UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d)
of the Securities Exchange Act of 1934
Date of Report (Date of earliest event reported): December 14, 2023
MIND MEDICINE (MINDMED) INC.
(Exact name of Registrant as specified in its Charter)
| British Columbia, Canada | 001-40360 | 98-1582438 | ||
|
(State or other jurisdiction of incorporation or organization) |
(Commission File Number) |
(IRS Employer Identification No.) |
| One World Trade Center, Suite 8500 | ||||
| New York, NY | 10007 | |||
| (Address of principal executive offices) | (Zip Code) |
Registrant’s telephone number, including area code: (212) 220-6633
Not Applicable
(Former Name or Former Address, if Changed Since Last Report)
Check the appropriate box below if the Form 8-K filing is intended to simultaneously satisfy the filing obligation of the registrant under any of the following provisions:
| ☐ | Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425) |
| ☐ | Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12) |
| ☐ | Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)) |
| ☐ | Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section 12(b) of the Act:
Title of each class |
Trading |
Name of each exchange on which registered |
||
| Common Shares, no par value per share | MNMD | The Nasdaq Stock Market LLC |
Indicate by check mark whether the registrant is an emerging growth company as defined in Rule 405 of the Securities Act of 1933 (§230.405 of this chapter) or Rule 12b-2 of the Securities Exchange Act of 1934 (§240.12b-2 of this chapter).
Emerging growth company ☒
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Item 7.01. Regulation FD Disclosure.
On December 14, 2023, Mind Medicine (MindMed) Inc. (the “Company”) issued a press release announcing positive topline results data from its Phase 2b clinical trial of MM-120 in Generalized Anxiety Disorder, or GAD. A copy of the press release is furnished as Exhibit 99.1 to this Current Report on Form 8-K.
The information furnished under this Item 7.01, including Exhibit 99.1, shall not be deemed “filed” for purposes of Section 18 of the Securities Exchange Act of 1934, or the Exchange Act, or subject to the liabilities of that section or Sections 11 and 12(a)(2) of the Securities Act of 1933, or the Securities Act. The information in this Item 7.01, including Exhibit 99.1, shall not be deemed incorporated by reference into any other filing with the U.S. Securities Exchange Commission, or the SEC, made by the Company, whether made before or after the date hereof, regardless of any general incorporation language in such filing.
Item 8.01 Other Events.
As described in the press release, the Company will host a conference call and webcast to discuss the results of the MM-120 trial at 8:30 a.m. ET on December 14, 2023. A copy of the presentation to be used by the Company during the conference call is filed as Exhibit 99.2 to this Current Report on Form 8-K and is incorporated herein by reference.
| Item 9.01. | Financial Statements and Exhibits. |
(d) Exhibits.
| Exhibit No. |
Description |
|
| 99.1 | Press release, dated December 14, 2023 | |
| 99.2 | Presentation, dated December 14, 2023 | |
| 104 | Cover Page Interactive Data File (embedded within the Inline XBRL document). | |
SIGNATURES
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
| MIND MEDICINE (MINDMED) INC. | ||||||
| By: | /s/ Robert Barrow |
|||||
| Robert Barrow | ||||||
| Chief Executive Officer | ||||||
| Date: December 14, 2023 | ||||||
Exhibit 99.1

MindMed Announces Positive Topline Results from Phase 2b Trial of MM-120
in Generalized Anxiety Disorder
– Trial met its primary endpoint with MM-120 demonstrating a statistically significant dose-dependent improvement in HAM-A scores four weeks after a single-dose –
– MM-120 100 µg demonstrated a clinically and statistically significant HAM-A reduction of 21.3 points, representing a 7.6-point improvement over placebo at Week 4 (p=0.0004, Cohen’s d effect size = 0.88) –
– Clinical response rate of 78% in 100 µg and 200 µg dose groups and 50% clinical remission rate in the 100 µg dose group at Week 4 –
– MM-120 was generally well-tolerated with mostly mild-to-moderate adverse events that occurred on dosing day –
– Company plans to hold an End-of-Phase 2 meeting with the U.S. Food & Drug Administration (FDA) in the first half of 2024 and initiate a Phase 3 clinical program in the second half of 2024 –
– Conference call and webcast to take place today at 8:30 am EST –
NEW YORK, December 14, 2023 — Mind Medicine (MindMed) Inc. (NASDAQ: MNMD), (NEO: MMED), (the “Company” or “MindMed”), a clinical stage biopharmaceutical company developing novel product candidates to treat brain health disorders, today announced positive topline results from its Phase 2b clinical trial of MM-120 (lysergide d-tartrate) in generalized anxiety disorder (GAD). The trial met its primary endpoint, with MM-120 demonstrating statistically significant and clinically meaningful dose-dependent improvements on the Hamilton Anxiety rating scale (HAM-A) compared to placebo at Week 4. MM-120 was administered as a single-dose in a monitored clinical setting with no additional therapeutic intervention.
MM-120 100 µg – the dose achieving the highest level of clinical activity – demonstrated a 7.6-point reduction compared to placebo at Week 4 (-21.3 MM-120 vs. -13.7 placebo; p<0.0004; Cohen’s d=0.88). Clinical Global Impressions—Severity (CGI-S) scores on average improved from 4.8 to 2.4 in the 100 ug dose group, representing a two-category shift from ‘markedly ill’ to ‘borderline’ at Week 4 (p<0.001). This clinical activity was observed to be rapid and durable beginning on Day 2 and continuing through Week 4 with no loss of activity observed on either HAM-A or CGI-S.
“We are excited by the strong positive results for MM-120 in GAD, particularly given that this is the first study to assess the standalone drug effects of MM-120 in the absence of any psychotherapeutic intervention. These promising findings represent a major step forward in our goal to bring a paradigm-shifting treatment to the millions of patients who are profoundly impacted by GAD,” said Robert Barrow, Chief Executive Officer and Director of MindMed.
“We look forward to sharing additional study results in the coming months – including topline 12-week results in the first quarter of 2024 – and working closely with FDA as we finalize the Phase 3 development program for MM-120 in GAD. I would like to thank all of the participants in the study as well as the study investigators and our clinical development team, whose dedication made this important milestone possible.”
Daniel Karlin, MD, MA, Chief Medical Officer of MindMed said, “Generalized anxiety disorder is a common condition associated with significant impairment that adversely affects millions of people and there remains a serious unmet need for this patient population. The pharmaceutical industry has largely ignored GAD over recent decades as it has proved extremely difficult to target. Few new treatment options have shown robust activity in GAD since the last new drug approval in 2004, making the strong, rapid, and durable clinical activity of a single dose of MM-120 observed in the trial particularly notable. We believe this study is the first to rigorously assess the efficacy of a drug candidate in this class in the absence of a concurrent therapeutic intervention, which brings hope to the millions of people suffering from GAD and provides additional evidence that MM-120 may play an important role in revolutionizing the treatment of brain health disorders.”
Additional secondary and exploratory endpoints included in the primary topline results included HAM-A response and remission rates and Clinical Global Impressions—Severity (CGI-S) scores. Clinical response (50% or greater improvement in HAM-A) at Week 4 was achieved in 78% of participants treated with MM-120 (100 µg or 200 µg) compared to 31% for placebo. Clinical remission (HAM-A ≤ 7) at Week 4 was achieved in 50% of participants treated with MM-120 100 µg. CGI-S scores demonstrated a statistically significant and clinically meaningful improvement compared to placebo in the 100 µg (p≤0.001) and 200 µg (p≤0.01) dose groups. On average, participants receiving MM-120 (100 µg or 200 µg) experienced a 2-unit improvement in the CGI-S score at Week 4, with statistically significant improvements observed as early as one day after treatment and continuing at all evaluated timepoints through Week 4.
MM-120 was generally observed to be well tolerated, with mostly transient mild-to-moderate adverse events (AEs) that appear consistent with the pharmacodynamic effects of MM-120. The overall four-week completion rate in the trial was approximately 90% and was 97.5% in the high dose groups, and no participants in the high dose groups discontinued due to an adverse event through Week 4. The most common adverse events (at least 10% incidence in the high dose groups) occurred on dosing day and included illusion, hallucinations, euphoric mood, anxiety, thinking abnormal, headache, paraesthesia, dizziness, tremor, nausea, vomiting, feeling abnormal, mydriasis and hyperhidrosis.
The Company expects that results of this study will support the advancement of MM-120 into Phase 3 clinical development for GAD. The Company plans to hold an End-of-Phase 2 meeting with the FDA in the first half of 2024 and expects to initiate Phase 3 clinical trials in the second half of 2024. The Company expects to present additional topline 12-week data from the study in the first quarter of 2024 and to present full results at a scientific meeting in 2024.
Conference Call and Webcast
MindMed management will host a conference call at 8:30 AM EST today to discuss the results of MM-120 in GAD. Individuals may participate in the live call via telephone by dialing (877) 407-3982 (domestic) or (201) 493-6780 (international). The webcast can be accessed live here on the News & Events page in the Investors section of the MindMed website, https://mindmed.co/. The webcast will be archived on the Company’s website for at least 30 days after the conference call.
About Study MMED008
Study MMED008 is a multi-center, parallel, randomized, double-blind, placebo-controlled, dose-optimization study. The trial enrolled 198 participants who were randomized to receive a single administration of MM-120 at a dose of 25, 50, 100 or 200 µg or placebo. The full analysis set (FAS) for the trial included 194 subjects, those that had at least one valid post-baseline Hamilton Anxiety rating scale (HAM-A) score. Subjects enrolled in the trial presented with severe GAD symptoms (average baseline HAM-A scores of approximately 30). The primary objective of the study was to determine the dose-response relationship of four doses of MM-120 versus placebo as measured by the change in HAM-A from Baseline to Week 4. Secondary objectives, measured up to 12 weeks after the single administration, include assessments of anxiety symptoms, safety and tolerability, as well as other measures of efficacy and quality of life. More information about the trial is available on the MindMed website (mindmed.co) or on clinicaltrials.gov (identifier NCT05407064).
About MM-120
Lysergide is a synthetic tryptamine belonging to the group of classic, or serotonergic, psychedelics, which acts as a partial agonist at human serotonin-2A (5-hydroxytryptamine-2A [5-HT2A]) receptors. MindMed is developing MM-120 (lysergide D-tartrate), the tartrate salt form of lysergide, for GAD and ADHD.
About Generalized Anxiety Disorder
GAD is a brain health disorder that results in fear, persistent anxiety and a constant feeling of being overwhelmed. It is characterized by excessive, persistent, and unrealistic worry about everyday things. Approximately 10% of U.S. adults, representing around 20 million people, currently suffer from GAD, an underdiagnosed and underserved indication that is associated with significant impairment, less accomplishment at work and reduced labor force participation. Despite the significant personal and societal burden of GAD, there has been little innovation in the treatment of GAD in the past several decades, with the last new drug approval occurring in 2004.
About MindMed
MindMed is a clinical stage biopharmaceutical company developing novel product candidates to treat brain health disorders. Our mission is to be the global leader in the development and delivery of treatments that unlock new opportunities to improve patient outcomes. We are developing a pipeline of innovative product candidates, with and without acute perceptual effects, targeting neurotransmitter pathways that play key roles in brain health disorders.
MindMed trades on NASDAQ under the symbol MNMD and on the Cboe Canada (formerly known as the NEO Exchange, Inc.) under the symbol MMED.
Forward-Looking Statements
Certain statements in this news release related to the Company constitute “forward-looking information” within the meaning of applicable securities laws and are prospective in nature. Forward-looking information is not based on historical facts, but rather on current expectations and projections about future events and are therefore subject to risks and uncertainties which could cause actual results to differ materially from the future results expressed or implied by the forward-looking statements.
