third parties, such as consultants and contractors; |
| ● | the cost of developing and validating our manufacturing process for use in our preclinical studies and current and future clinical trials; and |
| ● | personnel-related expenses, including salaries, bonuses and equity-based compensation expense. |
We measure and recognize asset acquisitions or licenses to intellectual property that are not deemed to be business combinations based on the cost to acquire or license the asset or group of assets, which includes transaction costs. In an asset acquisition or license of intellectual property, the cost allocated to acquired in-process research and development, with no alternative future use is recognized as research and development expense on the acquisition date.
We expense research and development costs as incurred. Non-refundable advance payments that we make for goods or services to be received in the future for use in research and development activities are recorded as prepaid expenses. The prepaid amounts are expensed as the related goods are delivered or the services are performed, or when it is no longer expected that the goods will be delivered or the services rendered.
Our primary focus since inception has been the identification and development of our pipeline programs. Our research and development costs primarily consist of external costs, such as fees paid to Paragon under the Option Agreements, and the License Agreements. We do not separately track or segregate the amount of costs incurred under the Option Agreement due to the early-stage and discovery nature of the services. We do not allocate personnel-related costs by program because these resources are used and these costs are deployed across multiple programs under development, and, as such, are not separately classified.
129
We expect that our research and development expenses will increase substantially for the foreseeable future as we continue to invest in research and development activities related to the continued development of our programs, developing any future programs, including investments in manufacturing, as we advance any programs we may identify and continue to conduct clinical trials. The success of programs we may identify and develop will depend on many factors, including the following:
| ● | timely and successful completion of preclinical studies; |
| ● | effective INDs or comparable foreign applications that allow commencement of our planned clinical trials or future clinical trials for any programs we may develop; |
| ● | successful enrollment and completion of clinical trials; |
| ● | positive results from our future clinical trials that support a finding of safety and effectiveness, acceptable PK profile, and an acceptable risk-benefit profile in the intended populations; |
| ● | receipt of marketing approvals from applicable regulatory authorities; |
| ● | establishment of arrangements through our own facilities or with third-party manufacturers for clinical supply and, where applicable, commercial manufacturing capabilities; |
| ● | establishment, maintenance, defense and enforcement of patent, trademark, trade secret and other intellectual property protection or regulatory exclusivity for any products we may develop; and |
| ● | maintenance of a continued acceptable safety, tolerability and efficacy profile of any programs we may develop following approval. |
Any changes in the outcome of any of these variables with respect to the development of programs that we may identify could mean a significant change in the costs and possible delays in timing associated with the development of such programs. For example, if the FDA or another regulatory authority were to require us to conduct clinical trials beyond those that we currently anticipate will be required for the completion of clinical development of a program, or if we experience significant delays in our clinical trials due to patient enrollment or other reasons, we would be required to expend significant additional financial resources and time on the completion of clinical development. We may never obtain regulatory approval for any of our programs.
General and Administrative
General and administrative expenses consist primarily of personnel-related expenses, including salaries, bonuses, and equity-based compensation, for individuals in our executive, finance, operations, human resources, business development and other administrative functions. Other significant general and administrative expenses include legal fees relating to corporate matters, professional fees for accounting, auditing, tax and administrative consulting services, insurance costs and recruiting costs. These costs relate to the operation of the business, unrelated to the research and development function, or any individual program.
We expect that our general and administrative expenses will increase substantially for the foreseeable future as we increase our headcount to support the expected growth in our research and development activities and the potential commercialization of our programs, if approved. We also expect to incur increased expenses associated with being a public company, including increased costs of accounting, audit, legal, regulatory and tax-related services associated with maintaining compliance with exchange listing and SEC requirements, director and officer insurance costs, and investor and public relations costs.
130
We do not incur material operating expenses for the rent, maintenance and insurance of facilities or for depreciation of fixed assets.
Other Income (Expense), Net
Interest Income
Interest income consists of interest income earned from our cash, cash equivalents, and marketable securities and amortization of investment discounts.
Income Taxes
Since our inception, we have not recorded any income tax benefits for the net losses we have incurred or for the research and development tax credits generated in each period as we believe, based upon the weight of available evidence, that it is more likely than not that all of our net operating loss (“NOL”) carryforwards and tax credit carryforwards will not be realized. As of December 31, 2023, we had U.S. federal NOL carryforwards of approximately $23.6 million, which may be available to reduce future taxable income and have an indefinite carryforward period but are limited in their usage to an annual deduction equal to 80% of annual taxable income. As of December 31, 2023, we also had U.S. federal and state research and development tax credit carryforwards of approximately $2.7 million and $0.7 million, respectively, which may be available to reduce future tax liabilities. The U.S. federal research and development tax credit carryforwards expire at various dates beginning in 2042 and the state research and development tax credit carryforwards do not expire. We have recorded a full valuation allowance against our net deferred tax assets at the balance sheet date.
Comparison of the Year Ended December 31, 2023 to the Period from February 4, 2022 (inception) to December 31, 2022
The following table summarizes our consolidated statements of operations for the period presented (in thousands):
|
|
|
|
|
PERIOD FROM |
|
|
|
|
|
|
YEAR ENDED |
|
FEBRUARY 4, 2022 |
|
|
|
||
|
|
DECEMBER 31, |
|
(INCEPTION) TO |
|
|
|
||
|
|
2023 |
|
DECEMBER 31, 2022 |
|
$ CHANGE |
|||
Operating expenses: |
|
|
|
|
|
|
|
|
|
Research and development |
|
$ |
68,424 |
|
$ |
27,786 |
|
|
40,638 |
General and administrative |
|
|
24,579 |
|
|
2,941 |
|
|
21,638 |
Total operating expenses |
|
|
93,003 |
|
|
30,727 |
|
|
62,276 |
Loss from operations |
|
|
(93,003) |
|
|
(30,727) |
|
|
(62,276) |
Other income (expense), net: |
|
|
|
|
|
|
|
|
|
Interest income |
|
|
9,018 |
|
|
92 |
|
|
8,926 |
Other financing expense |
|
|
— |
|
|
(9,150) |
|
|
9,150 |
Total other income (expense), net |
|
|
9,018 |
|
|
(9,058) |
|
|
18,076 |
Net loss |
|
$ |
(83,985) |
|
$ |
(39,785) |
|
$ |
(44,200) |
131
Research and Development Expense
The following table summarizes our research and development expenses incurred for the periods presented (in thousands):
|
|
|
|
|
PERIOD FROM |
|
|
|
YEAR ENDED |
|
FEBRUARY 4, 2022 |
||
|
|
DECEMBER 31, |
|
(INCEPTION) TO |
||
|
|
2023 |
|
DECEMBER 31, 2022 |
||
External research and development costs by program: |
|
|
|
|
|
|
APG777 |
|
$ |
21,644 |
|
$ |
— |
APG808 (1) |
|
|
20,801 |
|
|
— |
Unallocated research and development costs: |
|
|
|
|
|
|
In-process research and development acquisitions |
|
|
— |
|
|
4,505 |
External-discovery related costs and other |
|
|
15,019 |
|
|
21,237 |
Personnel-related (including equity-based compensation) |
|
|
10,960 |
|
|
2,044 |
Total research and development expenses |
|
$ |
68,424 |
|
$ |
27,786 |
(1) |
External research and development costs for APG808 for the period from February 4, 2022 (inception) to December 31, 2022, were recorded as unallocated external discovery related costs. Note that the development candidate for APG808 was nominated in November 2023. |
Research and development expenses for the year ended December 31, 2023 were $68.4 million, compared to $27.8 million for the period from February 4, 2022 (inception) to December 31, 2022. For the year ended December 31, 2023, we recorded $21.6 million of external research and development expense related to the APG777 program, which included a $2.0 million milestone payable upon the first dosing of a human patient in a Phase 1 trial in August 2023, and no such expense was recorded in the period from February 4, 2022 (inception) to December 31, 2022, as APG777 expenses were recorded as unallocated external-discovery related costs until the program candidate was nominated in November 2022. For the year ended December 31, 2023, we recorded $20.8 million of external research and development expense related to the APG808 program, which included a $1.0 million milestone payable upon the nomination of a development candidate, and no such expense was recorded in the period from February 4, 2022 (inception) to December 31, 2022, as APG808 expenses were recorded as unallocated external-discovery related costs until the program candidate was nominated in November 2023. Other external-discovery related costs decreased from $21.2 million in the period from February 4, 2022 (inception) to December 31, 2022 to $15.0 million for the year ended December 31, 2023, due to the advancement of the APG777 and APG808 programs and those costs now reported as separate programs for the year ended December 31, 2023 due to the aforementioned nominations of the respective development candidates. Additionally, there was $4.5 million of in-process research and development acquisition costs in the period from February 4, 2022 (inception) to December 31, 2022. Our personnel related expenses were $11.0 million for the year ended December 31, 2023 compared to $2.0 million recorded for the period from February 4, 2022 (inception) to December 31, 2022. The increase in personnel related costs was primarily due to an increase in headcount and share-based compensation expense in the year ended December 31, 2023 compared to the period from February 4, 2022 (inception) to December 31, 2022.
General and Administrative Expense
The following table summarizes our general and administrative expenses for the periods presented (in thousands):
|
|
|
|
|
PERIOD FROM |
|
|
|
YEAR ENDED |
|
FEBRUARY 4, 2022 |
||
|
|
DECEMBER 31, |
|
(INCEPTION) TO |
||
|
|
2023 |
|
DECEMBER 31, 2022 |
||
Personnel-related (including equity-based compensation) |
|
$ |
12,577 |
|
$ |
1,642 |
Legal and professional fees |
|
|
4,322 |
|
|
1,073 |
Other |
|
|
7,680 |
|
|
226 |
Total general and administrative expenses |
|
$ |
24,579 |
|
$ |
2,941 |
132
General and administrative expenses for the year ended December 31, 2023 were $24.6 million, compared to $2.9 million in the period from February 4, 2022 (inception) to December 31, 2022. The increase of $21.7 million was primarily due to an increase of personnel costs of $11.0 million, an increase in legal and professional services costs of $3.2 million and an increase of other expenses of $7.5 million, all of which were the result of the expansion of our operations to support the growth in our business and the cost of operating as a public company.
Other Income (Expense), Net
Interest income increased $8.9 million for the year ended December 31, 2023 compared to the period from February 4, 2022 (inception) to December 31, 2022, which was primarily related to interest on our cash, cash equivalents and marketable securities.
Other financing expense was $9.2 million for the Period from February 4, 2022 (inception) to December 31, 2022, which was related to the change in fair value for the tranche options associated with the Series A Preferred Unit financing.
Liquidity and Capital Resources
Sources of Liquidity
Since our inception, we have incurred significant losses. We have not yet commercialized any of our programs, which are in various phases of early-stage development, and we do not expect to generate revenue from sales of any of our programs for several years, if at all. To date, we have financed our operations from the proceeds from the issuance of preferred units and the sale of common stock in our IPO. From inception through December 31, 2023, we have raised $484.4 million in aggregate cash proceeds from such transactions. As of December 31, 2023, we had cash and cash equivalents of $118.3 million and $277.1 million of marketable securities.
In connection with our IPO in July 2023, we issued and sold an aggregate of 20,297,500 shares of common stock (inclusive of 2,647,500 shares pursuant to the exercise in full of the underwriters’ option to purchase additional shares) at a price of $17.00 per share. We received net proceeds of $315.4 million, after deducting underwriting discounts and commissions and other offering expenses.
Cash Flows
The following table provides information regarding our cash flows for the periods presented (in thousands):
|
|
|
|
|
PERIOD FROM |
|
|
|
YEAR ENDED |
|
FEBRUARY 4, 2022 |
||
|
|
DECEMBER 31, |
|
(INCEPTION) TO |
||
|
|
2023 |
|
DECEMBER 31, 2022 |
||
Net cash, cash equivalents, and restricted cash provided by (used in): |
|
|
|
|
|
|
Operating activities |
|
$ |
(74,761) |
|
$ |
(16,427) |
Investing activities |
|
|
(273,910) |
|
|
— |
Financing activities |
|
|
315,391 |
|
|
168,317 |
Net (decrease) increase in cash equivalents, and restricted cash |
|
$ |
(33,280) |
|
$ |
151,890 |
Net Cash used in Operating Activities
Cash used in operating activities resulted primarily from our net losses adjusted for non-cash charges and changes in components of operating assets and liabilities, which are generally attributable to timing of payments, and the related effect on certain account balances, operational and strategic decisions and contracts to which we may be a party.
133
For the year ended December 31, 2023, operating activities used $74.8 million of cash, primarily due to a net loss of $84.0 million, partially offset by non-cash charges of $6.1 million for equity-based compensation and net changes in our operating assets and liabilities of $6.1 million.
For the period from February 4, 2022 (inception) to December 31, 2022, operating activities used $16.4 million of cash, primarily due to a net loss of $39.8 million, partially offset by non-cash charges including $2.2 million for equity-based compensation expense related to common units issued under the 2022 Option Agreement with Paragon, $2.1 million for equity-based compensation and non-cash loss on remeasurement of the tranche option liability of $9.2 million and net changes in operating assets and liabilities of $9.8 million.
Net Cash used in Investing Activities
During the year ended December 31, 2023, net cash used in investing activities of $273.9 million was primarily related to purchases of marketable securities, partially offset by the maturities of marketable securities.
Net Cash provided by Financing Activities
For the year ended December 31, 2023, financing activities provided $315.4 million of cash related to the issuance and sale of common stock in our IPO, net of paid issuance costs.
For the period from February 4, 2022 (inception) to December 31, 2022, financing activities provided $168.3 million of cash from the issuance and sale of our Series A preferred units.
Future Funding Requirements
To date, we have not generated any revenue from product sales. We do not expect to generate revenue from product sales unless and until we successfully complete preclinical and clinical development of, receive regulatory approval for, and commercialize a program and we do not know when, or if at all, that will occur. We expect our expenses to increase substantially in connection with our ongoing activities, particularly as we advance the preclinical activities and studies and initiate clinical trials. In addition, if we obtain regulatory approval for any programs, we expect to incur significant expenses related to product sales, marketing, and distribution to the extent that such sales, marketing and distribution are not the responsibility of potential collaborators. We expect to incur additional costs associated with operating as a public company. The timing and amount of our operating expenditures will depend largely on the factors set out above. Our funding requirements and timing and amount of our operating expenditures will depend on many factors, including, but not limited to:
| ● | the rate of progress in the development of our APG777 and APG808 programs and other development programs; |
| ● | the scope, progress, results and costs of preclinical studies and clinical trials for any other current and future programs; |
| ● | the number and characteristics of programs and technologies that we develop or may in-license; |
| ● | the costs and timing of future commercialization activities, including manufacturing, marketing, sales and distribution, for any of our programs for which we receive marketing approval; |
| ● | the costs necessary to obtain regulatory approvals, if any, for any approved products in the United States and other jurisdictions, and the costs of post-marketing studies that could be required by regulatory authorities in jurisdictions where approval is obtained; |
| ● | the costs and timing of preparing, filing and prosecuting patent applications, maintaining and enforcing our intellectual property rights and defending any intellectual property-related claims; |
134
| ● | the continuation of our existing licensing arrangements and entry into new collaborations and licensing arrangements; |
| ● | the costs we incur in maintaining business operations; |
| ● | the costs of hiring additional clinical, quality control, manufacturing and other scientific personnel; |
| ● | the costs adding operational, financial and management information systems and personnel; |
| ● | the costs associated with being a public company; |
| ● | the costs and timing of future laboratory facilities; |
| ● | the revenue, if any, received from commercial sales of our programs for which we receive marketing approval; |
| ● | the effect of competing technological and market developments; and |
| ● | the extent to which we acquire or invest in businesses, products and technologies, including entering into licensing or collaboration arrangements for programs. |
For more information, see the section titled “Risk Factors—Risks Related to Our Limited Operating History, Financial Position and Capital Requirements.”
Identifying potential programs and product candidates and conducting preclinical studies and clinical trials is a time consuming, expensive and uncertain process that takes years to complete, and we may never generate the necessary data or results required to obtain marketing approval and achieve product sales. In addition, our programs, if approved, may not achieve commercial success. Our commercial revenues, if any, will be derived from sales of products that we do not expect to be commercially available for many years, if ever. Accordingly, we will need to obtain substantial additional funds to achieve our business objectives.
Adequate additional funds may not be available to us on acceptable terms, or at all. We do not currently have any committed external source of funds. To the extent that we raise additional capital through the sale of equity or convertible debt securities, our stockholders’ ownership interests could be diluted, and the terms of these securities may include liquidation or other preferences that could adversely affect our stockholders’ rights.
Additional debt financing and preferred equity financing, if available, may involve agreements that include covenants limiting or restricting our ability to take specific actions, such as incurring debt, making capital expenditures or declaring dividends, and may require the issuance of warrants, which could potentially dilute our stockholders’ ownership interests.
If we raise additional funds through strategic collaborations or licensing arrangements with third parties, we may have to relinquish valuable rights to our technologies, future revenue streams, research programs, or product candidates or grant licenses on terms that may not be favorable to us.
If we are unable to raise additional funds through equity or debt financings when needed, we may be required to delay, limit or terminate our product development programs or any future commercialization efforts or grant rights to develop and market product candidates to third parties that we would otherwise prefer to develop and market ourselves.
As of December 31, 2023, we had $118.3 million of cash and cash equivalents and $277.1 million of marketable securities. Based on our current operating plan, as of the date of this Annual Report, we estimate that our existing cash, cash equivalents, and marketable securities will be sufficient to enable us to fund our operating expenses and capital expenditure requirements through at least the next twelve months following the issuance of our consolidated financial statements included elsewhere in the Annual Report.
135
Moreover, based on our current operating plan, we estimate that such funds will be sufficient to enable us to fund our operating expenses and capital expenditure requirements into the fourth quarter of 2026. We have based this estimate on assumptions that may prove to be wrong, and we could exhaust our available capital resources sooner than we expect.
Contractual Obligations and Other Commitments
We enter into contracts in the normal course of business with contract research organizations (“CROs”), contract manufacturing organizations (“CMOs”) and other third parties for preclinical research studies and testing, clinical trials, manufacturing and other services. These contracts do not contain any minimum purchase commitments and provide for termination by us upon prior written notice. Payments due upon cancellation consist only of payments for services provided and expenses incurred up to the date of cancellation, including non-cancelable obligations of our service providers and, in some cases, wind-down costs. The exact amounts of such obligations are dependent on the timing of termination and the terms of the associated agreement. Accordingly, these payments are not disclosed as the amount and timing of such payments are not known.
Our agreements to license intellectual property include potential milestone payments that are dependent upon the development of products using the intellectual property licensed under the agreements and contingent upon the achievement of specific development and clinical milestones. As of December 31, 2023, we have incurred $4.0 million of the maximum aggregate potential milestone payments. We are also obligated to pay royalties to (i) Paragon at a royalty rate of a low single-digit percentage based on net sales of any products under the License Agreements, once commercialized and (ii) WuXi Biologics at a royalty rate of a fraction of a single digit percentage of global net sales of WuXi Biologics Licensed Products manufactured by a third-party manufacturer.
We do not have any off-balance sheet arrangements that are material or reasonably likely to become material to our financial condition or results of operations.
Critical Accounting Policies and Significant Judgments and Estimates
Our management’s discussion and analysis of our financial condition and results of operations is based on our consolidated financial statements, which have been prepared in accordance with generally accepted accounting principles in the United States (GAAP). The preparation of these consolidated financial statements requires us to make estimates and assumptions that affect the reported amounts of assets and liabilities and the disclosure of contingent assets and liabilities at the date of the consolidated financial statements, as well as the reported revenues recognized and expenses incurred during the reporting periods. Our estimates are based on our historical experience and on various other factors that we believe are reasonable under the circumstances, the results of which form the basis for making judgments about the carrying value of assets and liabilities that are not readily apparent from other sources. Actual results may differ from these estimates under different assumptions or conditions.
We define our critical accounting policies as those accounting principles generally accepted in the United States of America that are most critical to the judgments and estimates used in the preparation of our consolidated financial statements. While our significant accounting policies are described in more detail in Note 2 to our consolidated financial statements appearing elsewhere in this Annual Report, we believe the following accounting policies used in preparation of our consolidated financial statements require the most significant judgements and estimates.
Research and Development Expense
Research and development costs are expensed as incurred. Research and development expenses consist of costs incurred in performing research and development activities, including salaries and bonuses, overhead costs, contract services and other related costs. The value of goods and services received from contract research organizations and contract manufacturing organizations in the reporting period are estimated based on the level of services performed, and progress in the period in cases when we have not received an invoice from the supplier. In circumstances where amounts have been paid in excess of costs incurred, we record a prepaid expense. When billing terms under these contracts do not coincide with the timing of when the work is performed, we are required to make estimates of outstanding obligations to those third parties as of period end.
136
Any accrual estimates are based on a number of factors, including our knowledge of the progress towards completion of the specific tasks to be performed, invoicing to date under the contracts, communication from the vendors of any actual costs incurred during the period that have not yet been invoiced and the costs included in the contracts. Significant judgments and estimates may be made in determining the accrued balances at the end of any reporting period. Actual results could differ from the estimates made by us.
Equity-Based Compensation
Prior to the Reorganization, we issued equity-based awards to employees, managers, executives, non-employees and service providers in the form of common units and incentive units. Subsequent to the Reorganization, we issued equity-based awards to employees, managers, executives, non-employees and service providers in the form of restricted common units and stock options. We account for equity-based compensation awards in accordance with FASB ASC Topic 718, Compensation—Stock Compensation (“ASC 718”).
Due to the absence of an active market for our common units or incentive units prior to the completion of the IPO, we utilized methodologies in accordance with the framework of the American Institute of Certified Public Accountants Accounting and Valuation Guide, Valuation of Privately-Held Company Equity Securities Issued as Compensation, to estimate the fair value of our common units and incentive units. The estimated fair value of the common units and incentive units was determined at each grant date based upon a variety of factors, including the illiquid nature of the common units, arm’s-length sales of our equity units (including preferred units), the effect of the rights and preferences of the preferred unit unitholders, and the prospects of a liquidity event. Among other factors are our financial position and historical financial performance, the status of technological developments within our research, the composition and ability of the current research and management team, an evaluation or benchmark of our competition, and the current business climate in the marketplace. Significant changes to the key assumptions underlying the factors used could have resulted in different fair values of the common units and incentive units at each valuation date.
Subsequent to the completion of the IPO, the fair value of our common stock underlying our equity awards is based on the quoted market price of our common stock on the grant date.
We estimate the fair value of our stock options using the Black-Scholes option pricing model, which uses as inputs the fair value of our common stock, and certain management estimates, including the expected stock price volatility, the expected term of the award, the risk-free rate, and expected dividends. Expected volatility is calculated based on reported volatility data for a representative group of publicly traded companies for which historical information is available. We select companies with comparable characteristics with historical share price information that approximates the expected term of the equity-based awards. We compute the historical volatility data using the daily closing prices for the selected companies’ shares during the equivalent period that approximates the calculated expected term of the stock options. We will continue to apply this method until a sufficient amount of historical information regarding the volatility of our stock price becomes available. The risk-free interest rate is based on the U.S. Treasury yield curve in effect at the time of grant commensurate with the expected term assumption. We use the simplified method, under which the expected term is presumed to be the midpoint between the vesting date and the end of the contractual term. We utilize this method due to lack of historical exercise data. The expected dividend yield is assumed to be zero as we have no current plans to pay any dividends on common stock. The fair value of the restricted stock units is calculated based on our stock price on the date of the grant.
137
We generally issue equity awards that are subject to either service-based vesting conditions and in limited instances, service-based and performance-based vesting conditions. Compensation expense for awards issued to grantees with service-based vesting conditions are recognized on a straight-line basis based on the grant date fair value over the associated requisite service period of the award, which is generally the vesting term. Compensation expense for awards to grantees with service-based and performance-based vesting conditions are recognized based on the grant-date fair value over the requisite service period using the accelerated attribution method to the extent achievement of the performance condition is probable. As of each reporting date, we estimate the probability that specified performance criteria will be met and do not recognize compensation expense until it is probable that the performance-based vesting condition will be achieved.
We evaluate whether an equity award should be classified and accounted for as a liability award or equity award for all equity-based compensation awards granted. As of December 31, 2023, all of our equity-based awards were equity classified. Forfeitures are recognized as they occur. We classify equity-based compensation expense in the accompanying consolidated statements of operations and comprehensive loss in the same manner in which the award recipient’s salary and related costs are classified or in which the award recipient’s service payments are classified, as applicable.
JOBS Act Transition Period and Smaller Reporting Company Status
We are an “emerging growth company” as defined in the Jumpstart Our Business Startups Act of 2012 (“JOBS Act”). Under the JOBS Act, an emerging growth company can take advantage of the extended transition period for complying with new or revised accounting standards and delay the adoption of certain accounting standards until those standards would otherwise apply to private companies. We have elected to avail ourselves of this exemption from complying with new or revised accounting standards and, therefore, will not be subject to the same new or revised accounting standards as other public companies that are not emerging growth companies. As a result, our financial statements may not be comparable to companies that comply with new or revised accounting pronouncements as of public company effective dates.
We are in the process of evaluating the benefits of relying on other exemptions and reduced reporting requirements under the JOBS Act. Subject to certain conditions, as an emerging growth company, we may rely on certain of these exemptions, including without limitation exemptions to the requirements for (i) providing an auditor’s attestation report on our system of internal controls over financial reporting pursuant to Section 404(b) of the Sarbanes-Oxley Act and (ii) complying with any requirement that may be adopted by the Public Company Accounting Oversight Board regarding mandatory audit firm rotation or a supplement to the auditor’s report providing additional information about the audit and the financial statements, known as the auditor discussion and analysis. We will remain an emerging growth company until the earlier to occur of (a) the last day of the fiscal year (A) following the fifth anniversary of the completion of our IPO, (B) in which we have total annual gross revenues of at least $1.235 billion or (C) in which we are deemed to be a “large accelerated filer” under the rules of the SEC, which means the market value of our common stock and non-voting common stock that is held by non-affiliates exceeds $700.0 million as of the prior June 30th, or (b) the date on which we have issued more than $1.0 billion in non-convertible debt during the prior three-year period.
We are also a “smaller reporting company,” as defined by Rule 12b-2 under the Securities Exchange Act of 1934, as amended (the “Exchange Act”), meaning that the market value of our common stock and non-voting common stock held by non-affiliates is less than $700.0 million and our annual revenue is less than $100.0 million during the most recently completed fiscal year. We may continue to be a smaller reporting company if either (i) the market value of our common stock and non-voting common stock held by non-affiliates is less than $250.0 million or (ii) our annual revenue is less than $100.0 million during the most recently completed fiscal year and the market value of our common stock and non-voting common stock held by non-affiliates is less than $700.0 million. If we are a smaller reporting company at the time we cease to be an emerging growth company, we may continue to rely on exemptions from certain disclosure requirements that are available to smaller reporting companies. Specifically, as a smaller reporting company we may choose to present only the two most recent fiscal years of audited financial statements in our Annual Report and, similar to emerging growth companies, smaller reporting companies have reduced disclosure obligations regarding executive compensation.
138
Recently Issued Accounting Pronouncements
We have reviewed all recently issued accounting standards and have determined that, other than as disclosed in Note 2 to our consolidated financial statements included elsewhere in this Annual Report, such standards are not expected to have a material impact on our consolidated financial statements or do not otherwise apply to our operations.
Item 7A. Quantitative and Qualitative Disclosures About Market Risk
We are a smaller reporting company, as defined in Rule 12b-2 of the Securities Exchange Act of 1934, as amended, for this reporting period and are not required to provide the information required under this Item.
139
Item 8. Financial Statements and Supplementary Data
Apogee Therapeutics, Inc.
INDEX TO FINANCIAL STATEMENTS
|
Page |
Report of the Independent Registered Public Accounting Firm (PCAOB ID: 42) |
141 |
142 |
|
143 |
|
144 |
|
Consolidated Statements of Preferred Units and Stockholders’ Equity/Members’ Deficit |
145 |
146 |
|
147 |
140
REPORT OF THE INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Stockholders of Apogee Therapeutics, Inc.
Opinion on the Financial Statements
We have audited the accompanying consolidated balance sheets of Apogee Therapeutics, Inc. (the Company) as of December 31, 2023 and 2022, the related consolidated statements of operations, comprehensive loss, preferred units and stockholders’ equity/members’ deficit and cash flows for the year ended December 31, 2023, and the period from February 4, 2022 (inception) to December 31, 2022, and the related notes (collectively referred to as the “consolidated financial statements”). In our opinion, the consolidated financial statements present fairly, in all material respects, the financial position of the Company at December 31, 2023 and 2022, and the results of its operations and its cash flows for the year ended December 31, 2023, and the period from February 4, 2022 (inception) to December 31, 2022, in conformity with U.S. generally accepted accounting principles.
Basis for Opinion
These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on the Company’s financial statements based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (PCAOB) and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. As part of our audits we are required to obtain an understanding of internal control over financial reporting but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion.
Our audits included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audits provide a reasonable basis for our opinion.
/s/ Ernst & Young LLP
Boston, Massachusetts
March 5, 2024
We have served as the Company’s auditor since 2023.
141
APOGEE THERAPEUTICS, INC.
