UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d)
of The Securities Exchange Act of 1934
Date of Report (Date of earliest event reported): June 26, 2025
ALTIMMUNE, INC.
(Exact name of registrant as specified in its charter)
Delaware |
|
001-32587 |
|
20-2726770 |
|
(State or other jurisdiction of incorporation) |
|
(Commission File Number) |
|
(IRS Employer Identification No.) |
|
|
|
|
|
|
910 Clopper Road, Suite 201S Gaithersburg, Maryland |
|
|
|
20878 |
(Address of principal executive offices) |
|
|
|
(Zip Code) |
Registrant’s telephone number including area code: (240) 654-1450
Not Applicable
(Former name or former address, if changed since last report)
Check the appropriate box below if the Form 8-K filing is intended to simultaneously satisfy the filing obligation of the registrant under any of the following provisions:
☐ |
Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425) |
☐ |
Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12) |
☐ |
Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)) |
☐ |
Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section 12(b) of the Act:
Title of each class |
Trading Symbol(s) |
Name of each exchange on which registered |
Common stock, par value $0.0001 per share |
ALT |
The NASDAQ Global Market |
Indicate by check mark whether the registrant is an emerging growth company as defined in Rule 405 of the Securities Act of 1933 (§230.405 of this chapter) or Rule 12b-2 of the Securities Exchange Act of 1934 (§240.12b-2 of this chapter).
Emerging growth company ☐
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Item 7.01 Regulation FD Disclosure.
On June 26, 2025, Altimmune, Inc. (the “Company”) issued a press release titled “Altimmune Announces Positive Topline Results from the IMPACT Phase 2b Trial of Pemvidutide in the Treatment of MASH.” A copy of the press release is furnished as Exhibit 99.1 to this Current Report on Form 8-K.
The Company intends to host a conference call and live webcast to discuss the results on June 26, 2025 at 8:30 a.m. E.T. The Company has made available the slide presentation to accompany the call, furnished herewith as Exhibit 99.2 to this Current Report on Form 8-K. The information under this Item 7.01, including Exhibit 99.1 and Exhibit 99.2 hereto, is being furnished herewith and shall not be deemed “filed” for the purposes of Section 18 of the Securities Exchange Act of 1934, as amended (the “Exchange Act”), or otherwise subject to the liabilities of that section, nor shall such information be deemed incorporated by reference into any filing under the Securities Act of 1933, as amended (the “Securities Act”), or the Exchange Act, except as expressly set forth by specific reference in such filing.
Item 8.01 Other Events.
On June 26, 2025, the Company released topline results from IMPACT, a Phase 2b trial in metabolic dysfunction-associated steatohepatitis (“MASH”). The Phase 2b trial enrolled 212 participants with biopsy-confirmed MASH and fibrosis stages F2/F3 with and without diabetes randomized 1:2:2 to receive either weekly subcutaneous pemvidutide at 1.2 mg or 1.8 mg doses or placebo for 24 weeks.
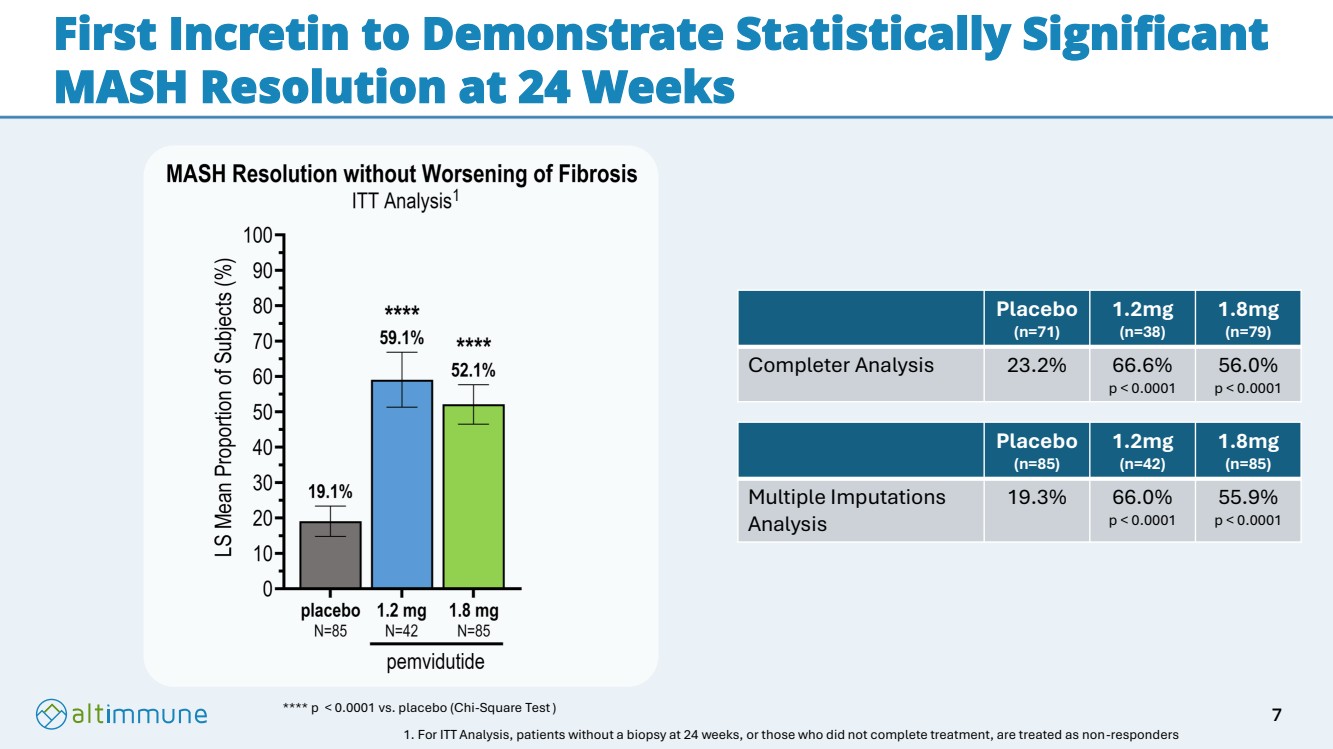