These statements generally can be identified by the use of forward-looking words such as “will”, “may”, “should”, “could”, “intend”, “estimate”, “plan”, “anticipate”, “expect”, “believe”, “potential” or “continue”, or the negative thereof or similar variations. Forward-looking information in this news release includes, but is not limited to, statements regarding anticipated upcoming milestones, and progress of trials and studies; results and timing of and reporting of full data from the Company’s Phase 2b clinical trial of MM-120; timing of a potential End-of-Phase-2 meeting with the FDA; timing of the initiation of a potential Phase 3 clinical trial of MM-120; and the potential benefits of the Company’s product candidates. There are numerous risks and uncertainties that could cause actual results and the Company’s plans and objectives to differ materially from those expressed in the forward-looking information, including history of negative cash flows; limited operating history; incurrence of future losses; availability of additional capital; lack of product revenue; compliance with laws and regulations; difficulty associated with research and development; risks associated with clinical trials or studies; heightened regulatory scrutiny; early stage product development; clinical trial risks; regulatory approval processes; novelty of the psychedelic inspired medicines industry; as well as those risk factors discussed or referred to herein and the risks described in the Company’s Annual Report on Form 10-K for the fiscal year ended December 31, 2022, the Company’s Quarterly Reports on Form 10-Q for the periods ended March 31, 2023, June 30, 2023 and September 30, 2023, under headings such as “Special Note Regarding Forward-Looking Statements,” “Risk Factors” and “Management’s Discussion and Analysis of Financial Condition and Results of Operations,” and other filings and furnishings made by the Company with the securities regulatory authorities in all provinces and territories of Canada which are available under the Company’s profile on SEDAR at www.sedar.com and with the U.S. Securities and Exchange Commission on EDGAR at www.sec.gov. Except as required by law, the Company undertakes no duty or obligation to update any forward-looking statements contained in this release as a result of new information, future events, changes in expectations or otherwise.
For Media & Investor Inquiries, please contact:
Maxim Jacobs, CFA
Vice President, Investor Relations and Corporate Communications
Mind Medicine (MindMed) Inc.
ir@mindmed.co
media@mindmed.co

Exhibit 99.2 MM-120 for Generalized Anxiety Disorder (GAD) Phase 2b Topline Data December 2023
Disclaimer This presentation (the “Presentation”) has been prepared by Mind Medicine (MindMed) Inc. (“MindMed” or the “Company”) solely for informational purposes. Any trademarks included herein are the property of the owners thereof and are used for reference purposes only. Such use should not be construed as an endorsement of the products or services of MindMed. Cautionary Note Regarding Forward-Looking Statements This Presentation contains, and our officers and representatives may from time to time make, “forward-looking statements” within the meaning of the safe harbor provisions of the U.S. Private Securities Litigation Reform Act of 1995 and other applicable securities laws. Forward-looking statements can often, but not always, be identified by words such as “plans”, “expects”, “is expected”, “budget”, “scheduled”, “estimates”, “forecasts”, “intends”, “anticipates”, will”, “projects”, or “believes” or variations (including negative variations) of such words and phrases, or statements that certain actions, events, results or conditions “may”, “could”, “would”, “might” or “will” be taken, occur or be achieved, and similar references to future periods. Except for statements of historical fact, examples of forward-looking statements include, among others, statements pertaining to: the anticipated timing and results of the Company’s 12-week data for their MM-120 Phase 2b study in Generalized Anxiety Disorder (“GAD”), the safety or efficacy of MM-120 in GAD or any other indications, expectations regarding a Phase 3 trial for MM-120, the development and commercialization of any product candidate or treatment, or the safety or efficacy of either of the foregoing, the success and timing of our development activities; the success and timing of our planned clinical trials; our ability to meet the milestones set forth herein; the likelihood of success of any clinical trials or of obtaining FDA or other regulatory approvals; the likelihood of obtaining patents or the efficacy of such patents once granted and the potential for the markets that MindMed is anticipating to access. Forward-looking statements are neither historical facts nor assurances of future performance. Instead, they are based only on our current beliefs, expectations and assumptions regarding