CONSOLIDATED BALANCE SHEETS
(In thousands, except unit/share data)
|
|
DECEMBER 31, |
|
DECEMBER 31, |
||
|
|
2023 |
|
2022 |
||
Assets |
|
|
|
|
|
|
Current assets: |
|
|
|
|
|
|
Cash and cash equivalents |
|
$ |
118,316 |
|
$ |
151,890 |
Marketable securities |
|
|
277,143 |
|
|
— |
Prepaid expenses and other current assets |
|
|
2,950 |
|
|
165 |
Total current assets |
|
|
398,409 |
|
|
152,055 |
Property and equipment, net |
|
|
377 |
|
|
— |
Right-of-use asset, net |
|
|
2,217 |
|
|
— |
Other non-current assets |
|
|
401 |
|
|
— |
Total assets |
|
$ |
401,404 |
|
$ |
152,055 |
Liabilities, preferred units and stockholders' equity/members’ deficit |
|
|
|
|
|
|
Current liabilities: |
|
|
|
|
|
|
Accounts payable |
|
$ |
2,143 |
|
$ |
418 |
Lease liability |
|
|
1,101 |
|
|
— |
Accrued expenses |
|
|
17,314 |
|
|
9,562 |
Total current liabilities |
|
|
20,558 |
|
|
9,980 |
Long-term liabilities: |
|
|
|
|
|
|
Lease liability, net of current |
|
|
933 |
|
|
— |
Total liabilities |
|
|
21,491 |
|
|
9,980 |
Commitments and contingencies (Note 9) |
|
|
|
|
|
|
Series A Preferred Units; no units authorized, issued and outstanding at December 31, 2023; 20,000,000 units authorized, issued and outstanding as of December 31, 2022 |
|
|
— |
|
|
28,971 |
Series B Preferred Units; no units authorized, issued and outstanding at December 31, 2023; 45,089,212 units authorized, issued and outstanding as of December 31, 2022 |
|
|
— |
|
|
148,496 |
Stockholders’ equity/members’ deficit: |
|
|
|
|
|
|
Common Units; no units authorized, issued and outstanding at December 31, 2023; 5,000,000 units authorized, issued and outstanding as of December 31, 2022 |
|
|
— |
|
|
2,251 |
Incentive Units; no units authorized, issued and outstanding at December 31, 2023; 12,412,473 units authorized, 9,648,374 issued and 1,625,086 outstanding as of December 31, 2022 |
|
|
— |
|
|
2,142 |
Preferred Stock; 10,000,000 authorized, $0.00001 par value, no shares issued and outstanding at December 31, 2023; No shares authorized, issued and outstanding at December 31, 2022 |
|
|
— |
|
|
— |
Common Stock; 400,000,000 authorized, $0.00001 par value, 50,655,671 issued and 48,338,769 outstanding as of December 31, 2023; No shares authorized, issued and outstanding at December 31, 2022 |
|
|
— |
|
|
— |
Additional paid-in capital |
|
|
503,354 |
|
|
— |
Accumulated other comprehensive income |
|
|
329 |
|
|
— |
Accumulated deficit |
|
|
(123,770) |
|
|
(39,785) |
Total stockholders’ equity/members’ deficit |
|
|
379,913 |
|
|
(35,392) |
Total liabilities, preferred units and stockholders’ equity/members’ deficit |
|
$ |
401,404 |
|
$ |
152,055 |
The accompanying notes are an integral part of these consolidated financial statements.
142
APOGEE THERAPEUTICS, INC.
CONSOLIDATED STATEMENTS OF OPERATIONS
(In thousands, except share and per share data)
|
|
|
|
|
PERIOD FROM |
|
|
|
YEAR ENDED |
|
FEBRUARY 4, 2022 |
||
|
|
DECEMBER 31, |
|
(INCEPTION) TO |
||
|
|
2023 |
|
DECEMBER 31, 2022 |
||
Operating expenses: |
|
|
|
|
|
|
Research and development (1) |
|
$ |
68,424 |
|
$ |
27,786 |
General and administrative (2) |
|
|
24,579 |
|
|
2,941 |
Total operating expenses |
|
|
93,003 |
|
|
30,727 |
Loss from operations |
|
|
(93,003) |
|
|
(30,727) |
Other income (expense), net: |
|
|
|
|
|
|
Interest income, net |
|
|
9,018 |
|
|
92 |
Other financing expense, net: |
|
|
— |
|
|
(9,150) |
Total other income (expense), net |
|
|
9,018 |
|
|
(9,058) |
Net loss |
|
$ |
(83,985) |
|
$ |
(39,785) |
Net loss per share, basic and diluted |
|
$ |
(3.36) |
|
$ |
(16.16) |
Weighted-average common shares outstanding, basic and diluted |
|
|
25,005,774 |
|
|
2,462,236 |
| (1) | Includes related-party amounts of $26,285 for the year ended December 31, 2023 and $23,326 for the period from February 4, 2022 (inception) to December 31, 2022. |
| (2) | Includes related-party amounts of $33 for the year ended December 31, 2023 and $317 for the period from February 4, 2022 (inception) to December 31, 2022. |
The accompanying notes are an integral part of these consolidated financial statements.
143
APOGEE THERAPEUTICS, INC.
CONSOLIDATED STATEMENTS OF COMPREHENSIVE LOSS
(In thousands)
|
|
|
|
|
PERIOD FROM |
|
|
|
|
|
FEBRUARY 4, 2022 |
||
|
|
YEAR ENDED |
|
(INCEPTION) TO |
||
|
|
DECEMBER 31, 2023 |
|
DECEMBER 31, 2022 |
||
|
|
|
|
|
|
|
Net loss |
|
$ |
(83,985) |
|
$ |
(39,785) |
Change in unrealized gains on marketable securities, net of tax |
|
|
329 |
|
|
— |
Comprehensive loss |
|
$ |
(83,656) |
|
$ |
(39,785) |
The accompanying notes are an integral part of these consolidated financial statements.
144
APOGEE THERAPEUTICS, INC.
CONSOLIDATED STATEMENTS OF PREFERRED UNITS AND STOCKHOLDERS’ EQUITY/MEMBERS’ DEFICIT
(In thousands, except unit/share data)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Total |
|
|
|
Series A |
|
Series B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accumulated |
|
Stockholders’ |
|||||||||||||||||
|
|
Preferred |
|
Preferred |
|
|
Common |
|
Incentive |
|
Common |
|
Additional |
|
|
|
Other |
|
Equity / |
|||||||||||||||||||
|
|
Units |
|
Units |
|
|
Units |
|
Units |
|
Stock |
|
Paid-in |
|
Accumulated |
|
Comprehensive |
|
Members’ |
|||||||||||||||||||
|
|
Units |
|
Amount |
|
Units |
|
Amount |
|
|
Units |
|
Amount |
|
Units |
|
Amount |
|
Units |
|
Amount |
|
Capital |
|
Deficit |
|
Income |
|
Deficit |
|||||||||
Balance at February 4, 2022 (inception) |
|
— |
|
$ |
— |
|
— |
|
$ |
— |
|
|
— |
|
$ |
— |
|
— |
|
$ |
— |
|
— |
|
$ |
— |
|
$ |
— |
|
$ |
— |
|
$ |
— |
|
$ |
— |
Issuance of Common Units in payment of option fee |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
5,000,000 |
|
|
2,251 |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
2,251 |
Issuance of Series A preferred units − initial closing, net of tranche rights of $1,050 and issuance costs of $179 |
|
5,000,000 |
|
|
3,771 |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
Issuance of Series A preferred units - subsequent closings, inclusive of tranche option liability |
|
15,000,000 |
|
|
25,200 |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
Issuance of Series B preferred units - initial closing, net of issuance costs of $504 |
|
— |
|
|
— |
|
45,089,212 |
|
|
148,496 |
|
|
— |
|
|
— |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
Equity Based Compensation Expense |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
1,625,086 |
|
|
2,142 |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
2,142 |
Net loss |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
(39,785) |
|
|
— |
|
|
(39,785) |
Balance at December 31, 2022 |
|
20,000,000 |
|
$ |
28,971 |
|
45,089,212 |
|
$ |
148,496 |
|
|
5,000,000 |
|
$ |
2,251 |
|
1,625,086 |
|
$ |
2,142 |
|
— |
|
$ |
— |
|
$ |
— |
|
$ |
(39,785) |
|
$ |
— |
|
$ |
(35,392) |
Vesting of incentive units |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
922,338 |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
Conversion of preferred, common, and incentive units into common stock |
|
(20,000,000) |
|
|
(28,971) |
|
(45,089,212) |
|
|
(148,496) |
|
|
(5,000,000) |
|
|
(2,251) |
|
(2,547,424) |
|
|
(4,686) |
|
27,597,438 |
|
|
— |
|
|
184,404 |
|
|
— |
|
|
— |
|
|
177,467 |
Common stock issued in IPO, net of issuance costs of $29,666 |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
— |
|
|
— |
|
20,297,500 |
|
|
— |
|
|
315,391 |
|
|
— |
|
|
— |
|
|
315,391 |
Vesting of restricted stock |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
— |
|
|
— |
|
443,831 |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
Equity-based compensation expense |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
— |
|
|
2,544 |
|
— |
|
|
— |
|
|
3,559 |
|
|
— |
|
|
— |
|
|
6,103 |
Change in unrealized gain on marketable securities, net of tax |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
329 |
|
|
329 |
Net loss |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
(83,985) |
|
|
— |
|
|
(83,985) |
Balance at December 31, 2023 |
|
— |
|
$ |
— |
|
— |
|
$ |
— |
|
|
— |
|
$ |
— |
|
— |
|
$ |
— |
|
48,338,769 |
|
$ |
— |
|
$ |
503,354 |
|
$ |
(123,770) |
|
$ |
329 |
|
$ |
379,913 |
The accompanying notes are an integral part of these consolidated financial statements.
145
APOGEE THERAPEUTICS, INC.
CONSOLIDATED STATEMENTS OF CASH FLOWS
(In thousands)
|
|
YEAR |
|
FEBRUARY 4, 2022 |
||
|
|
ENDED |
|
(INCEPTION) TO |
||
|
|
DECEMBER 31, 2023 |
|
DECEMBER 31, 2022 |
||
Cash flows from operating activities: |
|
|
|
|
|
|
Net loss |
|
$ |
(83,985) |
|
$ |
(39,785) |
Adjustments to reconcile net loss to net cash provided by (used in) operating activities: |
|
|
|
|
|
|
Equity-based compensation expense |
|
|
6,103 |
|
|
2,142 |
Loss on remeasurement of tranche option liability |
|
|
— |
|
|
9,150 |
Non-cash research and development license expense |
|
|
— |
|
|
2,251 |
Amortization of discounts on marketable securities |
|
|
(3,071) |
|
|
— |
Non-cash lease expense |
|
|
87 |
|
|
— |
Changes in operating assets and liabilities: |
|
|
|
|
|
|
Prepaid expenses and other current assets |
|
|
(2,785) |
|
|
(165) |
Other assets |
|
|
(107) |
|
|
— |
Accounts payable |
|
|
1,613 |
|
|
418 |
Operating lease liability |
|
|
(270) |
|
|
— |
Accrued expenses |
|
|
7,654 |
|
|
9,562 |
Net cash used in operating activities |
|
|
(74,761) |
|
|
(16,427) |
Cash flows from investing activities: |
|
|
|
|
|
|
Purchases of marketable securities |
|
|
(303,743) |
|
|
— |
Maturities of marketable securities |
|
|
30,000 |
|
|
— |
Purchases of property and equipment |
|
|
(167) |
|
|
— |
Net cash used in investing activities |
|
|
(273,910) |
|
|
— |
Cash flows from financing activities: |
|
|
|
|
|
|
Proceeds from issuance of Series A Preferred Units and the tranche option, net |
|
|
— |
|
|
19,821 |
Proceeds from issuance of Series B Preferred Units, net |
|
|
— |
|
|
148,496 |
Proceeds from issuance of common stock, net of issuance costs |
|
|
315,391 |
|
|
— |
Net cash provided by financing activities |
|
|
315,391 |
|
|
168,317 |
(Decrease) increase in cash, cash equivalents and restricted cash |
|
|
(33,280) |
|
|
151,890 |
Cash, cash equivalents and restricted cash, beginning of period |
|
|
151,890 |
|
|
— |
Cash, cash equivalents and restricted cash, end of period |
|
$ |
118,610 |
|
$ |
151,890 |
Supplemental disclosures of non-cash activities: |
|
|
|
|
|
|
Exchange of 72,636,636 preferred, common, and incentive units in connection with the Reorganization (Note 1) |
|
$ |
184,404 |
|
$ |
— |
Settlement of Series A Preferred Units tranche obligation |
|
$ |
— |
|
$ |
10,200 |
Operating lease right-of-use asset obtained in exchange for operating lease liability |
|
$ |
2,304 |
|
$ |
— |
Purchases of property and equipment included in accounts payable |
|
$ |
210 |
|
$ |
— |
Reconciliation of cash, cash equivalents and restricted cash: |
|
|
|
|
|
|
Cash and cash equivalents |
|
$ |
118,316 |
|
$ |
151,890 |
Restricted cash |
|
|
294 |
|
|
— |
Total |
|
$ |
118,610 |
|
$ |
151,890 |
The accompanying notes are an integral part of these consolidated financial statements.
146
APOGEE THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
1.Nature of the Business
Apogee Therapeutics, Inc., together with its consolidated subsidiary (collectively, “Apogee” or the “Company”), a successor to Apogee Therapeutics, LLC, is a biotechnology company seeking to develop differentiated biologics for the treatment of atopic dermatitis, asthma, chronic obstructive pulmonary disease and related inflammatory and immunology indications with high unmet need. The Company’s antibody programs are designed to overcome limitations of existing therapies by leveraging clinically validated mechanisms and incorporating advanced antibody engineering to optimize half-life and other properties designed.
The Company commenced its operations in February 2022 as a Delaware limited liability company named Apogee Therapeutics, LLC. The Company was founded by leading healthcare investors, Fairmount Funds and Venrock Healthcare Capital Partners and has since assembled a management team of drug developers with significant experience in clinical development. As a result of the Reorganization (as defined below) and in connection with the Company’s initial public offering (“IPO”) in July 2023, the Company directly wholly owns the assets of Apogee Therapeutics, LLC, including the stock of its subsidiary. In addition, the Company engages third parties, including Paragon Therapeutics, Inc. (“Paragon”), who is also a related party, to perform ongoing research and development and other services on its behalf.
In February 2022, the Company entered into an antibody discovery and option agreement with Paragon, which was subsequently amended in November 2022 (as amended, the “2022 Option Agreement”). Under the terms of the 2022 Option Agreement, Paragon identifies, evaluates and develops antibodies directed against certain mutually agreed therapeutic targets of interest to the Company. The 2022 Option Agreement initially included two selected targets, IL-13 and IL-4Rα, and was subsequently amended in November 2022 to include an additional selected target, OX40L. Under the 2022 Option Agreement, the Company has the exclusive option to, on a research program-by-research program basis, be granted an exclusive, worldwide license to all of Paragon’s rights, title and interest in and to the intellectual property resulting from the applicable research program to develop, manufacture and commercialize the antibodies and products directed to the selected targets. In November 2023, the Company entered into an additional antibody discovery and option agreement with Paragon (the “2023 Option Agreement”). Under the terms of the 2023 Option Agreement, Paragon identifies, evaluates and develops antibodies directed against certain mutually agreed therapeutic targets of interest to the Company.
In November 2022, the Company exercised its option available under the 2022 Option Agreement with respect to the IL-13 Research Program (as defined below) and, in April 2023, the Company exercised its options available under the 2022 Option Agreement with respect to the IL-4Rα Research Program and OX40L Research Program. Upon such exercises, the parties entered into associated license agreements for each target. Under the terms of each license agreement, Paragon granted to the Company an exclusive, worldwide, royalty-bearing, sublicensable right and license with respect to certain information, patent rights and sequence information related to antibodies directed at the respective target to use, make, sell, import, export and otherwise exploit the antibodies directed at the respective target. The Company is solely responsible for the development, manufacture and commercialization of IL-13, IL-4Rα and OX40L products at its own cost and expense.
On July 13, 2023, the Company completed a reorganization, pursuant to which the members of Apogee Therapeutics, LLC contributed their units in Apogee Therapeutics, LLC to Apogee Therapeutics, Inc. in exchange for shares of common stock or non-voting common stock of Apogee Therapeutics, Inc. and Apogee Therapeutics, LLC became a wholly-owned subsidiary of Apogee Therapeutics, Inc. (the “Reorganization”), as follows:
| ● | holders of Series A Preferred Units of Apogee Therapeutics, LLC received 7,678,000 shares of non-voting common stock of Apogee Therapeutics, Inc.; |
| ● | holders of Series B Preferred Units of Apogee Therapeutics, LLC received 11,501,108 shares of common stock and 5,808,642 shares of non-voting common stock of Apogee Therapeutics, Inc.; |
147
| ● | holders of common units of Apogee Therapeutics, LLC received 1,919,500 shares of common stock of Apogee Therapeutics, Inc.; |
| ● | holders of vested incentive units of Apogee Therapeutics, LLC received 690,188 shares of common stock of Apogee Therapeutics, Inc.; and |
| ● | holders of unvested incentive units of Apogee Therapeutics, LLC received 2,779,358 shares of restricted common stock of Apogee Therapeutics, Inc. |
On July 18, 2023, the Company completed its IPO, pursuant to which it issued and sold an aggregate of 20,297,500 shares of its common stock (inclusive of 2,647,500 shares pursuant to the exercise of the underwriters’ overallotment option in full) at the IPO price of $17.00 per share for net cash proceeds of $315.4 million, after deducting underwriting discounts and commissions and other offering expenses. The shares of Apogee Therapeutics, Inc. began trading on the Nasdaq Global Market on July 14, 2023 under the symbol APGE.
The Company is subject to risks and uncertainties common to early stage companies in the biotechnology industry, including, but not limited to, completing preclinical studies and clinical trials, obtaining regulatory approval for its programs, market acceptance of products, development by competitors of new technological innovations, dependence on key personnel, the ability to attract and retain qualified employees, reliance on third-party organizations, protection of proprietary technology, compliance with government regulations, and the ability to raise additional capital to fund operations. The Company’s two most advanced programs currently under development, APG777 and APG808, as well as other programs, will require significant additional research and development efforts, including extensive preclinical and clinical testing and regulatory approval prior to commercialization. These efforts require significant amounts of additional capital, adequate personnel and infrastructure, and extensive compliance reporting capabilities. Even if the Company’s development efforts are successful, it is uncertain when, if ever, the Company will realize revenue from product sales. The Company has primarily funded its operations with proceeds from the sales of preferred units and common stock and has not generated any revenue since inception.
As a result, the Company will need substantial additional funding to support its continued operations and growth strategy. Until such a time as the Company can generate significant revenue from product sales, if ever, the Company expects to finance its operations through the sale of equity, debt financings or other capital sources, including collaborations with other companies or other strategic transactions. The Company may be unable to raise additional funds or enter into such other agreements on favorable terms, or at all. If the Company fails to raise capital or enter into such agreements as, and when, needed, the Company may have to significantly delay, scale back or discontinue the development and commercialization of one or more of its programs.
Company Liquidity
The Company has evaluated whether there are conditions and events, considered in the aggregate, that raise substantial doubt about its ability to continue as a going concern within one year after the date that the accompanying consolidated financial statements are issued. The Company had an accumulated deficit of $123.8 million as of December 31, 2023. Further, the Company incurred a net loss of $84.0 million and experienced negative cash flows from operations of $74.8 million for the year ended December 31, 2023. Based on the Company’s current operating plan, it estimates that its existing cash and cash equivalents of $118.3 million, and marketable securities of $277.1 million as of December 31, 2023 will be sufficient to enable the Company to fund its operating expenses and capital requirements through at least the next twelve months from the issuance of these consolidated financial statements.
The Company is subject to those risks associated with any biotechnology company that has substantial expenditures for research and development. There can be no assurance that the Company’s research and development projects will be successful, that products developed will obtain necessary regulatory approval, or that any approved product will be commercially viable. In addition, the Company operates in an environment of rapid technological change and is largely dependent on the services of its employees and consultants. If the Company fails to become profitable or is unable to sustain profitability on a continuing basis, then it may be unable to continue its operations at planned levels and be forced to reduce its operations.
148
2.Summary of Significant Accounting Policies
Basis of Presentation
The consolidated financial statements prior to the Reorganization include the accounts of Apogee Therapeutics, LLC and its wholly-owned subsidiary. The consolidated financial statements subsequent to the Reorganization include the accounts of Apogee Therapeutics, Inc. and its wholly-owned subsidiary.
These consolidated financial statements have been prepared in conformity with accounting principles generally accepted in the United States of America (“GAAP”). Any reference in these notes to applicable guidance is meant to refer to the authoritative GAAP as found in the Accounting Standards Codification (“ASC”) and Accounting Standards Updates of the Financial Accounting Standards Board (“FASB”). In the Company’s management opinion, the information furnished in these consolidated financial statements reflect all adjustments, all of which are of a normal and recurring nature, necessary for a fair presentation of the financial position and results of operations for the reported periods. The Company considers events or transactions that occur after the balance sheet date but before the financial statements are issued to provide additional evidence relative to certain estimates or to identify matters that require additional disclosure.
Principles of Consolidation
The accompanying consolidated financial statements include the accounts of Apogee Therapeutics, Inc. and its wholly-owned subsidiary, Apogee Biologics, Inc. All intercompany balances and transactions have been eliminated in consolidation.
Use of Estimates
The preparation of financial statements in conformity with GAAP requires management to make estimates and assumptions that affect the reported amounts in the financial statements and accompanying notes. Actual results could materially differ from those estimates. Management considers many factors in selecting appropriate financial accounting policies and controls, and in developing the estimates and assumptions that are used in the preparation of these financial statements. Management must apply significant judgment in this process. In addition, other factors may affect estimates, including: expected business and operational changes, sensitivity and volatility associated with the assumptions used in developing estimates, and whether historical trends are expected to be representative of future trends. The estimation process often may yield a range of potentially reasonable estimates of the ultimate future outcomes and management must select an amount that falls within that range of reasonable estimates. Significant estimates relied upon in preparing the accompanying consolidated financial statements include, among others: research and development expenses and related prepaid or accrued costs, the valuation of equity-based compensation awards and related expense, the valuation of preferred units and preferred unit tranche rights.
Segments
The Company has one operating segment and one reporting unit. The Company’s chief operating decision maker, its Chief Executive Officer, manages the Company’s operations on a consolidated basis for the purposes of assessing performance and allocating resources. All of the Company’s assets are located in the United States.
Deferred Offering Costs
The Company capitalizes certain legal, accounting and other third-party fees that are directly associated with in-process equity financings as deferred offering costs until such financings are consummated. After the consummation of the equity financing, these costs are recorded in stockholders’ equity/members’ deficit as a reduction of additional paid-in capital or the associated preferred unit account, as applicable. In the event the offering is terminated, all capitalized deferred offering costs are expensed. As of December 31, 2023, the Company had no deferred offering costs.
149
Fair Value of Financial Instruments
The Company is required to disclose information on all assets and liabilities reported at fair value that enables an assessment of the inputs used in determining the reported fair values. FASB ASC Topic 820, Fair Value Measurements and Disclosures (“ASC 820”), establishes a hierarchy of inputs used in measuring fair value that maximizes the use of observable inputs and minimizes the use of unobservable inputs by requiring that the observable inputs be used when available. Observable inputs are inputs that market participants would use in pricing the asset or liability based on market data obtained from sources independent of the Company. Unobservable inputs are inputs that reflect the Company’s assumptions about the inputs that market participants would use in pricing the asset or liability and are developed based on the best information available in the circumstances. The fair value hierarchy applies only to the valuation inputs used in determining the reported fair value of the investments and is not a measure of the investment credit quality. The three levels of the fair value hierarchy are described below:
Level 1—Valuations based on quoted prices in active markets for identical assets or liabilities that the Company has the ability to access at the measurement date.
Level 2—Valuations based on quoted prices for similar assets or liabilities in markets that are not active or for which all significant inputs are observable, either directly or indirectly.
Level 3—Valuations that require inputs that reflect the Company’s own assumptions that are both significant to the fair value measurement and unobservable.
To the extent that valuation is based on models or inputs that are less observable or unobservable in the market, the determination of fair value requires more judgment. A financial instrument’s level within the fair value hierarchy is based on the lowest level of any input that is significant to the fair value measurement.
Items measured at fair value on a recurring basis as of December 31, 2023 include cash equivalents and marketable securities (Notes 3 and 4). The carrying amounts reflected in the accompanying consolidated balance sheets for prepaid expenses and other current assets, accounts payable and accrued expenses approximate their fair values due to their short-term nature.
Property and Equipment, net
Property and equipment are recorded at cost. Depreciation is calculated using the straight-line method over the following estimated useful lives of the assets:
|
|
ESTIMATED |
|
Laboratory equipment |
|
5 years |
|
Upon disposal, retirement or sale, the cost of assets disposed of and the related accumulated depreciation are removed from the accounts and any resulting gain or loss is included in the results of operations. Expenditures for repairs and maintenance that do not improve or extend the lives of the respective assets are charged to expense as incurred.
Preferred Units Tranche Option Freestanding Financial Instrument
The unit purchase agreement for the Company’s Series A Preferred Units (see Note 10) provided for three subsequent closings following the initial closing, which such subsequent closings were subject to approval of the Company’s Board of Managers (the “Board of Managers”), which was controlled by the holders of the Series A Preferred Units (“Tranche Options”).
The Company classified these Tranche Options as an asset or liability as each preferred unit Tranche Option is a freestanding financial instrument that may require the Company to transfer assets upon satisfaction of certain conditions. Each preferred unit Tranche Option was initially recorded at fair value upon the date of issuance of each preferred unit tranche option and was subsequently remeasured to fair value at each reporting date.
150
Changes in the fair value of the Tranche Option were recognized as a component of other income (expense), net in the accompanying consolidated statement of operations and comprehensive loss. Changes in the fair value of the Tranche Option were recognized until each respective Tranche Option was settled. As of December 31, 2023, all Tranche Options issued in connection with the Series A Preferred Unit purchase agreement had been fully settled.
Preferred Units
The Company has classified the preferred units as temporary equity in the accompanying consolidated balance sheets because the units could become effectively settled for cash or other assets due to certain contingent event clauses that are outside of the Company’s control. The preferred units are not currently settleable, but are entitled to a distribution of available proceeds upon a change of control or a sale event which is a bona fide, negotiated transaction in which the Company has determined to affect a change of control. Because the occurrence of a change of control and a sale event is not currently probable, the carrying values of the preferred units are not being accreted to their redemption values. Subsequent adjustments to the carrying values of the preferred units would be made only when the change of control or sale event becomes probable.
Research and Development Expense
Research and development costs are expensed as incurred. Research and development expenses consist of costs incurred in performing research and development activities, including salaries and bonuses, overhead costs, contract services and other related costs. The value of goods and services received from contract research organizations and contract manufacturing organizations in the reporting period are estimated based on the level of services performed, and progress in the period in cases when the Company has not received an invoice from the supplier. In circumstances where amounts have been paid in excess of costs incurred, the Company records a prepaid expense. When billing terms under these contracts do not coincide with the timing of when the work is performed, the Company is required to make estimates of outstanding obligations to those third parties as of period end. Any accrual estimates are based on a number of factors, including the Company’s knowledge of the progress towards completion of the specific tasks to be performed, invoicing to date under the contracts, communication from the vendors of any actual costs incurred during the period that have not yet been invoiced and the costs included in the contracts. Significant judgments and estimates may be made in determining the accrued balances at the end of any reporting period. Actual results could differ from the estimates made by the Company.
Income Taxes
Income taxes are recorded in accordance with FASB ASC Topic 740, Income Taxes (“ASC 740”), which provides for deferred taxes using an asset and liability approach. The Company recognizes deferred tax assets and liabilities for the expected future tax consequences of events that have been included in the financial statements or tax returns. Deferred tax assets and liabilities are determined based on the difference between the financial statement and tax basis of assets and liabilities using enacted tax rates in effect for the year in which the differences are expected to reverse.
Valuation allowances are provided if, based upon the weight of available evidence, it is more likely than not that some or all of the deferred tax assets will not be realized. The Company makes estimates and judgments about future taxable income based on assumptions that are consistent with the Company’s plans and estimates. Should the actual amounts differ from these estimates, the amount of the Company’s valuation allowance could be materially impacted. Changes in these estimates may result in significant increases or decreases to the tax provision in a period in which such estimates are changed, which in turn would affect net income or loss.
The Company accounts for uncertain tax positions in accordance with the provisions of ASC 740. When uncertain tax positions exist, the Company recognizes the tax benefit to the extent that the position is more likely than not to be sustained on examination by the taxing authorities based on the technical merits of the position as well as consideration of the available facts and circumstances. The Company records interest and penalties related to uncertain tax positions, if applicable, as a component of income tax expense.
151
Cash and Cash Equivalents
The Company considers all highly liquid investments purchased with original final maturities of three months or less from the date of purchase to be cash equivalents. Cash and cash equivalents include cash held in banks and amounts held in interest-bearing money market funds and U.S. treasury securities.
Marketable Securities
The Company’s investments are comprised of U.S. government agency securities and U.S. treasury securities. Investments are classified at the time of purchase, based on management’s intent, as held-to-maturity, available-for-sale, or trading. All of the Company’s marketable security investments are classified as available-for-sale securities and are reported at fair market value using quoted prices in active markets for similar securities. The cost of securities sold is determined on a specific identification basis, and realized gains and losses are included as a component of other income within the consolidated statements of operations and comprehensive loss.