Treatment discontinuation rates were low, with only 9% of participants prematurely discontinuing treatment. In an intent-to-treat (ITT) analysis, in which participants with missing biopsies were considered non-responders, the proportions of participants achieving MASH resolution without worsening of fibrosis at 24 weeks were 59.1% and 52.1%, for pemvidutide 1.2 mg and 1.8 mg, respectively versus 19.1% for placebo (p< 0.0001 both doses). The effects on fibrosis improvement without worsening of MASH in an ITT analysis were 31.8% and 34.5% for pemvidutide 1.2 mg and 1.8 mg, respectively compared with 25.9% for placebo (differences not statistically significant). A supplemental AI-based analysis demonstrated statistically significant reductions in fibrosis, including 30.6% of participants receiving pemvidutide 1.8 mg achieving a 60% or more reduction in fibrosis compared to 8.2% receiving placebo (p< 0.001).
Statistically significant changes in well-established non-invasive tests (NITs) of fibrosis, including Enhanced Liver Fibrosis score (ELF) and Vibration-Controlled Transient Elastography (VCTE) were also observed compared with placebo at both doses. Together, these data suggest strong evidence of anti-fibrotic activity of pemvidutide in the MASH population. At 24 weeks, mean weight loss in pemvidutide-treated participants was 5.0% and 6.2% at the 1.2 mg and 1.8 mg doses, respectively, versus 1.0% in the placebo arm (p< 0.001, both doses). Pemvidutide also demonstrated favorable safety and tolerability, with 0.0% and 1.2% adverse events (AE) related discontinuations in the pemvidutide 1.2 mg and 1.8 mg groups versus 2.4% in the placebo group, and there were no serious adverse events (SAEs) related to study medication.
Highlights from the 24-week Topline Results
| ● | In an ITT analysis, MASH resolution without worsening of fibrosis was achieved in 59.1% and 52.1% of participants treated with pemvidutide 1.2 mg and 1.8 mg, respectively, vs. 19.1% of participants treated with placebo (p< 0.0001, both doses). |
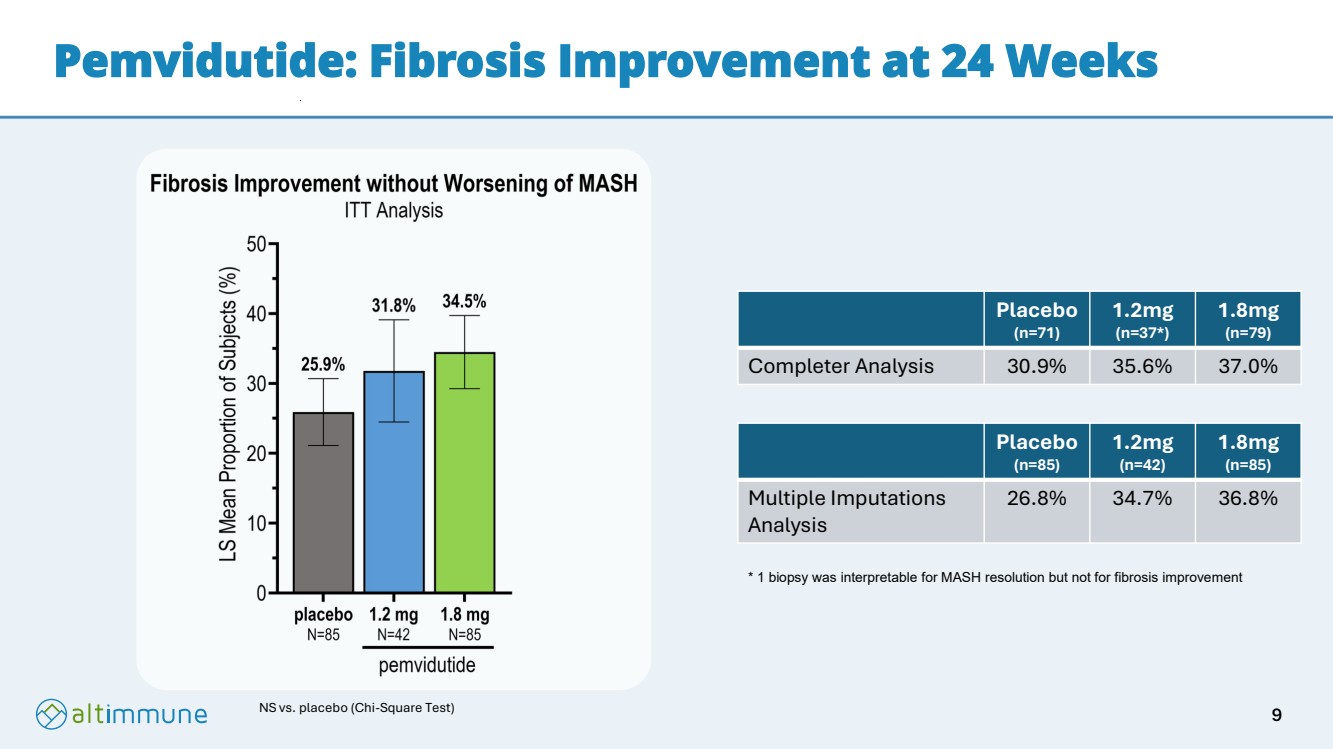
| ● | In an additional ITT analysis, fibrosis improvement without worsening of MASH was achieved in 31.8% and 34.5% of participants treated with pemvidutide 1.2 mg and 1.8 mg vs. 25.9% of participants treated with placebo (differences not significant). |
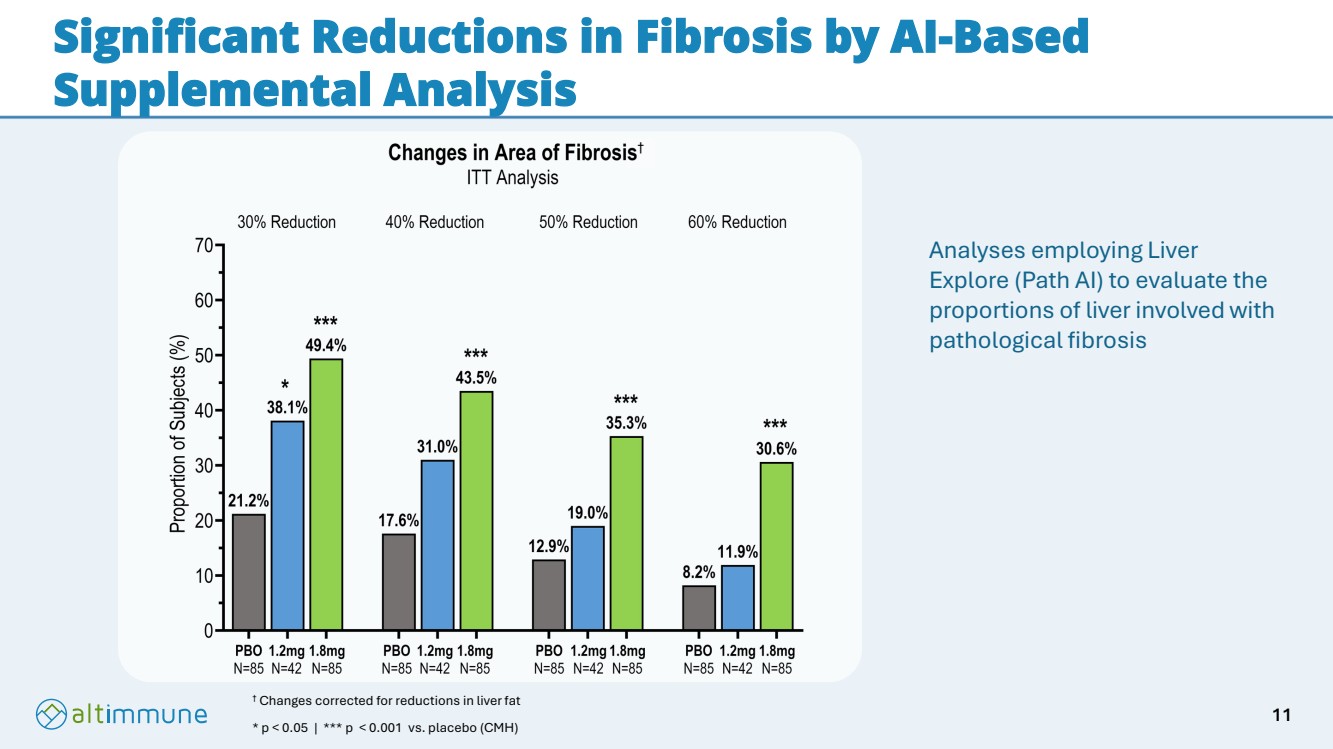
| ● | A supplemental AI-based analysis demonstrated statistically significant reductions in fibrosis, which included 30.6% of participants receiving pemvidutide 1.8 mg achieving a 60% or more reduction in fibrosis compared to 8.2% receiving placebo (p< 0.001). |
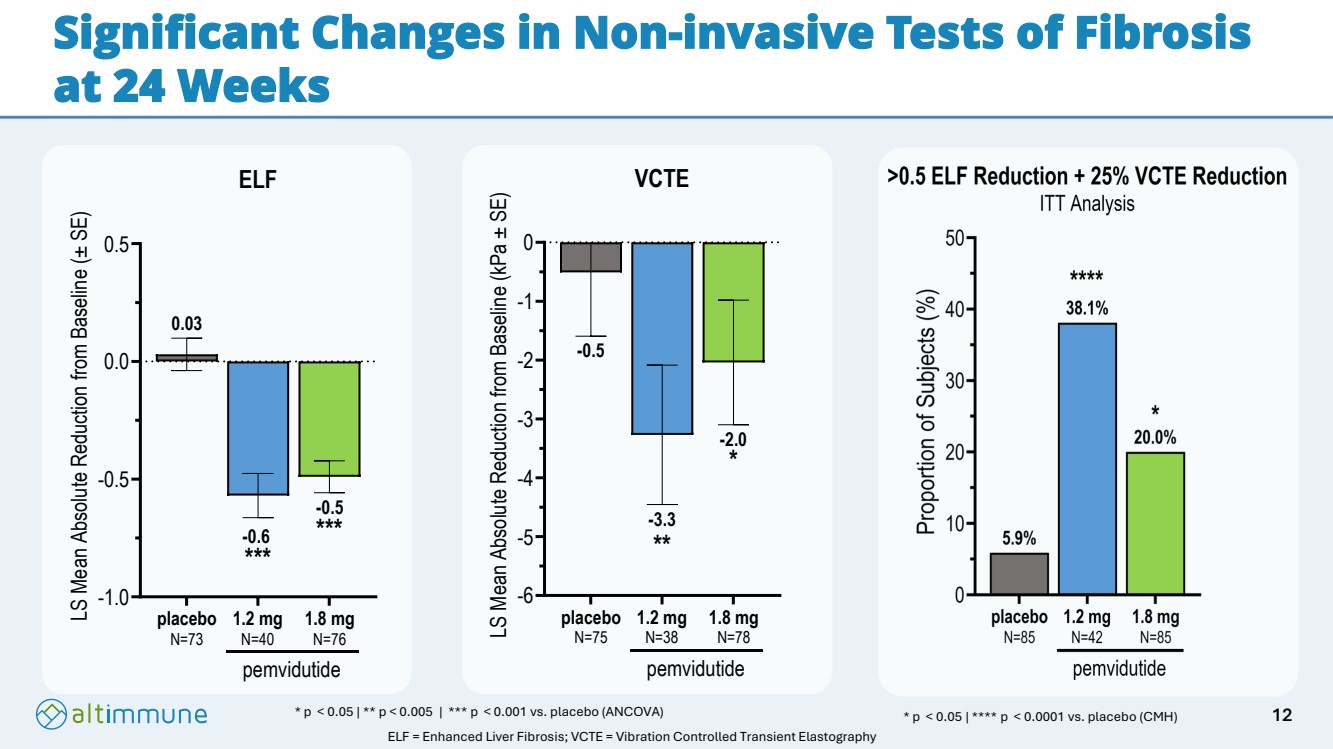
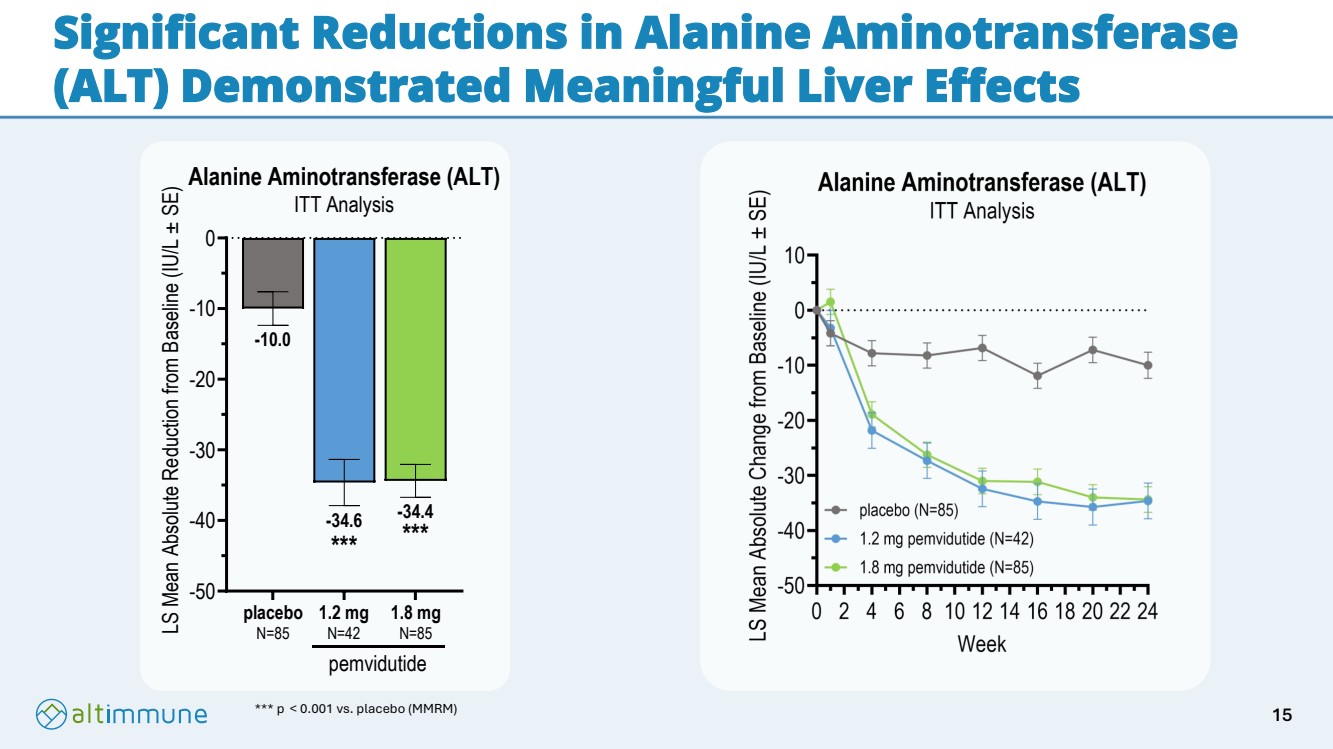
| ● | Pemvidutide-treated participants also achieved statistically significant reductions in non-invasive tests of fibrosis (ELF and VCTE) and inflammation (alanine aminotransferase, ALT). |
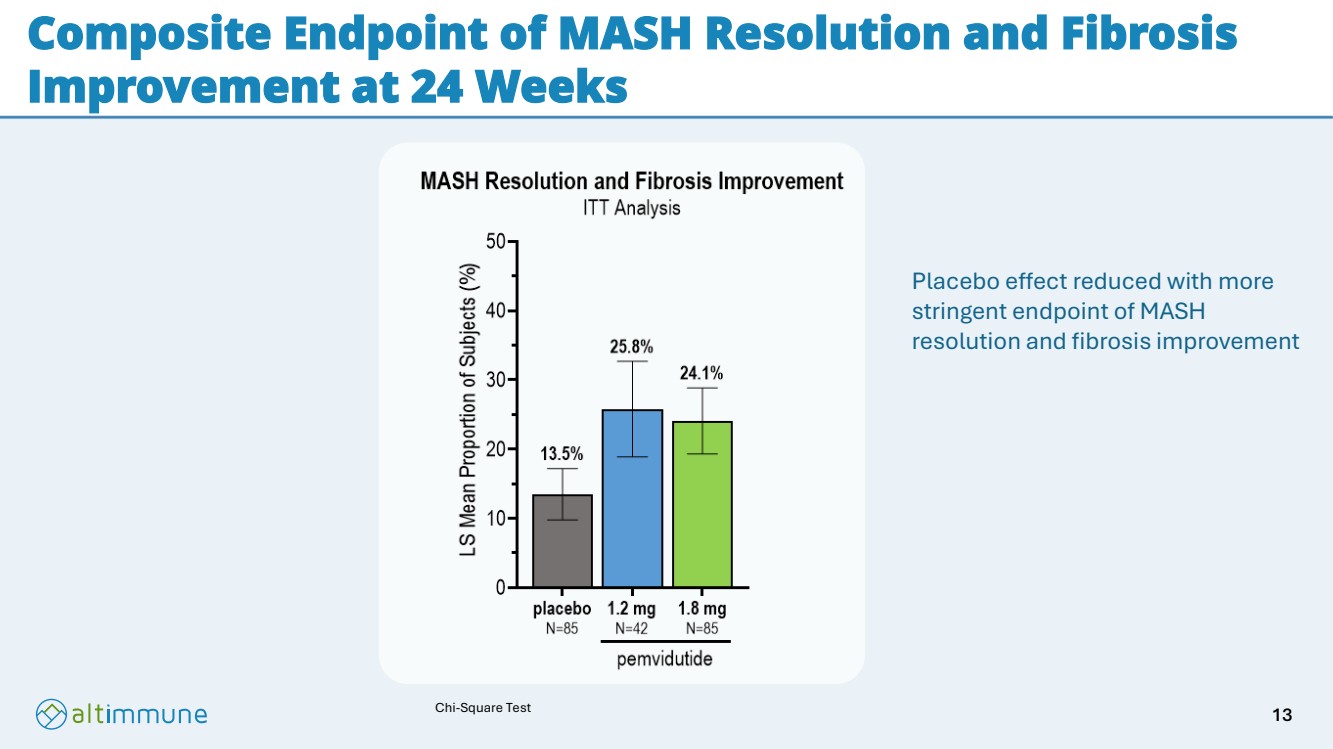
| ● | A total of 25.8% and 24.1% of participants receiving pemvidutide 1.2 mg and 1.8 mg, respectively, achieved the stringent endpoint of MASH resolution and fibrosis improvement versus 13.5% in participants receiving placebo (differences not significant). |
| ● | Participants receiving pemvidutide 1.2 mg and 1.8 mg achieved weight loss of 5.0% and 6.2% vs. 1.0% in placebo (p< 0.001), with the trajectory showing no plateauing at 24 weeks. |
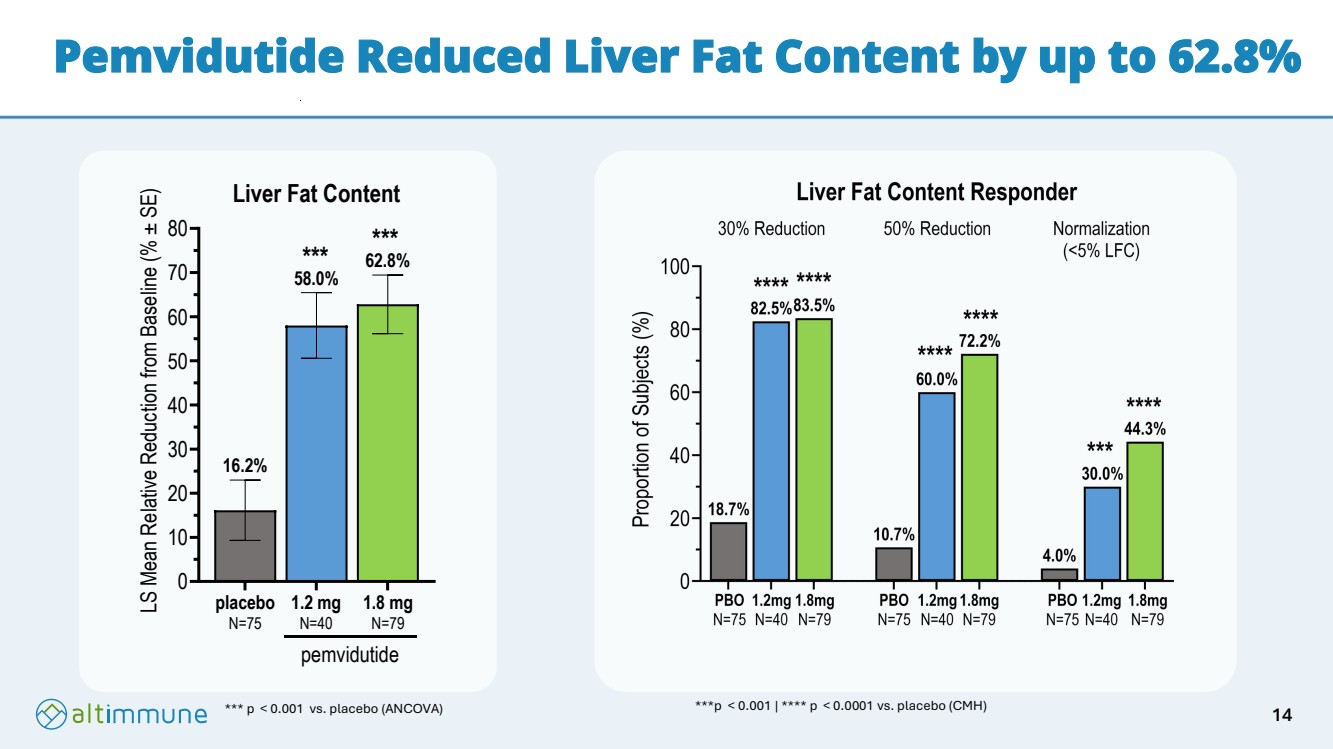
| ● | Liver fat reductions of 58.0% and 62.8% were achieved in participants who received pemvidutide 1.2 mg and 1.8 mg, respectively, vs. 16.2% in participants who received placebo (p< 0.001, both doses). |
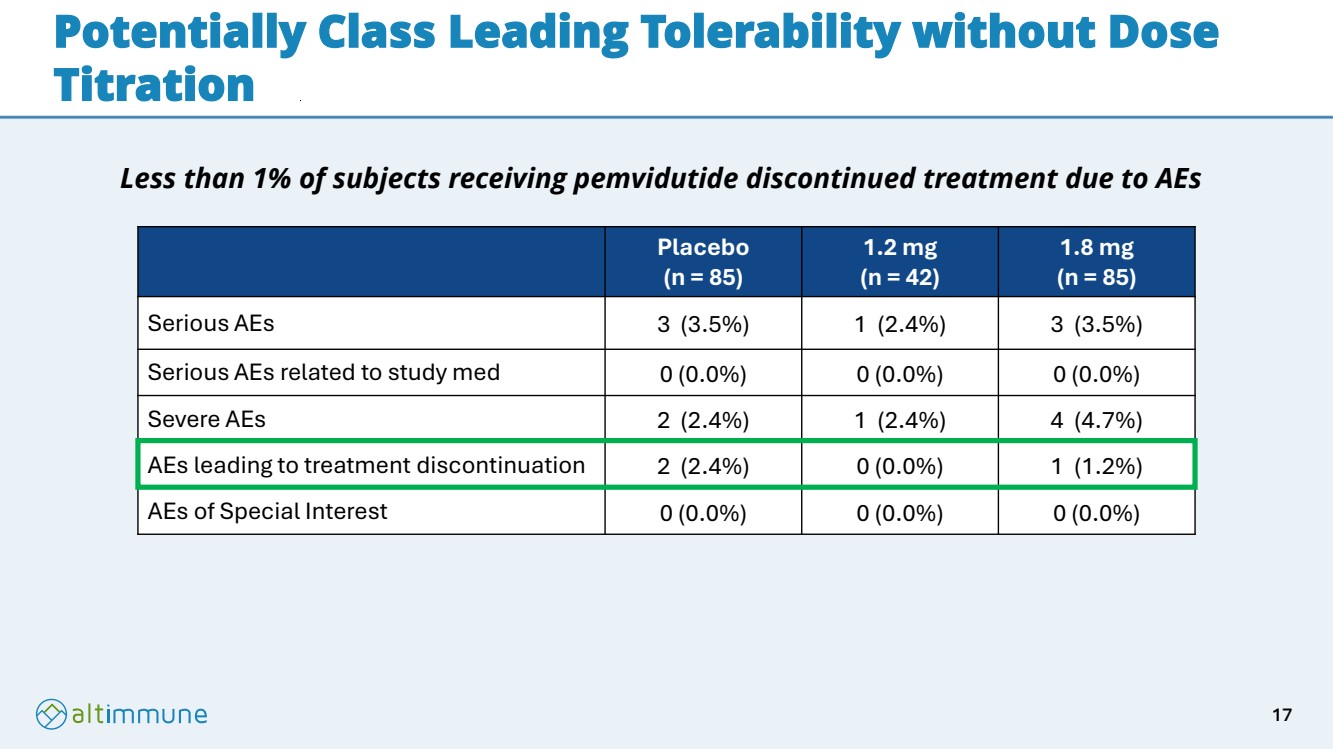