the future of our business, future plans and strategies, projections, anticipated events and trends, the economy and other future conditions as of the date of this Presentation. While MindMed considers these assumptions to be reasonable, the assumptions are inherently subject to significant business, social, economic, political, regulatory, competitive and other risks and uncertainties that are difficult to predict and many of which are outside of MindMed’s control, and actual results and financial condition may differ materially from those indicated in the forward-looking statements. Therefore, you should not rely on any of these forward-looking statements. Important factors that could cause actual results and financial condition to differ materially from those indicated in the forward-looking statements include, among others, the following: MindMed’s ability to raise capital to complete its plans and fund its studies; the medical and commercial viability of the contemplated medicines and treatments being developed; MindMed’s history of negative cash flows; MindMed’s limited operating history; incurrence of future losses; lack of revenue; compliance with laws and regulations; difficulty associated with research and development; risks associated with clinical trials or studies; heightened regulatory scrutiny in connection with a controlled substance in approval processes; early stage product development; clinical trial risks; regulatory approval processes; novelty of the psychedelic inspired medicines industry; as well as those risk factors discussed or referred to throughout the “Risk Factors” sections of MindMed’s most recently filed Annual Report on Form 10-K filed with the Securities and Exchange Commission (“SEC”), Quarterly Report on Form 10-Q for the periods ended September 30, 2023 filed with the SEC and in other filings we make in the future with the SEC and the securities regulatory authorities in all provinces and territories of Canada, available under the Company’s profile on SEDAR at www.sedar.com. Any forward-looking statement made by MindMed in this Presentation is based only on information currently available to the Company and speaks only as of the date on which it is made. MindMed undertakes no obligation to publicly update any forward-looking statement, whether written or oral, that may be made from time to time, whether as a result of new information, future developments or otherwise. Cautionary Note Regarding Regulatory Matters The United States federal government regulates drugs through the Controlled Substances Act. MM-120 is a proprietary, pharmaceutically optimized form of lysergide D-tartrate. Lysergide is a Schedule I substance under the Controlled Substances Act. While the Company is focused on programs using psychedelic or hallucinogenic compounds and non-hallucinogenic derivatives of these compounds, including in its MM-120 and MM-402 product candidates, the Company does not have any direct or indirect involvement with the illegal selling, production or distribution of any substances in the jurisdictions in which it operates. The Company is a neuro-pharmaceutical drug development company and does not deal with psychedelic or hallucinogenic substances except within laboratory and clinical trial settings conducted within approved regulatory frameworks. The Company’s products will not be commercialized prior to applicable regulatory approval, which will only be granted if clinical evidence of safety and efficacy for the intended uses is successfully developed. Market and Industry Data This Presentation includes market and industry data that has been obtained from third-party sources, including industry publications. MindMed believes that the industry data is accurate and that the estimates and assumptions are reasonable, but there is no assurance as to the accuracy or completeness of this data. Third party sources generally state that the information contained therein has been obtained from sources believed to be reliable, but there is no assurance as to the accuracy or completeness of included information. Although the data is believed to be reliable, MindMed has not independently verified any of the data from third party sources referred to in this Presentation or ascertained the underlying economic assumptions relied upon by such sources. References in this Presentation to research reports or to articles and publications should be not construed as depicting the complete findings of the entire referenced report or article. MindMed does not make any representation as to the accuracy of such information. December 2023 2 Topline Data from Study MMED008
Today’s Agenda Speaker Topic Introduction Schond Greenway - Chief Financial Officer Summary of Phase 2b GAD Trial Results Rob Barrow - Chief Executive Officer Phase 2b GAD Trial Results Analysis Dan Karlin, MD - Chief Medical Officer MM-120 Development Plan Rob Barrow - Chief Executive Officer Summary and Closing Remarks Questions & Answers Rob Barrow - Chief Executive Officer Dan Karlin, MD - Chief Medical Officer Miri Halperin Wernli, PhD - Executive President Francois Lilienthal, MD - Chief Commercial Officer Schond Greenway - Chief Financial Officer December 2023 3 Topline Data from Study MMED008