The Company assesses its available-for-sale securities under the available-for-sale security impairment model in ASU 2016-13, Financial Instruments-Credit Losses (Topic 326): Measurement of Credit Losses on Financial Statements as of each reporting date in order to determine if a portion of any decline in fair value below carrying value is the result of a credit loss for its available-for-sale securities. The Company records credit losses for its available-for-sale securities in the consolidated statements of operations and comprehensive loss as credit loss expense, which is limited to the difference between the fair value and the amortized cost of the security. To date, the Company has not recorded any credit losses on its available-for-sale securities. Declines in fair value below carrying value attributable to non-credit related factors are recorded as accumulated other comprehensive loss, which is a separate component of stockholders’ equity.
The Company classifies its available-for-sale securities as current assets on the consolidated balance sheets as they mature within one year from the balance sheet date.
Leases
The Company determines the initial classification and measurement of its right-of-use assets and lease liabilities at the lease commencement date and thereafter if modified. The lease term includes any renewal options and termination options that the Company is reasonably assured to exercise. The present value of lease payments is determined by using the interest rate implicit in the lease, if that rate is readily determinable; otherwise, the Company uses its incremental borrowing rate. The incremental borrowing rate is determined by using the rate of interest that the Company would pay to borrow on a collateralized basis an amount equal to the lease payments for a similar term and in a similar economic environment.
Fixed lease expense for operating leases is recognized on a straight-line basis, unless the right-of-use assets have been impaired, over the reasonably assured lease term based on the total lease payments and is included in operating expenses in the statements of operations and comprehensive loss.
Equity-Based Compensation
Prior to the Reorganization, the Company issued equity-based awards to employees, managers, executives, non-employees and service providers in the form of common units and incentive units. Subsequent to the Reorganization, the Company issued equity-based awards to employees, managers, executives, non-employees and service providers in the form of restricted common units and stock options. The Company accounts for equity-based compensation awards in accordance with FASB ASC Topic 718, Compensation—Stock Compensation (“ASC 718”).
Due to the absence of an active market for the Company’s common units or incentive units prior to the completion of the IPO, the Company utilized methodologies in accordance with the framework of the American Institute of Certified Public Accountants Accounting and Valuation Guide, Valuation of Privately-Held Company Equity Securities Issued as Compensation, to estimate the fair value of its common units and incentive units. The estimated fair value of the common units and incentive units was determined at each grant date based upon a variety of factors, including the illiquid nature of the common units, arm’s-length sales of the Company’s equity units (including preferred units), the effect of the rights and preferences of the preferred unit unitholders, and the prospects of a liquidity event.
152
Among other factors are the Company’s financial position and historical financial performance, the status of technological developments within the Company’s research, the composition and ability of the current research and management team, an evaluation or benchmark of the Company’s competition, and the current business climate in the marketplace. Significant changes to the key assumptions underlying the factors used could have resulted in different fair values of the common units and incentive units at each valuation date.
Subsequent to the completion of the IPO, the fair value of the Company’s common stock underlying its equity awards is based on the quoted market price of the Company’s common stock on the grant date.
The Company estimates the fair value of its stock options using the Black-Scholes option pricing model, which uses as inputs the fair value of the Company’s common stock, and certain management estimates, including the expected stock price volatility, the expected term of the award, the risk-free rate, and expected dividends. Expected volatility is calculated based on reported volatility data for a representative group of publicly traded companies for which historical information is available. The Company selects companies with comparable characteristics with historical share price information that approximates the expected term of the equity-based awards. The Company computes the historical volatility data using the daily closing prices for the selected companies’ shares during the equivalent period that approximates the calculated expected term of the stock options. The Company will continue to apply this method until a sufficient amount of historical information regarding the volatility of its stock price becomes available. The risk-free interest rate is based on the U.S. Treasury yield curve in effect at the time of grant commensurate with the expected term assumption. The Company uses the simplified method, under which the expected term is presumed to be the midpoint between the vesting date and the end of the contractual term. The Company utilizes this method due to lack of historical exercise data. The expected dividend yield is assumed to be zero as the Company has no current plans to pay any dividends on common stock. The fair value of the RSUs are based on the Company’s stock price on the date of the grant.
The Company generally issues equity awards that are subject to either service-based vesting conditions and in limited instances, service-based and performance-based vesting conditions. Compensation expense for awards issued to grantees with service-based vesting conditions are recognized on a straight-line basis based on the grant date fair value over the associated requisite service period of the award, which is generally the vesting term. Compensation expense for awards to grantees with service-based and performance-based vesting conditions are recognized based on the grant-date fair value over the requisite service period using the accelerated attribution method to the extent achievement of the performance condition is probable. As of each reporting date, the Company estimates the probability that specified performance criteria will be met and does not recognize compensation expense until it is probable that the performance-based vesting condition will be achieved.
The Company evaluates whether an equity award should be classified and accounted for as a liability award or equity award for all equity-based compensation awards granted. As of December 31, 2023, all of the Company’s equity-based awards were equity classified. Forfeitures are recognized as they occur. The Company classifies equity-based compensation expense in the accompanying consolidated statements of operations and comprehensive loss in the same manner in which the award recipient’s salary and related costs are classified or in which the award recipient’s service payments are classified, as applicable.
Concentrations of Credit Risk and Significant Suppliers
Financial instruments that potentially expose the Company to credit risk primarily consist of cash and cash equivalents, restricted cash, and marketable securities. The Company’s investment portfolio is comprised of money market funds and debt securities issued by U.S. government. The Company maintains its deposits with accredited financial institutions and, consequently, the Company does not believe it is subject to unusual credit risk beyond the normal credit risk associated with commercial banking relationships. Bank accounts in the United States are insured by the Federal Deposit Insurance Corporation (“FDIC”) up to $250,000. As of December 31, 2023 and December 31, 2022, predominantly all of the Company’s primary operating accounts significantly exceeded the FDIC limits.
153
The Company is dependent on third-party organizations to research, develop, manufacture and process its product candidates for its development programs. In particular, the Company relies on one third-party contract manufacturer to produce and process its two most advanced programs, APG777 and APG808, for preclinical and clinical activities. The Company expects to continue to be dependent on a small number of manufacturers to supply it with its requirements for all products. The Company’s research and development programs could be adversely affected by a significant interruption in the supply of the necessary materials. A significant amount of the Company’s research and development activities are performed under its agreements with Paragon (see Note 8).
Off-Balance Sheet Arrangements
As of December 31, 2023 and December 31, 2022, the Company had no off-balance sheet risks such as foreign exchange contracts, option contracts or other foreign hedging arrangements.
Comprehensive Loss
Comprehensive loss includes net loss as well as other changes in stockholders’ equity that result from transactions and events other than those with stockholders. The Company’s unrealized gains and losses on marketable securities represent the only component of other comprehensive loss that are excluded from the reported net loss and that are presented in the consolidated statements of comprehensive loss.
Net Loss Per Share
The Company follows the two-class method when computing net loss per share. Prior to the Reorganization, the Company issued units that met the definition of participating securities, including the Company’s Series A Preferred Units, the Series B Preferred Units, and vested incentive units (each a participating security), and subsequent to the Reorganization, the Company has two classes of common stock outstanding comprised of voting and non-voting shares. The rights of the holders of voting and non-voting shares are identical, except with respect to voting and conversion. Each share of non-voting stock may be converted into one share of voting stock at any time at the option of the stockholder, subject to certain beneficial ownership limitations. The two-class method determines net loss per unit and net loss per share for each class of common and participating securities according to dividends declared or accumulated and participation rights in undistributed earnings. The two-class method requires income for the period to be allocated between common and participating securities based upon their respective rights to share in the income as if all income for the period had been distributed. Prior to the Reorganization, during periods of loss, there was no allocation required under the two-class method since the participating securities did not have a contractual obligation to fund the losses of the Company. Subsequent to the Reorganization, net loss per share for each class of common stock issued is the same as they are entitled to the same liquidation and dividend rights.
Prior to the Reorganization, the Company calculated basic net loss per common share by dividing net loss by the weighted-average number of common units outstanding for the period. Subsequent to the Reorganization, the Company calculates basic net loss per common share by dividing net loss by the weighted-average number of common shares outstanding for the period. The Company has generated a net loss in the periods presented so the basic and diluted net loss per unit and net loss per share are the same as the inclusion of the potentially dilutive securities would be anti-dilutive.
For periods presented that include the Reorganization, including the year ended December 31, 2023, the weighted-average shares of common stock outstanding include the weighted average number of common units outstanding prior to the Reorganization.
154
3.Marketable Securities
The Company did not hold any available-for-sale securities as of December 31, 2022. The following is a summary of the Company’s investing portfolio as of December 31, 2023 (in thousands):
|
|
AS OF DECEMBER 31, 2023 |
||||||||||
|
|
|
|
UNREALIZED |
|
|
||||||
|
|
COST |
|
GAINS |
|
LOSSES |
|
FAIR VALUE |
||||
Marketable securities: |
|
|
|
|
|
|
|
|
|
|
|
|
U.S. treasury securities |
|
$ |
123,836 |
|
$ |
140 |
|
$ |
(2) |
|
$ |
123,974 |
Debt securities issued by U.S. government agencies |
|
|
152,978 |
|
|
199 |
|
|
(8) |
|
|
153,169 |
|
|
$ |
276,814 |
|
$ |
339 |
|
$ |
(10) |
|
$ |
277,143 |
As of December 31, 2023, the Company had five securities with a total fair market value of $62.5 million in an unrealized loss position. The Company does not intend to sell its investments before recovery of the amortized cost basis of its debt securities at maturity and no allowance for credit losses was recorded as of December 31, 2023. All securities held by the Company have a maturity date of one year or less.
Securities are evaluated at the end of each reporting period. The Company did not record any impairment related to its available-for-sale securities during the year ended December 31, 2023.
4.Fair Value Measurements
The Company estimated the fair value of the Tranche Options, as defined below (see Note 10), at the time of issuance and subsequently remeasured them at each reporting period and prior to settlement, which occurred prior to December 31, 2022. The fair value of the Tranche Options was determined using a contingent forward model, which considered as inputs the estimated fair value of the preferred units as of each valuation date, the risk-free interest rate, probability of achievement, salvage value and estimated time to each tranche closing. The most significant assumptions in the contingent forward model impacting the fair value of the Tranche Options is the fair value of the Company’s Series A Preferred Unit, probability of achievement and time to the tranche closing as of each measurement date. The Company determined the fair value per share of the underlying preferred unit by taking into consideration the most recent sales of its preferred units, results obtained from third-party valuations and additional factors the Company deems relevant.
The following table presents information about the Company’s financial assets and liabilities measured at fair value on a reoccurring basis and indicates the level of fair value hierarchy utilized to determine such values as of December 31, 2023 (in thousands):
|
|
AS OF DECEMBER 31, 2023 |
||||||||||
|
|
LEVEL 1 |
|
LEVEL 2 |
|
LEVEL 3 |
|
TOTAL |
||||
Assets: |
|
|
|
|
|
|
|
|
|
|
|
|
Cash equivalents: |
|
|
|
|
|
|
|
|
|
|
|
|
Money market funds |
|
$ |
110,655 |
|
$ |
— |
|
$ |
— |
|
$ |
110,655 |
Marketable securities: |
|
|
|
|
|
|
|
|
|
|
|
|
U.S. treasury securities |
|
|
123,974 |
|
|
— |
|
|
— |
|
|
123,974 |
Debt securities issued by U.S. government agencies |
|
|
— |
|
|
153,169 |
|
|
— |
|
|
153,169 |
|
|
$ |
234,629 |
|
$ |
153,169 |
|
$ |
— |
|
$ |
387,798 |
As of December 31, 2022, the Company did not have any assets or liabilities measured at fair value using Level 3 significant unobservable inputs. The following table provides a reconciliation of all assets and liabilities measured at fair value using Level 3 significant unobservable inputs which were settled during the period ended December 31, 2022 (in thousands):
155
|
|
TRANCHE OPTION |
|
TRANCHE OPTION |
|
|
|||
|
|
PREFERRED UNIT |
|
PREFERRED UNIT |
|
|
|||
|
|
ASSET |
|
(LIABILITY) |
|
TOTAL |
|||
Balance as of February 4, 2022 (inception) |
|
$ |
— |
|
$ |
— |
|
$ |
— |
Issuance |
|
|
650 |
|
|
(1,700) |
|
|
(1,050) |
Change in fair value |
|
|
(50) |
|
|
(9,100) |
|
|
(9,150) |
Transfer to temporary equity upon settlement |
|
|
(600) |
|
|
10,800 |
|
|
10,200 |
Balance as of December 31, 2022 |
|
$ |
— |
|
$ |
— |
|
$ |
— |
5.Property and Equipment, net
As of December 31, 2023, the Company had property and equipment, net of $0.4 million, which consisted entirely of lab equipment. The Company recognized an immaterial amount of depreciation expense for the year ended December 31, 2023. The Company did not own any property and equipment as of December 31, 2022.
6.Prepaids and Other Assets
Prepaid expenses and other current assets consisted of the following (in thousands):
|
|
DECEMBER 31, |
|
DECEMBER 31, |
||
|
|
2023 |
|
2022 |
||
Prepaid expenses |
|
$ |
1,736 |
|
$ |
108 |
Other current assets |
|
|
1,214 |
|
|
57 |
Total |
|
$ |
2,950 |
|
$ |
165 |
As of December 31, 2023, the Company had restricted cash of $0.3 million held as a letter of credit for the benefit of a contract research organization. The related letter of credit was classified within other non-current assets on the consolidated balance sheet as of December 31, 2023. The Company had no restricted cash as of December 31, 2022.
7.Accrued Expenses
Accrued expenses consisted of the following (in thousands):
|
|
DECEMBER 31, |
|
DECEMBER 31, |
||
|
|
2023 |
|
2022 |
||
Accrued external research and development expenses |
|
$ |
6,685 |
|
$ |
8,847 |
Accrued manufacturing expenses |
|
|
9,219 |
|
|
— |
Accrued other |
|
|
1,243 |
|
|
200 |
Accrued employee compensation |
|
|
167 |
|
|
515 |
Total |
|
$ |
17,314 |
|
$ |
9,562 |
8.Other Significant Agreements
Paragon Option Agreements
In February 2022, the Company entered into an antibody discovery and option agreement with Paragon, which was subsequently amended in November 2022 (as amended, the “2022 Option Agreement”). Under the terms of the 2022 Option Agreement, Paragon identifies, evaluates and develops antibodies directed against certain mutually agreed therapeutic targets of interest to the Company. The 2022 Option Agreement initially included two selected targets, IL-13 and IL-4Rα, and was subsequently amended in November 2022 to include an additional selected target, OX40L. Under the 2022 Option Agreement, the Company has the exclusive option to, on a research program-by-research program basis, be granted an exclusive, worldwide license to all of Paragon’s right, title and interest in and to the intellectual property resulting from the applicable research program to develop, manufacture and commercialize the antibodies and products directed to the selected targets (each, an “Option”).
156
From time to time, the Company can choose to add additional targets to the collaboration by mutual agreement with Paragon.
Pursuant to the terms of the 2022 Option Agreement, the parties initiated certain research programs that generally focus on a particular target (each, a “Research Program”). Each Research Program is aimed at discovering, generating, identifying and/or characterizing antibodies directed to the respective target. For each Research Program, the parties established a research plan that sets forth the activities that will be conducted, and the associated research budget (each, a “Research Plan”). Upon execution of the 2022 Option Agreement, the Company and Paragon agreed on an initial Research Plan that outlined the services that will be performed commencing at inception of the arrangement related to IL-13 and IL-4Rα. The Research Plan for OX40L was agreed to prior to December 31, 2022. The Company’s exclusive option with respect to each Research Program is exercisable at its sole discretion at any time during the period beginning on the initiation of activities under the associated Research Program and ending a specified number of days following the delivery of the data package from Paragon related to the results of the Research Plan activities (the “Option Period”). There is no payment due upon exercise of an Option pursuant to the 2022 Option Agreement.
Unless terminated earlier, the 2022 Option Agreement shall continue in force on a Research Program-by-Research Program basis until the earlier of: (i) the end of the Option Period for such Research Program, as applicable, if such Option is not exercised by the Company; and (ii) the effective date of the license agreement for such Research Program if the Company exercises its Option with respect to such Research Program (the “2022 Term”). Upon the expiration of the 2022 Term for all then-existing Research Programs, under the 2022 Option Agreement, the 2022 Option Agreement will automatically expire in its entirety. The Company may terminate the 2022 Option Agreement or any Research Program at any time for any or no reason upon 30 days’ prior written notice to Paragon, provided that the Company must pay certain unpaid fees due to Paragon upon such termination, as well as any non-cancellable obligations reasonably incurred by Paragon in connection with its activities under any terminated Research Program. Each party has the right to terminate the 2022 Option Agreement or any Research Program upon (i) 30 days’ prior written notice of the other party’s material breach that remains uncured for the 30 day period and (ii) the other party’s bankruptcy.
In consideration for the exclusive options granted under the 2022 Option Agreement, the Company paid an upfront cash amount of $1.3 million and issued 1,250,000 common units to Paragon. Paragon was also entitled to up to an additional 3,750,000 of common units in exchange for the rights granted under the 2022 Option Agreement, which were issued in connection with the closings of the additional Tranche Options of the Series A Preferred Unit financing (see Note 10). Through December 31, 2023, the Company had issued a total of 5,000,000 common units to Paragon with an aggregate fair value of $2.2 million on the grant date. Under the 2022 Option Agreement, on a Research Program-by-Research Program basis following the finalization of the Research Plan for each respective Research Program, the Company is required to pay Paragon a nonrefundable fee in cash of $0.5 million. The Company is also obligated to compensate Paragon on a quarterly basis for its services performed under each Research Program based on the actual costs incurred. The Company expenses the service fees as the associated costs are incurred when the underlying services are rendered. Such amounts are classified within research and development expenses in the accompanying consolidated statement of operations and comprehensive loss.
The Company concluded that the rights obtained under the 2022 Option Agreement represent an asset acquisition whereby the underlying assets comprise in-process research and development assets with no alternative future use. The 2022 Option Agreement did not qualify as a business combination because substantially all of the fair value of the assets acquired was concentrated in the exclusive license options, which represent a group of similar identifiable assets. Therefore, the aggregate acquisition cost of $3.5 million, related to the upfront cash and equity payments, was recognized as acquired in-process research and development expense, which is reported as a component of research and development expense during the period from February 4, 2022 (inception) to December 31, 2022. Amounts paid as on-going development cost reimbursements associated with services being rendered under the related Research Programs is recognized as research and development expense when incurred.
In November 2023, the Company entered into an additional antibody discovery and option agreement with Paragon (the “2023 Option Agreement,” and together with the 2022 Option Agreement, collectively the “Option Agreements”).
157
Under the terms of the 2023 Option Agreement, Paragon identifies, evaluates and develops antibodies directed against certain mutually agreed therapeutic targets of interest to the Company. The 2023 Option Agreement initially includes one undisclosed target. Under the 2023 Option Agreement, the Company has the exclusive option to, on a research program-by-research program basis, be granted an exclusive, worldwide license to all of Paragon’s right, title and interest in and to the intellectual property resulting from the applicable research program to develop, manufacture and commercialize the antibodies and products directed to the selected targets Option. From time to time, the Company can choose to add additional targets to the collaboration by mutual agreement with Paragon.
Pursuant to the terms of the 2023 Option Agreement, the parties may initiate Research Programs. Each Research Program is aimed at discovering, generating, identifying and/or characterizing antibodies directed to the respective target. For each Research Program, the parties must establish a Research Plan. In January 2024, the Company and Paragon agreed on an initial Research Plan that outlines the services that will be performed commencing at inception of the arrangement related to the undisclosed target. The Company’s exclusive option with respect to each Research Program is exercisable at its sole discretion at any time during the period beginning on the initiation of activities under the associated Research Program and ending a specified number of days following the delivery of the data package from Paragon related to the results of the Research Plan activities. There is no payment due upon exercise of an Option pursuant to the 2023 Option Agreement. Following entry into the 2023 Option Agreement, the Company and Paragon will negotiate a form of License Agreement to be entered into in the event that the Company exercises its exclusive option with respect to each Research Program, which License Agreement will include certain pre-agreed economic and other business terms.
Unless terminated earlier, the 2023 Option Agreement shall continue in force on a Research Program-by-Research Program basis until the earlier of: (i) the end of the Option Period for such Research Program, as applicable, if such Option is not exercised by the Company; and (ii) the effective date of the license agreement for such Research Program if the Company exercises its Option with respect to such Research Program (the “2023 Term”). Upon the expiration of the 2023 Term for all then-existing Research Programs, under the 2023 Option Agreement, the 2023 Option Agreement will automatically expire in its entirety. The Company may terminate the 2023 Option Agreement or any Research Program at any time for any or no reason upon 30 days’ prior written notice to Paragon, provided that the Company must pay certain unpaid fees due to Paragon upon such termination, as well as any non-cancellable obligations reasonably incurred by Paragon in connection with its activities under any terminated Research Program. Each party has the right to terminate the 2023 Option Agreement or any Research Program upon (i) 30 days’ prior written notice of the other party’s material breach that remains uncured for the 30 day period and (ii) the other party’s bankruptcy.
Under the 2023 Option Agreement, on a Research Program-by-Research Program basis following the finalization of the Research Plan for each respective Research Program, the Company is required to pay Paragon a nonrefundable fee in cash of $2.0 million. The Company is also obligated to compensate Paragon on a quarterly basis for its services performed under each Research Program based on the actual costs incurred. The Company expenses the service fees as the associated costs are incurred when the underlying services are rendered.
For the year ended December 31, 2023 and for the period from February 4, 2022 (inception) to December 31, 2022, the Company recognized $15.9 million and $22.3 million, respectively, of research and development expense in connection with services provided by Paragon under the Option Agreements, including nonrefundable fees following the finalization of a Research Plan.
Paragon License Agreements
In November 2022, the Company exercised its option available under the 2022 Option Agreement with respect to the IL-13 Research Program. Upon such exercise, the parties entered into an associated license agreement (the “IL-13 License Agreement”). In April 2023, the Company exercised its option available under the 2022 Option Agreement with respect to the IL-4Rα Research Program and OX40L Research Program. Upon such exercise, the parties entered into associated license agreements (the “IL-4Rα License Agreement” and the “OX40L License Agreement,” respectively, and collectively with the IL-13 License Agreement, the “License Agreements”). Under the terms of each of the License Agreements, Paragon granted to the Company an exclusive, worldwide, royalty-bearing, sublicensable right and license with respect to certain information, patent rights and sequence information related to antibodies directed at the respective target to use, make, sell, import, export and otherwise exploit the antibodies directed at the respective target.
158
Pursuant to the License Agreements, the Company granted to Paragon a similar license (except that such license the Company granted to Paragon is non-exclusive) to the respective licenses with respect to multispecific antibodies that are directed at the respective target and one or more other antibodies. The Company was also granted a right of first negotiation with Paragon concerning the development, license and grant of rights to certain multispecific antibodies associated with each license. The Company is solely responsible for the continued development, manufacture and commercialization of products at its own cost and expense for each licensed target.
The Company is obligated to pay Paragon up to $3.0 million upon the achievement of specific development and clinical milestones for the first product under each of the License Agreements that achieves such specified milestones, including a payment of $1.0 million upon the nomination of a development candidate and $2.0 million upon the first dosing of a human patient in a Phase 1 trial. Upon execution of the IL-13 License Agreement, the Company paid Paragon a $1.0 million fee for the nomination of a development candidate. In August 2023, the Company announced the dosing of its first participant in the Phase 1 trial of APG777 and incurred a milestone payment of $2.0 million to Paragon in the third quarter of 2023. In November 2023, the Company finalized the nomination of a development candidate under the IL-4Rα License Agreement and made a milestone payment of $1.0 million to Paragon in the fourth quarter of 2023. Except for the three milestone payments totaling an aggregate of $4.0 million, no other milestone or royalty payments have become due to Paragon through December 31, 2023.
The Company is also obligated to pay royalties to Paragon equal to a low-single digit percentage of net sales of any products under each of the License Agreements, and Paragon has a similar obligation to pay royalties to the Company with respect to the each of the multispecific licenses. Royalties are due on a product-by-product and country-by-country basis beginning upon the first commercial sale of each product and ending on the later of (i) 12 years after the first commercial sale of such product in such country and (ii) expiration of the last valid claim of a patent covering such product in such country (the “Royalty Term”).
Unless earlier terminated, the License Agreements remain in effect until the expiration of the last-to-expire Royalty Term for any and all Products associated with the respective license. The Company may terminate the agreement in its entirety or on a country-by-country or product-by-product at any time for any or no reason upon 60 days’ advance written notice to Paragon, and either party may terminate for (i) the other party’s material breach that remains uncured for 90 days (or 30 days with respect to any failure to make payments) following notice of such breach and (ii) the other party’s bankruptcy. Upon any termination prior to the expiration of a License Agreement, all licenses and rights granted pursuant to such License Agreement will automatically terminate and revert to the granting party and all other rights and obligations of the parties will terminate.
The Company concluded that each of the License Agreements constitutes an asset acquisition of in-process research and development assets with no alternative future use. Each of the arrangements did not qualify as a business combination because substantially all of the fair value of the assets acquired was concentrated in the license which comprises a single identifiable asset. Therefore, the aggregate acquisition cost for each license was recognized as research and development expense. For the year ended December 31, 2023 and for the period from February 4, 2022 (inception) to December 31, 2022, the Company recognized $10.4 million and $1.0 million, respectively, of research and development expense in connection with services provided by Paragon under the License Agreements.
Biologics Master Services Agreement — WuXi Biologics (Hong Kong) Limited
In June 2022, Paragon and WuXi Biologics (Hong Kong) Limited (“WuXi Biologics”) entered into a biologics master services agreement (the “WuXi Biologics MSA”), which was subsequently novated to the Company by Paragon in the second quarter of 2023. The WuXi Biologics MSA governs all development activities and GMP manufacturing and testing for APG777 and APG808 programs, as well as the Company’s other programs, on a work order basis. Under the WuXi Biologics MSA, the Company is obligated to pay WuXi Biologics a service fee and all non-cancellable obligations in the amount specified in each work order associated with the agreement for the provision of services.
The WuXi Biologics MSA terminates on the later of (i) June 20, 2027 or (ii) the completion of services under all work orders executed by the parties prior to June 20, 2027, unless terminated earlier. The term of each work order terminates upon completion of the services under such work order, unless terminated earlier. The Company can terminate the WuXi Biologics MSA or any work order at any time upon 30 days’ prior written notice and immediately upon written notice if WuXi Biologics fails to obtain or maintain required material governmental licenses or approvals.
159
Either party may terminate a work order (i) at any time upon six months’ prior notice with reasonable cause, provided however that if WuXi Biologics terminates a work order in such manner, no termination or cancellation fees shall be paid busy the Company and (ii) immediately for cause upon (a) the other party’s material breach that remains uncured for 30 days after notice of such breach, (b) the other party’s bankruptcy or (c) a force majeure event that prevents performance for a period of at least 90 days.
For the year ended December 31, 2023, the Company recognized $20.2 million of research and development expense in connection with the WuXi Biologics MSA subsequent to novation. As of December 31, 2023, there were no non-cancelable obligations under the WuXi Biologics MSA.
Cell Line License Agreement — WuXi Biologics (Hong Kong) Limited
In June 2022, Paragon and WuXi Biologics entered into a cell line license agreement (the “Cell Line License Agreement”), which was subsequently novated to the Company by Paragon in the second quarter of 2023. Under the Cell Line License Agreement, the Company received a non-exclusive, worldwide, sublicensable license to certain of WuXi Biologics’ know-how, cell line, biological materials (the “WuXi Biologics Licensed Technology”) and media and feeds to make, have made, use, sell and import certain therapeutic products produced through the use of the cell line licensed by WuXi Biologics under the Cell Line License Agreement (the “WuXi Biologics Licensed Products”). Specifically, the WuXi Biologics Licensed Technology is used to manufacture a component of the APG777 and APG808 programs.
In consideration for the license, the Company agreed to pay WuXi Biologics a non-refundable license fee of $150,000. Additionally, if the Company manufactures all of its commercial supplies of bulk drug product with a manufacturer other than WuXi Biologics or its affiliates, it is required to make royalty payments to WuXi Biologics in an amount equal to a fraction of a single digit percentage of global net sales of WuXi Biologics Licensed Products manufactured by a third-party manufacturer (the “Royalty”). If the Company manufactures part of its commercial supplies of the WuXi Biologics Licensed Products with WuXi Biologics or its affiliates, then the Royalty will be reduced accordingly on a pro rata basis.
The Cell Line License Agreement will continue indefinitely unless terminated (i) by the Company upon six months’ prior written notice and its payment of all undisputed amounts due to WuXi Biologics through the effective date of termination, (ii) by WuXi Biologics for a material breach by the Company that remains uncured for 60 days after written notice, (iii) by WuXi Biologics if the Company fails to make a payment and such failure continues for 30 days after receiving notice of such failure, or (iv) by either party upon the other party’s bankruptcy.
9.Commitments and Contingencies
Other Contracts
Currently, all of the Company’s preclinical and clinical drug manufacturing, storage, distribution or quality testing are outsourced to third-party manufacturers. As development programs progress and new process efficiencies are built, the Company expects to continually evaluate this strategy with the objective of satisfying demand for registration trials and, if approved, the manufacture, sale and distribution of commercial products. Under such agreements, the Company is contractually obligated to make certain payments to vendors upon early termination, primarily to reimburse them for their unrecoverable outlays incurred prior to cancellation as well as any amounts owed by the Company prior to early termination. The actual amounts the Company could pay in the future to the vendors under such agreements may differ from the purchase order amounts due to cancellation provisions.
Indemnification Agreements
The Company enters into standard indemnification agreements and/or indemnification sections in other agreements in the ordinary course of business. Pursuant to the agreements, the Company indemnifies, holds harmless, and agrees to reimburse the indemnified party for losses suffered or incurred by the indemnified party, generally the Company’s business partners.