| ● | AEs leading to treatment discontinuation were 0.0% and 1.2% for pemvidutide 1.2 mg and 1.8 mg, respectively, vs. 2.4% in participants on placebo. |
| ● | No SAEs related to study drug or arrhythmias were reported at 24 weeks. |
| ● | Glycemic control was maintained with minimal changes in HbA1C regardless of diabetic status. |
|
Primary Endpoint (ITT analyses) |
Placebo (N=85) |
Pemvidutide 1.2 mg (N=42) |
Pemvidutide 1.8 mg (N=85) |
|
MASH resolution without worsening of fibrosis (%; LSM, Chi-Square Test) |
19.1 |
59.1**** |
52.1**** |
|
Fibrosis improvement without worsening of MASH (%; LSM, Chi-Square Test) |
25.9 |
31.8 |
34.5 |
|
****p < 0.0001 vs. placebo; LSM, least squares mean
Secondary Endpoints |
Placebo (N=85) |
Pemvidutide 1.2 mg (N=42) |
Pemvidutide 1.8 mg (N=85) |
|
Proportion of participants achieving the composite of both MASH resolution and improvement of liver fibrosis at 24 weeks (%; LSM, Chi-Square Test) |
13.5 |
25.8 |
24.1 |
|
Relative change in body weight at 24 weeks (%; LSM, MMRM) |
-1.0 |
-5.0*** |
-6.2*** |
|
***p < 0.001 vs. placebo; LSM, least square mean; MMRM, mixed model for repeated measures
Other Secondary Endpoints |
Placebo |
Pemvidutide 1.2 mg |
Pemvidutide 1.8 mg |
|
Relative reduction in liver fat content by MRI-PDFF (%; LSM, ANCOVA) |
16.2 N=75 |
58.0*** N=40 |
62.8*** N=79 |
|
Absolute change in alanine aminotransferase (ALT) (IU/L; LSM, MMRM) |
-10.0 N=85 |
-34.6*** N=42 |
-34.4*** N=85 |
|
Absolute change in Enhanced Liver Fibrosis (ELF) score (LSM, ANCOVA) |
0.03 N=73 |
-0.6*** N=40 |
-0.5*** N=76 |
|
Absolute change in Vibration-Controlled Transient Elastography (VCTE) (kPa; LSM, ANCOVA) |
-0.5 N=75 |
-3.3** N=38 |
-2.0* N=78 |
|
Proportion of participants with reduction of > 0.5 ELF + 25% VCTE, (%; CMH) |
5.9 N=85 |
38.1†††† N=42 |
20.0† N=85 |
|
*p < 0.05, ** p< 0.005, *** p< 0.001 vs. placebo (ANCOVA or MMRM)
†p < 0.05, †††† p< 0.0001 vs. placebo; LSM, least square mean; CMH, Cochran-Mantel-Haenszel; ANCOVA, analysis of co-variance
AI-based Fibrosis Analysis (ITT analyses) |
Placebo (N=85) |
1.2 mg (N=42) |
1.8 mg (N=85) |
|
Proportion of participants with a 30% reduction (%; CMH) |
21.2 |
38.1† |
49.4††† |
|
Proportion of participants with a 40% reduction (%; CMH) |
17.6 |
31.0 |
43.5††† |
|
Proportion of participants with a 50% reduction (%; CMH) |
12.9 |
19.0 |
35.3††† |
|
Proportion of participants with a 60% reduction (%; CMH) |
8.2 |
11.9 |
30.6††† |
|
†p< 0.05, ††† p< 0.001 vs. placebo; CMH, Cochran-Mantel-Haenszel
Adverse Events (AEs) |
Placebo (N=85) |
1.2 mg (N=42) |
1.8 mg (N=85) |
|
Serious AEs, n (%) |
3 (3.5) |
1 (2.4) |
3 (3.5) |
|
Serious AEs related to study med, n (%) |
0 (0.0) |
0 (0.0) |
0 (0.0) |
|
Severe AEs, n (%) |
2 (2.4) |
1 (2.4) |
4 (4.7) |
|
AEs leading to treatment discontinuation, n (%) |
2 (2.4) |
0 (0.0) |
1 (1.2) |
|
AEs of Special Interest, n (%) |
0 (0.0) |
0 (0.0) |
0 (0.0) |
|
This Current Report on Form 8-K and certain materials furnished or filed herewith contain forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995, as amended, including, without limitation, implied and express statements regarding: the Company’s business plans and objectives, including future plans or expectations for pemvidutide and ongoing clinical studies (including IMPACT), including the anticipated or potential therapeutic effects of pemvidutide, as well as the dosing, safety and tolerability of pemvidutide.