MM-120 Summary of Phase 2b LSD D-tartrate GAD Trial Results for Generalized Anxiety Disorder (GAD) December 2023 4 Topline Data from Study MMED008
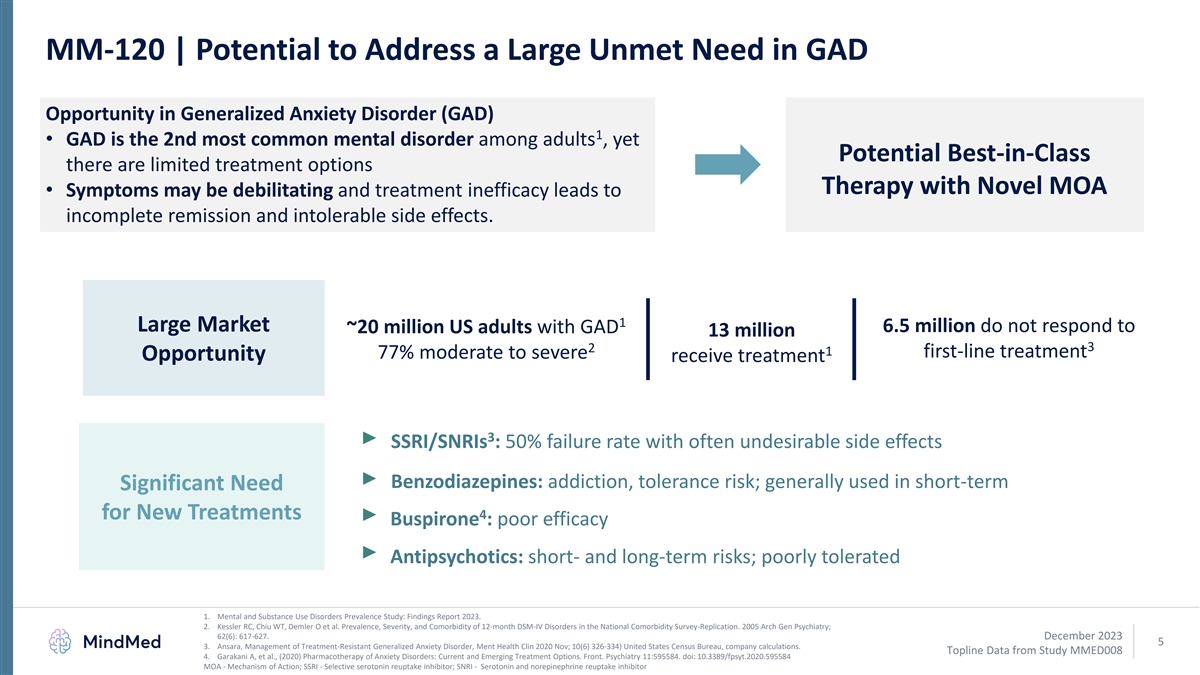
MM-120 | Potential to Address a Large Unmet Need in GAD Opportunity in Generalized Anxiety Disorder (GAD) 1 • GAD is the 2nd most common mental disorder among adults , yet Potential Best-in-Class there are limited treatment options Therapy with Novel MOA • Symptoms may be debilitating and treatment inefficacy leads to incomplete remission and intolerable side effects. 1 Large Market 6.5 million do not respond to ~20 million US adults with GAD 13 million 3 2 1 first-line treatment 77% moderate to severe Opportunity receive treatment 3 SSRI/SNRIs : 50% failure rate with often undesirable side effects Benzodiazepines: addiction, tolerance risk; generally used in short-term Significant Need 4 for New Treatments Buspirone : poor efficacy Antipsychotics: short- and long-term risks; poorly tolerated 1. Mental and Substance Use Disorders Prevalence Study: Findings Report 2023. 2. Kessler RC, Chiu WT, Demler O et al. Prevalence, Severity, and Comorbidity of 12-month DSM-IV Disorders in the National Comorbidity Survey-Replication. 2005 Arch Gen Psychiatry; 62(6): 617-627. December 2023 5 3. Ansara, Management of Treatment-Resistant Generalized Anxiety Disorder, Ment Health Clin 2020 Nov; 10(6) 326-334) United States Census Bureau, company calculations. Topline Data from Study MMED008 4. Garakani A, et al., (2020) Pharmacotherapy of Anxiety Disorders: Current and Emerging Treatment Options. Front. Psychiatry 11:595584. doi: 10.3389/fpsyt.2020.595584 MOA - Mechanism of Action; SSRI - Selective serotonin reuptake inhibitor; SNRI - Serotonin and norepinephrine reuptake inhibitor
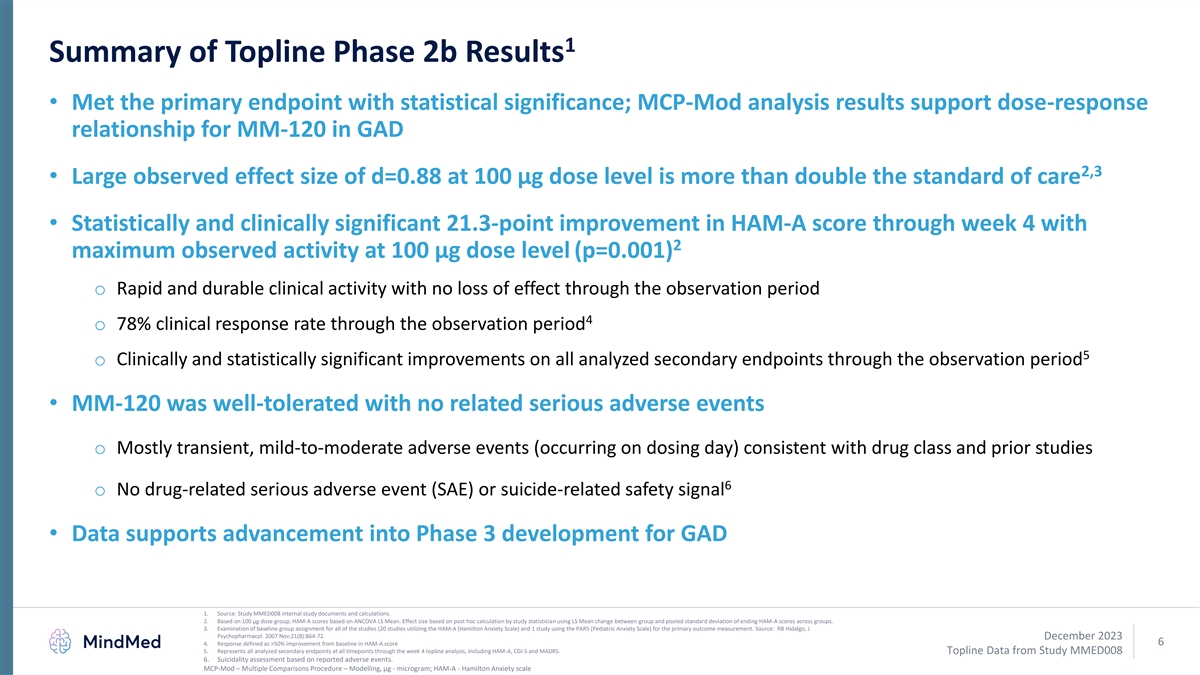
1 Summary of Topline Phase 2b Results • Met the primary endpoint with statistical significance; MCP-Mod analysis results support dose-response relationship for MM-120 in GAD 2,3 • Large observed effect size of d=0.88 at 100 µg dose level is more than double the standard of care • Statistically and clinically significant 21.3-point improvement in HAM-A score through week 4 with 2 maximum observed activity at 100 µg dose level (p=0.001) o Rapid and durable clinical activity with no loss of effect through the observation period 4 o 78% clinical response rate through the observation period 5 o Clinically and statistically significant improvements on all analyzed secondary endpoints through the observation period • MM-120 was well-tolerated with no related serious adverse events o Mostly transient, mild-to-moderate adverse events (occurring on dosing day) consistent with drug class and prior studies 6 o No drug-related serious adverse event (SAE) or suicide-related safety signal • Data supports advancement into Phase 3 development for GAD 1. Source: Study MMED008 internal study documents and calculations. 2. Based on 100 µg dose group; HAM-A scores based on ANCOVA LS Mean. Effect size based on post hoc calculation by study statistician using LS Mean change between group and pooled standard deviation of ending HAM-A scores across groups. 3. Examination of baseline group assignment for all of the studies (20 studies utilizing the HAM-A (Hamilton Anxiety Scale) and 1 study using the PARS (Pediatric Anxiety Scale) for the primary outcome measurement. Source: RB Hidalgo, J Psychopharmacol. 2007 Nov;21(8):864-72. December 2023 6 4. Response defined as >50% improvement from baseline in HAM-A score 5. Represents all analyzed secondary endpoints at all timepoints through the week 4 topline analysis, including HAM-A, CGI-S and MADRS. Topline Data from Study MMED008 6. Suicidality assessment based on reported adverse events. MCP-Mod – Multiple Comparisons Procedure – Modelling, μg - microgram; HAM-A - Hamilton Anxiety scale
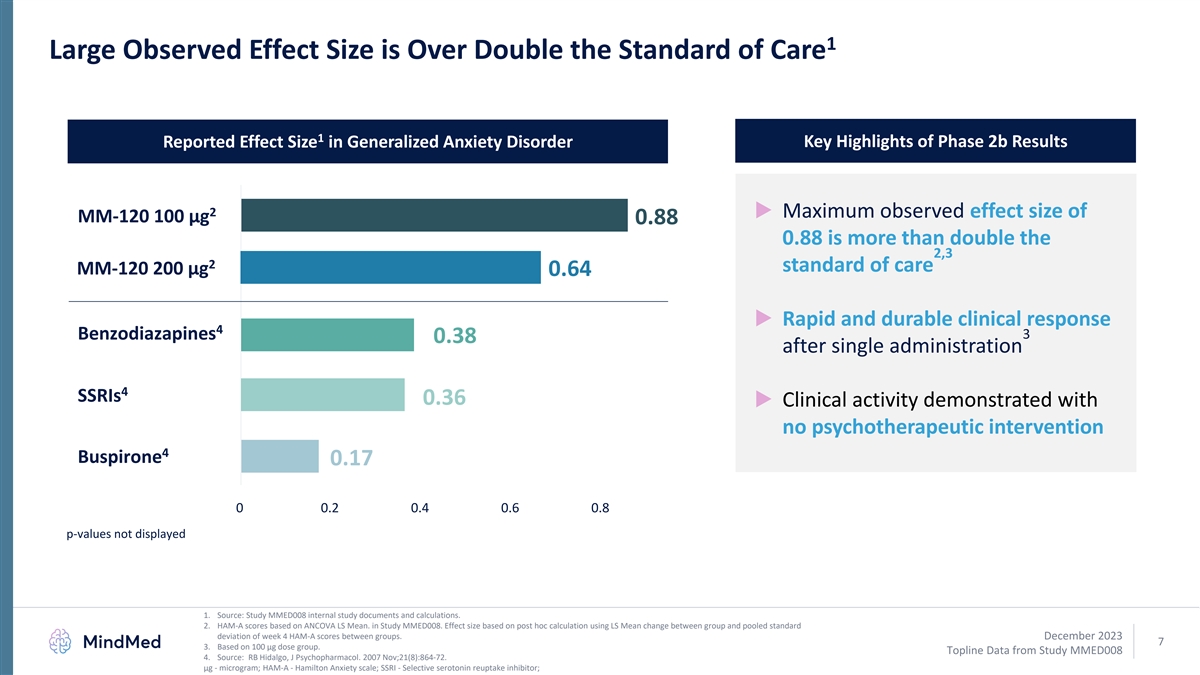
1 Large Observed Effect Size is Over Double the Standard of Care 1 Reported Effect Size in Generalized Anxiety Disorder Key Highlights of Phase 2b Results 2 ▶ Maximum observed effect size of MM-120 100 µg 0.88 0.88 is more than double the 2,3 2 standard of care MM-120 200 µg 0.64 ▶ Rapid and durable clinical response 4 3 Benzodiazapines 0.38 after single administration 4 SSRIs 0.36 ▶ Clinical activity demonstrated with no psychotherapeutic intervention 4 Buspirone 0.17 0 0.2 0.4 0.6 0.8 p-values not displayed 1. Source: Study MMED008 internal study documents and calculations. 2. HAM-A scores based on ANCOVA LS Mean. in Study MMED008. Effect size based on post hoc calculation using LS Mean change between group and pooled standard deviation of week 4 HAM-A scores between groups. December 2023 7 3. Based on 100 µg dose group. Topline Data from Study MMED008 4. Source: RB Hidalgo, J Psychopharmacol. 2007 Nov;21(8):864-72. μg - microgram; HAM-A - Hamilton Anxiety scale; SSRI - Selective serotonin reuptake inhibitor;