160
The term of these indemnification agreements is generally perpetual any time after execution of the agreement. There is no limit to the maximum potential amount of future payments the Company could be required to make under these indemnification agreements. As of December 31, 2023, the Company has not incurred costs to defend lawsuits or settle claims related to these indemnification agreements. The Company was not aware of any claims under these indemnification arrangements as of December 31, 2023 and December 31, 2022.
Legal Proceedings
The Company is not currently party to any material legal proceedings. At each reporting date, the Company evaluates whether or not a potential loss amount or a potential range of loss is probable and reasonably estimable under the provisions of FASB ASC Topic 450, Contingencies (“ASC 450”). The Company expenses as incurred the costs related to its legal proceedings.
10.Preferred Shares
As of December 31, 2022, the Company had authorized, issued and outstanding an aggregate of 65,089,212 preferred units, of which 20,000,000 units had been designated as Series A Preferred Units and 45,089,212 units had been designated as Series B Preferred Units. All outstanding preferred units were exchanged for 24,987,750 shares of common stock (or non-voting common stock in lieu thereof) in connection with the IPO in July 2023. As of December 31, 2023, the Company did not have any outstanding preferred units.
Series A Preferred Units
On February 24, 2022, the Company executed the Series A Preferred Unit Purchase Agreement (the “Series A Agreement”) to issue and sell up to 20,000,000 Series A Preferred Units at a purchase price of $1.00 per unit. In the initial closing on February 24, 2022, the Company issued 5,000,000 Series A Preferred Units at a purchase price of $1.00, resulting in gross cash proceeds to the Company of $5.0 million, and incurred $0.2 million of issuance costs. The Series A Agreement provided for three tranche option closings following the initial closing (the “Tranche Options”), which Tranche Option closings were subject to approval of the Board of Managers of Apogee Therapeutics, LLC (the “Board of Managers”), which was controlled by the holders of the Series A Preferred Units. The Board of Managers approved all such subsequent closings resulting in investors purchasing 5,000,000 Series A Preferred Units in each of the three subsequent Tranche Option closings throughout 2022. As a result, the Company received an aggregate of $20.0 million in gross proceeds associated with the Series A Agreement.
The Company assessed the Tranche Options and concluded that they met the definition of a freestanding financial instrument, as the Tranche Options were legally detachable and separately exercisable from the Series A Preferred Units. Therefore, the Company allocated the proceeds between the Tranche Options and the Series A Preferred Units sold at the initial closing. As the Series A Preferred Units are contingently redeemable upon an event that is not completely within the control of the Company, the Tranche Options are classified as an asset or liability and are initially recorded at fair value. The Tranche Options are measured at fair value at each reporting period, through the settlement of the instrument. Since the Tranche Options are subject to fair value accounting, the Company allocated $1.1 million of the initial proceeds to the Tranche Options based on the fair value at the date of issuance with the remaining proceeds beings allocated to the Series A Preferred Units. Upon the Tranche Option closings in August and October 2022, the respective Tranche Option value was remeasured at fair value and then reclassified to Series A Preferred Units upon settlement.
Series B Preferred Units
On November 15, 2022, the Company executed the Series B Preferred Unit Purchase Agreement (the “Series B Agreement”) to issue and sell 45,089,212 Series B Preferred Units in a single closing at a purchase price of $3.30456 per unit, resulting in gross cash proceeds to the Company of $149.0 million. The Company incurred $0.5 million of issuance costs in connection with the issuance of the Series B Preferred Units.
161
The Company’s preferred units as of December 31, 2022 consisted of the following (in thousands, except unit amounts):
|
|
|
|
PREFERRED |
|
|
|
|
|
|
|
|
PREFERRED |
|
UNITS |
|
|
|
|
|
|
|
|
UNITS |
|
ISSUED AND |
|
CARRYING |
|
LIQUIDATION |
||
|
|
AUTHORIZED |
|
OUTSTANDING |
|
VALUE |
|
PREFERENCE |
||
Series A Preferred Units |
|
20,000,000 |
|
20,000,000 |
|
$ |
28,971 |
|
$ |
20,000 |
Series B Preferred Units |
|
45,089,212 |
|
45,089,212 |
|
|
148,496 |
|
|
149,000 |
Total |
|
65,089,212 |
|
65,089,212 |
|
$ |
177,467 |
|
$ |
169,000 |
Embedded Securities Evaluation
The Company assessed the Series A Preferred Units and the Series B Preferred Units for any features that may require separate accounting under FASB ASC Topic 815-Derivatives and Hedging (“ASC 815”). The Company concluded that none of the features required separate accounting as a derivative.
11.Common Stock
In July 2023, the Company completed its IPO, selling an aggregate 20,297,500 shares of common stock. All outstanding preferred units were exchanged into 24,987,750 shares of common stock in connection with the IPO. Following the IPO, the Company is authorized to issue 400,000,000 shares of common stock, par value $0.00001. As of December 31, 2023, 50,655,671 and 48,338,769 shares of common stock were issued and outstanding, respectively. The 50,655,671 shares of common stock issued is comprised of 37,169,029 shares of voting common stock, and 13,486,642 shares of non-voting common stock, respectively. As of December 31, 2023, there are 2,316,902 shares of unvested restricted common stock included within the shares of common stock issued.
As of December 31, 2022, the Company had 5,000,000 common units authorized, issued and outstanding.
12.Equity-Based Compensation
Incentive Units
Prior to the Reorganization, the Company periodically granted incentive units to employees, managers and executives, as well as to consultants and service providers of the Company. The incentive units represent a separate substantive class of members’ equity with defined rights. The incentive units represent profits interest in the increase in the value of the entity over a threshold value, or strike price, as determined at the time of grant. The strike price is established for tax compliance purposes related to Internal Revenue Service Revenue Procedure 93-27 and 2001-43 where the Company allocates equity value to separate classes of equity in a hypothetical liquidation transaction as of the date of grant. Each incentive unit issued includes a strike price determined by the Board of Managers. The strike price is based on an estimate of the amount a common unit would receive on the date of issuance of such incentive units in a hypothetical liquidation of the Company in which the Company sold its assets for their fair market value, satisfied its liabilities, and distributed the net proceeds to the holders of units in liquidation of the Company.
The Company accounts for equity-based compensation in accordance with ASC 718. In accordance with ASC 718, compensation cost is measured at estimated fair value and is included as compensation expense over the vesting period during which service is provided in exchange for the award. The service-based incentive unit grants generally vest over a four-year service period, with the first 25% vesting on the 12-month anniversary of the vesting start date and the remaining vesting in equal monthly installments over the following 36 months. The service-based and performance-based incentive unit grant, which the Company has one such award, vests in the same manner as the service-based award upon the achievement of the performance condition. The Company had one incentive unit grant which vested immediately upon issuance. The holders of vested incentive units are entitled to distributions and are not required to purchase or “exercise” their incentive units in order to receive such distributions. However, distributions to incentive unit holders began only after the cumulative amount distributed to common unit holders exceeds the strike price with respect to such incentive unit.
162
The Company determined that incentive units issued to employees, managers, executives, non-employees and service providers are equity-based service payments and, as such, the Company measures and recognizes the related compensation expense in a manner consistent with its accounting policy for equity-based awards.
The fair value of each incentive unit grant is estimated on the grant date using either an option pricing method (“OPM”), or a hybrid method, both of which use market approaches to estimate the Company’s enterprise value. The OPM treats common units, incentive units and preferred units as call options on the total equity value of a company, with exercise prices based on the value thresholds at which the allocation among the various holders of a company’s securities changes. Under this method, the incentive units have value only if the funds available for distribution to unitholders exceed the value of the preferred and common unit distribution preferences and the strike price with respect to such incentive unit at the time of the liquidity event. The hybrid method is a probability-weighted expected return method (“PWERM”), where the equity value is allocated in one or more of the scenarios using an OPM. The PWERM is a scenario-based methodology that estimates the fair value of each unit based upon an analysis of future values, assuming various outcomes. The incentive unit value is based on the probability-weighted value across the scenarios, considering the OPM to estimate the value within each scenario given the rights of each class of unit. A discount for lack of marketability of the incentive unit is then applied to arrive at an indication of fair value for the incentive unit.
The following assumptions were used in determining the fair value of incentive units granted during the period:
|
|
|
|
FEBRUARY 4, 2022 |
|
|
|
YEAR ENDED |
|
(INCEPTION) TO |
|
|
|
DECEMBER 31, 2023 |
|
DECEMBER 31, 2022 |
|
Risk free interest rate |
|
4.1% - 4.9 |
% |
4.1% - 4.3 |
% |
Expected dividend yield |
|
0.0 |
% |
0.0 |
% |
Expected term (in years) |
|
0.17 - 2.00 |
|
0.71 - 2.25 |
|
Expected volatility |
|
84.0% - 90.0 |
% |
77.0% - 86.0 |
% |
The following table summarizes the Company’s unvested incentive unit activity:
|
|
|
|
WEIGHTED- |
|
|
|
|
|
AVERAGE |
|
|
|
NUMBER OF |
|
GRANT DATE FAIR |
|
|
|
SHARES |
|
VALUE PER UNIT |
|
Unvested incentive units as of December 31, 2022 |
|
8,023,288 |
|
$ |
1.20 |
Granted |
|
4,621,901 |
|
$ |
1.32 |
Vested |
|
(922,338) |
|
$ |
1.54 |
Exchanged for unvested restricted common stock |
|
(11,722,851) |
|
$ |
1.22 |
Unvested incentive units as of December 31, 2023 |
|
— |
|
$ |
— |
The fair value of incentive units vested during the year ended December 31, 2023 was $1.4 million.
163
Restricted Common Stock
Concurrent with the Reorganization, all of the outstanding incentive units were exchanged into 3,469,546 shares of common stock, of which 2,779,358 were unvested restricted common stock. The following table provides a summary of the unvested restricted common stock award activity during the year ended December 31, 2023:
|
|
|
|
WEIGHTED- |
|
|
|
|
|
AVERAGE |
|
|
|
NUMBER OF |
|
GRANT DATE FAIR |
|
|
|
SHARES |
|
VALUE PER SHARE |
|
Unvested restricted common stock as of December 31, 2022 |
|
— |
|
$ |
— |
Exchange of incentive units |
|
2,779,358 |
|
$ |
5.16 |
Vested |
|
(443,831) |
|
$ |
4.02 |
Forfeited |
|
(18,625) |
|
$ |
13.08 |
Unvested restricted common stock as of December 31, 2023 |
|
2,316,902 |
|
$ |
5.31 |
The fair value of restricted stock vested during the year ended December 31, 2023 was $1.8 million.
2023 Equity Incentive Plan
In July 2023, in connection with the IPO, the Company’s Board of Directors (the “Board”) and stockholders approved the 2023 Equity Incentive Plan (the “2023 Plan”), which became effective on the date of the effectiveness of the registration statement for the IPO. The 2023 Plan provides for the grant of incentive stock options, non-qualified stock options, stock appreciation rights, awards of restricted stock, restricted stock units and other stock-based awards. As of December 31, 2023, the number of shares of common stock reserved for issuance under the 2023 Plan is equal to 6,706,037 shares of common stock. The number of shares available for grant and issuance under the 2023 Plan will be automatically increased on January 1 of each year by a number of shares equal to up to 5% of the outstanding shares of common stock on such date.
The Company uses the Black-Scholes option pricing model to estimate the fair value of stock options granted with the following assumptions:
|
|
YEAR ENDED |
|
|
DECEMBER 31, |
|
|
2023 |
Common stock fair value |
|
$17.00 - $27.94 |
Risk free interest rate |
|
3.9% - 4.9% |
Expected dividend yield |
|
0.0% |
Expected term (in years) |
|
5.75 – 6.25 |
Expected volatility |
|
96.8% - 104.7% |
164
The following table provides a summary of stock option activity under the 2023 Plan during the year ended December 31, 2023:
|
|
|
|
|
|
WEIGHTED- |
|
|
|||
|
|
|
|
WEIGHTED- |
|
AVERAGE |
|
AGGREGATE |
|||
|
|
|
|
AVERAGE |
|
REMAINING |
|
INTRINSIC |
|||
|
|
|
|
EXERCISE |
|
CONTRACTUAL TERM |
|
VALUE |
|||
|
|
OPTIONS |
|
PRICE |
|
(IN YEARS) |
|
(IN THOUSANDS) |
|||
Outstanding as of December 31, 2022 |
|
— |
|
$ |
— |
|
|
— |
|
$ |
— |
Granted |
|
2,518,728 |
|
$ |
21.50 |
|
|
— |
|
|
— |
Forfeited |
|
(12,711) |
|
$ |
23.60 |
|
|
— |
|
|
— |
Outstanding as of December 31, 2023 |
|
2,506,017 |
|
$ |
21.49 |
|
|
9.80 |
|
|
16,154 |
Vested and expected to vest as of December 31, 2023 |
|
2,506,017 |
|
$ |
21.49 |
|
|
9.80 |
|
|
16,154 |
Exercisable as of December 31, 2023 |
|
5,555 |
|
$ |
23.60 |
|
|
9.63 |
|
|
24 |
The fair value of options vested during the year ended December 31, 2023 was $0.1 million.
The following table provides a summary of restricted stock unit activity under the 2023 Plan during the year ended December 31, 2023:
|
|
|
|
WEIGHTED- |
|
|
|
|
|
AVERAGE |
|
|
|
NUMBER OF |
|
GRANT DATE FAIR |
|
|
|
SHARES |
|
VALUE PER SHARE |
|
Unvested restricted stock units as of December 31, 2022 |
|
— |
|
$ |
— |
Granted |
|
144,090 |
|
$ |
22.86 |
Unvested restricted stock units as of December 31, 2023 |
|
144,090 |
|
$ |
22.86 |
2023 Employee Stock Purchase Plan
In July 2023, the Board adopted and the Company’s stockholders approved the 2023 Employee Stock Purchase Plan, (the “ESPP”), which became effective on July 13, 2023. As of December 31, 2023, a total of 479,003 shares of common stock were reserved for issuance under the ESPP, and no shares have been issued under the ESPP.
Equity-Based Compensation Expense
The following table presents the classification of equity-based compensation expense related to equity awards granted to employees, managers, executives, and service providers (in thousands):
|
|
|
|
|
PERIOD FROM |
|
|
|
YEAR ENDED |
|
FEBRUARY 4, 2022 |
||
|
|
DECEMBER 31, |
|
(INCEPTION) TO |
||
|
|
2023 |
|
DECEMBER 31, 2022 |
||
Research and development expense |
|
$ |
1,574 |
|
$ |
1,502 |
General and administrative expense |
|
|
4,529 |
|
|
640 |
Total |
|
$ |
6,103 |
|
$ |
2,142 |
As of December 31, 2023, the total unrecognized compensation expense related to the Company’s unvested restricted stock, restricted stock units, and stock options was $56.1 million, which the Company expects to recognize over a weighted-average period of approximately 3.7 years. For the period from February 4, 2022 (inception) to December 31, 2022, the Company recognized an additional $2.2 million of equity-based compensation expense, in connection with the additional common units issued under the 2022 Option Agreement with Paragon.
In August 2023, the Board approved two option grants to the new Chairman of the Board, (1) to purchase 50,000 shares of the Company’s common stock under the 2023 Plan (“first option”), and (2) to purchase 100,000 shares of the
165
Company’s common stock outside of the 2023 Plan (“second option”), in which the shares underlying both options will vest and become exercisable in equal monthly installments over a three-year period from August 2023. The second option is contingent upon approval of the shares underlying the award by the Company’s stockholders at the 2024 Annual Meeting of Stockholders and failure to obtain stockholder approval will result in the forfeiture of the award. Prior to receiving stockholder approval for the second option, neither a grant date nor a service inception date will occur, and no compensation cost is recognized for the award. Should stockholder approval be received at the 2024 Annual Meeting of Stockholders, a cumulative catch-up in equity-based compensation for the second option will be recognized on the date of stockholder approval.
13.Related Parties
Under the Option Agreements and the License Agreements, Paragon, a stockholder of the Company which was founded by a Series A Preferred Unit investor, received upfront consideration in the form of common units, is entitled to receive milestone and royalty payments upon specific conditions and receives payments from the Company for providing ongoing services under the agreements (see Note 8). As of December 31, 2023 and December 31, 2022, $5.2 million and $8.0 million was due to Paragon, respectively. The Company incurred $26.3 million of research and development expenses with Paragon for the year ended December 31, 2023. The Company incurred $23.3 million of research and development expenses, exclusive of $3.7 million of equity-based research and development expense with Paragon, and $0.3 million of general and administrative expenses with Paragon for the period from February 4, 2022 (inception) to December 31, 2022.
14.Net Loss Per Share
Basic and diluted net loss per share attributable to common stockholders was calculated as follows (in thousands, except share and per share data):
|
|
YEAR ENDED |
|
FEBRUARY 4 |
||
|
|
DECEMBER 31, |
|
(INCEPTION) TO |
||
|
|
2023 |
|
DECEMBER 31, 2022 |
||
Numerator: |
|
|
|
|
|
|
Net loss |
|
$ |
(83,985) |
|
$ |
(39,785) |
Net loss attributable to common stockholders, basic and diluted |
|
$ |
(83,985) |
|
$ |
(39,785) |
Denominator: |
|
|
|
|
|
|
Weighted average shares of common stock outstanding, basic and diluted |
|
|
25,005,774 |
|
|
2,462,236 |
Net loss per share attributable to common stockholders, basic and diluted |
|
$ |
(3.36) |
|
$ |
(16.16) |
The following potential common shares, presented based on amounts outstanding period end, were excluded from the calculation of diluted net loss per share attributable to common stockholders for the period indicated because including them would have been anti-dilutive:
|
|
|
|
PERIOD FROM |
|
|
YEAR |
|
FEBRUARY 4 |
|
|
ENDED |
|
(INCEPTION) TO |
|
|
DECEMBER 31, 2023 |
|
DECEMBER 31, 2022 |
Series A Preferred Units |
|
— |
|
20,000,000 |
Series B Preferred Units |
|
— |
|
45,089,212 |
Vested Incentive Units |
|
— |
|
1,625,086 |
Unvested Incentive Units |
|
— |
|
8,023,288 |
Stock options |
|
2,506,017 |
|
— |
Unvested restricted common stock |
|
2,316,902 |
|
— |
Unvested restricted stock units |
|
144,090 |
|
— |
Total |
|
4,967,009 |
|
74,737,586 |
166
15.Operating Leases
In November 2023, the Company entered into a lease agreement for lab space. As of December 31, 2023, the current and non-current portions of the total liability for the operating lease were $1.1 million and $0.9 million, respectively. As of December 31, 2023, the remaining lease term on the Company’s operating lease was 1.9 years. As of December 31, 2023, the incremental borrowing rate used to determine the operating lease liabilities included on the balance sheet was 10%.
As of December 31, 2023, the future minimum lease payments for the Company’s operating lease for each of the years ending December 31 were as follows (in thousands):
|
|
Amount |
|
2024 |
|
$ |
1,244 |
2025 |
|
|
964 |
Thereafter |
|
|
— |
Total undiscounted lease payments |
|
|
2,208 |
Present value adjustment |
|
|
(174) |
Total net lease liabilities |
|
$ |
2,034 |
Lease expense was $0.1 million for the year ended December 31, 2023.
16.Income Tax
Prior to the Reorganization, Apogee Therapeutics, LLC was taxed under the Partnership provisions of the Internal Revenue Code. Accordingly, all income and deductions of Apogee Therapeutics, LLC were reported on the members’ individual income tax returns, and no income taxes were recorded by Apogee Therapeutics, LLC. Apogee Biologics, Inc., the operating subsidiary of the Company, was separately taxed as a C corporation for federal tax purposes. Subsequent to the Reorganization, Apogee Therapeutics, Inc. and its subsidiary, are taxed as a consolidated C corporation for federal tax purposes. The Company’s loss before income taxes is comprised solely of domestic losses. There is no income tax expense for the year ended December 31, 2023. The Company generated taxable losses for the respective period.
The difference between the effective tax rate and the U.S. federal tax rate were as follows:
|
|
YEAR ENDED |
|
FEBRUARY 4, 2022 |
|
|
|
DECEMBER 31, |
|
(INCEPTION) TO |
|
|
|
2023 |
|
DECEMBER 31, 2022 |
|
|
|
% |
|
% |
|
U.S. federal statutory tax rate |
|
(21.0) |
% |
(21.0) |
% |
Partnership operating expenses not subject to income taxes |
|
— |
% |
4.8 |
% |
State and local income taxes, net of federal income tax benefit |
|
(4.9) |
% |
(0.3) |
% |
Change in state effective income rate |
|
(1.8) |
% |
— |
% |
Nondeductible items |
|
1.5 |
% |
1.1 |
% |
Change in valuation allowance |
|
27.9 |
% |
16.9 |
% |
Tax credits |
|
(1.9) |
% |
(1.5) |
% |
Other |
|
0.2 |
% |
— |
% |
Effective tax rate |
|
— |
% |
— |
% |
167
Deferred taxes are recognized for temporary differences between the basis of assets and liabilities for financial statement and income tax purposes. The significant components of the Company’s deferred tax assets and liabilities consisted of the following (in thousands):
|
|
As of |
|
As of |
||
|
|
December 31, 2023 |
|
December 31, 2022 |
||
Deferred tax assets: |
|
|
|
|
|
|
Capitalized license and research and development payments |
|
$ |
21,034 |
|
$ |
4,563 |
Net operating loss carryforwards |
|
|
5,370 |
|
|
620 |
Research and development credits |
|
|
2,415 |
|
|
697 |
Intangible assets |
|
|
1,244 |
|
|
695 |
Reserves and accruals not currently deductible |
|
|
— |
|
|
108 |
Stock compensation |
|
|
186 |
|
|
— |
Lease liability |
|
|
502 |
|
|
— |
Other |
|
|
1 |
|
|
— |
Total deferred tax assets |
|
|
30,752 |
|
|
6,683 |
Deferred tax liabilities: |
|
|
|
|
|
|
Right-of-use asset |
|
|
(574) |
|
|
— |
Total deferred tax liabilities |
|
|
(574) |
|
|
— |
Valuation allowance |
|
|
(30,178) |
|
|
(6,683) |
Net deferred tax assets |
|
|
— |
|
|
— |
The Company has evaluated the positive and negative evidence bearing upon its ability to realize the deferred tax assets. Management has considered the Company’s cumulative net losses and its lack of commercialization of any products or generation of any revenue from product sales since inception and has concluded that it is more likely than not that the Company will not realize the benefits of the deferred tax assets. Accordingly, a full valuation allowance has been established against the net deferred tax assets as of December 31, 2023. The change in the valuation allowance for the year ended December 31, 2023 and period ended December 31, 2022 was $23.5 million and $6.7 million, respectively. Management reevaluates the positive and negative evidence at each reporting period.
As of December 31, 2023 and 2022, the Company had U.S. federal net operating loss carryforwards of approximately $23.6 million and $3.0 million, respectively, which have no expiration for federal tax purposes. As of December 31, 2023, the Company also had state net operating loss carryforwards of approximately $6.5 million, which will begin to expire in 2043 for state tax purposes.
As of December 31, 2023 and 2022, the Company had federal research and development credit carryforwards of approximately $2.7 million and $0.6 million, respectively, which will begin to expire in 2042. The Company also had California research and development credit carryforwards of approximately $0.7 million and $0.1 million, respectively, which will not expire.
The Company will conduct a study of its research and development credit carryforwards, which may result in an adjustment to its unrecognized tax benefits. However, a full valuation allowance has been provided against the Company’s research and development credits and, if an adjustment is required, this adjustment would be offset by an adjustment to the valuation allowance. Thus, there would be no impact to the accompanying consolidated balance sheet or statement of operations if an adjustment were required.
A reconciliation of the beginning and ending amount of gross unrecognized tax benefits is as follows (in thousands):
Beginning balance as of December 31, 2022 |
|
|
— |
Changes related to tax positions taken in the prior year |
|
|
187 |
Changes related to tax positions taken in the current year |
|
|
717 |
Ending Balance as of December 31, 2023 |
|
$ |
904 |
168
The Company files tax returns as prescribed by the tax laws of the jurisdictions in which it operates. Net operating losses are subject to review and possible adjustment by the Internal Revenue Service and state tax authorities. Net operating loss carryforwards may become subject to an annual limitation in the event of certain cumulative changes in the ownership interest of significant members over a three-year period in excess of 50%, as defined under Sections 382 and 383 of the Internal Revenue Code, respectively, as well as similar state provisions. This could limit the amount of tax attributes that can be utilized annually to offset future taxable income or tax liabilities. The amount of the annual limitation is determined based on the value of the company immediately prior to the ownership change. Subsequent ownership changes may further affect the limitation in future years. The Company has not yet completed a study to determine if any such changes have occurred that could limit its ability to use the net operating losses and tax credit carryforwards.
All tax returns will remain open for examination by the federal and state taxing authorities for three and four years, respectively, from the date of utilization of any net operating loss carryforwards or research and development credits.
It is the Company’s policy to include penalties and interest expense related to income taxes as a component of income tax expense, as necessary. As of December 31, 2023 and 2022, the Company had no accrued interest or penalties related to uncertain tax positions. The Company does not expect that its uncertain tax positions will materially change in the next twelve months.
The Tax Cuts and Jobs Act (“TCJA”) included a change in the treatment of research and development expenditures for tax purposes under Section 174. Effective for tax years beginning after December 31, 2021, specified R&D expenditures must undergo a 5-year amortization period for domestic spend and a 15-year amortization period for foreign spend. Prior to the effective date (2021 tax year and prior), taxpayers were able to immediately expense R&D costs under Section 174(a) or had the option to capitalize and amortize R&D expenditures over a 5-year recovery period under Section 174(b). The Company has evaluated the current legislation at this time and prepared the provision by following the treatment of research and development expenditures for tax purposes under Section 174.
17.Subsequent Events
In January 2024, the Company finalized the Research Plan with Paragon related to the undisclosed target, pursuant to the 2023 Option Agreement with Paragon. As such, the Company made a one-time non-refundable payment of $2.0 million to Paragon in the first quarter of 2024.
169
Item 9. Changes in and Disagreements with Accountants on Accounting and Financial Disclosure.
None.
Item 9A. Controls and Procedures
Evaluation of Disclosure Controls and Procedures
Our management, with the participation of our Principal Executive Officer and our Principal Financial Officer, evaluated the effectiveness of our disclosure controls and procedures as of December 31, 2023. Based on the foregoing evaluation, our Principal Executive Officer and Principal Financial Officer concluded that our disclosure controls and procedures were effective at a reasonable assurance level as of December 31, 2023. The term “disclosure controls and procedures,” as defined in Rules 13a-15(e) and 15d-15(e) under the Exchange Act means controls and other procedures of a company that are designed to ensure that information required to be disclosed by a company in the reports that it files or submits under the Exchange Act is recorded, processed, summarized and reported within the time periods specified in the SEC’s rules and forms. Disclosure controls and procedures include, without limitation, controls and procedures designed to ensure that information required to be disclosed by us in the reports we file or submit under the Exchange Act is accumulated and communicated to our management, including our Principal Executive Officer and Principal Financial Officer, or persons performing similar functions, as appropriate to allow timely decisions regarding required disclosure.
Management recognizes that any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving their objectives, and our management necessarily applies its judgment in evaluating the cost-benefit relationship of possible controls and procedures.
Internal Control over Financial Reporting
This Annual Report does not include a report of management’s assessment regarding internal control over financial reporting or an attestation report of our independent registered public accounting firm due to a transition period established by the rules of the SEC for newly public companies. Additionally, for as long as we remain an “emerging growth company” as defined in Section 2(a) of the Securities Act, as modified by the Jumpstart Our Business Startups Act of 2012, we intend to take advantage of the exemption permitting us not to comply with the requirement that our independent registered public accounting firm provide an attestation on the effectiveness of our internal control over financial reporting.
Changes in Internal Control over Financial Reporting
There were no changes in our internal control over financial reporting during the quarter ended December 31, 2023 that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
Item 9B. Other Information.
Trading Plans
During the quarter ended December 31, 2023, no director or Section 16 officer adopted or terminated any Rule 10b5-1 trading arrangements or non-Rule 10b5-1 trading arrangements (in each case, as defined in Item 408(a) of Regulation S-K).
Item 9C. Disclosure Regarding Foreign Jurisdictions that Prevent Inspections.
Not applicable.
170
PART III
Item 10. Directors, Executive Officers and Corporate Governance.
Management and Board of Directors
The following table sets forth the names, ages as of February 1, 2024, and positions of the individuals who currently serve as directors and executive officers of Apogee Therapeutics, Inc.