Any forward-looking statements are based on management’s current expectations of future events and are subject to a number of risks and uncertainties that could cause actual results to differ materially and adversely from those set forth in or implied by such forward-looking statements. Risks that contribute to the uncertain nature of the forward-looking statements include: the success, cost, and timing of the Company’s product candidate development activities and planned clinical trials; the Company’s ability to execute on its strategy; positive results from any of its clinical studies may not necessarily be predictive of the results of future or ongoing clinical studies; regulatory developments in the United States and foreign countries; the Company’s ability to fund operations. For a discussion of these and other risks and uncertainties, and other important factors, any of which could cause the Company’s actual results to differ from those contained in the forward-looking statements, see the section entitled “Risk Factors” in the Company’s annual report on Form 10-K filed, with the United States Securities and Exchange Commission (SEC) and quarterly reports on Form 10-Q filed with the SEC, as well as discussions of potential risks, uncertainties, and other important factors in the Company’s other filings with the SEC. All forward-looking statements contained in this presentation speak only as of the date on which they were made. The Company undertakes no obligation to update such statements to reflect events that occur or circumstances that exist after the date on which they were made.
Item 9.01 Financial Statements and Exhibits.
(d) Exhibits
Exhibit Number |
|
Description |
|
|
|
99.1 |
|
|
|
|
|
99.2 |
|
Phase 2b IMPACT Study slide presentation of Altimmune, Inc. dated June 26, 2025 |
|
|
|
104 |
|
Cover Page Interactive Data File (embedded within the Inline XBRL document) |
SIGNATURE
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
|
ALTIMMUNE, INC. |
||
|
|
|
|
|
By: |
|
/s/ Gregory Weaver |
|
|
|
Name: Gregory Weaver |
|
|
|
Title: Chief Financial Officer |
Dated: June 26, 2025

Exhibit 99.1
Altimmune Announces Positive Topline Results from the IMPACT Phase 2b Trial of Pemvidutide in the Treatment of MASH
First product candidate to demonstrate significant MASH effects and weight loss at 24 weeks
Trial met its primary endpoint with statistically significant MASH resolution without worsening of fibrosis in up to 59.1% of participants in an ITT analysis
Fibrosis improvement without worsening of MASH in up to 34.5% of participants in an ITT analysis
Supplemental AI-based analysis demonstrated statistically significant reductions in liver fibrosis at 24 weeks
Weight loss of up to 6.2% at 24 weeks with no plateauing
Potentially best-in-class tolerability, with less than 1% treatment discontinuations due to adverse events in pemvidutide-treated participants
Conference call to be held on June 26, 2025 at 8:30 am ET
GAITHERSBURG, MD, – June 26, 2025 – Altimmune, Inc. (Nasdaq: ALT), a late clinical-stage biopharmaceutical company developing novel peptide-based therapeutics for liver and cardiometabolic diseases, today announced positive topline results from the IMPACT Phase 2b trial in metabolic dysfunction-associated steatohepatitis (MASH).
The Phase 2b trial enrolled 212 participants with biopsy-confirmed MASH and fibrosis stages F2/F3 with and without diabetes randomized 1:2:2 to receive either weekly subcutaneous pemvidutide at 1.2 mg or 1.8 mg doses or placebo for 24 weeks. Treatment discontinuation rates were low, with only 9% of participants prematurely discontinuing treatment. In an intent-to-treat (ITT) analysis, in which participants with missing biopsies were considered non-responders, the proportions of participants achieving MASH resolution without worsening of fibrosis at 24 weeks were 59.1% and 52.1%, for pemvidutide 1.2 mg and 1.8 mg, respectively versus 19.1% for placebo (p< 0.0001 both doses). The effects on fibrosis improvement without worsening of MASH in an ITT analysis were 31.8% and 34.5% for pemvidutide 1.2 mg and 1.8 mg, respectively compared with 25.9% for placebo (differences not statistically significant). A supplemental AI-based analysis demonstrated statistically significant reductions in fibrosis, including 30.6% of participants receiving pemvidutide 1.8 mg achieving a 60% or more reduction in fibrosis compared to 8.2% receiving placebo (p< 0.001). Statistically significant changes in well-established non-invasive tests (NITs) of fibrosis, including Enhanced Liver Fibrosis score (ELF) and Vibration-Controlled Transient Elastography (VCTE) were also observed compared with placebo at both doses. Together, these data suggest strong evidence of anti-fibrotic activity of pemvidutide in the MASH population.
At 24 weeks, mean weight loss in pemvidutide-treated participants was 5.0% and 6.2% at the 1.2 mg and 1.8 mg doses, respectively, versus 1.0% in the placebo arm (p< 0.001, both doses). Pemvidutide also demonstrated favorable safety and tolerability, with 0.0% and 1.2% adverse events (AE) related discontinuations in the pemvidutide 1.2 mg and 1.8 mg groups versus 2.4% in the placebo group, and there were no serious adverse events (SAEs) related to study medication.
“These data represent an important step forward in the development of pemvidutide for the treatment of MASH and reinforce our conviction in its potential to disrupt the treatment paradigm in this serious and rapidly growing disease,” said Vipin K. Garg, Ph.D., President and Chief Executive Officer of Altimmune. “Despite a prevalence expected to exceed 27 million by 2030 in the United States alone, current treatment options are limited. We are excited to continue our efforts to bring this potentially transformative therapy to MASH patients.”
Dr. Mazen Noureddin, Professor of Medicine at the Houston Methodist Hospital and Co-Chairman of the Board for Summit and Pinnacle Clinical Research, commented, “The combination of MASH resolution and weight loss achieved at only 24 weeks is unique among drugs in development for MASH. The tolerability of pemvidutide was also impressive, with one of the lowest rates of AE-related drug discontinuations observed in any MASH clinical trial to date. The significant reduction in fibrosis in AI-based readings and its corroboration with established NITs suggest that pemvidutide has potent anti-fibrotic activity and that statistical significance on the fibrosis improvement endpoint could be achieved with longer durations of treatment.”
Dr. Scott Harris, Chief Medical Officer of Altimmune, emphasized that “Based on the results generated in the IMPACT trial, pemvidutide demonstrated significant MASH resolution and encouraging evidence of fibrosis improvement at 24 weeks. Additionally, when one considers the weight loss and favorable tolerability associated with pemvidutide, we believe that there is a clear path to a successful End of Phase 2 meeting with the FDA in the fourth quarter of 2025, enabling rapid progression to Phase 3.”
Highlights from the 24-week Topline Results
| ● | In an ITT analysis, MASH resolution without worsening of fibrosis was achieved in 59.1% and 52.1% of participants treated with pemvidutide 1.2 mg and 1.8 mg, respectively, vs. 19.1% of participants treated with placebo (p< 0.0001, both doses). |
| ● | In an additional ITT analysis, fibrosis improvement without worsening of MASH was achieved in 31.8% and 34.5% of participants treated with pemvidutide 1.2 mg and 1.8 mg vs. 25.9% of participants treated with placebo (differences not significant). |
| ● | A supplemental AI-based analysis demonstrated statistically significant reductions in fibrosis, which included 30.6% of participants receiving pemvidutide 1.8 mg achieving a 60% or more reduction in fibrosis compared to 8.2% receiving placebo (p< 0.001). |
| ● | Pemvidutide-treated participants also achieved statistically significant reductions in non-invasive tests of fibrosis (ELF and VCTE) and inflammation (alanine aminotransferase, ALT). |
| ● | A total of 25.8% and 24.1% of participants receiving pemvidutide 1.2 mg and 1.8 mg, respectively, achieved the stringent endpoint of MASH resolution and fibrosis improvement versus 13.5% in participants receiving placebo (differences not significant). |
| ● | Participants receiving pemvidutide 1.2 mg and 1.8 mg achieved weight loss of 5.0% and 6.2% vs. 1.0% in placebo (p< 0.001), with the trajectory showing no plateauing at 24 weeks. |
| ● | Liver fat reductions of 58.0% and 62.8% were achieved in participants who received pemvidutide 1.2 mg and 1.8 mg, respectively, vs. 16.2% in participants who received placebo (p< 0.001, both doses). |
| ● | AEs leading to treatment discontinuation were 0.0% and 1.2% for pemvidutide 1.2 mg and 1.8 mg, respectively, vs. 2.4% in participants on placebo. |
| ● | No SAEs related to study drug or arrhythmias were reported at 24 weeks. |
| ● | Glycemic control was maintained with minimal changes in HbA1C regardless of diabetic status |
|
Primary Endpoint (ITT analyses) |
Placebo (N=85) |
Pemvidutide 1.2 mg (N=42) |
Pemvidutide 1.8 mg (N=85) |
|
MASH resolution without worsening of fibrosis (%; LSM, Chi-Square Test) |
19.1 |
59.1**** |
52.1**** |
|
Fibrosis improvement without worsening of MASH (%; LSM, Chi-Square Test) |
25.9 |
31.8 |
34.5 |
|
****p < 0.0001 vs. placebo; LSM, least squares mean
Secondary Endpoints |
Placebo (N=85) |
Pemvidutide 1.2 mg (N=42) |
Pemvidutide 1.8 mg (N=85) |
|
Proportion of participants achieving the composite of both MASH resolution and improvement of liver fibrosis at 24 weeks (%; LSM, Chi-Square Test) |
13.5 |
25.8 |
24.1 |
|
Relative change in body weight at 24 weeks (%; LSM, MMRM) |
-1.0 |
-5.0*** |
-6.2*** |
|
***p < 0.001 vs. placebo; LSM, least square mean; MMRM, mixed model for repeated measures
Other Secondary Endpoints |
Placebo |
Pemvidutide 1.2 mg |
Pemvidutide 1.8 mg |
|
Relative reduction in liver fat content by MRI-PDFF (%; LSM, ANCOVA) |
16.2 N=75 |
58.0*** N=40 |
62.8*** N=79 |
|
Absolute change in alanine aminotransferase (ALT) (IU/L; LSM, MMRM) |
-10.0 N=85 |
-34.6*** N=42 |
-34.4*** N=85 |
|
Absolute change in Enhanced Liver Fibrosis (ELF) score (LSM, ANCOVA) |
0.03 N=73 |
-0.6*** N=40 |
-0.5*** N=76 |
|
Absolute change in Vibration-Controlled Transient Elastography (VCTE) (kPa; LSM, ANCOVA) |
-0.5 N=75 |
-3.3** N=38 |
-2.0* N=78 |
|
Proportion of participants with reduction of > 0.5 ELF + 25% VCTE, (%; CMH) |
5.9 N=85 |
38.1†††† N=42 |
20.0† N=85 |
|
*p < 0.05, ** p< 0.005, *** p< 0.001 vs. placebo (ANCOVA or MMRM)
†p < 0.05, †††† p< 0.0001 vs. placebo; LSM, least square mean; CMH, Cochran-Mantel-Haenszel; ANCOVA, analysis of co-variance
AI-based Fibrosis Analysis (ITT analyses) |
Placebo (N=85) |
1.2 mg (N=42) |
1.8 mg (N=85) |
|
Proportion of participants with a 30% reduction (%; CMH) |
21.2 |
38.1† |
49.4††† |
|
Proportion of participants with a 40% reduction (%; CMH) |
17.6 |
31.0 |
43.5††† |
|
Proportion of participants with a 50% reduction (%; CMH) |
12.9 |
19.0 |
35.3††† |
|
Proportion of participants with a 60% reduction (%; CMH) |
8.2 |
11.9 |
30.6††† |
|
†p< 0.05, ††† p< 0.001 vs. placebo; CMH, Cochran-Mantel-Haenszel
Adverse Events (AEs) |
Placebo (N=85) |
1.2 mg (N=42) |
1.8 mg (N=85) |
|
Serious AEs, n (%) |
3 (3.5) |
1 (2.4) |
3 (3.5) |
|
Serious AEs related to study med, n (%) |
0 (0.0) |
0 (0.0) |
0 (0.0) |
|
Severe AEs, n (%) |
2 (2.4) |
1 (2.4) |
4 (4.7) |
|
AEs leading to treatment discontinuation, n (%) |
2 (2.4) |
0 (0.0) |
1 (1.2) |
|
AEs of Special Interest, n (%) |
0 (0.0) |
0 (0.0) |
0 (0.0) |
|
Conference Call and Webcast
Altimmune will host a conference call and webcast on Thursday, June 26, 2025 at 8:30 am ET to review the Topline IMPACT data. In addition to remarks from Altimmune management, the call will include a discussion of the data and its implications with IMPACT Principal Investigator, Mazen Noureddin, M.D., MHSc.