MM-120 Phase 2b GAD Trial LSD D-tartrate Key Design Elements for Generalized Anxiety Disorder (GAD) December 2023 8 Topline Data from Study MMED008
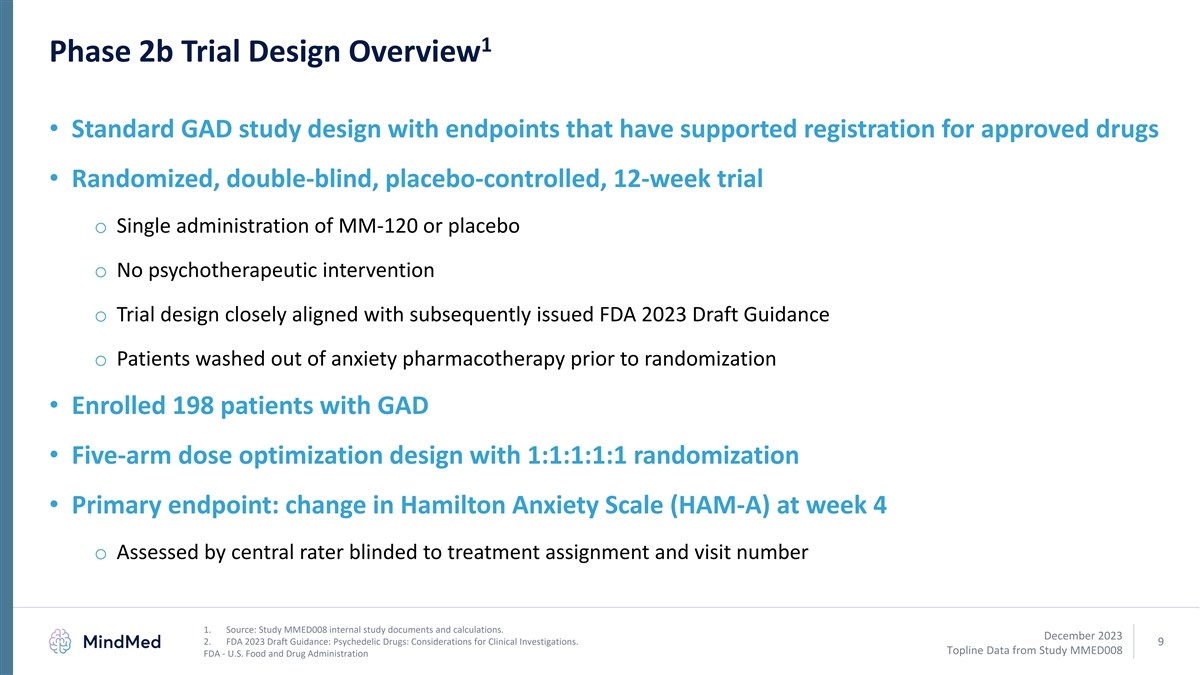
1 Phase 2b Trial Design Overview • Standard GAD study design with endpoints that have supported registration for approved drugs • Randomized, double-blind, placebo-controlled, 12-week trial o Single administration of MM-120 or placebo o No psychotherapeutic intervention o Trial design closely aligned with subsequently issued FDA 2023 Draft Guidance o Patients washed out of anxiety pharmacotherapy prior to randomization • Enrolled 198 patients with GAD • Five-arm dose optimization design with 1:1:1:1:1 randomization • Primary endpoint: change in Hamilton Anxiety Scale (HAM-A) at week 4 o Assessed by central rater blinded to treatment assignment and visit number 1. Source: Study MMED008 internal study documents and calculations. December 2023 2. FDA 2023 Draft Guidance: Psychedelic Drugs: Considerations for Clinical Investigations. 9 Topline Data from Study MMED008 FDA - U.S. Food and Drug Administration
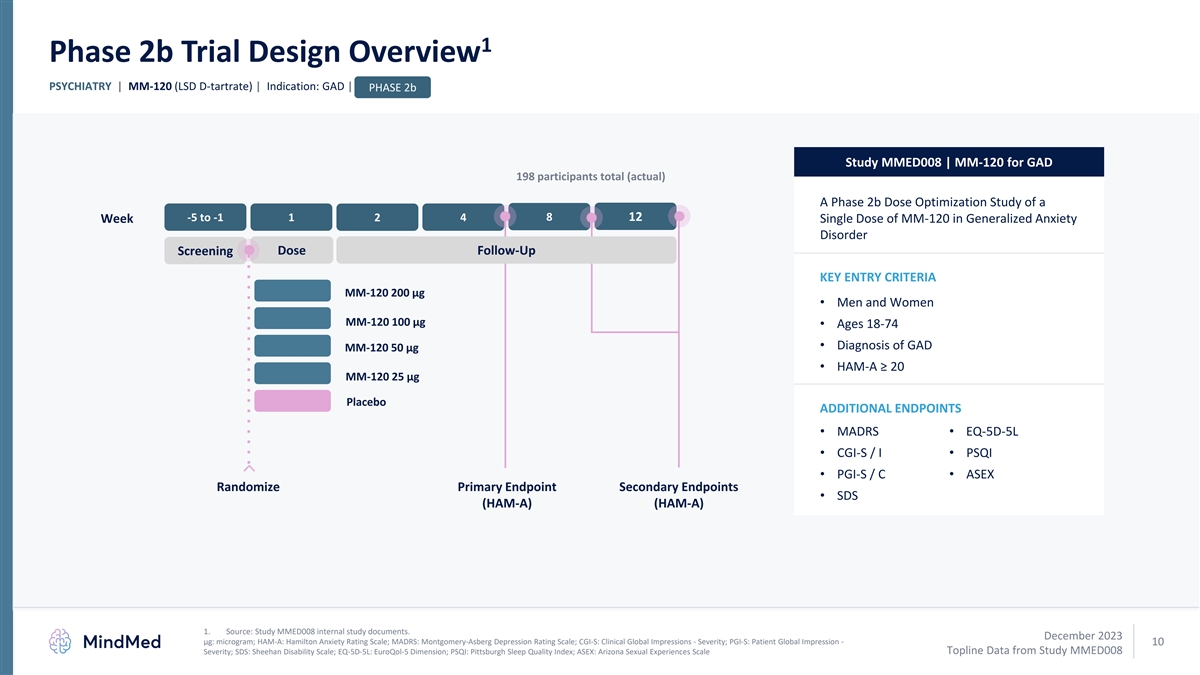
1 Phase 2b Trial Design Overview PSYCHIATRY | MM-120 (LSD D-tartrate) | Indication: GAD | PHASE 2b Study MMED008 | MM-120 for GAD 198 participants total (actual) A Phase 2b Dose Optimization Study of a -5 to -1 1 2 4 8 12 Week Single Dose of MM-120 in Generalized Anxiety Disorder Screening Dose Follow-Up KEY ENTRY CRITERIA MM-120 200 µg • Men and Women MM-120 100 µg • Ages 18-74 • Diagnosis of GAD MM-120 50 µg • HAM-A ≥ 20 MM-120 25 µg Placebo ADDITIONAL ENDPOINTS • MADRS• EQ-5D-5L • CGI-S / I• PSQI • PGI-S / C• ASEX Randomize Primary Endpoint Secondary Endpoints • SDS (HAM-A) (HAM-A) 1. Source: Study MMED008 internal study documents. December 2023 μg: microgram; HAM-A: Hamilton Anxiety Rating Scale; MADRS: Montgomery-Asberg Depression Rating Scale; CGI-S: Clinical Global Impressions - Severity; PGI-S: Patient Global Impression - 10 Topline Data from Study MMED008 Severity; SDS: Sheehan Disability Scale; EQ-5D-5L: EuroQol-5 Dimension; PSQI: Pittsburgh Sleep Quality Index; ASEX: Arizona Sexual Experiences Scale
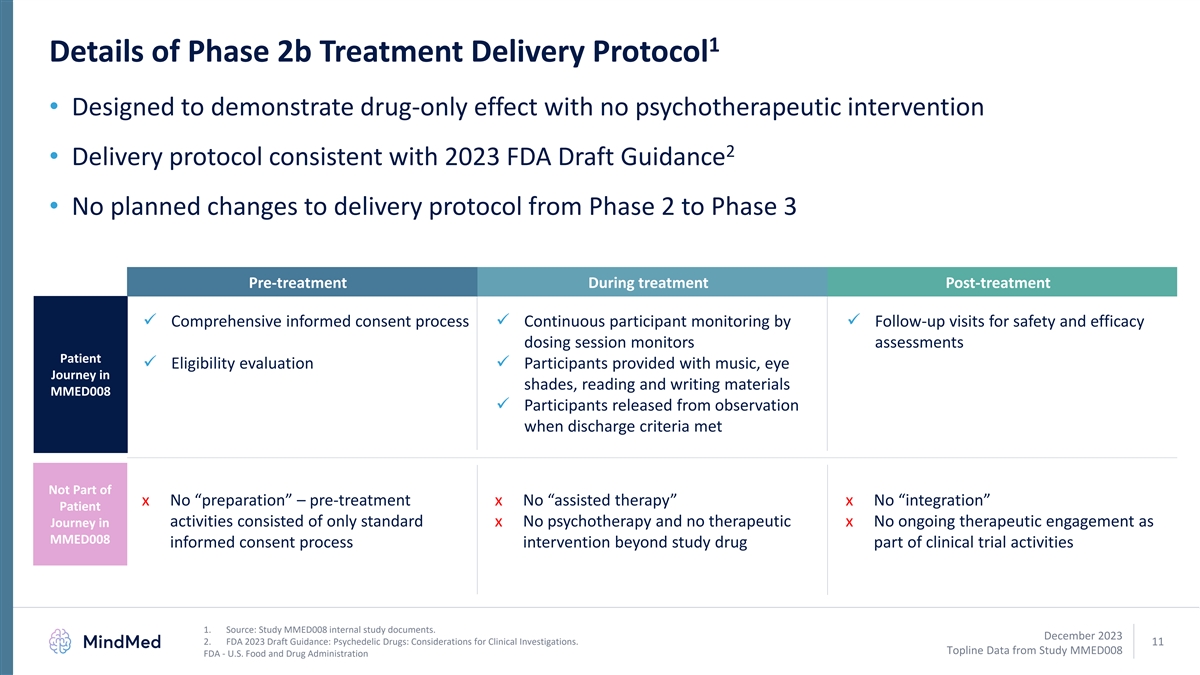
1 Details of Phase 2b Treatment Delivery Protocol • Designed to demonstrate drug-only effect with no psychotherapeutic intervention 2 • Delivery protocol consistent with 2023 FDA Draft Guidance • No planned changes to delivery protocol from Phase 2 to Phase 3 Pre-treatment During treatment Post-treatment ✓ Comprehensive informed consent process✓ Continuous participant monitoring by ✓ Follow-up visits for safety and efficacy dosing session monitors assessments Patient ✓ Eligibility evaluation✓ Participants provided with music, eye Journey in shades, reading and writing materials MMED008 ✓ Participants released from observation when discharge criteria met Not Part of x No “preparation” – pre-treatment x No “assisted therapy” x No “integration” Patient activities consisted of only standard x No psychotherapy and no therapeutic x No ongoing therapeutic engagement as Journey in MMED008 informed consent process intervention beyond study drug part of clinical trial activities 1. Source: Study MMED008 internal study documents. December 2023 2. FDA 2023 Draft Guidance: Psychedelic Drugs: Considerations for Clinical Investigations. 11 Topline Data from Study MMED008 FDA - U.S. Food and Drug Administration
MM-120 Phase 2b GAD Trial LSD D-tartrate Results Analysis for Generalized Anxiety Disorder (GAD) December 2023 12 Topline Data from Study MMED008
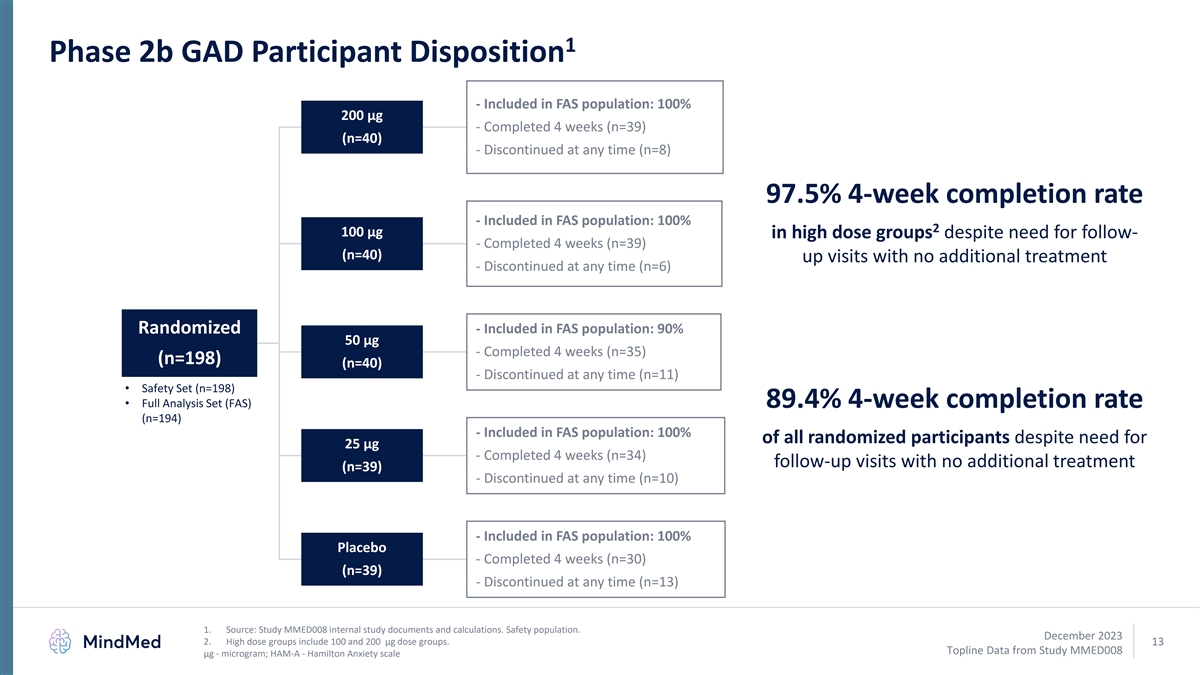
1 Phase 2b GAD Participant Disposition - Included in FAS population: 100% 200 µg - Completed 4 weeks (n=39) (n=40) - Discontinued at any time (n=8) 97.5% 4-week completion rate - Included in FAS population: 100% 2 100 µg in high dose groups despite need for follow- - Completed 4 weeks (n=39) (n=40) up visits with no additional treatment - Discontinued at any time (n=6) Randomized - Included in FAS population: 90% 50 µg - Completed 4 weeks (n=35) (n=198) (n=40) - Discontinued at any time (n=11) • Safety Set (n=198) • Full Analysis Set (FAS) 89.4% 4-week completion rate (n=194) - Included in FAS population: 100% of all randomized participants despite need for 25 µg - Completed 4 weeks (n=34) follow-up visits with no additional treatment (n=39) - Discontinued at any time (n=10) - Included in FAS population: 100% Placebo - Completed 4 weeks (n=30) (n=39) - Discontinued at any time (n=13) 1. Source: Study MMED008 internal study documents and calculations. Safety population. December 2023 2. High dose groups include 100 and 200 µg dose groups. 13 Topline Data from Study MMED008 μg - microgram; HAM-A - Hamilton Anxiety scale