NAME |
|
AGE |
|
POSITION(S) |
|
Executive Officers and Employee Director: |
|
|
|
|
|
Michael Henderson, M.D. |
|
34 |
|
Chief Executive Officer and Director |
|
Carl Dambkowski, M.D. |
|
39 |
|
Chief Medical Officer |
|
Jane Pritchett Henderson |
|
58 |
|
Chief Financial Officer |
|
Non-Employee Directors: |
|
|
|
|
|
Mark C. McKenna(2)(3) |
|
44 |
|
Chair and Director |
|
Jennifer Fox(1)(2) |
|
52 |
|
Director |
|
Andrew Gottesdiener, M.D.(1) |
|
33 |
|
Director |
|
Peter Harwin(1)(3) |
|
38 |
|
Director |
|
William (BJ) Jones, Jr.(2)(3) |
|
60 |
|
Director |
|
Tomas Kiselak |
|
37 |
|
Director |
|
Nimish Shah(3) |
|
46 |
|
Director |
|
(1)Member of the Audit Committee
(2)Member of the Compensation Committee
(3)Member of the Nominating and Corporate Governance Committee
Our business and affairs are managed by and under the direction of our Board, which currently consists of eight members. Our Board is divided into three classes, with members of each class holding office for staggered three-year terms. There are currently three Class I directors, Michael Henderson, M.D., Peter Harwin and Andrew Gottesdiener, M.D., whose terms expire at the 2024 Annual Meeting of Stockholders; two Class II directors, Tomas Kiselak and Nimish Shah, whose terms expire at the 2025 Annual Meeting of Stockholders; and three Class III directors, William (BJ) Jones, Jr., Jennifer Fox and Mark C. McKenna, whose terms expire at the 2026 Annual Meeting of Stockholders. Our executive officers are elected by the Board and serve at the Board’s discretion.
The following is a biographical summary of the experience of our executive officers and directors:
Executive Officers and Employee Director
Michael Henderson, M.D. has served as a member of our Board since June 2023, as a member of the board of managers of Apogee Therapeutics, LLC from 2022 to July 2023 and as our Chief Executive Officer since September 2022. Dr. Henderson is an experienced biotechnology executive with expertise in business leadership, drug development, and commercial strategy. He has overseen the creation of multiple companies, launched a significant number of drug development programs, and led teams to two FDA approvals, to date. Prior to joining Apogee, Dr. Henderson served as Chief Business Officer of BridgeBio Pharma, Inc. (Nasdaq: BBIO), a commercial-stage biopharmaceutical company, from January 2020 to September 2022, where he was responsible for furthering the overarching strategy of BridgeBio, identifying and investing in new technologies and running business development and operations. Prior to holding that position, he spent two years serving as BridgeBio’s Senior Vice President, Asset Acquisition, Strategy and Operations, where he was responsible for business development, strategy and operations. Dr. Henderson joined BridgeBio as Vice President of Asset Acquisition, Strategy and Operations in April 2016. Dr. Henderson also served as the Chief Executive Officer of a number of BridgeBio’s subsidiaries. Prior to BridgeBio, Dr. Henderson worked at McKinsey & Company, a global management consulting firm, from January 2015 to April 2016 and prior to that, he co-founded PellePharm, Inc., a biotechnology company, in August 2011. Dr. Henderson has served on the board of directors of ARYA Sciences Acquisition Corp IV (Nasdaq: ARYD), a special purpose acquisition company focused on the healthcare industry, since February 2021 and Spyre Therapeutics (Nasdaq: SYRE), a biotechnology company, since June 2023.
171
Dr. Henderson received a B.A. in global health from Harvard University and an M.D. from Stanford University.
We believe Dr. Henderson is qualified to serve on our Board because of his experience in business leadership, drug development, and commercial strategy in the area of life sciences.
Carl Dambkowski, M.D. has served as our Chief Medical Officer since September 2022. Prior to joining Apogee, Dr. Dambkowski served as a strategic and clinical leader for a variety of companies, including as Chief Medical Officer of QED Therapeutics, Inc., a private biotechnology company, from July 2021 to September 2022; Chief Strategy Officer and EVP of Operations of Origin Biosciences, Inc., a private bioecology company, from March 2018 to June 2021; and Chief Medical Officer of Navire Pharma, Inc., a private biotechnology company, from January 2020 to September 2022, where he served as the clinical lead starting prior to IND for BBP-398 through the out licensing of the compound to Bristol-Myers Squibb based on initial clinical data and for low-dose infigratinib in achondroplasia through initial proof-of-concept data. He was part of the core team that brought TRUSELTIQ® (infigratinib) and NULIBRY® (fosdenopterin) through regulatory review and FDA approval at QED Therapeutics and Origin Biosciences, respectively. From July 2016 to March 2018, Dr. Dambkowski was an associate at McKinsey & Company, a global management consulting firm, where he advised biotech and pharmaceutical companies across the world on a range of research and development activities. Dr. Dambkowski co-founded Novonate, Inc., a private medical device company focused on building life-saving devices for neonates, in January 2015. Dr. Dambkowski has coauthored numerous peer-reviewed publications and scientific abstracts and is a named inventor on multiple published and granted patents. Dr. Dambkowski was trained as a physician at Stanford University, where he also received his M.D. with a concentration in bioengineering. He also received a B.A. (with honors) from Stanford University and an M.A. from Columbia University.
Jane Pritchett Henderson has served as our Chief Financial Officer since January 2023. Prior to joining Apogee, Ms. Henderson served as the Chief Financial Officer and Chief Business Officer of Adagio Therapeutics, Inc. (now Invivyd, Inc.) (Nasdaq: IVVD), a biotechnology company developing antibody therapeutics for coronaviruses, from December 2020 to November 2022. Prior to joining Adagio Therapeutics, Ms. Henderson served as Chief Financial Officer of Turnstone Biologics Corp., a private viral immuno-oncology company, from June 2018 to December 2020, as Chief Financial Officer and Senior Vice President of Corporate Development of Voyager Therapeutics, Inc. (Nasdaq: VYGR), a gene therapy company, from January 2017 to June 2018, and as the Senior Vice President, Chief Financial and Business Officer of Kolltan Pharmaceuticals, Inc., a private oncology biopharmaceutical company, from February 2013 until November 2016, when Kolltan Pharmaceuticals was acquired by Celldex Therapeutics, Inc. Prior to Kolltan Pharmaceuticals, Ms. Henderson served in various financial and business development executive roles at biopharmaceutical companies after spending almost 20 years in health care investment banking. During the past five years, Ms. Henderson has served on the board of directors of Akero Therapeutics, Inc. (Nasdaq: AKRO), a biotechnology company, since April 2019, and Ventus Therapeutics, Inc., a private biopharmaceutical company. She also served on the board of directors of IVERIC Bio, Inc. (Nasdaq: ISEE), a biopharmaceutical company, from January 2018 until its acquisition by Astellas Pharma Inc. in July 2023, and Sesen Bio Inc. (Nasdaq: SESN), a biopharmaceutical company, from October 2018 to November 2021. Ms. Henderson also serves on the Dedman College Executive Board of Southern Methodist University. Ms. Henderson received a B.S. in psychology from Duke University.
Non-employee Directors
Mark McKenna has served as a member of our Board since August 2023. Mr. McKenna has served as Chief Investment Officer and Managing Director of McKenna Capital Partners, a family office dedicated to investing in breakthrough treatments for debilitating diseases, since June 2023. Mr. McKenna most recently served as the President and Chief Executive Officer and as a member of the board of directors of Prometheus Biosciences, Inc., a clinical stage biotechnology company, from September 2019 to June 2023, when Prometheus was acquired by Merck & Co., Inc., and as Chairman of the board of Prometheus from August 2021 to June 2023. Prior to Prometheus, he served as President of Salix Pharmaceuticals, Inc., a pharmaceutical company and wholly-owned subsidiary of Bausch Health Companies, Inc., from March 2016 through August 2019. Prior to Salix, Mr. McKenna spent more than a decade in various roles with Bausch + Lomb, also a division of Bausch Health Companies, Inc., most recently as Senior Vice President and General Manager of its U.S. Vision Care business. Before joining Bausch + Lomb, he held several positions with Johnson & Johnson. Mr. McKenna has served on the board of directors of Spyre Therapeutics, Inc. (Nasdaq: SYRE), a biotechnology company, since February 2024.
172
Mr. McKenna received a B.S. in Marketing from Arizona State University and an M.B.A. from Azusa Pacific University. We believe Mr. McKenna is qualified to serve on our Board because of his extensive experience as an executive officer in the biopharmaceutical industry.
Jennifer Fox has served as a member of our Board since June 2023 and as a member of the board of managers of Apogee Therapeutics, LLC from May 2023 to July 2023. Ms. Fox has served as the Chief Business Officer and Chief Financial Officer of Zenas BioPharma, Inc., a biopharmaceutical company, since December 2023.
Prior to joining Zenas BioPharma, Ms. Fox served as Chief Financial Officer of Nuvation Bio Inc. (NYSE: NUVB), a biopharmaceutical company, from October 2020 to November 2023. Prior to Nuvation Bio, Ms. Fox served as Managing Director, Co-Head of North America Healthcare Corporate and Investment Banking Group at Citigroup (NYSE: C), a global investment bank, from June 2015 to October 2020. From February 2006 to June 2015, Ms. Fox served as Managing Director at Deutsche Bank (NYSE: DB), a global investment bank, and most recently, as Co-Head of Life Sciences Investment Banking Group. Ms. Fox has served on the board of directors of ProKidney Corp. (Nasdaq: PROK), a biotechnology company, since July 2022. Ms. Fox received B.S. degrees in finance and marketing from Manhattan College. We believe Ms. Fox is qualified to serve on our Board because of her experience in the healthcare investment banking industry and as a lead advisor to life sciences companies on financing and strategic transactions.
Andrew Gottesdiener, M.D. co-founded Apogee and has served as a member of our Board since June 2023 and as a member of the board of managers of Apogee Therapeutics, LLC from 2022 to July 2023. Dr. Gottesdiener is a partner at Venrock Healthcare Capital Partners, an investment firm, in its New York office, where he focuses on healthcare investments. Prior to joining Venrock full-time in September 2018, Dr. Gottesdiener received an M.D. from Weill Cornell Medical College during which time he received an HHMI summer fellowship for basic science research. He also has an M.B.A. from Columbia Business School. Dr. Gottesdiener received an A.B. in economics from Washington University in St. Louis. We believe Dr. Gottesdiener is qualified to serve on our Board because of his extensive experience in the biotechnology industry providing leadership in biotechnology investments.
Peter Harwin has served as a member of our Board since June 2023 and as a member of the board of managers of Apogee Therapeutics, LLC from 2022 to July 2023. Mr. Harwin is a Managing Member at Fairmount Funds Management LLC, a healthcare investment firm he co-founded in April 2016. Prior to Fairmount, Mr. Harwin was a member of the investment team at Boxer Capital, LLC, an investment fund that was part of the Tavistock Group, based in San Diego. Mr. Harwin also serves as chairman of the board of directors of Cogent Biosciences, Inc. (Nasdaq: COGT) and is a director of Viridian Therapeutics, Inc. (Nasdaq: VRDN), Spyre Therapeutics, Inc. (Nasdaq: SYRE) and Paragon Therapeutics, Inc. Mr. Harwin received a B.B.A. from Emory University. We believe Mr. Harwin is qualified to serve on our Board because of his experience serving as a director of biotechnology companies and as a manager of funds specializing in the area of life sciences.
William (BJ) Jones, Jr. has served as a member of our Board since June 2023 and as a member of the board of managers of Apogee Therapeutics, LLC from May 2023 to July 2023. Mr. Jones previously served as Chief Commercial Officer, Migraine and Common Diseases of Biohaven Pharmaceuticals Holding Company Ltd., a biopharmaceutical company and subsidiary of Pfizer Inc. (NYSE: PFE), where he was responsible for building the company’s commercial capability and launching its first FDA-approved product (Nurtec ODT), from April 2019 to December 2022. Prior to Biohaven Pharmaceuticals, Mr. Jones served as Vice President, Head of Sales and Commercial Operations for the general medicine business unit of Takeda Pharmaceutical Company Limited (NYSE: TAK), a pharmaceutical company, from January 2016 to March 2019. Mr. Jones has served on the board of directors of Akili, Inc. (Nasdaq: AKLI), a digital medicine company, since August 2022. Mr. Jones received a B.S. in human factors engineering from the U.S. Air Force Academy, an M.S. in industrial engineering from Texas A&M University and an M.B.A. from the Stanford University Graduate School of Business. We believe Mr. Jones is qualified to serve on our Board because of his experience in drug development and commercial strategy in the pharmaceutical industry.
Tomas Kiselak has served as a member of our Board since June 2023 and as a member of the board of managers of Apogee Therapeutics, LLC from 2022 to July 2023. Mr. Kiselak is a Managing Member at Fairmount Funds Management LLC, a healthcare investment firm he co-founded in April 2016. Prior to Fairmount, Mr. Kiselak was a managing director at RA Capital Management, LLC, a healthcare and life science investment firm. Mr.
173
Kiselak currently serves as the chairman of the board of directors of Viridian Therapeutics, Inc. (Nasdaq: VRDN) and as a director for Spyre Therapeutics, Inc. (Nasdaq: SYRE), Dianthus Therapeutics, Inc. (Nasdaq: DNTH) and for several private companies. He received a B.S. in neuroscience and economics from Amherst College. We believe Mr. Kiselak is qualified to serve on our Board because of his experience advising biotechnology companies and as a manager of funds specializing in the area of life sciences.
Nimish Shah co-founded Apogee and has served as a member of our Board since June 2023 and as a member of the board of managers of Apogee Therapeutics, LLC from 2022 to July 2023. Mr. Shah is a partner at Venrock Healthcare Capital Partners, an investment firm, where he predominately works on Venrock’s public and cross-over biotech funds. Mr. Shah originally joined Venrock in 2013 and has been investing in public and private healthcare companies since 2010. Mr. Shah previously served as a director for Instil Bio, Inc. (Nasdaq: TIL) and board observer for LianBio (NASDAQ: LIAN), Biohaven Ltd. (NYSE: BHVN) and Viridian Therapeutics, Inc. (Nasdaq: VRDN). He is also a board observer for Dianthus Therapeutics, Inc. Mr. Shah received a B.S. in pharmacy from Rutgers College of Pharmacy, an M.P.H. from the Mailman School of Public Health at Columbia University and an M.B.A. from Columbia Business School. He is a member of the Columbia Business School Healthcare and Pharmaceutical Management Advisory Board. We believe Mr. Shah is qualified to serve on our Board because of his extensive experience in the biotechnology industry providing leadership in biotechnology investments.
Code of Business Conduct and Ethics
Our Board has adopted a Business Code of Conduct and Ethics (“the Code of Conduct”) that establishes the standards of ethical conduct applicable to all our directors, officers and employees, including our principal executive officer, principal financial officer, principal accounting officer or controller, or persons performing similar functions. The full text of our Code of Conduct is posted on our website at www.apogeetherapeutics.com. It addresses, among other matters, compliance with laws and policies, conflicts of interest, corporate opportunities, regulatory reporting, external communications, confidentiality requirements, insider trading, proper use of assets and how to report compliance concerns.
We intend to disclose any amendments to the Code of Conduct, or any waivers of its requirements, on our website to the extent required by applicable rules. The Audit Committee is responsible for applying and interpreting our Code of Conduct in situations where questions are presented to it.
Audit Committee and Audit Committee Financial Expert
We have a separately designated standing Audit Committee. The members of our Audit Committee are Jennifer Fox (Chair), Peter Harwin and Andrew Gottesdiener, M.D., each of whom qualifies as an “independent” director for audit committee purposes, as defined under Nasdaq listing rules and the rules and regulations established by the SEC. Jennifer Fox qualifies as an “audit committee financial expert,” as that term is defined under the rules and regulations established by the SEC, and all members of the Audit Committee are “financially literate” under Nasdaq listing rules.
Item 11. Executive Compensation.
Overview
This section describes the material elements of compensation awarded to, earned by or paid to each of our named executive officers (“NEOs”) in 2022 and 2023. We are an “emerging growth company,” within the meaning of the JOBS Act and a smaller reporting company under the Exchange Act and have elected to comply with the reduced compensation disclosure requirements available to emerging growth companies under the JOBS Act. Our NEOs for 2023 were Michael Henderson, M.D., Carl Dambkowski, M.D., and Jane Pritchett Henderson. This section also provides qualitative information regarding the manner and context in which compensation is awarded to and earned by our NEOs and is intended to place in perspective the data presented in the tables and narrative that follow.
Our current executive compensation program is intended to align executive compensation with our business objectives and to enable us to attract, retain and reward executive officers who contribute to our long-term success. The compensation paid or awarded to our executive officers is generally based on a qualitative assessment of each individual’s performance compared against the business objectives established for the fiscal year as well as market peer group data and our historical compensation practices.
174
In the case of new hire executive officers, their compensation is primarily determined based on the negotiations of the parties, as well as our historical compensation practices and market peer group data. For 2022 and 2023, the material elements of our executive compensation program were base salary, annual cash bonuses awards and long-term equity incentives in the form of incentive units prior to the IPO and stock options following the IPO.
In preparing to become a public company, we conducted a thorough review of all elements of our executive compensation program, including the function and design of our equity incentive program. We expect that our executive compensation program will continue to evolve to reflect our status as a newly publicly traded company, while still supporting our overall business and compensation objectives. In connection with the IPO, our Board retained the services of Alpine Rewards, LLC, an independent executive compensation consultant, to help advise on our post-IPO executive compensation program, as described further below.
Summary Compensation Table
The following table sets forth the total compensation that was awarded to, earned by or paid to our NEOs for services rendered during the years ended December 31, 2022 and 2023 (respectively, the “2022 Fiscal Year” and the “2023 Fiscal Year”).
|
|
|
|
|
|
|
|
|
|
|
|
|
STOCK |
|
ALL OTHER |
|
|
|
||
|
|
|
|
SALARY |
|
BONUS |
|
OPTIONS |
|
AWARDS |
|
COMPENSATION |
|
TOTAL |
||||||
NAME AND PRINCIPAL POSITION |
|
YEAR |
|
($) |
|
($)(2) |
|
($)(3) |
|
($)(4) |
|
($)(5) |
|
($) |
||||||
Michael Henderson, M.D. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chief Executive Officer |
|
2023 |
|
$ |
564,833 |
|
$ |
606,375 |
|
$ |
7,500,000 |
|
|
— |
|
|
— |
|
$ |
8,671,208 |
|
|
2022(1) |
|
$ |
145,833 |
|
$ |
167,123 |
|
|
— |
|
$ |
6,079,410 |
|
$ |
56,750 |
|
$ |
6,449,116 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Carl Dambkowski, M.D. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chief Medical Officer |
|
2023 |
|
$ |
477,083 |
|
$ |
393,750 |
|
$ |
3,300,000 |
|
|
— |
|
|
— |
|
$ |
4,170,833 |
|
|
2022(6) |
|
$ |
176,250 |
|
$ |
212,932 |
|
|
— |
|
$ |
1,194,638 |
|
|
— |
|
$ |
1,583,820 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Jane Pritchett Henderson(7) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chief Financial Officer |
|
2023 |
|
$ |
469,311 |
|
$ |
374,332 |
|
$ |
3,300,000 |
|
$ |
881,270 |
|
|
— |
|
$ |
5,024,913 |
(1) |
Dr. Henderson was appointed as our Chief Executive Officer in September 2022. Prior to this appointment, Dr. Henderson served exclusively as a member of our Board. As such, the amounts reported for Dr. Henderson for 2022 are pro-rated to reflect his commencement date. |
(2) |
The amount in this column includes for each of Dr. Dambkowski, Dr. Henderson, and Ms. Henderson discretionary annual bonuses with respect to the 2023 Fiscal Year. See the subsection titled “Narrative Disclosure to the Summary Compensation Table—Annual Cash Bonuses” below for additional information regarding these awards. |
(3) |
Amount represents the aggregate grant date fair value of stock options, computed in accordance with Financial Accounting Standards Board (FASB) Accounting Standards Codification Topic 718 (ASC Topic 718), rather than the amounts paid to or realized by the named individual. We provide information regarding the assumptions used to calculate the value of these awards in Note 2 to our audited consolidated financial statements included elsewhere in this Annual Report. These amounts do not reflect the actual economic value that may be realized by the NEOs. |
(4) |
Prior to our IPO in July 2023, we did not grant stock options; however, we granted to each of Dr. Henderson, Dr. Dambkowski, and Ms. Henderson incentive units under the Second Amended and Restated Limited Liability Company Agreement of Apogee Therapeutics, LLC (the “LLC Agreement”), the economics of which are similar to stock options. The amounts disclosed represent the aggregate grant date fair value of incentive units granted under the LLC Agreement during the indicated fiscal year computed in accordance with ASC Topic 718. The assumptions used in calculating the grant date fair value of the incentive units during the 2022 Fiscal year are set forth in the notes to our audited consolidated financial statements included elsewhere in this Annual Report. These amounts do not reflect the actual economic value that may be realized by the NEOs. |
175
(5) |
Amounts reported in the “All Other Compensation” column for Dr. Henderson for 2022 include board fees paid for his service as a member of our Board prior to his appointment as our Chief Executive Officer in September 2022. |
(6) |
Dr. Dambkowski was appointed as our Chief Medical Officer in September 2022. Prior to his appointment, Dr. Dambkowski provided consulting services to the Company. As such, the amounts reported for Dr. Dambkowski for 2022 are pro-rated to reflect his commencement date. In addition, Dr. Dambkowski’s salary for 2022 also includes consulting fees paid for his service as a consultant to the Company prior to his appointment as our Chief Medical Officer. |
(7) |
Ms. Henderson was appointed as our Chief Financial Officer in January 2023. As such, the amounts reported for Ms. Henderson are pro-rated to reflect her commencement date. |
Narrative Disclosure to Summary Compensation Table
Employment Agreements
Michael Henderson, M.D.
Dr. Henderson entered into an amended and restated employment agreement with the Company effective August 25, 2023 under which Dr. Henderson continues to serve as our Chief Executive Officer. Pursuant to the terms of his amended and restated employment agreement, for his services as the Company’s Chief Executive Officer, Dr. Henderson is eligible to receive an annual base salary of $630,000, a target annual bonus of 55%, and participation in our employee benefit plans as in effect from time to time. Dr. Henderson’s amended and restated employment agreement also provides that Dr. Henderson may be eligible for severance benefits upon certain terminations of employment pursuant to the terms of our Executive Severance Policy (as defined below), as described below under the subsection titled “Additional Narrative Disclosure — Potential Payments Upon Termination or Change in Control.”
Carl Dambkowski, M.D.
We entered into an amended and restated employment agreement with Dr. Dambkowski effective August 25, 2023, under which Dr. Dambkowski continues to serve as our Chief Medical Officer. Under his amended and restated employment agreement, Dr. Dambkowski is eligible to receive an annual base salary of $500,000, a target annual bonus of 45%, and participation in our employee benefit plans as in effect from time to time.
Dr. Dambkowski’s amended and restated employment agreement also provides that Dr. Dambkowski may be eligible for severance benefits upon certain terminations of employment pursuant to the terms of our Executive Severance Policy, as described below under the subsection titled “Additional Narrative Disclosure — Potential Payments Upon Termination or Change in Control.”
Jane Pritchett Henderson
We entered into an amended and restated employment agreement with Ms. Henderson effective August 25, 2023, under which Ms. Henderson continues to serve as our Chief Financial Officer. Under her employment agreement, Ms. Henderson is eligible to receive an annual base salary of $500,000, a target annual bonus of 45%, and participation in our employee benefit plans as in effect from time to time.
Ms. Henderson’s amended and restated employment agreement also provides that Ms. Henderson may be eligible for severance benefits upon certain terminations of employment pursuant to the terms of our Executive Severance Policy, as described below under the subsection titled “Additional Narrative Disclosure — Potential Payments Upon Termination or Change in Control.”
176
Base Salary
We use base salaries to provide our NEOs with a fixed, base level of compensation. In setting the base salaries for our NEOs, we consider their experience, skills, knowledge and responsibilities, as well as market peer group data. The base salaries of our NEOs per their employment agreements are described above.
In December 2023, our Board approved an increase in the base salaries of Dr. Henderson to $661,500 (from $630,000), of Dr. Dambkowski to $525,000 (from $500,000) and of Ms. Henderson to $525,000 (from $500,000) effective January 1, 2024.
Annual Cash Bonuses
During the 2023 Fiscal Year, we did not maintain a formal performance-bonus program. Each of our NEOs was instead eligible to receive a discretionary bonus pursuant to the terms of their respective employment agreements in an amount determined by the Board. For the 2023 Fiscal Year, the target annual cash bonus for each of our NEOs was as follows:
|
|
TARGET ANNUAL CASH BONUS |
NAME |
|
(% OF BASE SALARY) |
Michael Henderson, M.D. |
|
55% |
Carl Dambkowski, M.D. |
|
45% |
Jane Pritchett Henderson |
|
45% |
The amount of each NEO’s actual annual cash bonus was determined by the Board based on its assessment of each NEO’s individual performance as well as the Board’s assessment of overall company performance. Annual bonuses with respect to the 2023 Fiscal Year were approved by the Board in the following amounts:
|
|
2023 ANNUAL CASH |
|
NAME |
|
BONUS |
|
Michael Henderson, M.D. |
|
$ |
606,375 |
Carl Dambkowski, M.D. |
|
$ |
393,750 |
Jane Pritchett Henderson |
|
$ |
374,332 |
Incentive Unit and Stock Option Awards
Prior to the IPO, we granted long-term incentive compensation to our NEOs pursuant to the LLC Agreement in the form of incentive units. On July 13, 2023, in connection with our IPO, all outstanding incentive units were exchanged for shares of common stock and holders of such incentive units under the LLC Agreement received a number of shares of common stock (with respect to vested incentive units) or restricted common stock (with respect to unvested incentive units) of Apogee Therapeutics, Inc. based on the fair value per incentive unit. Following the IPO, we have granted long-term incentive compensation to our NEOs in the form of stock options pursuant to our 2023 Plan.
Incentive Units
On October 3, 2022, Dr. Henderson received 1,527,777 incentive units under the LLC Agreement and received an additional 1,375,292 incentive units under the LLC Agreement on December 21, 2022. Additionally, on October 17, 2022, Dr. Henderson received 1,634,524 incentive units under the LLC Agreement the vesting of which was subject to the occurrence of a specified dilution event on or prior to December 31, 2022, which dilution event did occur within such timeframe. In connection with the IPO, the foregoing incentive units held by Dr. Henderson were exchanged for 1,489,487 shares of common stock, consisting of (i) 350,615 shares of fully vested common stock as of the date of the exchange, (ii) 851,495 shares of restricted common stock, which vest in 34 equal monthly installments through May 2, 2026, and (iii) 287,377 shares of restricted common stock, one quarter of which vested on December 14, 2023, with the remaining three quarters vesting in equal monthly installments over the following three years, in each case subject to Dr. Henderson’s continued service to us through each applicable vesting date.
177
On October 3, 2022, Dr. Dambkowski received a grant of 347,222 incentive units under the LLC Agreement and received an additional 807,802 incentive units under the LLC Agreement on December 21, 2022. In connection with the IPO, the foregoing incentive units held by Dr. Dambkowski were exchanged for 300,788 shares of restricted common stock, consisting of (i) 131,992 shares of restricted common stock, one quarter of which vested on September 16, 2023, with the remaining three quarters vesting in equal monthly installments over the following three years, and (ii) 168,796 shares of restricted common stock, one quarter of which vested on December 14, 2023, with the remaining three quarters vesting in equal monthly installments over the following three years, in each case subject to Dr. Dambkowski’s continued service to us through each applicable vesting date.
On February 1, 2023, Ms. Henderson received 990,020 incentive units under the LLC Agreement. In connection with the IPO, the foregoing incentive units held by Ms. Henderson were exchanged for 206,871 shares of restricted common stock, one quarter of which vested on February 1, 2024, with the remaining three quarters vesting in equal monthly installments over the following three years, subject to Ms. Henderson’s continued service to us through each applicable vesting date.
Stock Options
On December 18, 2023, each of Dr. Henderson, Dr. Dambkowski, and Ms. Henderson received a grant of stock options pursuant to the 2023 Plan in the amounts of 398,512 options, 175,345 options, and 175,345 options, respectively. The options have a per share exercise price of $22.86 and vest in forty-eight equal monthly installments over a four-year period from the date of grant, subject to recipient’s continued service to us through each applicable vesting date.
Other Compensation Elements
We offer participation in broad-based retirement, health and welfare plans to all of our employees. We currently maintain a retirement plan intended to provide benefits under section 401(k) of the Code (as defined below) in which employees, including the NEOs, are allowed to contribute portions of their eligible compensation to a tax-qualified retirement account. Effective January 1, 2024, we established a 401(k) matching program which enables our employees, including the NEOs, to receive a dollar-for-dollar Company match of up to 4% of his or her compensation to the 401(k) fund, subject to limitations under applicable law. See the subsection titled “Additional Narrative Disclosure — Retirement Benefits” for more information.