The event will be available via the Events section of the Altimmune website.
About the IMPACT Study
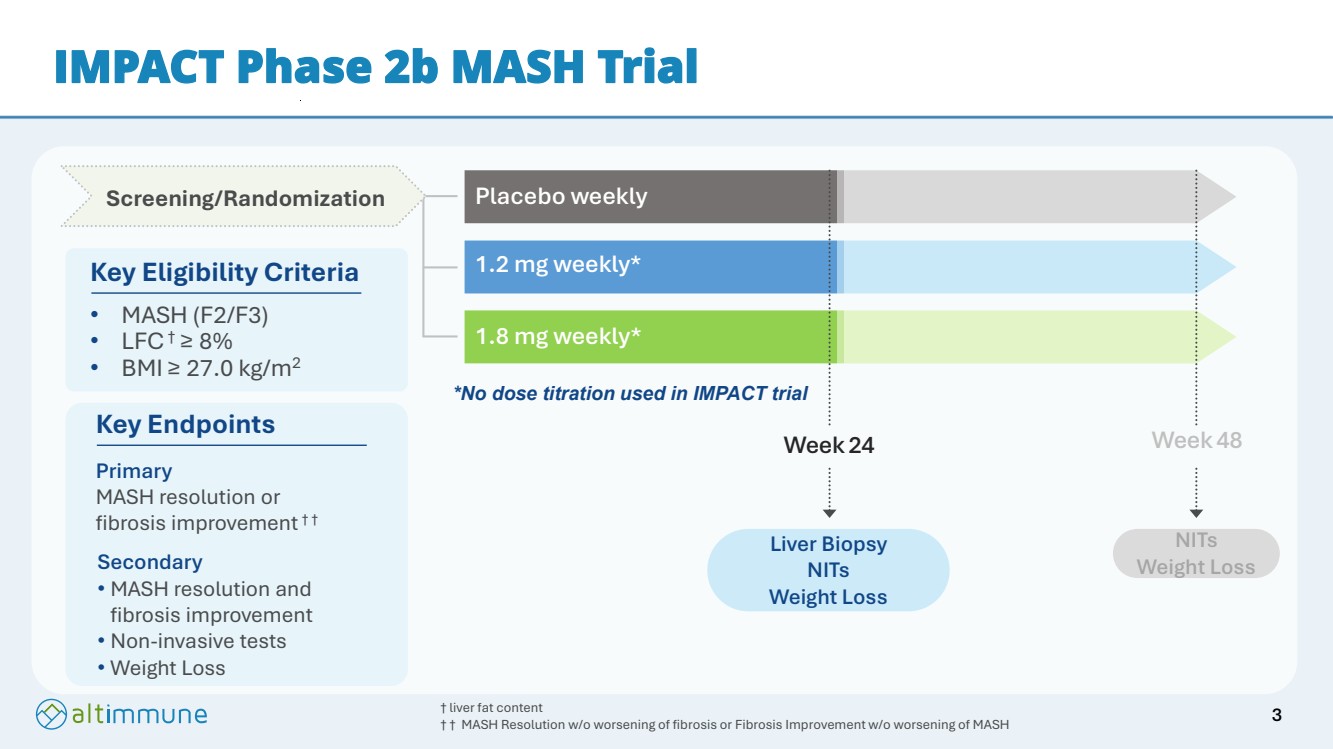
The IMPACT (NCT05989711) trial enrolled 212 participants with biopsy-confirmed MASH and fibrosis stages F2/F3 with and without diabetes randomized 1:2:2 to receive either weekly subcutaneous pemvidutide at 1.2 mg and 1.8 mg doses or placebo for 24 weeks. Key efficacy endpoints were MASH resolution without worsening of fibrosis, or fibrosis improvement without worsening of MASH at 24 weeks. Secondary endpoints included weight loss and non-invasive tests of fibrosis. Participants will receive a total of 48 weeks of treatment, and a final readout is anticipated in the fourth quarter of 2025.
About Pemvidutide
Pemvidutide is a novel, investigational, peptide-based 1:1 GLP-1/glucagon dual receptor agonist in development for the treatment of MASH, obesity, Alcohol Use Disorder (AUD) and Alcohol-associated Liver Disease (ALD). Activation of the GLP-1 and glucagon receptors is believed to mimic the complementary effects of diet and exercise on weight loss, with GLP-1 suppressing appetite and glucagon increasing energy expenditure. Glucagon is also recognized as having direct effects on hepatic fat metabolism, which is believed to lead to rapid reductions in levels of liver fat and serum lipids. In clinical trials to date, once-weekly pemvidutide has demonstrated statistically significant MASH resolution and positive trends in liver fibrosis improvement, compelling weight loss with class-leading lean mass preservation, and robust reductions in liver fat content, triglycerides, LDL cholesterol and blood pressure. The U.S. FDA has granted Fast Track designation to pemvidutide for the treatment of MASH. Pemvidutide completed the MOMENTUM Phase 2 obesity trial in 2024 and is being studied in the ongoing IMPACT Phase 2b MASH trial. IND applications in AUD and ALD have received FDA clearance, with a Phase 2 trial in AUD underway and a Phase 2 trial in ALD scheduled to commence in the third quarter of 2025.
About Altimmune
Altimmune is a late clinical-stage biopharmaceutical company focused on developing novel peptide-based therapeutics for liver and cardiometabolic diseases. The Company’s lead program is pemvidutide, a GLP-1/glucagon dual receptor agonist for the treatment of MASH, obesity, AUD and ALD. For more information, please visit www.altimmune.com.
Follow @Altimmune, Inc. on LinkedIn
Follow @AltimmuneInc on Twitter
Forward-Looking Statement
Any statements made in this press release related to the development or commercialization of product candidates and other business and financial matters, including without limitation, trial results and data, including the results of the IMPACT Phase 2b Trial and statements relating to fibrosis improvement and the achievement of statistical significance on the fibrosis improvement endpoint, the timing of key milestones for the Company’s clinical assets, future plans or expectations for pemvidutide for the treatment of MASH, and the prospects for receiving regulatory approval or commercializing or selling any product or drug candidates, are forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995.
In addition, when or if used in this press release, the words "may," "could," "should," "anticipate," "believe," "estimate," "expect," "intend," "plan," "predict" and similar expressions and their variants, as they relate to Altimmune, Inc. may identify forward-looking statements. The Company cautions that these forward-looking statements are subject to numerous assumptions, risks, and uncertainties, which change over time. Important factors that may cause actual results to differ materially from the results discussed in the forward looking statements or historical experience include risks and uncertainties, including risks relating to: delays in regulatory review, manufacturing and supply chain interruptions, access to clinical sites, enrollment, adverse effects on healthcare systems and disruption of the global economy; the reliability of the results of studies relating to human safety and possible adverse effects resulting from the administration of the Company's product candidates; the Company's ability to manufacture clinical trial materials on the timelines anticipated; and the success of future product advancements, including the success of future clinical trials. Further information on the factors and risks that could affect the Company's business, financial conditions and results of operations are contained in the Company's filings with the U.S. Securities and Exchange Commission, including under the heading "Risk Factors" in the Company's most recent annual report on Form 10-K, quarterly report on Form 10-Q and the Company’s other filings with the SEC, which are available at www.sec.gov.