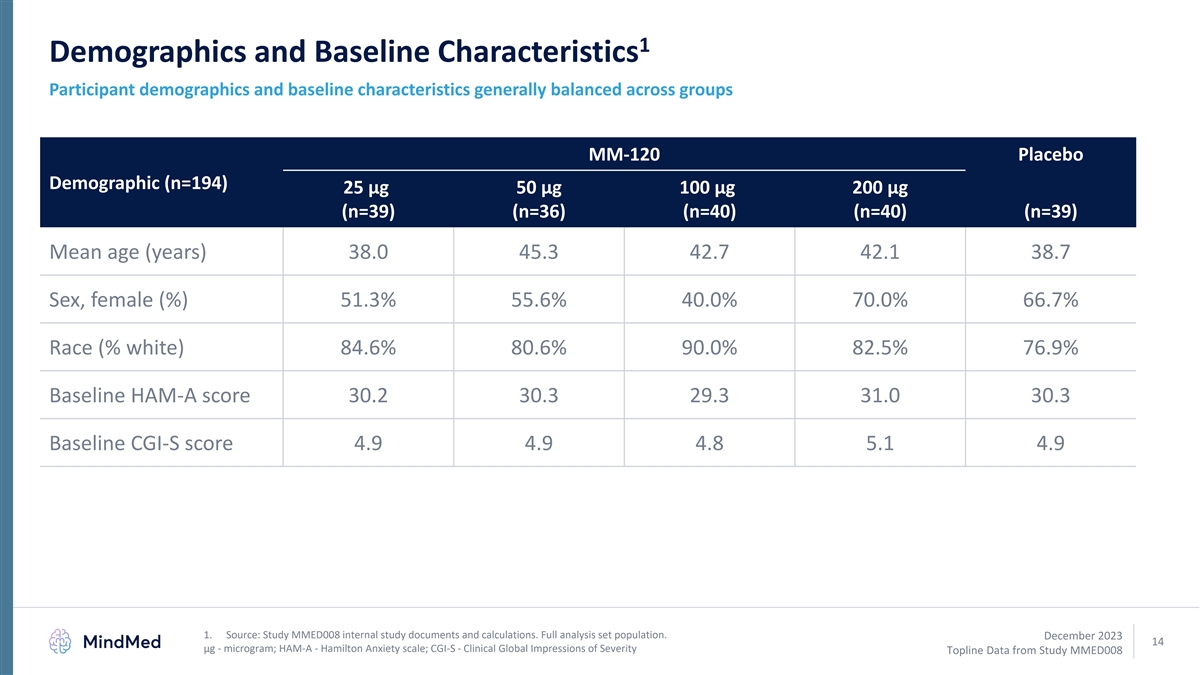
1 Demographics and Baseline Characteristics Participant demographics and baseline characteristics generally balanced across groups MM-120 Placebo Demographic (n=194) 25 µg 50 µg 100 µg 200 µg (n=39) (n=36) (n=40) (n=40) (n=39) Mean age (years) 38.0 45.3 42.7 42.1 38.7 Sex, female (%) 51.3% 55.6% 40.0% 70.0% 66.7% Race (% white) 84.6% 80.6% 90.0% 82.5% 76.9% Baseline HAM-A score 30.2 30.3 29.3 31.0 30.3 Baseline CGI-S score 4.9 4.9 4.8 5.1 4.9 1. Source: Study MMED008 internal study documents and calculations. Full analysis set population. December 2023 14 μg - microgram; HAM-A - Hamilton Anxiety scale; CGI-S - Clinical Global Impressions of Severity Topline Data from Study MMED008
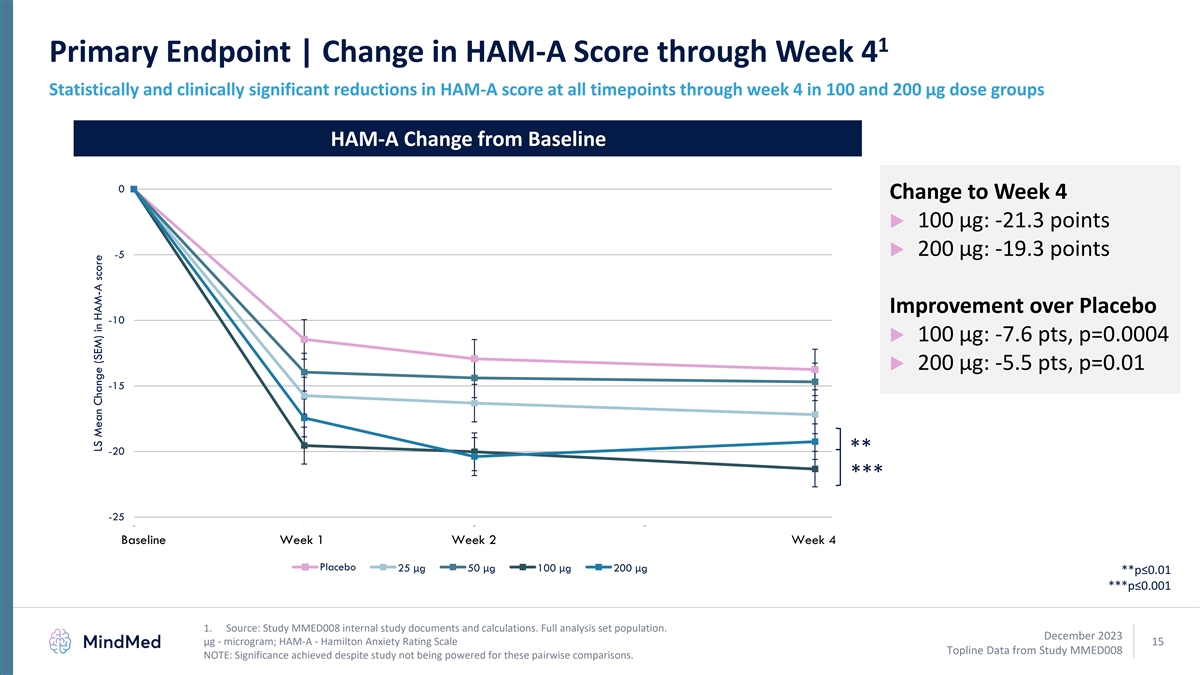
1 Primary Endpoint | Change in HAM-A Score through Week 4 Statistically and clinically significant reductions in HAM-A score at all timepoints through week 4 in 100 and 200 µg dose groups HAM-A Change from Baseline 0 Change to Week 4 ▶ 100 µg: -21.3 points ▶ 200 µg: -19.3 points -5 Improvement over Placebo -10 ▶ 100 µg: -7.6 pts, p=0.0004 ▶ 200 µg: -5.5 pts, p=0.01 -15 ** -20 *** -25 0 1 2 3 4 Baseline Week 1 Week 2 Week 4 Placebo 25 μg 50 μg 100 μg 200 μg **p≤0.01 ***p≤0.001 1. Source: Study MMED008 internal study documents and calculations. Full analysis set population. December 2023 µg - microgram; HAM-A - Hamilton Anxiety Rating Scale 15 Topline Data from Study MMED008 NOTE: Significance achieved despite study not being powered for these pairwise comparisons. LS Mean Change (SEM) in HAM-A score
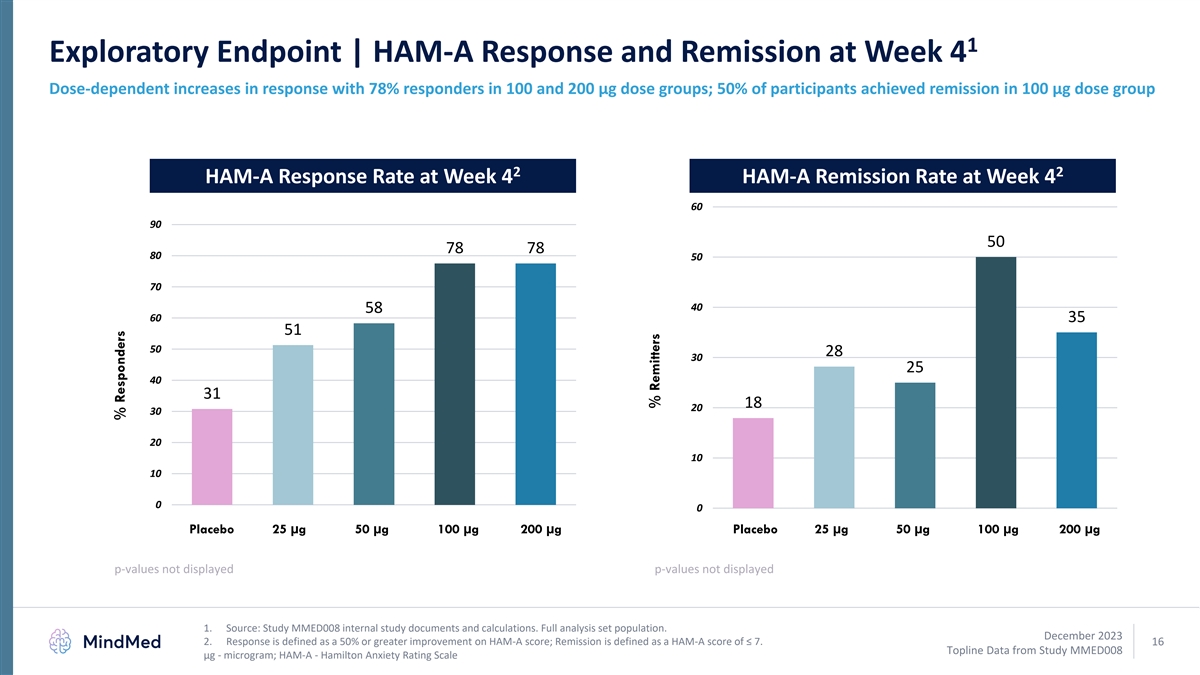
1 Exploratory Endpoint | HAM-A Response and Remission at Week 4 Dose-dependent increases in response with 78% responders in 100 and 200 µg dose groups; 50% of participants achieved remission in 100 µg dose group 2 2 HAM-A Response Rate at Week 4 HAM-A Remission Rate at Week 4 60 90 50 78 78 80 50 70 40 58 60 35 51 50 28 30 25 40 31 18 20 30 20 10 10 0 0 Placebo 25 µg 50 µg 100 µg 200 µg Placebo 25 µg 50 µg 100 µg 200 µg p-values not displayed p-values not displayed 1. Source: Study MMED008 internal study documents and calculations. Full analysis set population. December 2023 2. Response is defined as a 50% or greater improvement on HAM-A score; Remission is defined as a HAM-A score of ≤ 7. 16 Topline Data from Study MMED008 µg - microgram; HAM-A - Hamilton Anxiety Rating Scale % Responders % Remitters
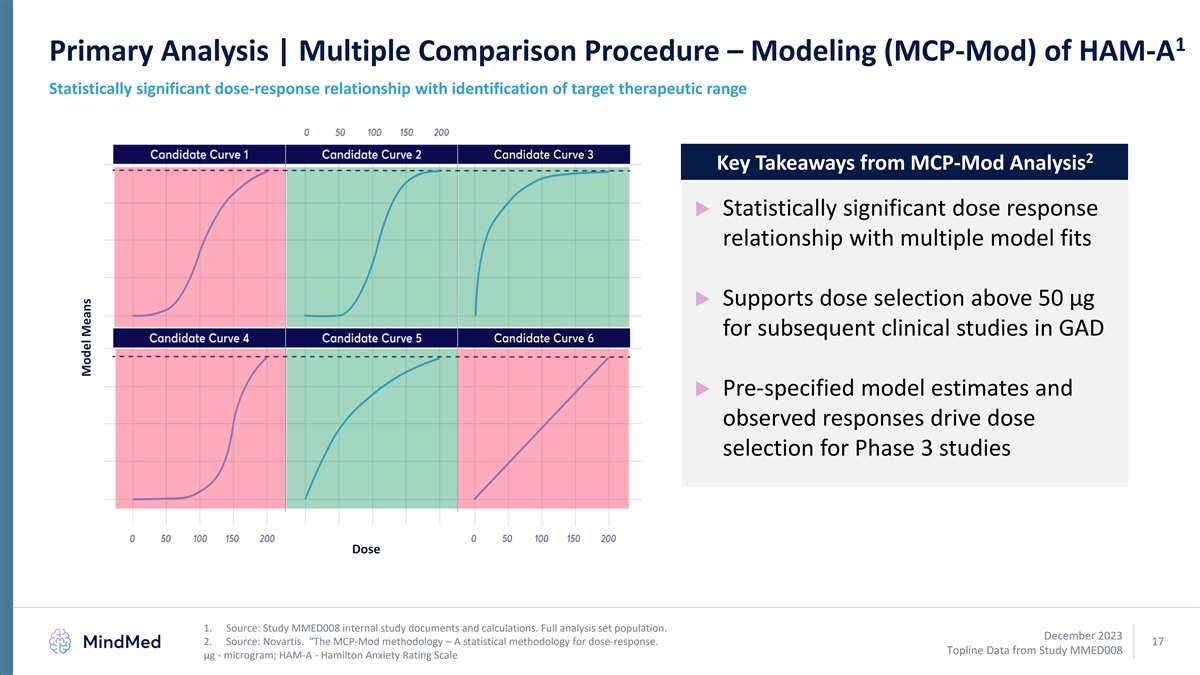
1 Primary Analysis | Multiple Comparison Procedure – Modeling (MCP-Mod) of HAM-A Statistically significant dose-response relationship with identification of target therapeutic range 2 Key Takeaways from MCP-Mod Analysis ▶ Statistically significant dose response relationship with multiple model fits ▶ Supports dose selection above 50 µg for subsequent clinical studies in GAD ▶ Pre-specified model estimates and observed responses drive dose selection for Phase 3 studies Dose 1. Source: Study MMED008 internal study documents and calculations. Full analysis set population. December 2023 2. Source: Novartis. “The MCP-Mod methodology – A statistical methodology for dose-response. 17 Topline Data from Study MMED008 µg - microgram; HAM-A - Hamilton Anxiety Rating Scale Model Means
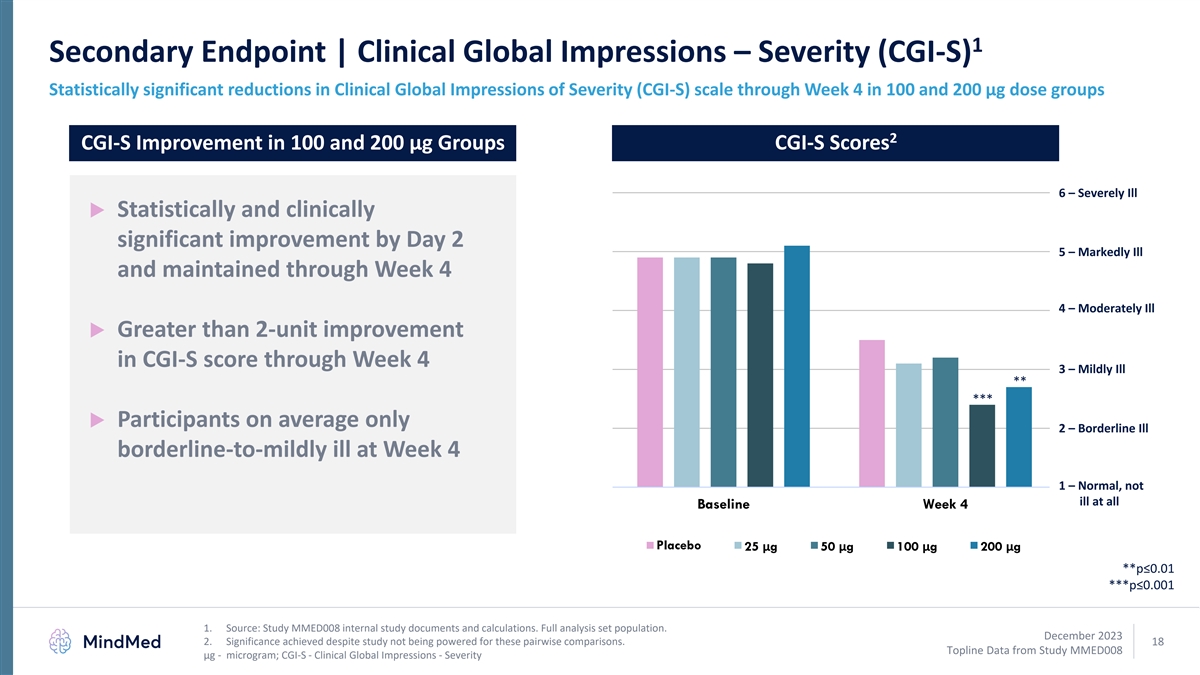
1 Secondary Endpoint | Clinical Global Impressions – Severity (CGI-S) Statistically significant reductions in Clinical Global Impressions of Severity (CGI-S) scale through Week 4 in 100 and 200 µg dose groups 2 CGI-S Improvement in 100 and 200 µg Groups CGI-S Scores 6 – Severely Ill ▶ Statistically and clinically significant improvement by Day 2 5 – Markedly Ill and maintained through Week 4 4 – Moderately Ill ▶ Greater than 2-unit improvement in CGI-S score through Week 4 3 – Mildly Ill ** *** ▶ Participants on average only 2 – Borderline Ill borderline-to-mildly ill at Week 4 1 – Normal, not ill at all Baseline Week 4 Placebo 25 μg 50 μg 100 μg 200 μg **p≤0.01 ***p≤0.001 1. Source: Study MMED008 internal study documents and calculations. Full analysis set population. December 2023 2. Significance achieved despite study not being powered for these pairwise comparisons. 18 Topline Data from Study MMED008 µg - microgram; CGI-S - Clinical Global Impressions - Severity
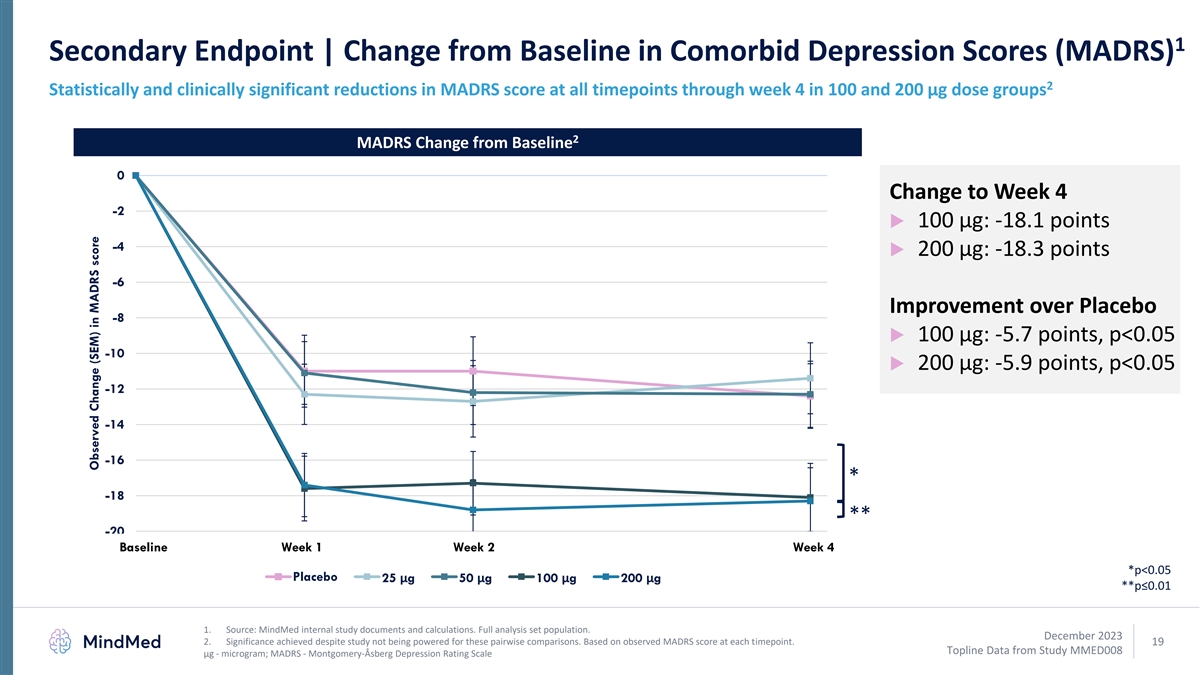
1 Secondary Endpoint | Change from Baseline in Comorbid Depression Scores (MADRS) 2 Statistically and clinically significant reductions in MADRS score at all timepoints through week 4 in 100 and 200 µg dose groups 2 MADRS Change from Baseline 0 Change to Week 4 -2 ▶ 100 µg: -18.1 points -4 ▶ 200 µg: -18.3 points -6 Improvement over Placebo -8 ▶ 100 µg: -5.7 points, p<0.05 -10 ▶ 200 µg: -5.9 points, p<0.05 -12 -14 -16 * -18 ** -20 Base 0 line Wee 1k 1 Wee 2k 2 3 Wee 4 k 4 *p<0.05 Placebo 25 μg 50 μg 100 μg 200 μg **p≤0.01 1. Source: MindMed internal study documents and calculations. Full analysis set population. December 2023 2. Significance achieved despite study not being powered for these pairwise comparisons. Based on observed MADRS score at each timepoint. 19 Topline Data from Study MMED008 µg - microgram; MADRS - Montgomery-Åsberg Depression Rating Scale Observed Change (SEM) in MADRS score