178
Outstanding Equity Awards at 2023 Fiscal Year-End Table
The following table summarizes equity awards held by our NEOs as of the end of the 2023 Fiscal Year. Prior to the IPO, our NEOs each held incentive units pursuant to the LLC Agreement, which were exchanged for shares of common stock (with respect to vested incentive units) or restricted common stock (with respect to unvested incentive units) in connection with our IPO. Each of the equity awards in the table below may be subject to accelerated vesting, as described below under the subsection titled “Additional Narrative Disclosure — Potential Payments Upon Termination or Change in Control.”
|
|
STOCK OPTIONS |
|
STOCK AWARDS |
||||||||
|
|
NUMBER OF |
|
NUMBER OF |
|
|
|
|
|
|
|
|
|
|
SECURITIES |
|
SECURITIES |
|
|
|
|
|
|
|
MARKET |
|
|
UNDERLYING |
|
UNDERLYING |
|
|
|
|
|
|
|
VALUE OF |
|
|
UNEXERCISED |
|
UNEXERCISED |
|
|
|
|
|
NUMBER OF |
|
SHARES |
|
|
OPTIONS |
|
OPTIONS |
|
OPTION |
|
OPTION |
|
SHARES |
|
THAT HAVE |
|
|
EXERCISABLE |
|
UNEXERCISABLE |
|
EXERCISE |
|
EXPIRATION |
|
THAT HAVE |
|
NOT VESTED |
NAME |
|
(#) |
|
(#)(1) |
|
PRICE |
|
DATE |
|
NOT VESTED |
|
($) |
Michael Henderson, M.D. |
|
— |
|
398,512 |
|
22.86 |
|
12/18/2033 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
726,276 |
(2) |
20,292,151 |
|
|
|
|
|
|
|
|
|
|
215,533 |
(3) |
6,021,992 |
Carl Dambkowski, M.D. |
|
— |
|
175,345 |
|
22.86 |
|
12/18/2033 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
90,745 |
(4) |
2,535,415 |
|
|
|
|
|
|
|
|
|
|
126,597 |
(5) |
3,537,120 |
Jane Pritchett Henderson |
|
— |
|
175,345 |
|
22.86 |
|
12/18/2033 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
206,871 |
(6) |
5,779,976 |
(1) |
Shares subject to the option vest in 48 monthly installments beginning on December 18, 2023, subject to the recipient’s continued service to us through each applicable vesting date. |
(2) |
25% of the awards vested on May 2, 2023, with the remainder vesting in equal monthly installments until May 2026, subject to Dr. Henderson’s continued service to us through each applicable vesting date. |
(3) |
25% of the awards vested on December 14, 2023, with the remainder vesting in equal monthly installments until December 2026, subject to Dr. Henderson’s continued service to us through each applicable vesting date. |
(4) |
25% of the awards vested on September 16, 2023, with the remainder vesting in equal monthly installments until September 2026, subject to Dr. Dambkowski’s continued service to us through each applicable vesting date |
(5) |
25% of the awards vested on December 14, 2023, with the remainder vesting in equal monthly installments until December 2026, subject to Dr. Dambkowski’s continued service to us through each applicable vesting date. |
(6) |
25% of the awards vested on February 1, 2024, with the remainder vesting in equal monthly installments until February 2027, subject to Ms. Henderson’s continued service to us through each applicable vesting date. |
Additional Narrative Disclosure
Retirement Benefits
We have not maintained, and do not currently maintain, a defined benefit pension plan or nonqualified deferred compensation plan. We maintain a 401(k) plan in which employees, including our NEOs, are allowed to contribute portions of their eligible compensation to a tax-qualified retirement account.
179
Potential Payments Upon Termination or Change in Control
Executive Severance Policy
In June 2023, our Board approved an executive severance policy that covers Dr. Henderson, Dr. Dambkowski, and Ms. Henderson, which was further amended in August 2023 (Executive Severance Policy). Potential payments in connection with a change in control to each of Dr. Henderson, Dr. Dambkowski, and Ms. Henderson are governed by the Executive Severance Policy.
Under the Executive Severance Policy, Dr. Henderson is eligible to receive upon a termination by us without cause (as defined below) or a resignation for good reason (as defined below) that is not within the change in control period (as defined below): (i) 1.5 times his annual base salary, (ii) payment of any bonus amount earned but unpaid for the year prior to the year of termination, (iii) payment of a pro-rata portion of the target bonus that he would have earned for the year in which the termination occurs, (iv) subsidized continued health coverage for up to 18 months, and (v) the immediate acceleration of 30% of his equity-based awards. In addition, upon a termination by us without cause or a resignation for good reason, occurring within the change in control period, Dr. Henderson will be eligible to receive: (i) 1.5 times his annual base salary, (ii) payment of any bonus amount earned but unpaid for the year prior to the year of termination, (iii) payment of the full target bonus he would have earned for the year in which the termination occurs, (iv) subsidized continued health coverage for up to 18 months, and (v) the immediate acceleration of 100% of his equity-based awards.
Under the Executive Severance Policy, Dr. Dambkowski and Ms. Henderson are eligible to receive upon a termination by us without cause or a resignation for good reason (as defined below) that is not within the change in control period:
(i) 1.0 times annual base salary, (ii) payment of any bonus amount earned but unpaid for the year prior to the year of termination, (iii) payment of a pro-rata portion of the target bonus that he or she would have earned for the year in which the termination occurs, and (iv) subsidized continued health coverage for up to 12 months. In addition, upon a termination by us without cause or a resignation for good reason, occurring within the change in control period, Dr. Dambkowski and Ms. Henderson will be eligible to receive the benefits listed in items (i), (ii), and (iv) and the payment of the full target bonus he or she would have earned for the year in which the termination occurs and the immediate acceleration of 100% of his or her equity-based awards.
For purposes of the Executive Severance Policy, the following definitions apply:
180
2023 Equity Incentive Plan
Our Board and stockholders adopted our 2023 Equity Incentive Plan (the “2023 Plan”), which became effective immediately following the Reorganization. The purpose of the 2023 Plan is to promote and closely align the interests of our employees, officers, non-employee directors and other service providers and our stockholders by providing stock-based compensation and other performance-based compensation. The 2023 Plan allows for the grant of stock options, both incentive stock options and “non-qualified” stock options; stock appreciation rights (SARs), alone or in conjunction with other awards; restricted stock and restricted stock units; incentive bonuses, which may be paid in cash, stock, or a combination thereof; and other stock-based awards. We refer to these collectively herein as Awards.
181
2023 Employee Stock Purchase Plan
Our Board and stockholders adopted our 2023 Employee Stock Purchase Plan (the “ESPP”), which became effective immediately following the Reorganization. The purpose of the ESPP is to encourage and enable our eligible employees to acquire a proprietary interest in us through the ownership of our common stock.
DIRECTOR COMPENSATION
The following table presents all of the compensation awarded to, earned by, or paid to our non-employee directors during the year ended December 31, 2023. We have reimbursed and will continue to reimburse all of our non-employee directors for their reasonable out-of-pocket expenses incurred in attending board of directors and committee meetings.
|
|
OPTION |
|
STOCK |
|
FEES EARNED |
|
|
|
|||
|
|
AWARDS |
|
AWARDS |
|
OR PAID IN |
|
|
|
|||
NAME |
|
($)(1)(2) |
|
($)(3) |
|
CASH ($) |
|
TOTAL ($) |
||||
Peter Harwin |
|
$ |
642,823 |
|
|
— |
|
$ |
25,750 |
|
$ |
668,573 |
Jennifer Fox |
|
|
— |
|
$ |
381,323 |
|
$ |
33,250 |
|
$ |
414,573 |
Andrew Gottesdiener, M.D. |
|
$ |
642,823 |
|
|
— |
|
$ |
23,750 |
|
$ |
666,573 |
William (BJ) Jones, Jr. |
|
|
— |
|
$ |
381,323 |
|
$ |
30,333 |
|
$ |
411,656 |
Tomas Kiselak |
|
$ |
642,823 |
|
|
— |
|
$ |
20,000 |
|
$ |
662,823 |
Mark McKenna |
|
$ |
940,000 |
|
|
— |
|
$ |
32,870 |
|
$ |
972,870 |
Nimish Shah |
|
$ |
642,823 |
|
|
— |
|
$ |
22,000 |
|
$ |
664,823 |
(1) |
The amounts disclosed represent the aggregate grant date fair value of the stock options and awards granted to our non-employee directors during 2023 under our 2023 Plan, computed in accordance with ASC Topic 718. The assumptions used in calculating the grant date fair value of the stock options are set forth in Note 2 to our audited consolidated financial statements included elsewhere in this Annual Report. These amounts do not reflect the actual economic value that may be realized by the director. |
(2) |
In 2023, Messrs. Harwin, Gottesdiener, Kiselak and Shah were awarded 47,758 option each to purchase shares of our common stock, as described further below. Mr. Mckenna was awarded 50,000 options to purchase shares of our common stock, of which 5,555 were vested as of December 31, 2023, as described further below. |
(3) |
In 2023, Ms. Fox and Mr. Jones were each awarded 34,824 shares of restricted common stock, as described further below. |
In July 2023, in connection with the IPO, we granted Messrs, Harwin, Kiselak, Shah, and Gottesdiener 47,758 stock options pursuant to our 2023 Plan, with a per share exercise price of $17.00, subject to annual vesting over three years commencing on July 13, 2023 subject to the director’s continued service to us through each applicable vesting date.
In connection with our IPO, Ms. Fox’s and Mr. Jones’s pre-IPO incentive units under the LLC Agreement were exchanged for 34,824 shares of restricted common stock, one quarter of which will vest on May 28, 2024, and May 26, 2024, respectively, with the remaining three quarters vesting in equal monthly installments over the following three years, subject to each director’s continued service to us through each applicable vesting date.
In August 2023, we granted Mr. McKenna 50,000 stock options pursuant to our 2023 Plan, with a per share exercise price of $23.60, which such options vest monthly in thirty-six equal installments commencing on August 17, 2023 subject to his continued service to us through each applicable vesting date. We granted an additional 100,000 stock options to Mr. McKenna outside of the 2023 Plan with the same vesting conditions described in the preceding sentence, which such options are contingent upon approval at our 2024 Annual Meeting of Stockholders.
182
Director Compensation Policy
Our Board approved our amended director compensation policy for our non-employee directors which went into effect in February 2024 and which consists of the following:
| ● | an annual cash retainer of $40,000 for service on the Board (other than as Chair); |
| ● | an annual cash retainer of $70,000 for service as Chair of the Board; |
| ● | an annual cash retainer of $15,000 for service as chairperson of the Audit Committee of the Board; |
| ● | an annual cash retainer of $10,000 for service as chairperson of the Compensation Committee of the Board; |
| ● | an annual cash retainer of $8,000 for service as chairperson of the Nominating and Corporate Governance Committee of the Board; |
| ● | an annual cash retainer of $7,500 for service on the Audit Committee of the Board (other than as chairperson); |
| ● | an annual cash retainer of $5,000 for service on the Compensation Committee of the Board (other than as chairperson); |
| ● | an annual cash retainer of $4,000 for service on the Nominating and Corporate Governance Committee of the Board (other than as a chairperson); |
| ● | an initial one-time equity grant of stock options with a fair value of $700,000 (valued based on the grant date fair value and subject to a limit of 60,000 stock options) under the 2023 Plan, subject to annual vesting over three years following the date of grant; |
| ● | an annual equity grant of stock options with a fair value of $350,000 (valued based on the grant date fair value and subject to a limit of 30,000 stock options) under the 2023 Plan, subject to vesting on the one year anniversary of the date of grant; and |
| ● | a director compensation limit of $1,000,000 during the year such director is appointed and $750,000 annually thereafter. |
Compensation Committee Interlocks and Insider Participation
None of the members of our Compensation Committee has at any time been one of our officers or employees since our inception. None of our executive officers currently serves, or in the past fiscal year has served, as a member of the board of directors or compensation committee of any entity that has one or more executive officers serving on our Board or Compensation Committee.
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters.
Security Ownership of Certain Beneficial Owners and Management
The following table presents information regarding beneficial ownership of our equity interests as of March 1, 2024 by:
| ● | each stockholder or group of stockholders known by us to be the beneficial owner of more than 5% of our common stock and non-voting common stock; |
183
| ● | each of our directors; |
| ● | each of our NEOs; and |
| ● | all of our current directors and executive officers as a group. |
Beneficial ownership is determined in accordance with the rules of the SEC, and thus represents voting or investment power with respect to our securities as of March 1, 2024. Under such rules, beneficial ownership includes any shares of common stock over which the individual or entity has sole or shared voting power or investment power as well as any shares of common stock that the individual or entity has the right to acquire within 60 days after March 1, 2024 through the exercise of any stock option, warrant or other right. To our knowledge and subject to applicable community property rules, and except as otherwise indicated below, the persons and entities named in the table have sole voting and sole investment power with respect to all shares beneficially owned.
The percentage ownership information shown in the column titled “Total Percentage Ownership” in the table below is based on 37,169,029 shares of our voting common stock outstanding, including 2,136,345 unvested shares of restricted common stock, and 13,486,642 non-voting common stock as of the date of this table (plus, as to any particular beneficial owner, any shares as to which such person has the right to acquire beneficial ownership within 60 days thereafter). The percentage ownership information shown in the column titled “Voting Power” in the table below is based on 35,032,684 shares of our voting common stock outstanding, and excludes 2,136,345 unvested shares of restricted common stock.
184
Unless otherwise indicated, the address of each beneficial owner listed in this table is the Company’s address set forth on the cover page of this Annual Report.
|
|
Number of |
|
Number of |
|
|
|
|
|
|
|
Shares of |
|
Shares of |
|
|
|
|
|
|
|
Voting |
|
Non-Voting |
|
|
|
|
|
|
|
Common |
|
Common |
|
Total |
|
|
|
|
|
Stock |
|
Stock |
|
Percentage |
|
Voting |
|
Name of Beneficial Owner |
|
Owned |
|
Owned |
|
Ownership(1) |
|
Power(2) |
|
Greater than 5% Stockholders: |
|
|
|
|
|
|
|
|
|
Entities affiliated with Fairmount Funds Management LLC** (3) |
|
2,048,647 |
** |
6,743,321 |
|
17.4 |
% |
5.8 |
% |
Entities affiliated with Venrock Healthcare Capital Partners III, L.P.** (4) |
|
1,750,000 |
** |
6,743,321 |
|
16.8 |
% |
5.0 |
% |
Entities affiliated with FMR LLC (Fidelity) (5) |
|
5,018,880 |
|
— |
|
9.9 |
% |
14.3 |
% |
Wellington Biomedical Innovation Master Investors (Cayman) II, L.P. (6) |
|
2,527,901 |
|
— |
|
5.0 |
% |
7.2 |
% |
Entities affiliated with Deep Track Capital, LP (7) |
|
2,323,456 |
|
— |
|
4.6 |
% |
6.6 |
% |
Paragon (8) |
|
2,259,073 |
|
— |
|
4.5 |
% |
6.4 |
% |
Entities affiliated with RTW Investments, LP (9) |
|
2,142,592 |
|
— |
|
4.2 |
% |
6.1 |
% |
Entities affiliated with RA Capital (10) |
|
1,977,901 |
|
— |
|
3.9 |
% |
5.6 |
% |
Perceptive Xontogeny Venture Fund II, LP (11) |
|
1,977,901 |
|
— |
|
3.9 |
% |
5.6 |
% |
Entities affiliated with AI Biotechnology (12) |
|
1,940,364 |
|
— |
|
3.8 |
% |
5.5 |
% |
Named Executive Officers and Directors: |
|
|
|
|
|
|
|
|
|
Michael Henderson, M.D. (13) |
|
705,011 |
|
— |
|
1.4 |
% |
2.0 |
% |
Carl Dambkowski, M.D. (14) |
|
123,123 |
|
— |
|
* |
|
* |
|
Jane Pritchett Henderson (15) |
|
74,948 |
|
— |
|
* |
|
* |
|
Mark C. McKenna (16) |
|
11,111 |
|
— |
|
* |
|
* |
|
Peter Harwin (3) |
|
2,099,813 |
|
6,743,321 |
|
17.5 |
% |
6.0 |
% |
Jennifer Fox |
|
— |
|
— |
|
* |
|
* |
|
Andrew Gottesdiener, M.D. |
|
— |
|
— |
|
* |
|
* |
|
William (BJ) Jones, Jr. |
|
— |
|
— |
|
* |
|
* |
|
Tomas Kiselak (3) |
|
2,099,813 |
|
6,743,321 |
|
17.5 |
% |
6.0 |
% |
Nimish Shah (4) |
|
1,750,000 |
|
6,743,321 |
|
16.8 |
% |
5.0 |
% |
All current executive officers and directors as a group (10 persons) (17) |
|
6,863,819 |
|
20,229,963 |
|
53.5 |
% |
19.6 |
% |
* |
Represents beneficial ownership of less than one percent. |
** |
Entities affiliated with Fairmount Funds Management LLC and entities affiliated with Venrock Healthcare Capital Partners III, L.P. each beneficially own the shares of common stock underlying their non-voting common stock, subject to an ownership limitation of 9.99% of outstanding common stock. Accordingly, such entities have the ability to convert their shares of non-voting common stock into common stock, and thereby increase their voting power, subject to such ownership limitation. |
(1) |
Calculated based on the sum of “Number of Shares of Voting Common Stock Owned” and “Number of Shares of Non-Voting Common Stock Owned,” divided by the sum of (1) the number of shares of voting common stock outstanding as of the date of this table, and (2) the number of shares of common stock that a person has the right to acquire within 60 days after the date of this table (which includes the number of shares of non-voting common stock owned by such person to the extent they can be converted to common stock within 60 days after the date of this table). |
(2) |
Calculated based on “Number of Shares of Voting Common Stock Owned” divided by the number of shares of voting common stock outstanding as of the date of this table, excluding unvested shares of restricted common stock. |
(3) |
Based on a Schedule 13D/A filed on January 31, 2024 and Company records. Consists of 59,913 shares of common stock and 221,426 shares of non-voting common stock held by Fairmount Healthcare Fund L.P. (“Fairmount Fund”) |
185
and 1,992,734 shares of common stock and 6,521,895 shares of non-voting common stock held by Fairmount Healthcare Fund II L.P. (“Fairmount Fund II”). Fairmount Funds Management LLC (“Fairmount”) is the investment manager for Fairmount Fund and Fairmount Fund II. Peter Harwin and Tomas Kiselak are the managing members of Fairmount. Fairmount, Peter Harwin and Tomas Kiselak may be deemed to have voting and investment power over the shares held by Fairmount Fund and Fairmount Fund II. Fairmount, Peter Harwin and Tomas Kiselak disclaim beneficial ownership of such shares, except to the extent of any pecuniary interest therein. The address for the entities listed is 200 Barr Harbor Drive, Suite 400, West Conshohocken, PA 19428.
(4) |
Based on a Schedule 13D filed on July 28, 2023 and Company records. Consists of 460,075 shares of common stock and 2,495,319 shares of non-voting common stock held by Venrock Healthcare Capital Partners III, L.P. (“VHCP III”); 46,025 shares of common stock and 249,522 shares of non-voting common stock held by VHCP Co-Investment Holdings III, LLC (“VHCP Co-III”); and 1,243,900 shares of common stock and 3,998,480 shares of non-voting common stock held by Venrock Healthcare Capital Partners EG, L.P. (“VHCP EG”). VHCP Management III, LLC (“VHCPM III”) is the sole general partner of VHCP III and the sole manager of VHCP Co-III. VHCP Management EG, LLC (“VHCPM EG”) is the sole general partner of VHCP EG. Dr. Bong Koh and Nimish Shah are the voting members of VHCPM III and VHCPM EG. Dr. Koh, Mr. Shah, VHCPM III and VHCPM EG disclaim beneficial ownership over all shares held by VHCP III, VHCP Co-III, and VHCP EG, except to the extent of their respective indirect pecuniary interests therein. The address for the entities listed is 3340 Hillview Avenue, Palo Alto, CA 94304. |
(5) |
Based on a Schedule 13G/A filed on February 9, 2024. The securities represented in the table above are owned by funds or accounts managed by direct or indirect subsidiaries of FMR LLC and are beneficially owned, or may be deemed to be beneficially owned, by FMR LLC. Abigail P. Johnson is a Director, the Chairman and the Chief Executive Officer of FMR LLC. Members of the Johnson family, including Abigail P. Johnson, are the predominant owners, directly or through trusts, of Series B voting common shares of FMR LLC, representing 49% of the voting power of FMR LLC. The Johnson family group and all other Series B shareholders have entered into a shareholders’ voting agreement under which all Series B voting common shares will be voted in accordance with the majority vote of Series B voting common shares. Accordingly, through their ownership of voting common shares and the execution of the shareholders’ voting agreement, members of the Johnson family may be deemed, under the Investment Company Act of 1940, to form a controlling group with respect to FMR LLC. The address of FMR LLC is 245 Summer Street, Boston, MA 02210. |
(6) |
Based on Company records. Consists of 2,527,901 shares of common stock held by Wellington Biomedical Innovation Master Investors (Cayman) II L.P. (“Wellington Biomedical Fund”). Wellington Management Company LLP, a registered investment adviser under the Investment Advisers Act of 1940, as amended, is the investment adviser to Wellington Biomedical Fund, and Wellington Alternative Investments LLC is its general partner. Wellington Management Investment, Inc. is the managing member of Wellington Alternative Investments LLC. Wellington Management Company LLP is an indirect subsidiary of Wellington Management Group LLP. Wellington Management Group LLP and Wellington Management Company LLP may be deemed beneficial owners with shared voting and investment power over the shares held by Wellington Biomedical Fund. Additional information about Wellington Management Company LLP is available in its Form ADV filed with the SEC. The address of all entities referenced in this footnote is 280 Congress Street, Boston, MA 02210. |
(7) |
Based on a Schedule 13G/A filed on February 14, 2024. Deep Track Biotechnology Master Fund, Ltd., Deep Track Capital, LP and David Kroin have shared voting and dispositive power over these securities. The address of Deep Track Capital, LP and David Kroin is 200 Greenwich Ave, 3rd Floor, Greenwich, Connecticut 06830. The address of Deep Track Biotechnology Master Fund, Ltd. is c/o Walkers Corporate Limited, 190 Elgin Ave, George Town, KY1-9001, Cayman Islands. |
(8) |
Based on Company records. Consists of 959,750 shares of common stock held by Paragon and 1,299,323 shares of common stock held by Paragee Holding. Paragee Holding is owned and controlled by Paragon. Paragon is managed by a board of directors. |
(9) |
Based on Company records. Consists of 2,142,592 shares held in the aggregate by RTW Innovation Master Fund, Ltd., RTW Master Fund, Ltd. and RTW Venture Fund Limited. RTW Investments, LP is the manager of RTW Master |
186
Fund, Ltd., RTW Venture Fund Limited and RTW Innovation Master Fund. Roderick Wong, M.D. is the Managing Partner and Chief Investment Officer of RTW Investments, LP and as such has sole voting and investment control over such shares. Dr. Wong disclaims beneficial ownership of such shares except to the extent of any pecuniary interest therein. The address of RTW Investments, LP and Dr. Wong is 40 10th Avenue, Floor 7, New York, New York, 10014.
(10) |
Based on a Schedule 13G filed on February 14, 2024. Includes 1,201,917 shares of common stock held by RA Capital Healthcare Fund, L.P. (“RA Healthcare”) and 775,984 shares of common stock held by RA Capital Nexus Fund III, L.P. (“Nexus III”). RA Capital Management, L.P. is the investment manager for RA Healthcare and Nexus III. The general partner of RA Capital Management, L.P. is RA Capital Management GP, LLC, of which Peter Kolchinsky, Ph.D. and Rajeev Shah are the managing members. RA Capital Management, L.P., RA Capital Management GP, LLC, Peter Kolchinsky, Ph.D. and Rajeev Shah may be deemed to have voting and investment power over the shares held of record by RA Healthcare and Nexus III. RA Capital Management, L.P., RA Capital Management GP, LLC, Peter Kolchinsky, Ph.D. and Rajeev Shah disclaim beneficial ownership of such shares, except to the extent of any pecuniary interest therein. The address of the entities listed above is 200 Berkeley Street, 18th Floor, Boston, Massachusetts 02116. |
(11) |
Based on Company records. The securities are directly held by Perceptive Xontogeny Venture Fund II, LP (“Perceptive Xontogeny”). Perceptive Venture Advisors, LLC (the “Venture Advisor”) serves as the investment advisor to Perceptive Xontogeny and is an affiliate of the Advisor. Joseph Edelman is the managing member of the Advisor. The Venture Advisor, the Advisor and Mr. Edelman disclaim, for purposes of Section 16 of the Exchange Act, beneficial ownership of such securities, except to the extent of his or its indirect pecuniary interest therein, and this report shall not be deemed an admission that they are the beneficial owner of such securities for purposes of Section 16 or for any other purposes. The address of the principal business office of each of foregoing persons is c/o 51 Astor Place, 10th Floor, New York, NY 10003. |
(12) |
Based on a Schedule 13G filed on November 3, 2023 . 1,940,364 shares of common stock are owned directly by AI Biotechnology LLC (AI Biotechnology) and may be deemed to be beneficially owned by Access Industries Holdings LLC (AIH), Access Industries Management, LLC (AIM) and Len Blavatnik because (i) Mr. Blavatnik controls AIM and holds a majority of the outstanding voting interests in AIH, (ii) AIM controls AIH, and (iii) AIH directly controls all of the outstanding voting interests in AI Biotechnology. Each of the Reporting Persons (other than AI Biotechnology) and each of their affiliated entities and the officers, partners, members and managers thereof, disclaims beneficial ownership of these securities. The address of the entites listed above is c/o Access Industries, Inc., 40 West 57th Street, 28th Floor, New York, NY 10019. |
(13) |
Includes 62,062 of restricted voting common stock that Dr. Henderson has the right to acquire within 60 days after the date of this table and 33,209 shares of common stock underlying options that have vested or will vest within 60 days after the date of this table. |
(14) |
Includes 12,532 shares of restricted voting common stock that Dr. Dambkowski has the right to acquire within 60 days after the date of this table and 14,612 shares of common stock underlying options that have vested or will vest within 60 days after the date of this table. |
(15) |
Includes 4,310 shares of restricted voting common stock that Ms. Henderson has the right to acquire within 60 days after the date of this table and 14,612 shares of common stock underlying options that have vested or will vest within 60 days after the date of this table. |
(16) |
Includes 11,111 shares of common stock underlying options that have vested or will vest within 60 days after the date of this table. |
(17) |
Includes 78,904 shares of restricted voting common stock that the directors and executive officers have the right to acquire within 60 days after the date of this table and 73,544 shares of common stock underlying options that have vested or will vest within 60 days after the date of this table. |
187
Securities Authorized for Issuance Under Equity Compensation Plans
The following table provides information as of December 31, 2023 with respect to the shares of our common stock that may be issued under our existing equity compensation plans.
|
|
|
|
|
|
|
Number of |
|
|
|
|
|
|
|
Securities |
|
|
|
|
|
|
|
Remaining |
|
|
|
|
|
|
|
Available for |
|
|
Number of |
|
Weighted |
|
Future Issuance |
|
|
|
Securities to |
|
Average |
|
Under |
|
|
|
be Issued Upon |
|
Exercise Price |
|
Equity |
|
|
|
Exercise |
|
of |
|
Compensation |
|
|
|
of Outstanding |
|
Outstanding |
|
Plans (Excluding |
|
|
|
Options, |
|
Options, |
|
Securities Reflected |
|
|
|
Warrants and |
|
Warrants and |
|
in |
|
Plan Category |
|
Rights |
|
Rights(1) |
|
the First Column) |
|
Equity compensation plans approved by stockholders(2) |
|
2,650,107 |
|
$ |
21.49 |
|
4,534,933 |
|
|
|
|
|
|
|
|
Total |
|
2,650,107 |
|
$ |
21.49 |
|
4,534,933 |
(1) |
The weighted-average exercise price does not take into account shares issuable upon vesting of any outstanding restricted stock units, which have no exercise price. |
(2) |
Includes the following plans: our 2023 Plan and our ESPP, including 479,003 shares subject to purchase thereunder during the purchase periods in effect as of December 31, 2023. Excludes 2,416,938 and 483,387 shares that were added to our 2023 Plan and our ESPP, respectively, on January 1, 2024 pursuant to the evergreen provisions thereunder that provide for automatic annual increases on January 1 of each year during the term of the respective plan equal to 5% of our outstanding shares as of the preceding December 31 (or such lesser amount as approved by the Compensation Committee), in the case of the 2023 Plan, or 1% of our outstanding shares as of the preceding December 31 (or such lesser amount as approved by the Compensation Committee), in the case of the ESPP. |
Item 13. Certain Relationships and Related Transactions, and Director Independence.
Certain Relationships and Transactions
The following is a summary of each transaction or series of similar transactions since February 4, 2022 (inception) or any currently proposed transaction, to which we were or are a party in which:
| ● | the amount involved exceeds $120,000; and |
| ● | any related person (including our directors, executive officers, beneficial owners of more than 5% of our voting capital stock and any affiliates or members of their immediate family) had or will have a direct or indirect material interest, other than compensation and other arrangements that are described under the sections titled “Executive Compensation” and “Director Compensation” or that were approved by our Compensation Committee. |
Beneficial ownership of securities is determined in accordance with the rules of the SEC.
188
Preferred Unit Financings
Series A Preferred Unit Financing
In February 2022, August 2022 and October 2022, we completed a preferred unit financing and issued and sold an aggregate of 20,000,000 Series A preferred units at a purchase price of $1.00 per unit. We issued and sold the Series A preferred units pursuant to a unit purchase agreement entered into with certain investors, for an aggregate purchase price of approximately $20.0 million. The following table summarizes purchases of our Series A preferred units by related persons:
|
|
|
|
CASH |
|
|
|
SERIES A |
|
PURCHASE |
|
PARTICIPANT |
|
PREFERRED UNITS |
|
PRICE |
|
Entities affiliated with Fairmount |
|
10,000,000 |
|
$ |
10,000,000 |
Entities affiliated with Venrock |
|
10,000,000 |
|
$ |
10,000,000 |
Series B Preferred Unit Financing
In November 2022, we completed a preferred unit financing and issued and sold an aggregate of 45,089,212 Series B preferred units at a purchase price of $3.30456 per unit. We issued and sold the Series B preferred units pursuant to a unit purchase agreement entered into with certain investors, for an aggregate purchase price of approximately $149.0 million. The following table summarizes purchases of our Series B preferred units by related persons:
|
|
|
|
CASH |
|
|
|
SERIES B |
|
PURCHASE |
|
PARTICIPANT |
|
PREFERRED UNITS |
|
PRICE |
|
Entities affiliated with Fairmount |
|
7,565,304 |
|
$ |
25,000,000.99 |
Entities affiliated with Venrock |
|
7,565,304 |
|
$ |
25,000,000.99 |
Insider Participation in Initial Public Offering
On July 18, 2023, we completed our IPO of our common stock. In our IPO, we issued and sold 20,297,500 shares of our common stock, including the full exercise of the underwriters’ option to purchase up to 2,647,500 additional shares, at a price to the public of $17.00 per share. The following table summarizes purchases of our shares in our IPO by related persons:
|
|
|
|
CASH |
|
|
|
COMMON |
|
PURCHASE |
|
PARTICIPANT |
|
STOCK |
|
PRICE |
|
Entities affiliated with Fairmount |
|
2,941,176 |
|
$ |
49,999,992 |
Entities affiliated with Venrock |
|
1,750,000 |
|
$ |
29,750,000 |
Our Relationship with Paragon
We are party to a number of agreements with Paragon. Paragon beneficially owns more than 5% of our capital stock through its holdings of incentive units and common units. Fairmount Funds Management LLC beneficially owns more than 5% of our capital stock, has two seats on our Board and beneficially owns more than 5% of Paragon, which is a joint venture between Fairmount Funds Management LLC and Fair Journey Biologics. Fairmount Funds Management LLC has appointed the sole director on Paragon’s board of directors and has the contractual right to approve the appointment of any executive officers.