Company Contact:
Gregory Weaver
Chief Financial Officer
Phone: 240-654-1450
ir@altimmune.com
Investor Contact:
Lee Roth
Burns McClellan
Phone: 646-382-3403
Iroth@burnsmc.com
Media Contact:
Jake Robison
Inizio Evoke Comms
Phone: 619-849-5383
jake.robison@inizioevoke.com
|
IMPACT Phase 2b MASH Trial - Topline Results Pemvidutide: Designed to be the Treatment of Choice for Liver and Cardiometabolic Diseases J u n e 2 6 , 2 0 2 5 Company Confidential |
|
Forward-looking statements Safe-Harbor Statement This presentation has been prepared by Altimmune, Inc. ("we," "us," "our," "Altimmune" or the "Company") and includes certain “forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995, including, but not limited to, statements relating to future financial or business performance, conditions, plans, prospects, trends, or strategies and other financial and business matters, including without limitation, the timing of key milestones for our clinical assets, the results of the IMPACT Phase 2b clinical trial evaluating pemvidutide in subjects with MASH, the performance of our drug candidates in ongoing and future clinical trials and the prospects for regulatory approval, commercializing or selling any product or drug candidates. In addition, when or if used in this press release, the words “may,” “could,” “should,” “anticipate,” “believe,” “estimate,” “expect,” “intend,” “plan,” “predict,” “suggest” and similar expressions and their variants, as they relate to the Company may identify forward-looking statements. The Company cautions that these forward-looking statements are subject to numerous assumptions, risks, and uncertainties, which change over time. Important factors that may cause actual results to differ materially from the results discussed in the forward looking statements or historical experience include risks and uncertainties, including risks such as delays in regulatory review, manufacturing and supply chain interruptions, access to clinical sites, enrollment, adverse effects on healthcare systems and disruption of the global economy; the impact subject baseline characteristics, including body weight, on the success of future trials; the reliability of the results of studies relating to human safety and possible adverse effects resulting from the administration of the Company’s product candidates; the Company’s ability to manufacture clinical trial materials on the timelines anticipated; and the success of future product advancements, including the success of future clinical trials. Further information on the factors and risks that could affect the Company's business, financial conditions and results of operations are contained in the Company’s filings with the U.S. Securities and Exchange Commission, including under the heading “Risk Factors” in the Company’s latest annual report on Form 10-K, quarterly report on Form 10-Q and our other filings with the SEC, which are available at www.sec.gov. 2 |
|
1.2 mg weekly* 1.8 mg weekly* Placebo weekly Week 48 NITs Weight Loss Week 24 Liver Biopsy NITs Weight Loss Screening/Randomization IMPACT Phase 2b MASH Trial Key Eligibility Criteria • MASH (F2/F3) • LFC† ≥ 8% • BMI ≥ 27.0 kg/m2 † liver fat content † † MASH Resolution w/o worsening of fibrosis or Fibrosis Improvement w/o worsening of MASH Key Endpoints Primary MASH resolution or fibrosis improvement † † Secondary • MASH resolution and fibrosis improvement • Non-invasive tests • Weight Loss *No dose titration used in IMPACT trial 3 |
|
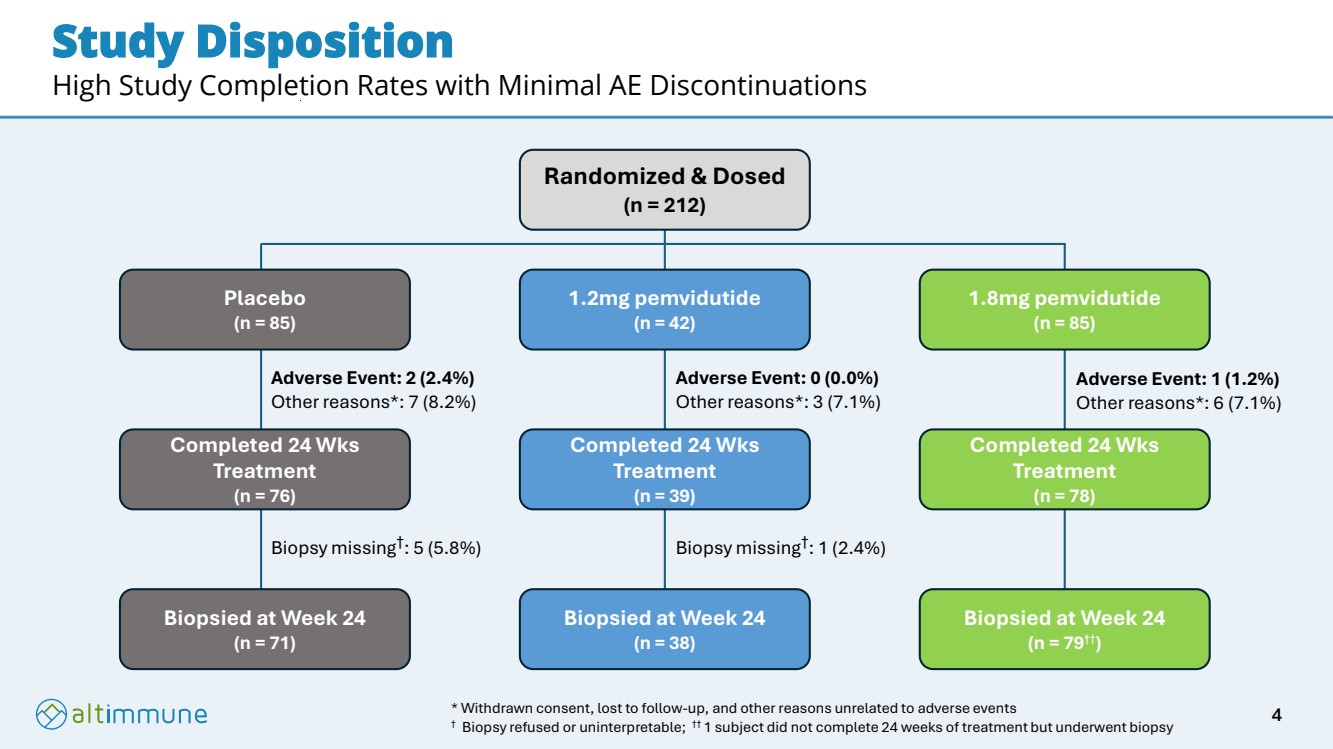
Study Disposition High Study Completion Rates with Minimal AE Discontinuations Randomized & Dosed (n = 212) Placebo (n = 85) 1.2mg pemvidutide (n = 42) 1.8mg pemvidutide (n = 85) Completed 24 Wks Treatment (n = 76) Completed 24 Wks Treatment (n = 39) Completed 24 Wks Treatment (n = 78) Biopsied at Week 24 (n = 71) Biopsied at Week 24 (n = 38) Biopsied at Week 24 (n = 79††) Adverse Event: 2 (2.4%) Other reasons*: 7 (8.2%) Biopsy missing† : 5 (5.8%) Biopsy missing† : 1 (2.4%) Adverse Event: 0 (0.0%) Other reasons*: 3 (7.1%) Adverse Event: 1 (1.2%) Other reasons*: 6 (7.1%) * Withdrawn consent, lost to follow-up, and other reasons unrelated to adverse events † Biopsy refused or uninterpretable; †† 1 subject did not complete 24 weeks of treatment but underwent biopsy 4 |
|
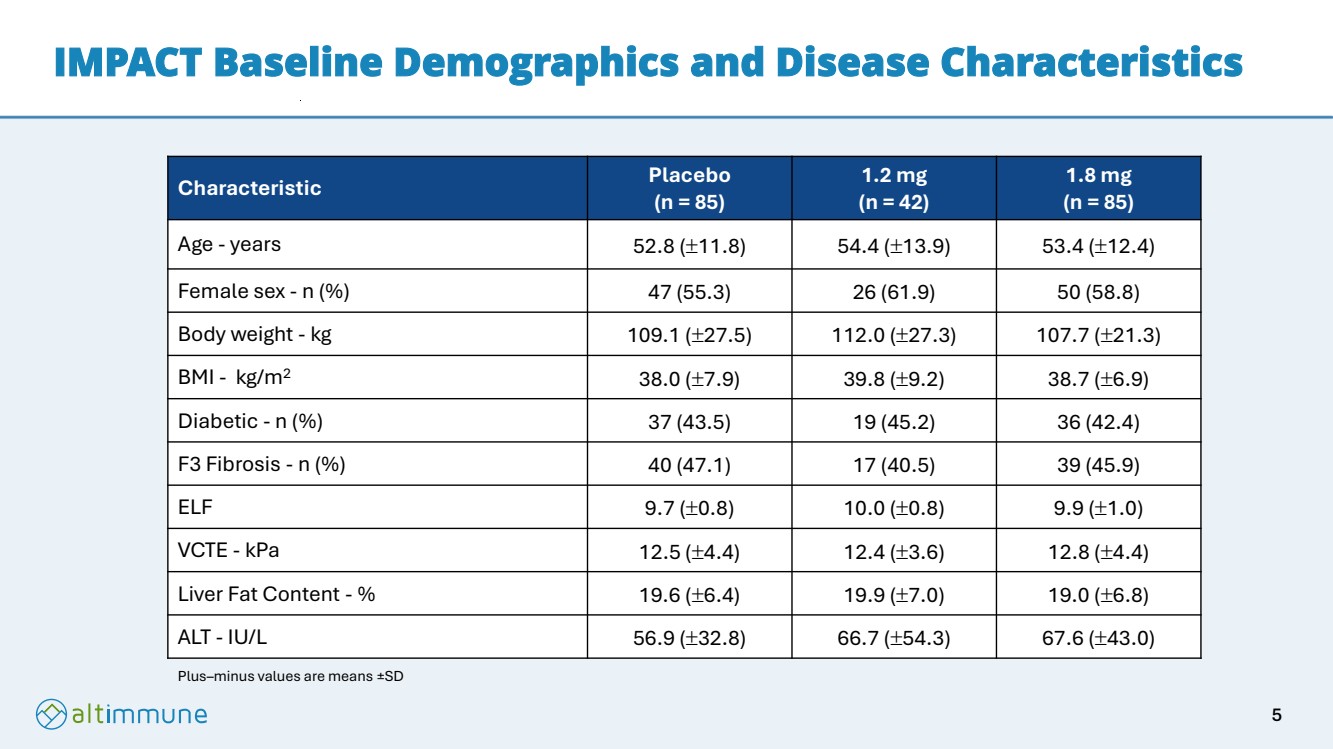