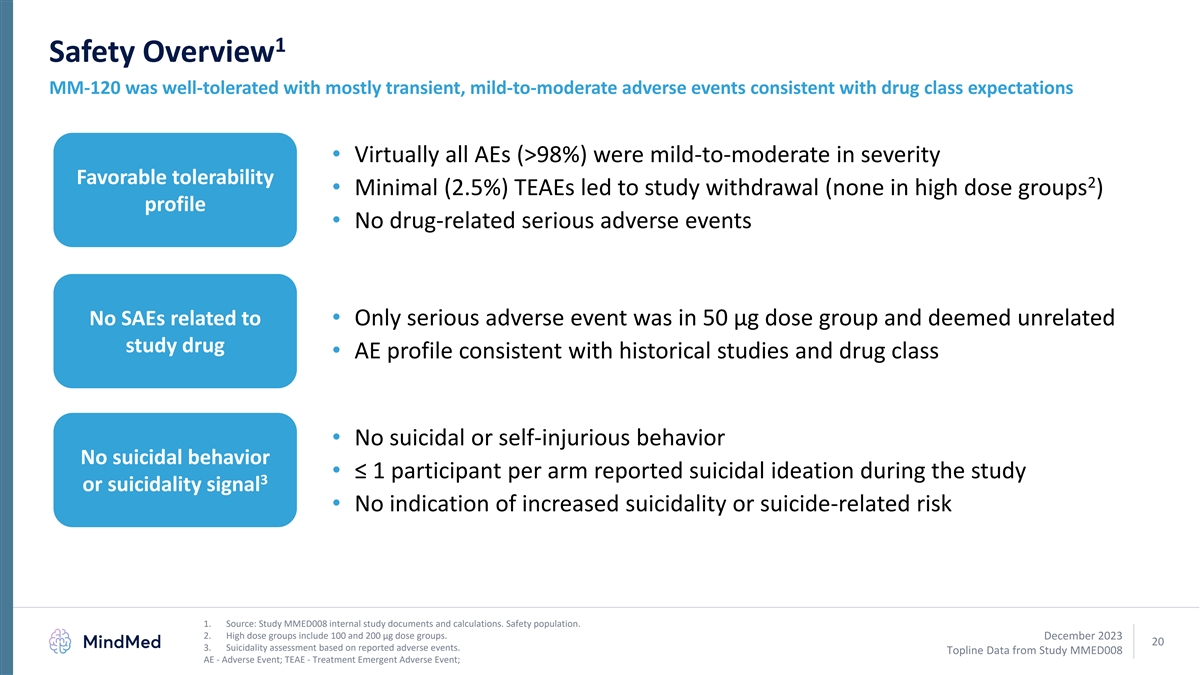
1 Safety Overview MM-120 was well-tolerated with mostly transient, mild-to-moderate adverse events consistent with drug class expectations • Virtually all AEs (>98%) were mild-to-moderate in severity Favorable tolerability 2 • Minimal (2.5%) TEAEs led to study withdrawal (none in high dose groups ) profile • No drug-related serious adverse events No SAEs related to • Only serious adverse event was in 50 µg dose group and deemed unrelated study drug • AE profile consistent with historical studies and drug class • No suicidal or self-injurious behavior No suicidal behavior • ≤ 1 participant per arm reported suicidal ideation during the study 3 or suicidality signal • No indication of increased suicidality or suicide-related risk 1. Source: Study MMED008 internal study documents and calculations. Safety population. 2. High dose groups include 100 and 200 µg dose groups. December 2023 20 3. Suicidality assessment based on reported adverse events. Topline Data from Study MMED008 AE - Adverse Event; TEAE - Treatment Emergent Adverse Event;
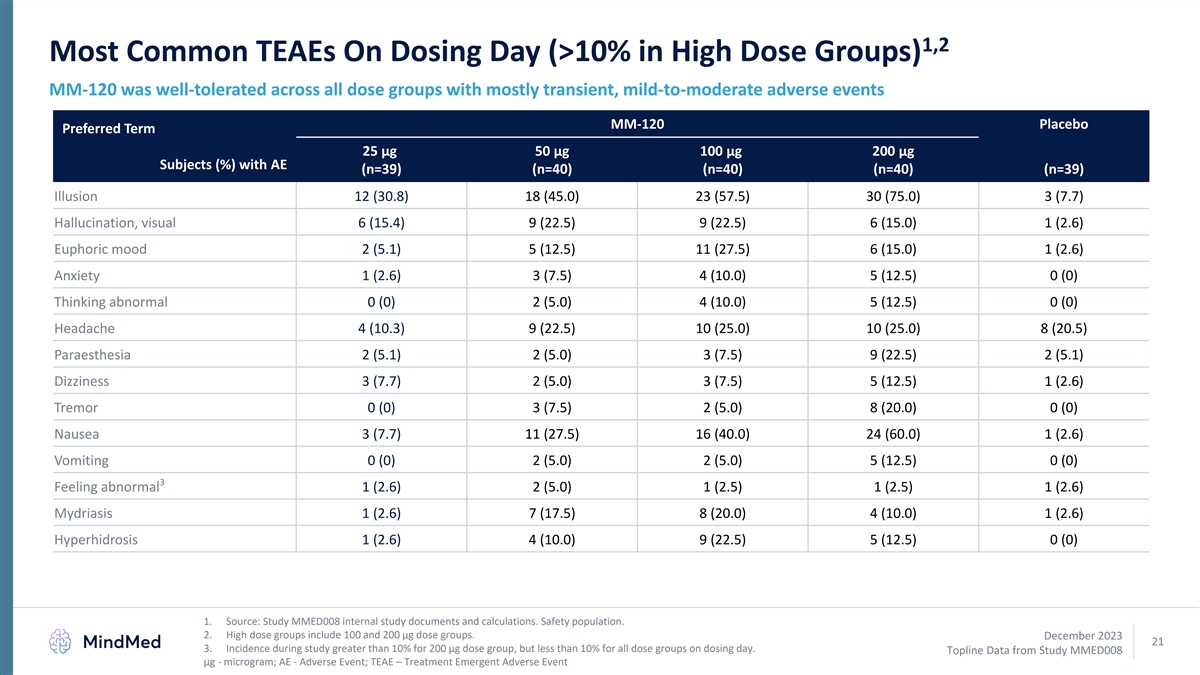
1,2 Most Common TEAEs On Dosing Day (>10% in High Dose Groups) MM-120 was well-tolerated across all dose groups with mostly transient, mild-to-moderate adverse events MM-120 Placebo Preferred Term 25 µg 50 µg 100 µg 200 µg Subjects (%) with AE (n=39) (n=40) (n=40) (n=40) (n=39) Illusion 12 (30.8) 18 (45.0) 23 (57.5) 30 (75.0) 3 (7.7) Hallucination, visual 6 (15.4) 9 (22.5) 9 (22.5) 6 (15.0) 1 (2.6) Euphoric mood 2 (5.1) 5 (12.5) 11 (27.5) 6 (15.0) 1 (2.6) Anxiety 1 (2.6) 3 (7.5) 4 (10.0) 5 (12.5) 0 (0) Thinking abnormal 0 (0) 2 (5.0) 4 (10.0) 5 (12.5) 0 (0) Headache 4 (10.3) 9 (22.5) 10 (25.0) 10 (25.0) 8 (20.5) Paraesthesia 2 (5.1) 2 (5.0) 3 (7.5) 9 (22.5) 2 (5.1) Dizziness 3 (7.7) 2 (5.0) 3 (7.5) 5 (12.5) 1 (2.6) Tremor 0 (0) 3 (7.5) 2 (5.0) 8 (20.0) 0 (0) Nausea 3 (7.7) 11 (27.5) 16 (40.0) 24 (60.0) 1 (2.6) Vomiting 0 (0) 2 (5.0) 2 (5.0) 5 (12.5) 0 (0) 3 Feeling abnormal 1 (2.6) 2 (5.0) 1 (2.5) 1 (2.5) 1 (2.6) Mydriasis 1 (2.6) 7 (17.5) 8 (20.0) 4 (10.0) 1 (2.6) Hyperhidrosis 1 (2.6) 4 (10.0) 9 (22.5) 5 (12.5) 0 (0) 1. Source: Study MMED008 internal study documents and calculations. Safety population. 2. High dose groups include 100 and 200 µg dose groups. December 2023 21 3. Incidence during study greater than 10% for 200 µg dose group, but less than 10% for all dose groups on dosing day. Topline Data from Study MMED008 µg - microgram; AE - Adverse Event; TEAE – Treatment Emergent Adverse Event
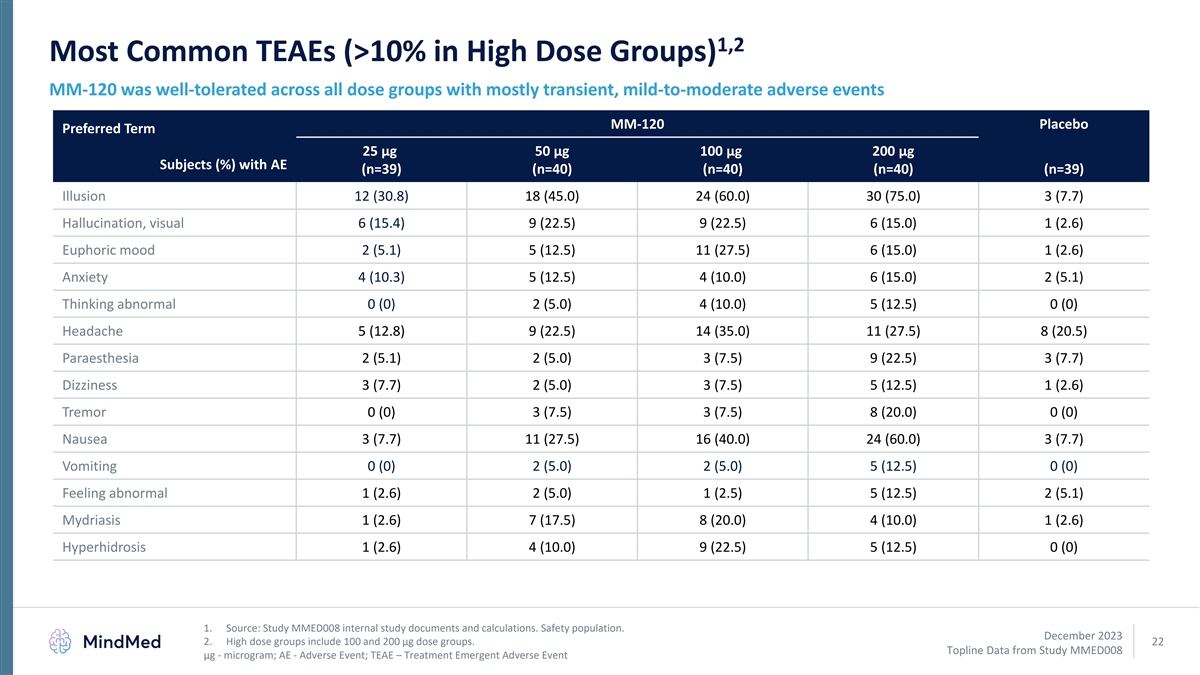
1,2 Most Common TEAEs (>10% in High Dose Groups) MM-120 was well-tolerated across all dose groups with mostly transient, mild-to-moderate adverse events MM-120 Placebo Preferred Term 25 µg 50 µg 100 µg 200 µg Subjects (%) with AE (n=39) (n=40) (n=40) (n=40) (n=39) Illusion 12 (30.8) 18 (45.0) 24 (60.0) 30 (75.0) 3 (7.7) Hallucination, visual 6 (15.4) 9 (22.5) 9 (22.5) 6 (15.0) 1 (2.6) Euphoric mood 2 (5.1) 5 (12.5) 11 (27.5) 6 (15.0) 1 (2.6) Anxiety 4 (10.3) 5 (12.5) 4 (10.0) 6 (15.0) 2 (5.1) Thinking abnormal 0 (0) 2 (5.0) 4 (10.0) 5 (12.5) 0 (0) Headache 5 (12.8) 9 (22.5) 14 (35.0) 11 (27.5) 8 (20.5) Paraesthesia 2 (5.1) 2 (5.0) 3 (7.5) 9 (22.5) 3 (7.7) Dizziness 3 (7.7) 2 (5.0) 3 (7.5) 5 (12.5) 1 (2.6) Tremor 0 (0) 3 (7.5) 3 (7.5) 8 (20.0) 0 (0) Nausea 3 (7.7) 11 (27.5) 16 (40.0) 24 (60.0) 3 (7.7) Vomiting 0 (0) 2 (5.0) 2 (5.0) 5 (12.5) 0 (0) Feeling abnormal 1 (2.6) 2 (5.0) 1 (2.5) 5 (12.5) 2 (5.1) Mydriasis 1 (2.6) 7 (17.5) 8 (20.0) 4 (10.0) 1 (2.6) Hyperhidrosis 1 (2.6) 4 (10.0) 9 (22.5) 5 (12.5) 0 (0) 1. Source: Study MMED008 internal study documents and calculations. Safety population. December 2023 2. High dose groups include 100 and 200 µg dose groups. 22 Topline Data from Study MMED008 µg - microgram; AE - Adverse Event; TEAE – Treatment Emergent Adverse Event

MM-120 MM-120 Development Plan LSD D-tartrate for Generalized Anxiety Disorder (GAD) December 2023 23 Topline Data from Study MMED008
Multiple Studies Support Phase 3 Development of MM-120 1 • Achieved goals of Phase 2 development o Characterized dose-response to inform dose selection in GAD o Achieved large, statistically significant and clinically meaningful effect in GAD o Showed rapid and durable therapeutic benefits on validated endpoint o Demonstrated standalone drug effect in absence of psychotherapeutic intervention • Multiple studies support activity of MM-120 o Phase 2b randomized, placebo-controlled dose optimization trial in GAD (Study MMED008) o One prior modern, randomized, placebo-controlled IIT of lysergide in anxiety disorders o Over twenty legacy studies of lysergide in anxiety and other neurotic disorders • Company believes Phase 2b data supports dose selection and advancement into Phase 3 development 1. Source: Study MMED008 internal study documents and calculations. December 2023 24 GAD - Generalized Anxiety Disorder; IIT - Investigator Initiated Trial Topline Data from Study MMED008