In February 2022, we entered into the 2022 Option Agreement with Paragon. In consideration for the exclusive options granted under the 2022 Option Agreement, we paid an upfront cash amount of $1.3 million and issued 1,250,000 common units to Paragon. Paragon was also entitled to up to an additional 3,750,000 common units in exchange for the rights granted under the 2022 Option Agreement, of which 1,250,000 were issued in connection with the additional closing of the Series A Preferred Unit financing in August 2022 and 2,500,000 were issued in connection with the additional closings of the Series A Preferred Unit financing in October 2022.
189
On a Research Program-by-Research Program basis following the finalization of the Research Plan for each respective Research Program, we are required to pay Paragon a nonrefundable fee in cash of $0.5 million under the 2022 Option Agreement. We are also obligated to compensate Paragon on a quarterly basis for its services performed under each Research Program based on the actual costs incurred.
In November 2023, we entered into the 2023 Option Agreement with Paragon. On a Research Program-by-Research Program basis following the finalization of the Research Plan for each respective Research Program, we are required to pay Paragon a nonrefundable fee in cash of $2.0 million under the 2023 Option Agreement. We are also obligated to compensate Paragon on a quarterly basis for its services performed under each Research Program based on the actual costs incurred. For the period from February 4, 2022 (inception) to December 31, 2022 and for the twelve months ended December 31, 2023, we recognized $22.3 million and $15.9 million, respectively, of expense in connection with the services provided by Paragon under the Option Agreements, including the nonrefundable fee following the finalization of the IL-13 Research Plan. In addition, in December 2022, we granted Paragon 1,625,086 incentive units as consideration under the Option Agreement.
In November 2022, we exercised our option available under the Option Agreement with respect to the IL-13 Research Program and entered into the IL-13 License Agreement. In April 2023, we exercised our option available under the Option Agreement with respect to the IL-4Rα Research Program and the OX40L Research Program and entered into the IL-4Rα License Agreement and OX40L License Agreement. In connection with each such exercise, we paid Paragon a nonrefundable fee in cash of $0.5 million per Research Program. We are also obligated to pay Paragon up to $3.0 million upon the achievement of specific development and clinical milestones for the first product under each of the IL-13 License Agreement, IL-4Rα License Agreement and OX40L License Agreement that achieves such specified milestones. Upon execution of the IL-13 License Agreement, we paid Paragon a $1.0 million fee for nomination of a development candidate. In August 2023, we announced the dosing of our first participant in the Phase 1 trial of APG777 and incurred a milestone payment of $2.0 million to Paragon in the third quarter of 2023. In November 2023, the Company finalized the nomination of a development candidate under the IL-4Rα License Agreement and made a milestone payment of $1.0 million to Paragon in the fourth quarter of 2023.We have not made any payments under the OX40L License Agreement. The Option Agreement, the IL-13 License Agreement, the IL-4Rα License Agreement and the OX40L License Agreement were negotiated on an arm’s-length basis and are market rate transactions on terms that we believe are no less favorable than would have been reached with an unrelated third party. For additional detail regarding our arrangements with Paragon, see Part I, Item 1,“Business — Our Collaboration, License and Services Agreements.”
Indemnification Agreements
In connection with our IPO, we entered into agreements to indemnify our directors and executive officers. These agreements, among other things, require us to indemnify these individuals for certain expenses (including attorneys’ fees), judgments, fines and settlement amounts reasonably incurred by such person in any action or proceeding, including any action by or in our right, on account of any services undertaken by such person on behalf of our company or that person’s status as a director or officer, as applicable, to the maximum extent allowed under Delaware law.
Option Grants to Executive Officers
We have granted options to our executive officers as more fully described in the section titled “Executive Compensation.”
Reorganization
In connection with our IPO, the members of Apogee Therapeutics, LLC contributed their units in Apogee Therapeutics, LLC to Apogee Therapeutics, Inc. in exchange for shares of common stock and/or non-voting common stock of Apogee Therapeutics, Inc, as applicable.
190
Registration Rights Agreement
We have entered into a registration rights agreement with the holders of 24,987,750 shares of our common stock (including shares of common stock issuable upon conversion of our non-voting common stock). The registration of shares of our common stock pursuant to the exercise of registration rights described below would enable holders to sell these shares without restriction under the Securities Act when the registration statement is declared effective. We will pay all expenses related to any demand, piggyback or Form S-3 registration described below, with the exception of underwriting discounts, selling commissions, and stock transfer taxes.
The registration rights described below will expire upon the earliest to occur of: (i) three years after the completion of our IPO; (ii) the closing of a merger or consolidation in which (A) we are constituent party or (B) a subsidiary of ours is a constituent party and we issue shares of our capital stock pursuant to such merger or consolidation; or (iii), with respect to any particular holder, at such time that such holder can sell its shares, under Rule 144 or another similar exemption under the Securities Act, during any three-month period without registration.
Form S-1 Demand Registration Rights
The holders of registrable securities who are party to the registration rights agreement (the “Registration Rights Holders”) are entitled to certain demand registration rights. At any time after January 9, 2024, Registration Rights Holders who hold a majority of the registrable securities then outstanding may request that we file a Form S-1 registration statement for which the anticipated aggregate offering price would exceed $20,000,000.
Form S-3 Demand Registration Rights
At any time after we are qualified to file a registration statement on Form S-3, and subject to limitations and conditions, Registration Rights Holders who hold at least 30% of the registrable securities then outstanding may make a written request that we prepare and file a registration statement on Form S-3 under the Securities Act covering their shares, so long as the aggregate price to the public, net of the underwriters’ discounts and commissions, is at least $5,000,000. We will prepare and file the Form S-3 registration statement as requested, unless, in the good faith judgment of our Board, such registration would be materially detrimental to the Company and its stockholders and filing should be deferred. We may defer only once in any 12-month period, and such deferral shall not exceed 90 days after receipt of the request. In addition, we are not obligated to prepare or file any of these registration statements (i) during the period that is 30 or 60 days, as the case may be, before our good faith estimate of the date of filing of, and ending on a date that is 180 days after the effective date of, a Company-initiated registration or (ii) if two of these registrations have been completed within any 12-month period.
Piggyback Registration Rights
Subject to certain specified exceptions, if we propose to register any of our securities under the Securities Act either for our own account or for the account of other stockholders, the Registration Rights Holders are entitled to notice and certain “piggyback” registration rights allowing them to include their shares in our registration statement. These registration rights are subject to specified conditions and limitations, including the right of the underwriters, in their sole discretion, to limit the number of shares included in any such offering under certain circumstances, but not below 30% of the total amount of securities included in such offering.
Related Party Transaction Policy
Our Board has a written policy regarding the review and approval or ratification by our Audit Committee of related person transactions. For purposes of our policy only, a related person transaction is a transaction, arrangement or relationship or any series of similar transactions, arrangements or relationships between us or any of our subsidiaries and any related person in which the aggregate amount involved since the beginning of our last completed fiscal year exceeds or is expected to exceed $120,000 and such related person has or will have a direct or indirect interest. A related person is defined to include any executive officers, directors or director nominees or beneficial owner of more than 5% of our common stock and any immediate family member of any of the foregoing persons.
191
In determining to approve or ratify any such transaction, our Audit Committee is expected to take into account, among other factors it deems appropriate, whether the transaction is on terms no less favorable than terms generally available to an unaffiliated third-party under the same or similar circumstances and the extent of the related person’s interest in the transaction. Transactions involving compensation for services provided to us as an employee or director, among other limited exceptions, are deemed under the terms of the policy to have standing pre-approval by the Audit Committee but may be specifically reviewed if appropriate in light of the facts and circumstances. Any director who is a related person with respect to a transaction under review is not permitted to participate in the deliberations (other than to provide information concerning the transaction to the Audit Committee) or vote on approval of the transaction.
The Series A Preferred Unit financing and the Series B Preferred Unit financing described above were consummated prior to our adoption of the formal, written policy described above, and, accordingly, the foregoing policies and procedures were not followed with respect to these transactions.
Director Independence
Nasdaq listing rules require a majority of a listed company’s board of directors to be comprised of independent directors who, in the opinion of the board of directors, do not have a relationship that would interfere with the exercise of independent judgment in carrying out the responsibilities of a director. Subject to specified exceptions, each member of a listed company’s audit, compensation and nominating committees must be independent, and audit and compensation committee members must satisfy additional independence criteria under the Exchange Act.
Our Board undertook a review of its composition and the independence of each director. Based upon information requested from and provided by each director concerning his or her background, employment and affiliations, our Board has determined that Andrew Gottesdiener, M.D., Jennifer Fox, Peter Harwin, William (BJ) Jones, Jr., Tomas Kiselak, Mark C. McKenna and Nimish Shah qualify as “independent directors” as defined by the Nasdaq listing rules. Michael Henderson, M.D., is not an independent director because he is our CEO. In making such determinations, our Board considered the relationships that each such non-employee director has with our Company and all other facts and circumstances our Board deemed relevant in determining independence, including the beneficial ownership of our capital stock by each non-employee director and any business, consulting or employment relationships with our significant investors. Our Board also determined that each of the directors currently serving on the Audit Committee and the Compensation Committee satisfy the additional independence criteria applicable to directors on such committees under Nasdaq listing rules and the rules and regulations established by the SEC.
Item 14. Principal Accountant Fees and Services.
Ernst & Young LLP (“EY”) has served as our independent auditor since 2023. The following table summarizes the audit fees billed and expected to be billed by EY for the indicated fiscal years and the fees billed by EY for all other services rendered during the indicated fiscal years.
|
|
Year Ended December 31, |
||||
|
|
2023 |
|
2022 |
||
Audit Fees (1) |
|
$ |
1,828,500 |
|
$ |
150,000 |
Audit-Related Fees (2) |
|
|
— |
|
|
— |
Tax Fees (3) |
|
|
— |
|
|
— |
All Other Fees (4) |
|
|
— |
|
|
— |
Total Fees |
|
$ |
1,828,500 |
|
|
150,000 |
(1) |
Consists of aggregate fees for professional services provided in connection with the annual audit of our consolidated financial statements, the review of our quarterly condensed consolidated financial statements and comfort letters, consents and review of documents filed with the SEC. Fees for fiscal year 2023 include services provided for the registration statement for our initial public offering. |
(2) |
Consists of fees for assurance and related services associated with consultations on matters directly related to the audit. |
192
(3) |
Consists of fees for tax compliance, advice and tax services. |
(4) |
Consists of fees for all other services. |
Pre-Approval Policies and Procedures
Our Audit Committee has adopted procedures requiring the pre-approval of all audit and non-audit services performed by our independent auditor in order to assure that these services do not impair the auditor’s independence. These procedures generally approve the performance of specific services subject to a cost limit for all such services. This general approval is reviewed, and if necessary modified, at least annually. Management must obtain the specific prior approval of the committee for each engagement of our auditor to perform other audit-related or non-audit services. The committee does not delegate its responsibility to pre-approve services performed by our auditor to any member of management. The committee has delegated authority to the committee chair to pre-approve audit and non-audit services to be provided to us by our auditor provided that the fees for such services do not exceed $200,000. Any pre-approval of services by the committee chair pursuant to this delegated authority must be reported to the committee at its next regularly scheduled meeting.
193
PART IV
Item 15. Exhibits
| 1. | Financial Statements: For a list of the financial statements included herein, see the Index to the Financial Statements on page 129 of this Annual Report, which is incorporated into this Item by reference. |
| 2. | Financial Statement Schedules: Financial statement schedules have been omitted because they are either not required or not applicable or the information is included in the consolidated financial statements or the notes thereto. |
Exhibit |
|
Description of Exhibit |
2.1 |
|
|
|
|
|
3.1 |
|
|
|
|
|
3.2 |
|
|
|
|
|
4.1 |
|
|
|
|
|
4.2 |
|
|
|
|
|
4.3* |
|
|
|
|
|
10.1+ |
|
|
|
|
|
10.2+ |
|
|
|
|
|
10.3+ |
|
|
|
|
|
10.4+ |
|
|
|
|
|
10.5+ |
|
|
|
|
|
10.6* |
|
Equity Incentive Plan Form of Restricted Unit Award Grant Notice |
|
|
|
10.7+ |
|
|
|
|
|
194
10.8# |
|
|
|
|
|
10.9 |
|
|
|
|
|
10.10# |
|
|
|
|
|
10.11 |
|
|
|
|
|
10.12 |
|
|
|
|
|
10.13# |
|
|
|
|
|
10.14# |
|
|
|
|
|
10.15 |
|
|
|
|
|
10.16# |
|
|
|
|
|
10.17# |
|
|
|
|
|
23.1* |
|
|
|
|
|
31.1* |
|
|
|
|
|
31.2* |
|
|
|
|
|
32.1*(1) |
|
|
|
|
|
97.1* |
|
|
|
|
|
101.INS* |
|
Inline XBRL Instance Document |
|
|
|
101.SCH* |
|
Inline XBRL Taxonomy Extension Schema Document |
|
|
|
195
101.CAL* |
|
Inline XBRL Taxonomy Extension Calculation LinkbaseDocument |
|
|
|
101.DEF* |
|
Inline XBRL Taxonomy Extension Definition |
|
|
|
101.LAB* |
|
Inline XBRL Taxonomy Extension Label Linkbase Document |
|
|
|
101.PRE* |
|
Inline XBRL Taxonomy Extension Presentation Linkbase Document |
|
|
|
104* |
|
The cover page for this report, formatted in Inline XBRL (included in Exhibit 101) |
* |
Filed herewith |
+ |
Indicates management contract or compensatory plan. |
# |
Portions of the exhibit have been omitted for confidentiality purposes. |
| (1) | Furnished herewith and not to be deemed “filed” for purposes of Section 18 of the Securities Exchange Act of 1934, as amended (the Exchange Act) or otherwise subject to the liability of such section, and not to be deemed incorporated by reference into any filing under the Securities Act of 1933, as amended, or the Exchange Act. |
Item 16. Form 10-K Summary.
None.
196
SIGNATURES
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned thereunto duly authorized.
|
|
Apogee Therapeutics, Inc. |
|
|
|
Date: March 5, 2024 |
|
|
|
By: |
/s/ Michael Henderson, M.D. |
|
|
Michael Henderson, M.D. |
|
|
Director and Chief Executive Officer |
|
|
(principal executive officer) |
|
|
|
Date: March 5, 2024 |
|
|
|
By: |
/s/ Jane Pritchett Henderson |
|
|
Jane Pritchett Henderson |
|
|
Chief Financial Officer |
|
|
(principal financial and accounting officer) |
197
SIGNATURES
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned thereunto duly authorized.
Signature |
|
Title |
|
Date |
|
|
|
|
|
/s/ Michael Henderson, M.D. |
|
Director and Chief Executive Officer |
|
March 5, 2024 |
Michael Henderson, M.D. |
|
(principal executive officer) |
|
|
|
|
|
|
|
/s/ Jane Pritchett Henderson |
|
Chief Financial Officer |
|
March 5, 2024 |
Jane Pritchett Henderson |
|
(principal financial and accounting officer) |
|
|
|
|
|
|
|
/s/ Mark C. McKenna |
|
|
|
|
Mark C. McKenna |
|
Chair and Director |
|
March 5, 2024 |
|
|
|
|
|
/s/ Peter Harwin |
|
|
|
|
Peter Harwin |
|
Director |
|
March 5, 2024 |
|
|
|
|
|
/s/ Jennifer Fox |
|
|
|
|
Jennifer Fox |
|
Director |
|
March 5, 2024 |
|
|
|
|
|
/s/ Andrew Gottesdiener, M.D. |
|
|
|
|
Andrew Gottesdiener, M.D. |
|
Director |
|
March 5, 2024 |
|
|
|
|
|
/s/ Tomas Kiselak |
|
|
|
|
Tomas Kiselak |
|
Director |
|
March 5, 2024 |
|
|
|
|
|
/s/ William Jones, Jr. |
|
|
|
|
William Jones, Jr. |
|
Director |
|
March 5, 2024 |
|
|
|
|
|
/s/ Nimish Shah |
|
|
|
|
Nimish Shah |
|
Director |
|
March 5, 2024 |
198
Exhibit 4.3
DESCRIPTION OF REGISTRANT’S SECURITIES REGISTERED PURSUANT TO
SECTION 12 OF THE SECURITIES EXCHANGE ACT OF 1934
General
The following is a summary of the material terms of the capital stock of Apogee Therapeutics, Inc. (“we,” “us,” “our” or the “Company”) as well as other material terms of our amended and restated certificate of incorporation and amended and restated bylaws and certain provisions of Delaware law. This summary does not purport to be complete and is qualified in its entirety by the provisions of our amended and restated certificate of incorporation and amended and restated bylaws, copies of which are filed as exhibits to our Annual Report on Form 10-K, to which this exhibit is also appended.
Our authorized capital stock consists of 386,513,358 shares of voting common stock, $0.00001 par value per share, 13,486,642 shares of non-voting common stock, $0.00001 par value per share, and 10,000,000 shares of “blank check” preferred stock, $0.00001 par value per share. Unless otherwise noted, all references to our “common stock” herein refers to our voting common stock.
Common Stock and Non-Voting Common Stock
Our amended and restated certificate of incorporation authorizes the issuance of up to 386,513,358 shares of our common stock and 13,486,642 of our non-voting common stock. All outstanding shares of our common stock and non-voting common stock are validly issued, fully paid and nonassessable.
The holders of our common stock and our non-voting common stock have identical rights, provided that, (i) except as otherwise expressly provided in our amended and restated certificate of incorporation or as required by applicable law, on any matter that is submitted to a vote by our stockholders, holders of our common stock are entitled to one vote per share of common stock, and holders of our non-voting common stock are not entitled to any votes per share of non-voting common stock, including for the election of directors, and (ii) holders of our common stock have no conversion rights, while holders of our non-voting common stock shall have the right to convert each share of our non-voting common stock into one share of common stock at such holder’s election, provided that as a result of such conversion, such holder, together with its affiliates and any members of a Schedule 13(d) group with such holder, would not beneficially own in excess of 9.99% of our common stock immediately prior to and following such conversion (the “Beneficial Ownership Limitation”), unless otherwise as expressly provided for in our amended and restated certificate of incorporation. However, the Beneficial Ownership Limitation may be increased or decreased to any other percentage (not to exceed 19.99%) designated by such holder of non-voting common stock upon 61 days’ notice to us.
Voting Rights. Our common stock is entitled to one vote per share on any matter that is submitted to a vote of our stockholders, except on matters relating solely to terms of preferred stock, and our non-voting common stock is not entitled to any votes per share. However, as long as any shares of non-voting common stock are outstanding, we will not, without the affirmative vote of the holders of a majority of the then outstanding shares of non-voting common stock, (i) alter or change adversely the powers, preferences or rights given to the non-voting common stock, alter, amend or repeal any provision of, or add any provision to, our amended and restated certificate of incorporation or our amended and restated bylaws, or file any articles of amendment, certificate of designations, preferences, limitations and relative rights of any series of Preferred Stock, if such action would adversely alter or change the preferences, rights, privileges or powers of, or restrictions provided for the benefit of the non-voting common stock, regardless of whether any of the foregoing actions shall be by means of amendment to our amended and restated certificate of incorporation or by merger, consolidation or otherwise, (ii) issue further shares of non-voting common stock or increase or decrease the number of authorized shares of non-voting common stock, (iii) prior to the Stockholder Approval (as defined in our amended and restated certificate of incorporation) or at any time while at least 6,061,821 shares of non-voting common stock remain issued and outstanding, consummate either: (A) any Fundamental Transaction (as defined in our amended and restated certificate of incorporation) or (B) any merger or consolidation of the Company with or into another entity or any stock sale to, or other business combination in which the stockholders of the Company immediately before such transaction do not hold at least a majority of the capital stock of the Company immediately after such transaction or (iv) enter into any agreement with respect to any of the foregoing.
1
Except as otherwise expressly provided in our amended and restated certificate of incorporation or required by applicable law, all shares of common stock and non-voting common stock have the same rights and privileges and rank equally, share ratably, and are identical in all respects for all matters, including those described below. Our amended and restated certificate of incorporation does not provide for cumulative voting in the election of directors.
Dividends. Subject to preferences that may apply to any shares of preferred stock outstanding at the time, the holders of our common stock and non-voting common stock are entitled to receive ratably any dividends declared by the Board of Directors of the Company (the “Board”) out of funds legally available therefor if our Board, in its discretion, determines to issue dividends and then only at the times and in the amounts that our Board may determine to issue dividends and then only at the times and in the amounts that our Board may determine.
Liquidation Rights. In the event of our liquidation, dissolution or winding-up, the holders of our common stock and non-voting common stock will be entitled to share equally, identically, and ratably in all assets remaining after payment of or provision for any liabilities, liquidation preferences and accrued or declared but unpaid dividends, if any, with respect to any outstanding preferred stock, unless a different treatment is approved by the affirmative vote of the holders of a majority of the outstanding shares of such affected class, voting separately as a class.
Other Rights. The holders of our common stock and non-voting common stock have no preemptive rights. There are no redemption or sinking fund provisions applicable to our common stock and non-voting common stock.
Preferred Stock
Under the terms of our amended and restated certificate of incorporation, our Board has the authority, without further action by our stockholders, to issue up to 10,000,000 shares of preferred stock in one or more series, to establish from time to time the number of shares to be included in each such series, to fix the designations, powers, preferences, and relative, participating, optional or other rights, if any, and the qualifications, limitations or restrictions, if any, of the shares of each such series.
Our Board may authorize the issuance of preferred stock with voting or conversion rights that could adversely affect the voting power or other rights of the holders of our common stock and non-voting common stock. The issuance of preferred stock, while providing flexibility in connection with possible acquisitions and other corporate purposes, could, among other things, have the effect of delaying, deferring or preventing a change in our control and may adversely affect the market price of our common stock and non-voting common stock and the voting and other rights of the holders of our common stock and non-voting common stock. We have no current plans to issue any shares of preferred stock.
Registration Rights
We have entered into a registration rights agreement with the holders of 24,987,750 shares of our common stock (including shares of common stock issuable upon conversion of our non-voting common stock). The registration of shares of our common stock pursuant to the exercise of registration rights described below would enable holders to sell these shares without restriction under the Securities Act of 1933, as amended (the “Securities Act”), when the registration statement is declared effective. We will pay all expenses related to any demand, piggyback or Form S-3 registration described below, with the exception of underwriting discounts, selling commissions, and stock transfer taxes.
The registration rights described below will expire upon the earliest to occur of: (i) July 18, 2026; (ii) the closing of a merger or consolidation in which (A) we are constituent party or (B) a subsidiary of ours is a constituent party and we issue shares of our capital stock pursuant to such merger or consolidation; or (iii) with respect to any particular holder, at such time that such holder can sell its shares, under Rule 144 or another similar exemption under the Securities Act, during any three-month period without registration.
2
Form S-1 Demand Registration Rights
The holders of registrable securities who are party to the registration rights agreement (the “Registration Rights Holders”) are entitled to certain demand registration rights. The Registration Rights Holders who hold a majority of the registrable securities then outstanding may request that we file a Form S-1 registration statement for which the anticipated aggregate offering price would exceed $20,000,000.
Form S-3 Demand Registration Rights
At any time after we are qualified to file a registration statement on Form S-3, and subject to limitations and conditions, Registration Rights Holders who hold at least 30% of the registrable securities then outstanding may make a written request that we prepare and file a registration statement on Form S-3 under the Securities Act covering their shares, so long as the aggregate price to the public, net of the underwriters’ discounts and commissions, is at least $5,000,000. We will prepare and file the Form S-3 registration statement as requested, unless, in the good faith judgment of our Board, such registration would be materially detrimental to the Company and its stockholders and filing should be deferred. We may defer only once in any 12-month period, and such deferral shall not exceed 90 days after receipt of the request. In addition, we are not obligated to prepare or file any of these registration statements (i) during the period that is 30 or 60 days, as the case may be, before our good faith estimate of the date of filing of, and ending on a date that is 180 days after the effective date of, a Company-initiated registration or (ii) if two of these registrations have been completed within any 12-month period.
Piggyback Registration Rights
Subject to certain specified exceptions, if we propose to register any of our securities under the Securities Act either for our own account or for the account of other stockholders, the Registration Rights Holders are entitled to notice and certain “piggyback” registration rights allowing them to include their shares in our registration statement. These registration rights are subject to specified conditions and limitations, including the right of the underwriters, in their sole discretion, to limit the number of shares included in any such offering under certain circumstances, but not below 30% of the total amount of securities included in such offering.
Anti-Takeover Effects of Our Amended and Restated Certificate of Incorporation, Amended and Restated Bylaws and Delaware Law
Our amended and restated certificate of incorporation and our amended and restated bylaws include a number of provisions that may have the effect of delaying, deferring or preventing another party from acquiring control of us and encouraging persons considering unsolicited tender offers or other unilateral takeover proposals to negotiate with our Board rather than pursue non-negotiated takeover attempts.
· |
Issuance of undesignated preferred stock: Under our amended and restated certificate of incorporation, our Board has the authority, without further action by the stockholders, to issue up to 10,000,000 shares of undesignated preferred stock with rights and preferences, including voting rights, designated from time to time by our Board. The existence of authorized but unissued shares of preferred stock enables our Board to make it more difficult to attempt to obtain control of us by means of a merger, tender offer, proxy contest or otherwise. |
· |
Classified board: Our amended and restated certificate of incorporation establishes a classified Board consisting of three classes of directors, with staggered three-year terms. Only one class of directors will be elected at each annual meeting of our stockholders to succeed the directors of the same class whose terms are then expiring, with the other classes continuing for the remainder of their respective three-year terms. This provision may have the effect of delaying a change in control of our Board. |
· |
Election and removal of directors and board vacancies: Our amended and restated bylaws provide that directors will be elected by a plurality vote. Our amended and restated certificate of incorporation and amended and restated bylaws also provide that our Board has the right to increase or decrease the size of the Board and to fill vacancies on the Board. Directors may be removed only for cause by the affirmative vote of at least 662∕3% of the voting power of the stock outstanding and entitled to vote thereon (which, for |
3
the avoidance of doubt, does not include non-voting common stock). Only our Board is authorized to fill vacant directorships. In addition, the number of directors constituting our Board may be set only by resolution adopted by a majority vote of the directors then in office. These provisions prevent stockholders from increasing the size of our Board and gaining control of our Board by filling the resulting vacancies with its own nominees.
· |
Requirements for advance notification of stockholder nominations and proposals: Our amended and restated bylaws establish advance notice procedures with respect to stockholder proposals and the nomination of candidates for election as directors that specify certain requirements as to the timing, form and content of a stockholder’s notice. Business that may be conducted at an annual meeting of stockholders are limited to those matters properly brought before the meeting. These provisions may make it more difficult for our stockholders to bring matters before our annual meeting of stockholders or to nominate directors at annual meetings of stockholders. |
· |
No written consent of stockholders: Our amended and restated certificate of incorporation provides that all stockholder actions be taken by a vote of the stockholders at an annual or special meeting, and that stockholders may not take any action by written consent in lieu of a meeting. This limit may lengthen the amount of time required to take stockholder actions and would prevent the removal of directors by our stockholders without holding a meeting of stockholders. |
· |
No stockholder ability to call special meetings: Our amended and restated certificate of incorporation and amended and restated bylaws provide that only our Board may be able to call special meetings of stockholders and only those matters set forth in the notice of the special meeting may be considered or acted upon at a special meeting of stockholders. |
· |
Amendments to certificate of incorporation and bylaws: Any amendment to our amended and restated certificate of incorporation is required to be approved by a majority of our Board as well as, if required by law or our amended and restated certificate of incorporation, a majority of the outstanding shares entitled to vote on the amendment and a majority of the outstanding shares of each class entitled to vote thereon as a class, except that the amendment of provisions to Board classification, stockholder action, certificate amendments and liability of directors and officers must be approved by not less than 66 2∕3% of the outstanding shares entitled to vote on the amendment, voting together as a single class. Any amendment to our amended and restated bylaws is required to be approved by either a majority of our Board or not less than 66 2∕3% of the outstanding shares entitled to vote on the amendment, voting together as a single class (which, for the avoidance of doubt, does not include non-voting common stock). |
These provisions are designed to enhance the likelihood of continued stability in the composition of our Board and its policies, to discourage certain types of transactions that may involve an actual or threatened acquisition of our company and to reduce our vulnerability to an unsolicited acquisition proposal. We also designed these provisions to discourage certain tactics that may be used in proxy fights. However, these provisions could have the effect of discouraging others from making tender offers for our shares and, as a consequence, they may also reduce fluctuations in the market price of our shares that could result from actual or rumored takeover attempts.