IMPACT Baseline Demographics and Disease Characteristics Characteristic Placebo (n = 85) 1.2 mg (n = 42) 1.8 mg (n = 85) Age - years 52.8 (11.8) 54.4 (13.9) 53.4 (12.4) Female sex - n (%) 47 (55.3) 26 (61.9) 50 (58.8) Body weight - kg 109.1 (27.5) 112.0 (27.3) 107.7 (21.3) BMI - kg/m2 38.0 (7.9) 39.8 (9.2) 38.7 (6.9) Diabetic - n (%) 37 (43.5) 19 (45.2) 36 (42.4) F3 Fibrosis - n (%) 40 (47.1) 17 (40.5) 39 (45.9) ELF 9.7 (0.8) 10.0 (0.8) 9.9 (1.0) VCTE - kPa 12.5 (4.4) 12.4 (3.6) 12.8 (4.4) Liver Fat Content - % 19.6 (6.4) 19.9 (7.0) 19.0 (6.8) ALT - IU/L 56.9 (32.8) 66.7 (54.3) 67.6 (43.0) Plus–minus values are means ±SD 5 |
|
Two Methods of Biopsy Reading Employed Pathologist reading • Biopsies independently scored by three pathologists using the mode method • Pathologists blinded to subject, treatment, and timepoint (sequence of sampling) Supplemental AI-based reading • Blindly scored biopsies without knowledge of treatment assignment or timepoint of treatment • Analyses limited to fibrosis quantification 6 |
|
First Incretin to Demonstrate Statistically Significant MASH Resolution at 24 Weeks **** p < 0.0001 vs. placebo (Chi-Square Test) Placebo (n=71) 1.2mg (n=38) 1.8mg (n=79) Completer Analysis 23.2% 66.6% p < 0.0001 56.0% p < 0.0001 Placebo (n=85) 1.2mg (n=42) 1.8mg (n=85) Multiple Imputations Analysis 19.3% 66.0% p < 0.0001 55.9% p < 0.0001 1. For ITT Analysis, patients without a biopsy at 24 weeks, or those who did not complete treatment, are treated as non-responders 1 7 |
|
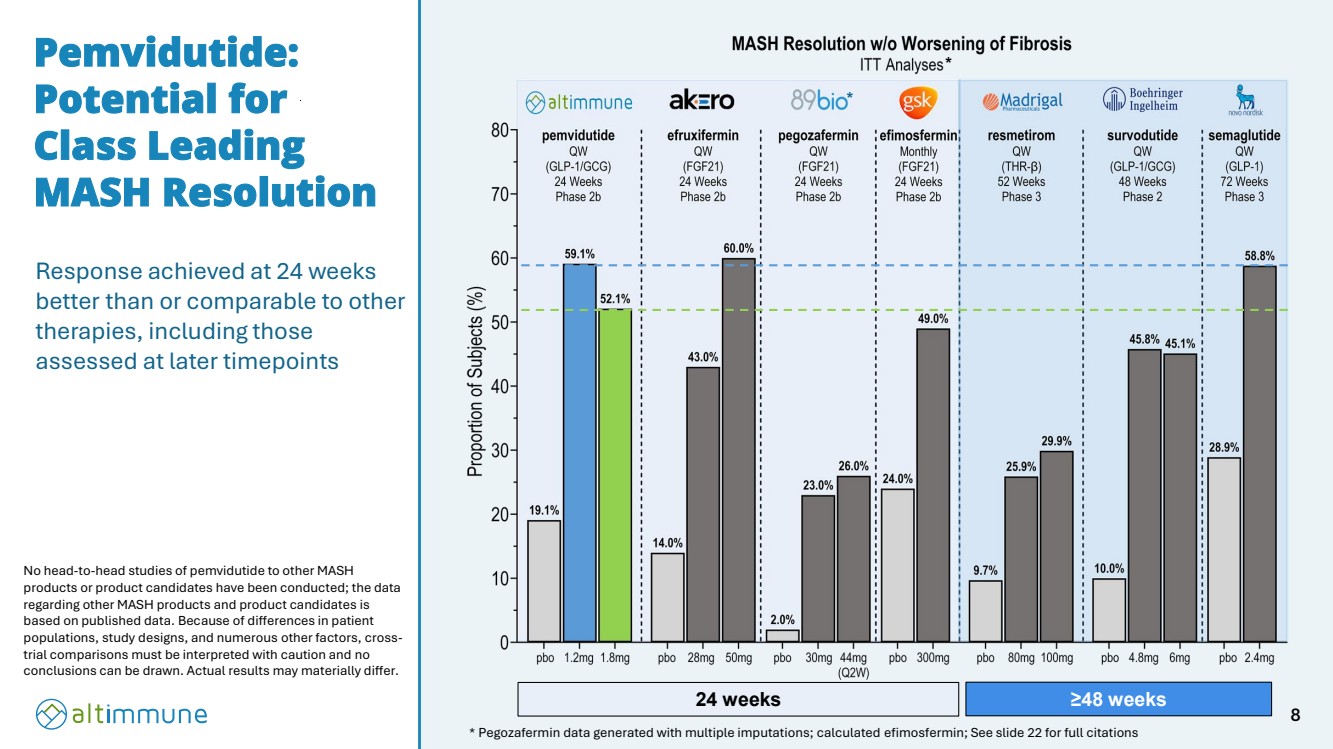
Response achieved at 24 weeks better than or comparable to other therapies, including those assessed at later timepoints Pemvidutide: Potential for Class Leading MASH Resolution * Pegozafermin data generated with multiple imputations; calculated efimosfermin; See slide 22 for full citations * No head-to-head studies of pemvidutide to other MASH products or product candidates have been conducted; the data regarding other MASH products and product candidates is based on published data. Because of differences in patient populations, study designs, and numerous other factors, cross-trial comparisons must be interpreted with caution and no conclusions can be drawn. Actual results may materially differ. 24 weeks ≥48 weeks * 8 |
|
Pemvidutide: Fibrosis Improvement at 24 Weeks NS vs. placebo (Chi-Square Test) Placebo (n=71) 1.2mg (n=37*) 1.8mg (n=79) Completer Analysis 30.9% 35.6% 37.0% Placebo (n=85) 1.2mg (n=42) 1.8mg (n=85) Multiple Imputations Analysis 26.8% 34.7% 36.8% * 1 biopsy was interpretable for MASH resolution but not for fibrosis improvement 9 |
|
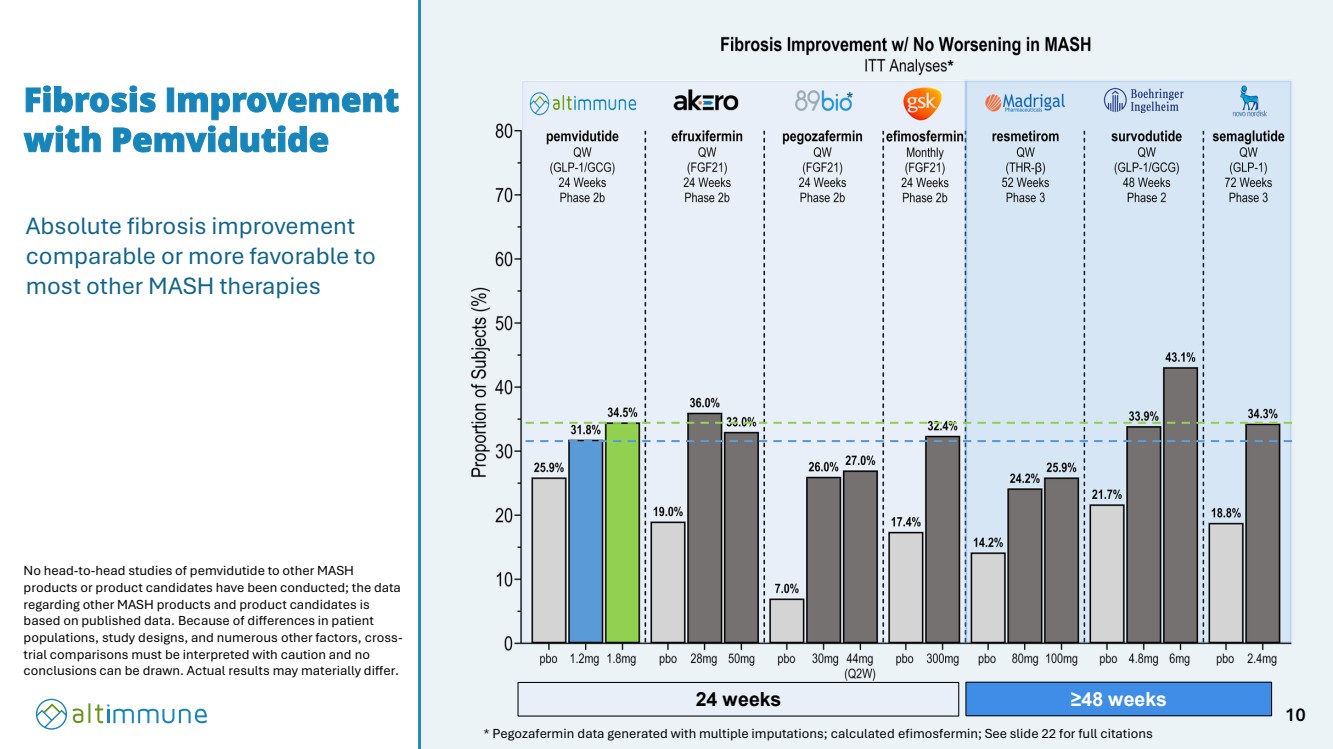
Fibrosis Improvement with Pemvidutide * * Pegozafermin data generated with multiple imputations; calculated efimosfermin; See slide 22 for full citations No head-to-head studies of pemvidutide to other MASH products or product candidates have been conducted; the data regarding other MASH products and product candidates is based on published data. Because of differences in patient populations, study designs, and numerous other factors, cross-trial comparisons must be interpreted with caution and no conclusions can be drawn. Actual results may materially differ. 24 weeks ≥48 weeks Absolute fibrosis improvement comparable or more favorable to most other MASH therapies * 10 |
|
Significant Reductions in Fibrosis by AI-Based Supplemental Analysis † Changes corrected for reductions in liver fat * p < 0.05 | *** p < 0.001 vs. placebo (CMH) † Analyses employing Liver Explore (Path AI) to evaluate the proportions of liver involved with pathological fibrosis 11 |
|
Significant Changes in Non-invasive Tests of Fibrosis at 24 Weeks * p < 0.05 | ** p < 0.005 | *** p < 0.001 vs. placebo (ANCOVA) -1.0 -0.5 0.0 0.5 ELF LS Mean Absolute Reduction from Baseline (± SE) placebo N=73 1.2 mg N=40 1.8 mg N=76 pemvidutide *** *** 0.03 -0.6 -0.5 -6 -5 -4 -3 -2 -1 0 -2.0 -3.3 -0.5 VCTE LS Mean Absolute Reduction from Baseline (kPa ± SE) placebo N=75 1.2 mg N=38 1.8 mg N=78 pemvidutide * ** * p < 0.05 | **** p < 0.0001 vs. placebo (CMH) ELF = Enhanced Liver Fibrosis; VCTE = Vibration Controlled Transient Elastography 12 |
|
Composite Endpoint of MASH Resolution and Fibrosis Improvement at 24 Weeks Chi-Square Test Placebo effect reduced with more stringent endpoint of MASH resolution and fibrosis improvement 13 |
|
Pemvidutide Reduced Liver Fat Content by up to 62.8% *** p < 0.001 vs. placebo (ANCOVA) 0 10 20 30 40 50 60 70 80 62.8% 58.0% 16.2% Liver Fat Content LS Mean Relative Reduction from Baseline (% ± SE) placebo N=75 1.2 mg N=40 1.8 mg N=79 pemvidutide *** *** ***p < 0.001 | **** p < 0.0001 vs. placebo (CMH) 14 |
|