Delaware General Corporation Law Section 203
As a Delaware corporation, we are also subject to the anti-takeover provisions of Section 203 of the Delaware General Corporation Law (the “DGCL”), which prohibits a Delaware corporation from engaging in a business combination specified in the statute with an interested stockholder (as defined in the statute) for a period of three years after the date of the transaction in which the person first becomes an interested stockholder, unless the business combination is approved in advance by a majority of the independent directors or by the holders of at least two-thirds of the outstanding disinterested shares. The application of Section 203 of the DGCL could also have the effect of delaying or preventing a change of control of us.
Exclusive Forum Selection Clause
Our amended and restated certificate of incorporation provides that, unless we consent in writing to the selection of an alternative forum, the sole and exclusive forum to the fullest extent permitted by law for: (i) any derivative action or proceeding brought on our behalf; (ii) any action asserting a breach of fiduciary duty owed by any director, officer or other employee to us or our stockholders; (iii) any action asserting a claim against us or any director or officer or other employee arising pursuant to the DGCL; (iv) any action to interpret, apply, enforce or determine the validity of our amended and restated certificate of incorporation or amended and restated bylaws; or (v) any other action asserting a claim that is governed by the internal affairs doctrine, shall be the Court of Chancery of the State of Delaware (or another state court or the federal court located within the State of Delaware if the Court of Chancery does not have or declines to accept jurisdiction), in all cases subject to the court’s having jurisdiction over indispensable parties named as defendants.
4
Our amended and restated certificate of incorporation provides that the federal district courts of the United States will be the exclusive forum for resolving any complaint asserting a cause of action arising under the Securities Act but the forum selection provisions will not apply to claims brought to enforce a duty or liability created by the Securities Exchange Act of 1934, as amended. Although we believe these provisions benefit us by providing increased consistency in the application of Delaware law for the specified types of actions and proceedings, the provisions may have the effect of imposing additional costs on stockholders in pursuing any such claims or limiting a stockholder’s ability to bring a claim in a judicial forum that it finds favorable for disputes, which may discourage lawsuits against us or our directors or officers. It is possible that a court could find that such provisions are inapplicable for a particular claim or action or that such provisions are unenforceable. In addition, under the Securities Act, federal courts have concurrent jurisdiction over all suits brought to enforce any duty or liability created by the Securities Act, and investors cannot waive compliance with the federal securities laws and the rules and regulations thereunder.
Transfer Agent and Registrar
Equiniti Trust Company, LLC serves as the transfer agent and registrar for our common stock. The address of the transfer agent and registrar is 6201 15th Avenue, Brooklyn, NY 11219.
Listing
Our common stock is listed on The Nasdaq Global Market under the symbol “APGE.” Our non-voting common stock is not listed on any securities exchange.
5
Exhibit 10.6
EMPLOYEE FORM
APOGEE THERAPEUTICS, INC.
2023 EQUITY INCENTIVE PLAN
GRANT NOTICE FOR
RESTRICTED STOCK UNIT AWARD
FOR GOOD AND VALUABLE CONSIDERATION, Apogee Therapeutics, Inc., a Delaware corporation (the “Company”), hereby grants to the Participant named below the number of Restricted Stock Units (the “RSUs”) specified below (the “Award”) under the Apogee Therapeutics, Inc. 2023 Equity Incentive Plan (the “Plan”). Each RSU represents the right to receive one share of Common Stock, upon the terms and subject to the conditions set forth in this Grant Notice, the Plan and the Standard Terms and Conditions (the “Standard Terms and Conditions”) promulgated under such Plan and attached hereto as Exhibit A. This Award is granted pursuant to the Plan and is subject to and qualified in its entirety by the Standard Terms and Conditions. Capitalized terms not otherwise defined herein shall have the meanings set forth in the Plan.
Name of Participant: |
|
Grant Date: |
|
Number of RSUs: |
|
[Vesting Commencement Date:] |
|
Vesting Schedule: |
Subject to the Plan and the Standard Terms and Conditions, the RSUs shall vest in accordance with the following schedule, so long as the Participant remains continuously employed by the Company or its Subsidiaries from the Grant Date through each such vesting date: [25% of the RSUs shall vest on each of the first four anniversaries of the Vesting Commencement Date]1. |
1 |
Note to Apogee: Please revise the vesting schedule as you wish. |
By accepting this Grant Notice, the Participant acknowledges that the Participant has received and read, and agrees that this Award shall be subject to, the terms of this Grant Notice, the Plan, and the Standard Terms and Conditions.
|
APOGEE THERAPEUTICS, INC. |
|
|
|
|
|
By: |
|
|
Name: |
|
|
Title: |
|
|
|
|
|
PARTICIPANT |
|
|
|
|
|
|
|
|
[Name] |
|
SIGNATURE PAGE TO
GRANT NOTICE FOR
RESTRICTED STOCK UNIT AWARD
EXHIBIT A
APOGEE THERAPEUTICS, INC.
2023 EQUITY INCENTIVE PLAN
STANDARD TERMS AND CONDITIONS FOR
RESTRICTED STOCK UNITS
These Standard Terms and Conditions apply to the Restricted Stock Units granted pursuant to the Apogee Therapeutics, Inc. 2023 Equity Incentive Plan (the “Plan”), which are evidenced by a Grant Notice or an action of the Committee that specifically refers to these Standard Terms and Conditions. In addition to these Standard Terms and Conditions, the Restricted Stock Units shall be subject to the terms of the Plan, which are incorporated into these Standard Terms and Conditions by this reference. Capitalized terms not otherwise defined herein shall have the meanings set forth in the Plan.
1. |
TERMS OF RESTRICTED STOCK UNITS |
Apogee Therapeutics, Inc., a Delaware corporation (the “Company”), has granted to the Participant named in the Grant Notice provided to said Participant herewith (the “Grant Notice”) an award of Restricted Stock Units (the “Award” or “RSUs”) specified in the Grant Notice, with each Restricted Stock Unit representing the right to receive one share of Common Stock. The Award is subject to the conditions set forth in the Grant Notice, these Standard Terms and Conditions and the Plan. For purposes of these Standard Terms and Conditions and the Grant Notice, any reference to the Company shall include a reference to any Subsidiary.
2. |
VESTING AND SETTLEMENT OF RESTRICTED STOCK UNITS |
(a)The Award shall not be vested as of the Grant Date set forth in the Grant Notice and shall be forfeitable unless and until otherwise vested pursuant to the terms of the Grant Notice and these Standard Terms and Conditions. After the Grant Date, subject to termination or acceleration as provided in these Standard Terms and Conditions and the Plan, the Award shall become vested as described in the Grant Notice with respect to that number of Restricted Stock Units as set forth in the Grant Notice. Restricted Stock Units that have vested and are no longer subject to forfeiture are referred to herein as “Vested RSUs.” Restricted Stock Units awarded hereunder that are not vested and remain subject to forfeiture are referred to herein as “Unvested RSUs.”
(b)As soon as administratively practicable following the vesting of the RSUs pursuant to the Grant Notice and this Section 2, but in no event later than 30 days after each vesting date, the Company shall deliver to the Participant shares of Common Stock equal to the number of RSUs that became Vested RSUs on such date.
(c)If the Participant’s Termination of Employment is by the Company without Cause or as a result of a material reduction in the Participant’s duties, authority or responsibilities within 12 months following a Change in Control, subject to the Participant’s execution and nonrevocation of a general release of claims in a form provided by the Company, all then Unvested RSUs shall become Vested RSUs effective as of the date of such Termination of Employment.
EXHIBIT A
STANDARD TERMS AND CONDITIONS FOR
RESTRICTED STOCK UNITS
(d)If the Participant’s Termination of Employment is for any reason other than as set forth in Section 4(c), any then Unvested RSUs shall be forfeited and canceled effective as of the date of such Termination of Employment.
3. |
RIGHTS AS STOCKHOLDER; DIVIDEND EQUIVALENTS |
(a)The Participant shall not be, nor have any of the rights or privileges of, a stockholder of the Company in respect of any RSUs (including any voting rights or rights to dividends or distributions paid on shares of Common Stock, except as provided in Section 3(b)) unless and until shares of Common Stock settled for such RSUs shall have been issued by the Company to the Participant (as evidenced by the appropriate entry on the books of the Company or of a duly authorized transfer agent of the Company).
(b)Notwithstanding the foregoing, from and after the Grant Date and until the earlier of (i) the Participant’s receipt of Common Stock upon settlement of RSUs and (ii) the time when the Participant’s right to receive Common Stock upon settlement of RSUs is forfeited, on the date that the Company pays a cash dividend (if any) to holders of Common Stock generally, the Participant shall be entitled, as a Dividend Equivalent, to a number of additional whole RSUs determined by dividing (i) the product of (A) the dollar amount of such cash dividend paid per share of Common Stock and (B) the total number of outstanding RSUs (including dividend equivalents paid thereon) held by the Participant on the record date for such dividend, by (ii) the Fair Market Value per share of Common Stock on the date such dividend is paid to holders of Common Stock generally. Such Dividend Equivalents (if any) shall be subject to the same terms and conditions and shall be settled or forfeited in the same manner and at the same time as the RSUs to which the Dividend Equivalents were credited.
4. |
RESTRICTIONS ON RESALES OF SHARES |
The Company may impose such restrictions, conditions or limitations as it determines appropriate as to the timing and manner of any resales by the Participant or other subsequent transfers by the Participant of any shares of Common Stock issued pursuant to Vested RSUs, including (a) restrictions under an insider trading policy, (b) restrictions designed to delay and/or coordinate the timing and manner of sales by the Participant and other holders and (c) restrictions as to the use of a specified brokerage firm for such resales or other transfers.
5. |
INCOME TAXES |
(a)The Participant acknowledges that, regardless of any action taken by the Company or, if different, the member of the Subsidiary or Affiliate for which the Participant provides services (the “Service Recipient”), the ultimate liability for all income tax, social insurance contributions, payroll tax, fringe benefits tax, payment on account, and other tax-related items related to the Participant’s participation in the Plan and legally applicable to the Participant (“Tax-Related Items”) is and remains the Participant’s responsibility and may exceed the amount, if any, actually withheld by the Company or the Service Recipient.
A-2
The Participant further acknowledges that the Company and/or the Service Recipient (i) make no representations or undertakings regarding the treatment of any Tax-Related Items in connection with any aspect of the Award, including, but not limited to, the grant, vesting or settlement of the Award, the subsequent sale of shares acquired pursuant to such settlement and the receipt of any dividends, Dividend Equivalents or other distributions paid on the shares, and (ii) do not commit to and are under no obligation to structure the terms of the grant or any aspect of the Award to reduce or eliminate the Participant’s liability for Tax-Related Items or achieve any particular tax result. Further, if the Participant is subject to Tax-Related Items in more than one jurisdiction, the Participant acknowledges that the Company and/or the Service Recipient (or former service recipient, as applicable) may be required to withhold or account for Tax-Related Items in more than one jurisdiction.
(b)Prior to any relevant taxable or tax-withholding event, as applicable, the Participant agrees to make arrangements satisfactory to the Company and/or the Service Recipient to satisfy any withholding obligations the Company and/or the Service Recipient may have for Tax-Related Items. In this regard, the Participant authorizes the Company to satisfy any withholding obligation for Tax-Related Items by withholding from proceeds of the sale of shares of Common Stock to be issued upon settlement of the Vested RSUs through a mandatory sale arranged by the Company (on the Participant’s behalf pursuant to this authorization without further consent); provided, however, if the proceeds from such sale of shares of Common Stock are not sufficient to fully satisfy any withholding obligation for Tax-Related Items, the Participant authorizes the Company to satisfy such excess withholding obligation by withholding from the Participant’s wages or other cash compensation payable to the Participant by the Company or the Service Recipient.
(c)The Company and/or the Service Recipient may withhold or account for Tax-Related Items by considering statutory withholding rates or other withholding rates, including maximum rates applicable in the Participant’s jurisdiction(s), in which case the Participant may receive a refund of any over-withheld amount in cash and will have no entitlement to the equivalent amount in shares of Common Stock.
(d)The Participant agrees to pay to the Company or the Service Recipient any amount of Tax-Related Items that the Company or the Service Recipient may be required to withhold or account for as a result of the Participant’s participation in the Plan that cannot be satisfied by the means previously described. The Company may refuse to deliver the shares of Common Stock or the proceeds from the sale of shares of Common Stock, if the Participant fails to comply with the Participant’s obligations for Tax-Related Items.
6. |
NONTRANSFERABILITY OF AWARD |
Except as permitted by the Committee or as permitted under Section 17 of the Plan, the Award may not be sold, assigned, transferred, pledged or otherwise directly or indirectly encumbered or disposed of other than by will or the laws of descent and distribution.
7. |
OTHER AGREEMENTS SUPERSEDED |
The Grant Notice, these Standard Terms and Conditions and the Plan constitute the entire understanding between the Participant and the Company regarding the Award. Any prior agreements, commitments or negotiations concerning the Award are superseded.
A-3
8. |
LIMITATION OF INTEREST IN SHARES SUBJECT TO RESTRICTED STOCK UNITS |
Neither the Participant (individually or as a member of a group) nor any beneficiary or other person claiming under or through the Participant shall have any right, title, interest, or privilege in or to any shares of Common Stock allocated or reserved for the purpose of the Plan or subject to the Grant Notice or these Standard Terms and Conditions except as to such shares of Common Stock, if any, as shall have been issued to such person in connection with the Award. Nothing in the Plan, in the Grant Notice, these Standard Terms and Conditions or any other instrument executed pursuant to the Plan shall confer upon the Participant any right to continue in the Company’s employ or service nor limit in any way the Company’s right to terminate the Participant’s employment at any time for any reason.
9. |
NO LIABILITY OF COMPANY |
The Company and any Affiliate which is in existence or hereafter comes into existence shall not be liable to the Participant or any other person as to: (a) the nonissuance or sale of shares of Common Stock as to which the Company has been unable to obtain from any regulatory body having jurisdiction the authority deemed by the Company’s counsel to be necessary to the lawful issuance and sale of any shares hereunder; and (b) any tax consequence expected, but not realized, by the Participant or other person due to the receipt or settlement of the Award.
10. |
GENERAL |
(a)In the event that any provision of the Grant Notice or these Standard Terms and Conditions is declared to be illegal, invalid or otherwise unenforceable by a court of competent jurisdiction, such provision shall be reformed, if possible, to the extent necessary to render it legal, valid and enforceable, or otherwise deleted, and the remainder of the Grant Notice and these Standard Terms and Conditions shall not be affected except to the extent necessary to reform or delete such illegal, invalid or unenforceable provision.
(b)The headings preceding the text of the sections hereof are inserted solely for convenience of reference, and shall not constitute a part of the Grant Notice or these Standard Terms and Conditions, nor shall they affect its meaning, construction or effect. Words in the masculine gender shall include the feminine gender, and where appropriate, the plural shall include the singular and the singular shall include the plural. The use herein of the word “including” following any general statement, term or matter shall not be construed to limit such statement, term or matter to the specific items or matters set forth immediately following such word or to similar items or matters, whether or not non-limiting language (such as “without limitation”, “but not limited to”, or words of similar import) is used with reference thereto, but rather shall be deemed to refer to all other items or matters that could reasonably fall within the broadest possible scope of such general statement, term or matter. References herein to any agreement, instrument or other document means such agreement, instrument or other document as amended, supplemented and modified from time to time to the extent permitted by the provisions thereof and not prohibited by the Plan, the Grant Notice or these Standard Terms and Conditions. Unless the context requires otherwise, all references to laws and regulations refer to such laws and regulations as they may be amended from time to time, and references to particular provisions of laws or regulations include a reference to the corresponding provisions of any succeeding law or regulation.
A-4
(c)The Grant Notice and these Standard Terms and Conditions shall inure to the benefit of and be binding upon the parties hereto and their respective permitted heirs, beneficiaries, successors and assigns.
(d)The Grant Notice and these Standard Terms and Conditions shall be construed in accordance with and governed by the laws of the State of Delaware, without regard to principles of conflicts of law.
(e)In the event of any conflict between the Grant Notice, these Standard Terms and Conditions and the Plan, the Grant Notice and these Standard Terms and Conditions shall control. In the event of any conflict between the Grant Notice and these Standard Terms and Conditions, the Grant Notice shall control.
(f)All questions arising under the Plan, the Grant Notice or under these Standard Terms and Conditions shall be decided by the Committee in its total and absolute discretion.
11. |
CLAWBACK |
The Restricted Stock Units and any shares of Common Stock issued pursuant to Vested RSUs will be subject to recoupment in accordance with any clawback policy adopted by the Company. No recovery of compensation under such a clawback policy will be an event giving rise to a right to resign for “good reason” or “constructive termination” (or similar term) under any agreement with the Company. By accepting the Award, the Participant is agreeing to be bound by any such clawback policy, as in effect or as may be adopted and/or modified from time to time by the Company in its discretion.
12. |
ELECTRONIC DELIVERY |
By executing the Grant Notice, the Participant hereby consents to the delivery of information (including information required to be delivered to the Participant pursuant to applicable securities laws) regarding the Company and the Subsidiaries, the Plan, the Restricted Stock Units and the Common Stock via Company web site or other electronic delivery.
A-5
Exhibit 23.1
CONSENT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
We consent to the incorporation by reference in the Registration Statement (Form S-8 No. 333-274234) pertaining to the 2023 Equity Incentive Plan and the 2023 Employee Stock Purchase Plan of Apogee Therapeutics, Inc. of our report dated March 5, 2024, with respect to the consolidated financial statements of Apogee Therapeutics, Inc. included in this Annual Report (Form 10-K) for the year ended December 31, 2023.
/s/ Ernst & Young LLP
Boston, Massachusetts
March 5, 2024
Exhibit 31.1
CERTIFICATION PURSUANT TO
RULES 13a-14(a) AND 15d-14(a) UNDER THE SECURITIES EXCHANGE ACT OF 1934,
AS ADOPTED PURSUANT TO SECTION 302 OF THE SARBANES-OXLEY ACT OF 2002
I, Michael Henderson, M.D., certify that:
1. |
I have reviewed this Annual Report on Form 10-K of Apogee Therapeutics, Inc.; |
2. |
Based on my knowledge, this report does not contain any untrue statement of a material fact or omit to state a material fact necessary to make the statements made, in light of the circumstances under which such statements were made, not misleading with respect to the period covered by this report; |
3. |
Based on my knowledge, the financial statements, and other financial information included in this report, fairly present in all material respects the financial condition, results of operations and cash flows of the registrant as of, and for, the periods presented in this report; |
4. |
The registrant's other certifying officer and I are responsible for establishing and maintaining disclosure controls and procedures (as defined in Exchange Act Rules 13a-15(e) and 15d-15(e)) for the registrant and have: |
| (a) | Designed such disclosure controls and procedures, or caused such disclosure controls and procedures to be designed under our supervision, to ensure that material information relating to the registrant, including its consolidated subsidiaries, is made known to us by others within those entities, particularly during the period in which this report is being prepared; |
| (b) | Evaluated the effectiveness of the registrant's disclosure controls and procedures and presented in this report our conclusions about the effectiveness of the disclosure controls and procedures, as of the end of the period covered by this report based on such evaluation; and |
| (c) | Disclosed in this report any change in the registrant's internal control over financial reporting that occurred during the registrant's most recent fiscal quarter (the registrant's fourth fiscal quarter in the case of an annual report) that has materially affected, or is reasonably likely to materially affect, the registrant's internal control over financial reporting; and |
5. |
The registrant's other certifying officer and I have disclosed, based on our most recent evaluation of internal control over financial reporting, to the registrant's auditors and the audit committee of the registrant's board of directors (or persons performing the equivalent functions): |
| (a) | All significant deficiencies and material weaknesses in the design or operation of internal control over financial reporting which are reasonably likely to adversely affect the registrant's ability to record, process, summarize and report financial information; and |
| (b) | Any fraud, whether or not material, that involves management or other employees who have a significant role in the registrant's internal control over financial reporting. |
Date: March 5, 2024 |
By: |
/s/ Michael Henderson, M.D. |
|
|
Michael Henderson, M.D. |
|
|
Chief Executive Officer |
Exhibit 31.2
CERTIFICATION PURSUANT TO
RULES 13a-14(a) AND 15d-14(a) UNDER THE SECURITIES EXCHANGE ACT OF 1934,
AS ADOPTED PURSUANT TO SECTION 302 OF THE SARBANES-OXLEY ACT OF 2002
I, Jane Pritchett Henderson, certify that:
1. |
I have reviewed this Annual Report on Form 10-K of Apogee Therapeutics, Inc.; |
2. |
Based on my knowledge, this report does not contain any untrue statement of a material fact or omit to state a material fact necessary to make the statements made, in light of the circumstances under which such statements were made, not misleading with respect to the period covered by this report; |
3. |
Based on my knowledge, the financial statements, and other financial information included in this report, fairly present in all material respects the financial condition, results of operations and cash flows of the registrant as of, and for, the periods presented in this report; |
4. |
The registrant's other certifying officer and I are responsible for establishing and maintaining disclosure controls and procedures (as defined in Exchange Act Rules 13a-15(e) and 15d-15(e)) for the registrant and have: |
| (a) | Designed such disclosure controls and procedures, or caused such disclosure controls and procedures to be designed under our supervision, to ensure that material information relating to the registrant, including its consolidated subsidiaries, is made known to us by others within those entities, particularly during the period in which this report is being prepared; |
| (b) | Evaluated the effectiveness of the registrant's disclosure controls and procedures and presented in this report our conclusions about the effectiveness of the disclosure controls and procedures, as of the end of the period covered by this report based on such evaluation; and |
| (c) | Disclosed in this report any change in the registrant's internal control over financial reporting that occurred during the registrant's most recent fiscal quarter (the registrant's fourth fiscal quarter in the case of an annual report) that has materially affected, or is reasonably likely to materially affect, the registrant's internal control over financial reporting; and |
5. |
The registrant's other certifying officer and I have disclosed, based on our most recent evaluation of internal control over financial reporting, to the registrant's auditors and the audit committee of the registrant's board of directors (or persons performing the equivalent functions): |
| (a) | All significant deficiencies and material weaknesses in the design or operation of internal control over financial reporting which are reasonably likely to adversely affect the registrant's ability to record, process, summarize and report financial information; and |
| (b) | Any fraud, whether or not material, that involves management or other employees who have a significant role in the registrant's internal control over financial reporting. |
Date: March 5, 2024 |
By: |
/s/ Jane Pritchett Henderson |
|
|
Jane Pritchett Henderson |
|
|
Chief Financial Officer (principal financial and accounting officer) |
Exhibit 32.1
CERTIFICATION PURSUANT TO
18 U.S.C. SECTION 1350, AS ADOPTED PURSUANT TO
SECTION 906 OF THE SARBANES-OXLEY ACT OF 2002
In connection with the Annual Report on Form 10-K of Apogee Therapeutics, Inc. (the “Company”) for the year ended December 31, 2023 as filed with the Securities and Exchange Commission on the date hereof (the “Report”), each of the undersigned officers of the Company hereby certifies, pursuant to 18 U.S.C. § 1350, as adopted pursuant to § 906 of the Sarbanes-Oxley Act of 2002, that to the best of his knowledge:
Date: March 5, 2024 |
By: |
/s/ Michael Henderson, M.D. |
|
|
Michael Henderson, M.D. |
|
|
Chief Executive Officer |
|
|
|
Date: March 5, 2024 |
By: |
/s/ Jane Pritchett Henderson |
|
|
Jane Pritchett Henderson |
|
|
Chief Financial Officer |
The foregoing certification is being furnished solely to accompany the Report pursuant to 18 U.S.C. § 1350, and is not being filed for purposes of Section 18 of the Securities Exchange Act of 1934, as amended, and is not to be incorporated by reference into any filing of the Company, whether made before or after the date hereof, regardless of any general incorporation language in such filing.
Note: A signed original of this written statement required by § 906 has been provided to the Company and will be retained by the Company and furnished to the Securities and Exchange Commission or its staff upon request.
Exhibit 97.1

INCENTIVE COMPENSATION CLAWBACK POLICY
Recoupment of Incentive-Based Compensation
It is the policy of Apogee Therapeutics, Inc. (the “Company”) that, in the event the Company is required to prepare an accounting restatement of the Company’s financial statements (including any such correction that is material to the previously issued financial statements, or that would result in a material misstatement if the error were corrected in the current period or left uncorrected in the current period) due to material non-compliance with any financial reporting requirement under the federal securities laws, the Company will recover on a reasonably prompt basis the amount of any Incentive-Based Compensation Received by a Covered Executive during the Recovery Period that exceeds the amount that otherwise would have been Received had it been determined based on the restated financial statements.
Policy Administration and Definitions
This Incentive Compensation Clawback Policy (the “Policy”) is administered by the Compensation Committee (the “Committee”) of the Company’s Board of Directors, and is intended to comply with, and as applicable to be administered and interpreted consistent with, and subject to the exceptions set forth in, Listing Rule 5608 adopted by the Nasdaq Stock Market to implement Rule 10D-1 under the Securities Exchange Act of 1934, as amended (collectively, “Rule 10D-1”).
For purposes of this Policy:
“Incentive-Based Compensation” means any compensation granted, earned or vested based in whole or in part on the Company’s attainment of a Financial Reporting Measure that was Received by a person (i) on or after October 2, 2023 (or such later date on which Listing Rule 5608 becomes effective in accordance with its terms) and after the person began service as a Covered Executive, and (ii) who served as a Covered Executive at any time during the performance period for the Incentive-Based Compensation.
A “Financial Reporting Measure” is (i) any measure that is determined and presented in accordance with the accounting principles used in preparing the Company’s financial statements and any measure derived wholly or in part from such a measure, and (ii) any measure based in whole or in part on the Company’s stock price or total shareholder return. Incentive-Based Compensation includes cash compensation and any equity awards to the extent based in whole or in part on such attainment.
Incentive-Based Compensation is deemed to be “Received” in the fiscal period during which the relevant Financial Reporting Measure is attained, regardless of when the compensation is actually paid or awarded.
“Covered Executive” means any “executive officer” of the Company as defined under Rule 10D-1.
“Recovery Period” means the three completed fiscal years immediately preceding the date that the Company is required to prepare the accounting restatement described in this Policy, as determined pursuant to Rule 10D-1, and any transition period of less than nine months that is within or immediately following such three fiscal years, all as determined pursuant to Rule 10D-1.
Determinations by the Compensation Committee
If the Committee determines the amount of Incentive-Based Compensation Received by a Covered Executive during a Recovery Period exceeds the amount that would have been Received if determined or calculated based on the Company’s restated financial results, such excess amount of Incentive-Based Compensation shall be subject to recoupment by the Company pursuant to this Policy. For Incentive-Based Compensation based on stock price or total shareholder return, where the amount of erroneously awarded compensation is not subject to mathematical recalculation directly from the information in an accounting restatement, the Committee will determine the amount based on a reasonable estimate of the effect of the accounting restatement on the relevant stock price or total shareholder return. In all cases, the calculation of the excess amount of Incentive-Based Compensation to be recovered will be determined on a pre-tax basis. The Company will maintain and will provide to The Nasdaq Stock Market documentation of all determinations and actions taken in complying with this Policy. Any determinations made by the Committee under this Policy shall be final and binding on all affected individuals.
Methods of Clawback
The Company may effect any recovery pursuant to this Policy in any manner consistent with applicable law, including by requiring payment of such amount(s) to the Company, by set-off, by reducing future compensation, or by such other means or combination of means as the Committee determines to be appropriate. The Company need not recover the excess amount of Incentive-Based Compensation if and to the extent that the Committee determines that such recovery is impracticable, subject to and in accordance with any applicable exceptions under the Nasdaq Stock Market listing rules and not required under Rule 10D-1, including if the Committee determines that the direct expense paid to a third party to assist in enforcing this Policy would exceed the amount to be recovered after making a reasonable attempt to recover such amounts. The Company is authorized to take appropriate steps to implement this Policy with respect to Incentive-Based Compensation arrangements with Covered Executives.
Additional Recoupment for Fraud or Misconduct.
In any instance in which, in the view of the Committee, a Covered Executive engaged in an act of fraud or misconduct that contributed to the need for a financial restatement, the Committee may, in its discretion, recover and the Covered Executive shall forfeit or repay, all of the Covered Executive’s Incentive-Based Compensation for the relevant period, plus a reasonable rate of interest.
2
Not Exclusive Remedy
Any right of recoupment or recovery pursuant to this Policy is in addition to, and not in lieu of, any other remedies or rights of recoupment that may be available to the Company pursuant to the terms of any other policy, any employment agreement or plan or award terms, and any other legal remedies available to the Company; provided that the Company shall not recoup amounts pursuant to such other policy, terms or remedies to the extent it is recovered pursuant to this Policy. This Policy is also in addition to, and is not a substitute for, the requirements of Section 304 of the Sarbanes-Oxley Act of 2002. The Company shall not indemnify any Covered Executive against the loss of any Incentive-Based Compensation pursuant to this Policy.
RELATED DOCUMENTS
Document Number |
Title |
POL-001 |
Code of Business Conduct and Ethics |
POLICY OWNER
Title |
Responsibility |
General Counsel |
Under the oversight and direction of the Compensation Committee, responsible for administering policy |
REVISION HISTORY
Version |
Effective |
Summary of Change and Justification |
1.0 |
07/13/2023 |
Initial release of new policy and templates. |
3
APPROVALS
Name and Title |
Signature and Date |
|
|
|
|
|
|
4