Significant Reductions in Alanine Aminotransferase (ALT) Demonstrated Meaningful Liver Effects *** p < 0.001 vs. placebo (MMRM) -50 -40 -30 -20 -10 0 -34.4 -34.6 -10.0 Alanine Aminotransferase (ALT) ITT Analysis LS Mean Absolute Reduction from Baseline (IU/L ± SE) placebo N=85 1.2 mg N=42 1.8 mg N=85 pemvidutide *** *** 15 |
|
Significant Weight Loss at 24 weeks Weight loss has been shown to be a critical element in MASH therapy1 Weight loss continuing at week 24 with no plateauing Opportunity to achieve greater weight loss with 2.4 mg dose in Phase 3 1. Vilar-Gomez E, et al. Weight Loss Through Lifestyle Modification Significantly Reduces Features of Nonalcoholic Steatohepatitis. Gastroenterology. 2015 Aug;149(2):367-78 *** p < 0.001 vs. placebo (MMRM) Weight Loss -10 -9 -8 -7 -6 -5 -4 -3 -2 -1 0 -6.2 -5.0 -1.0 LS Mean Relative Change from Baseline (% ± SE) placebo N=85 1.2 mg N=42 1.8 mg N=85 pemvidutide *** *** 16 |
|
Potentially Class Leading Tolerability without Dose Titration Placebo (n = 85) 1.2 mg (n = 42) 1.8 mg (n = 85) Serious AEs 3 (3.5%) 1 (2.4%) 3 (3.5%) Serious AEs related to study med 0 (0.0%) 0 (0.0%) 0 (0.0%) Severe AEs 2 (2.4%) 1 (2.4%) 4 (4.7%) AEs leading to treatment discontinuation 2 (2.4%) 0 (0.0%) 1 (1.2%) AEs of Special Interest 0 (0.0%) 0 (0.0%) 0 (0.0%) Less than 1% of subjects receiving pemvidutide discontinued treatment due to AEs 17 |
|
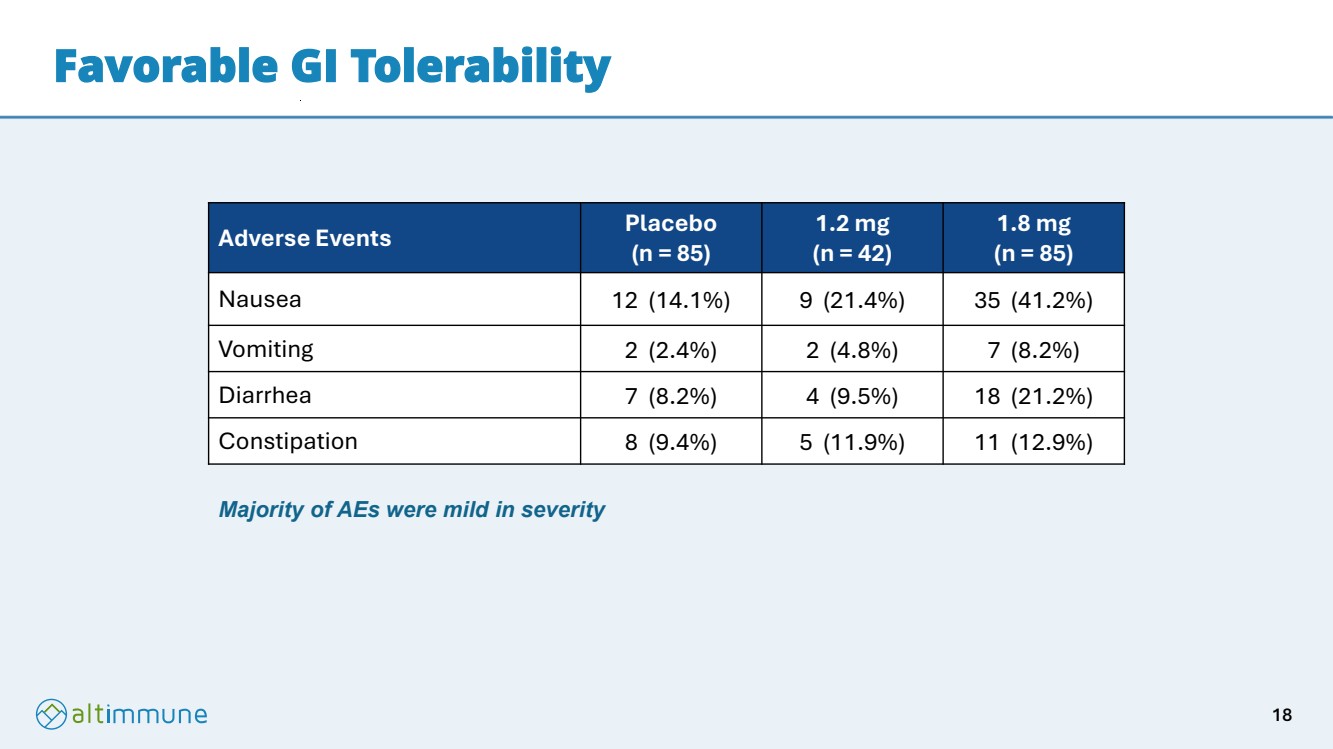
Favorable GI Tolerability Adverse Events Placebo (n = 85) 1.2 mg (n = 42) 1.8 mg (n = 85) Nausea 12 (14.1%) 9 (21.4%) 35 (41.2%) Vomiting 2 (2.4%) 2 (4.8%) 7 (8.2%) Diarrhea 7 (8.2%) 4 (9.5%) 18 (21.2%) Constipation 8 (9.4%) 5 (11.9%) 11 (12.9%) Majority of AEs were mild in severity 18 |
|
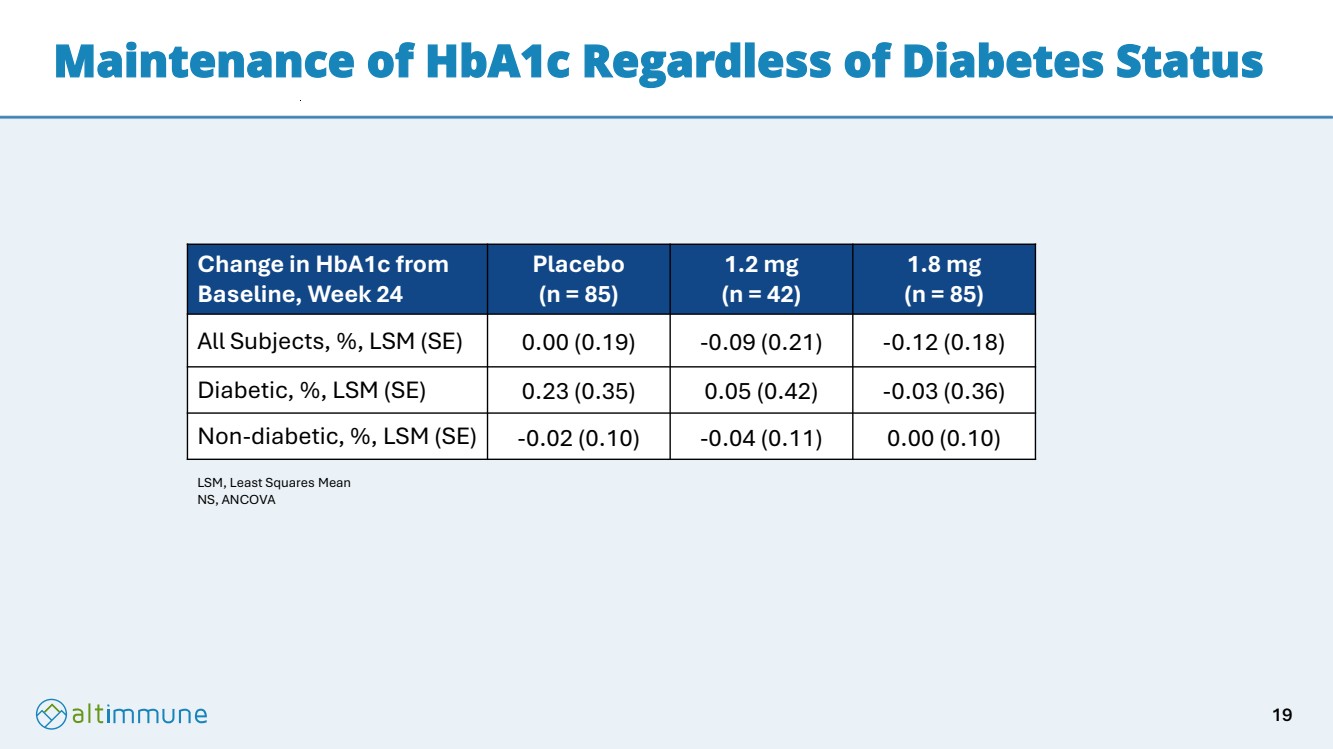
Maintenance of HbA1c Regardless of Diabetes Status Change in HbA1c from Baseline, Week 24 Placebo (n = 85) 1.2 mg (n = 42) 1.8 mg (n = 85) All Subjects, %, LSM (SE) 0.00 (0.19) -0.09 (0.21) -0.12 (0.18) Diabetic, %, LSM (SE) 0.23 (0.35) 0.05 (0.42) -0.03 (0.36) Non-diabetic, %, LSM (SE) -0.02 (0.10) -0.04 (0.11) 0.00 (0.10) LSM, Least Squares Mean NS, ANCOVA 19 |
|
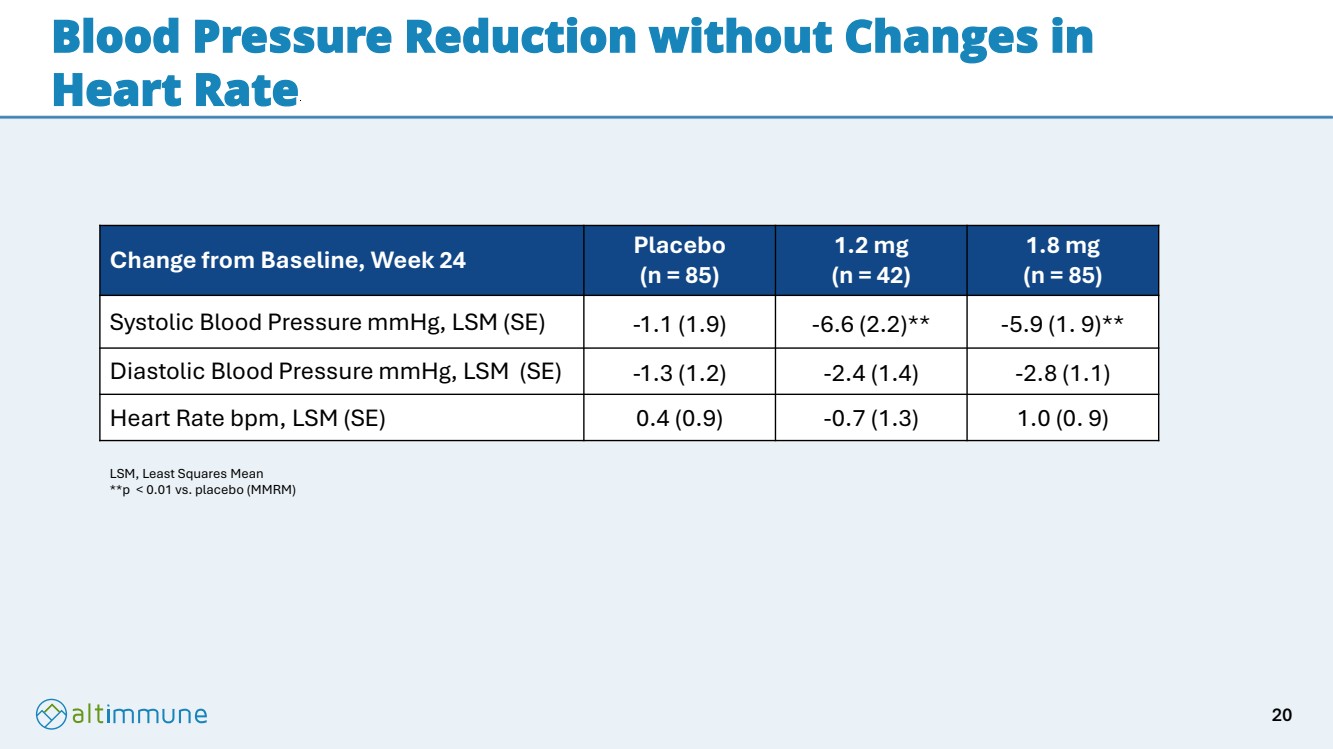
Blood Pressure Reduction without Changes in Heart Rate Change from Baseline, Week 24 Placebo (n = 85) 1.2 mg (n = 42) 1.8 mg (n = 85) Systolic Blood Pressure mmHg, LSM (SE) -1.1 (1.9) -6.6 (2.2)** -5.9 (1. 9)** Diastolic Blood Pressure mmHg, LSM (SE) -1.3 (1.2) -2.4 (1.4) -2.8 (1.1) Heart Rate bpm, LSM (SE) 0.4 (0.9) -0.7 (1.3) 1.0 (0. 9) LSM, Least Squares Mean **p < 0.01 vs. placebo (MMRM) 20 |
|
Pemvidutide IMPACT Phase 2b MASH Trial Summary First Product Candidate to Demonstrate Significant MASH Effects and Weight Loss at 24 Weeks • Trial met its primary endpoint with statistically significant and potentially class leading MASH resolution without worsening of fibrosis of up to 59.1% at 24 weeks • Fibrosis improvement without worsening of MASH of up to 34.5% at 24 weeks • Supplemental AI-based analysis demonstrated reductions in area of fibrosis • Statistically significant improvement in widely used non-invasive tests (NITs) of fibrosis • Robust liver fat reduction of up to 62.8% • Weight loss of up to 6.2% continuing at 24 weeks with no plateauing Potentially Best in Class Tolerability with No Dose Titration • Less than 1% discontinuation rate due to adverse events in subjects receiving pemvidutide • No heart rate increases or difference in cardiac AEs between pemvidutide and placebo • Maintenance of HbA1c regardless of diabetes status 21 |
|
References • MASH Resolution w/o Worsening of Fibrosis o Efruxifermin: Harrison et al. Lancet 2023 (Fig 2B). ITT analysis o Pegozafermin: Loomba et al. NEJM2023 (Fig. 1B). Multiple imputations o Efimosfermin: 11/2024 Phase 2 Results Deck (calculated based on completer data; Pbo N=41, 300mg N=43). Calculated ITT o Resmetirom: Harrison et al. NEJM 2024 (Fig 1A) . ITT analysis o Survodutide: Sanyal et al NEJM 2024 (Figure S7B). ITT analysis o Semaglutide: Sanyal et al NEJM 2025 (Table S4). ITT analysis • Fibrosis Improvement with No worsening in MASH o Efruxifermin: Harrison et al. Lancet 2023 (Fig 2B). ITT analysis o Pegozafermin: Loomba et al. NEJM2023 (Fig. 1B). Multiple imputations o Efimosfermin: 11/2024 Phase 2 Results Deck (calculated internally based on completer data; Pbo N=41, 300mg N=43). Calculated ITT o Resmetirom: Harrison et al. NEJM 2024 (Fig 1A) . ITT analysis o Survodutide: Sanyal et al NEJM 2024 (Figure S7B). ITT analysis o Semaglutide: Sanyal et al NEJM 2025 (Table S4). ITT analysis 22 |
|
Thank you 23 |