MM-120 Development Pathway • Key design elements expected to be consistent between Phase 2b and Phase 3 studies o Hamilton Anxiety Scale (HAM-A) at week 4 expected primary endpoint o Limited changes to key inclusion/exclusion criteria o No planned change in dosing session monitoring protocol • Two Phase 3 pivotal clinical trials in planning o 12-week randomized, placebo-controlled primary efficacy study design o Open-label extension to establish retreatment parameters o Expect to initiate Phase 3 development in the second half of 2024 December 2023 1. Phase 3 and subsequent clinical study design subject to regulatory discussion and review, including at potential End of Phase 2 meeting. 25 Topline Data from Study MMED008
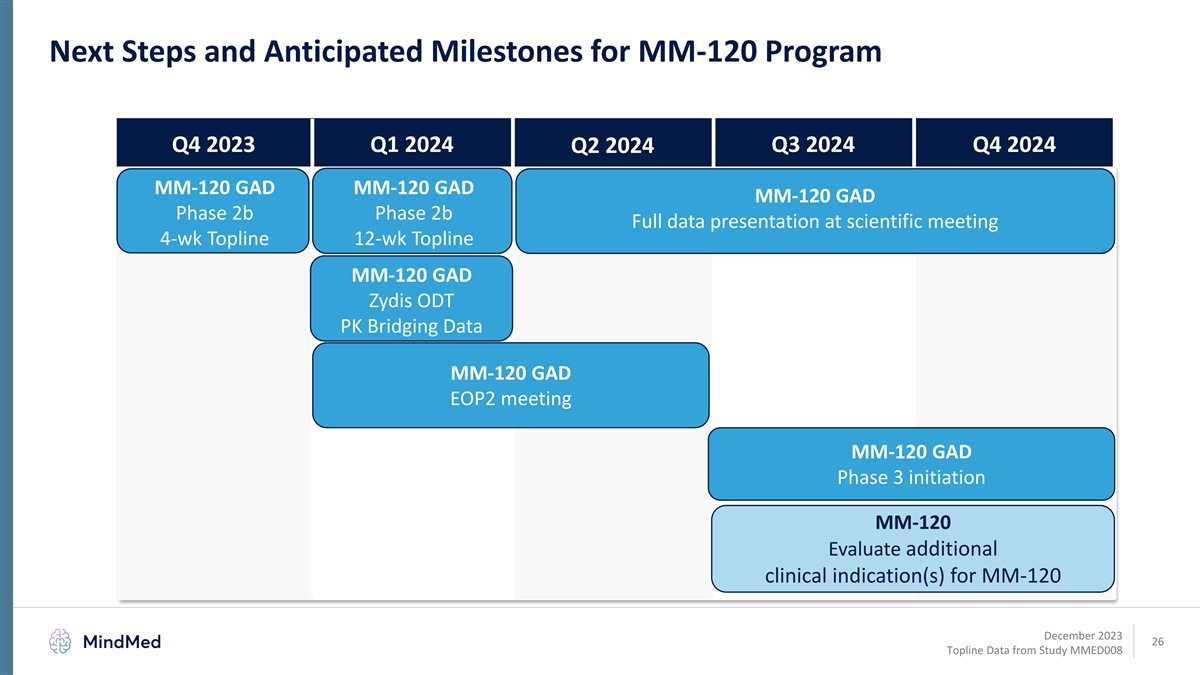
Next Steps and Anticipated Milestones for MM-120 Program Q4 2023 Q1 2024 Q3 2024 Q4 2024 Q2 2024 MM-120 GAD MM-120 GAD MM-120 GAD Phase 2b Phase 2b Full data presentation at scientific meeting 4-wk Topline 12-wk Topline MM-120 GAD Zydis ODT PK Bridging Data MM-120 GAD EOP2 meeting MM-120 GAD Phase 3 initiation MM-120 Evaluate additional clinical indication(s) for MM-120 December 2023 26 Topline Data from Study MMED008
Q&A December 2023 27 Topline Data from Study MMED008
Appendix – Phase 2b GAD Study December 2023 28 Topline Data from Study MMED008
1 Phase 2b Trial Design Aligns with Subsequent FDA Draft Guidance FDA issued 2023 draft guidance on clinical trials with psychedelic drugs • Provides clarity on regulatory expectations and R&D considerations • Guidance will “help researchers design studies that will yield interpretable results 1 that will be capable of supporting future drug applications” Phase 2b design is aligned with FDA guidance • No concurrent psychotherapy – “Psychotherapeutic interventions have the 1 potential to increase expectancy and performance biases” 1 • Placebo-controlled – “allows for better contextualization of safety findings” • Dose-ranging – “The dose-response relationship for most psychedelic drugs is poorly understood. Sponsors should take appropriate steps to characterize the 1 dose-response relationship.” December 2023 1. FDA 2023 Draft Guidance: Psychedelic Drugs: Considerations for Clinical Investigations. 29 Topline Data from Study MMED008
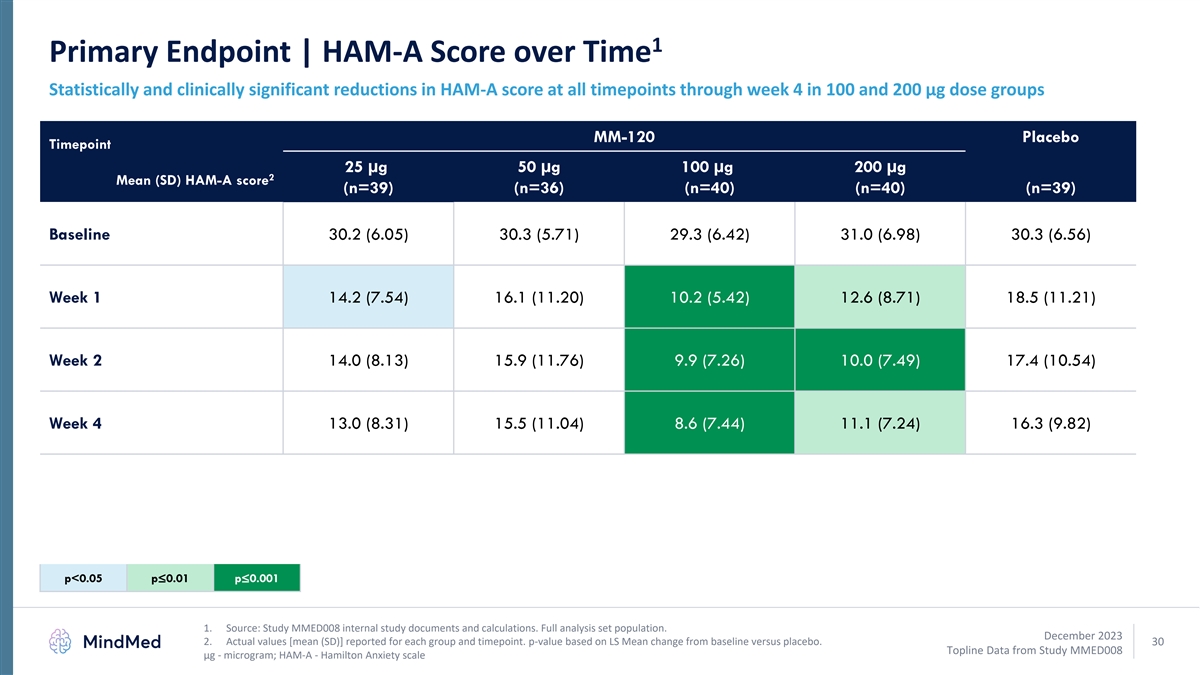
1 Primary Endpoint | HAM-A Score over Time Statistically and clinically significant reductions in HAM-A score at all timepoints through week 4 in 100 and 200 µg dose groups MM-120 Placebo Timepoint 25 µg 50 µg 100 µg 200 µg 2 Mean (SD) HAM-A score (n=39) (n=36) (n=40) (n=40) (n=39) Baseline 30.2 (6.05) 30.3 (5.71) 29.3 (6.42) 31.0 (6.98) 30.3 (6.56) Week 1 14.2 (7.54) 16.1 (11.20) 10.2 (5.42) 12.6 (8.71) 18.5 (11.21) Week 2 14.0 (8.13) 15.9 (11.76) 9.9 (7.26) 10.0 (7.49) 17.4 (10.54) Week 4 13.0 (8.31) 15.5 (11.04) 8.6 (7.44) 11.1 (7.24) 16.3 (9.82) p<0.05p≤0.01p≤0.001 1. Source: Study MMED008 internal study documents and calculations. Full analysis set population. December 2023 2. Actual values [mean (SD)] reported for each group and timepoint. p-value based on LS Mean change from baseline versus placebo. 30 Topline Data from Study MMED008 µg - microgram; HAM-A - Hamilton Anxiety scale
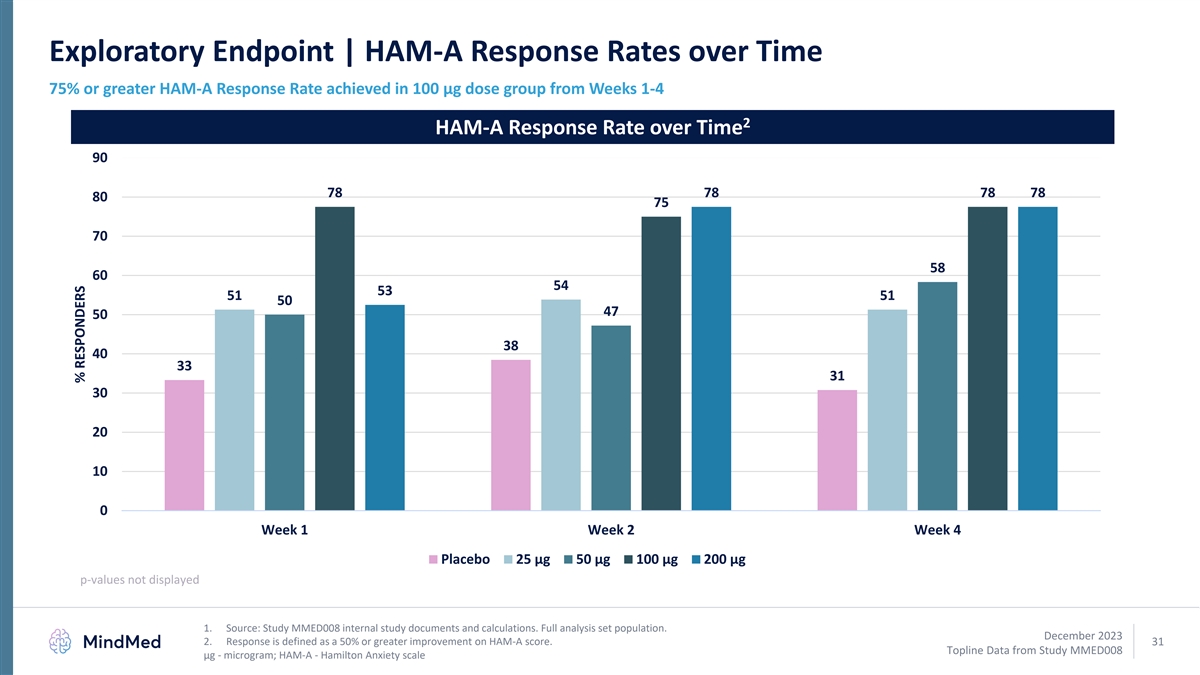
Exploratory Endpoint | HAM-A Response Rates over Time 75% or greater HAM-A Response Rate achieved in 100 µg dose group from Weeks 1-4 2 HAM-A Response Rate over Time 90 78 78 78 78 80 75 70 58 60 54 53 51 51 50 47 50 38 40 33 31 30 20 10 0 Week 1 Week 2 Week 4 Placebo 25 μg 50 μg 100 μg 200 μg p-values not displayed 1. Source: Study MMED008 internal study documents and calculations. Full analysis set population. December 2023 2. Response is defined as a 50% or greater improvement on HAM-A score. 31 Topline Data from Study MMED008 µg - microgram; HAM-A - Hamilton Anxiety scale % RESPONDERS
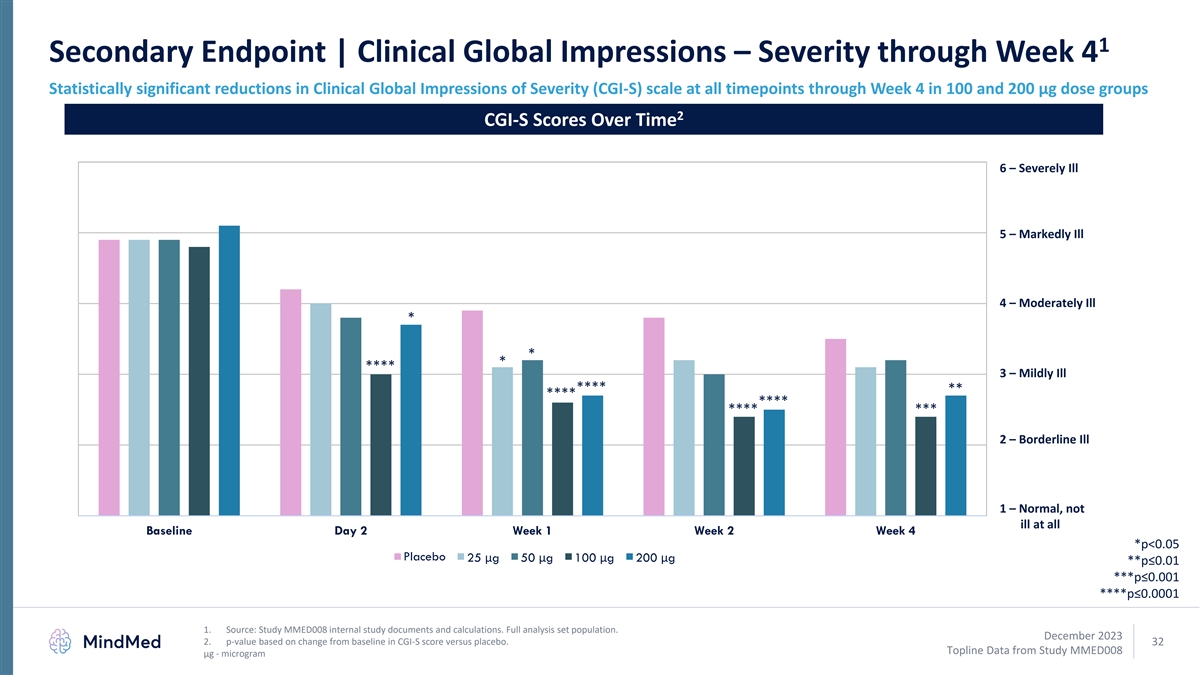
1 Secondary Endpoint | Clinical Global Impressions – Severity through Week 4 Statistically significant reductions in Clinical Global Impressions of Severity (CGI-S) scale at all timepoints through Week 4 in 100 and 200 µg dose groups 2 CGI-S Scores Over Time 6 – Severely Ill 5 – Markedly Ill 4 – Moderately Ill * * * **** 3 – Mildly Ill **** ** **** **** **** *** 2 – Borderline Ill 1 – Normal, not ill at all Baseline Day 2 Week 1 Week 2 Week 4 *p<0.05 Placebo 25 μg 50 μg 100 μg 200 μg **p≤0.01 ***p≤0.001 ****p≤0.0001 1. Source: Study MMED008 internal study documents and calculations. Full analysis set population. December 2023 2. p-value based on change from baseline in CGI-S score versus placebo. 32 Topline Data from Study MMED008 μg - microgram
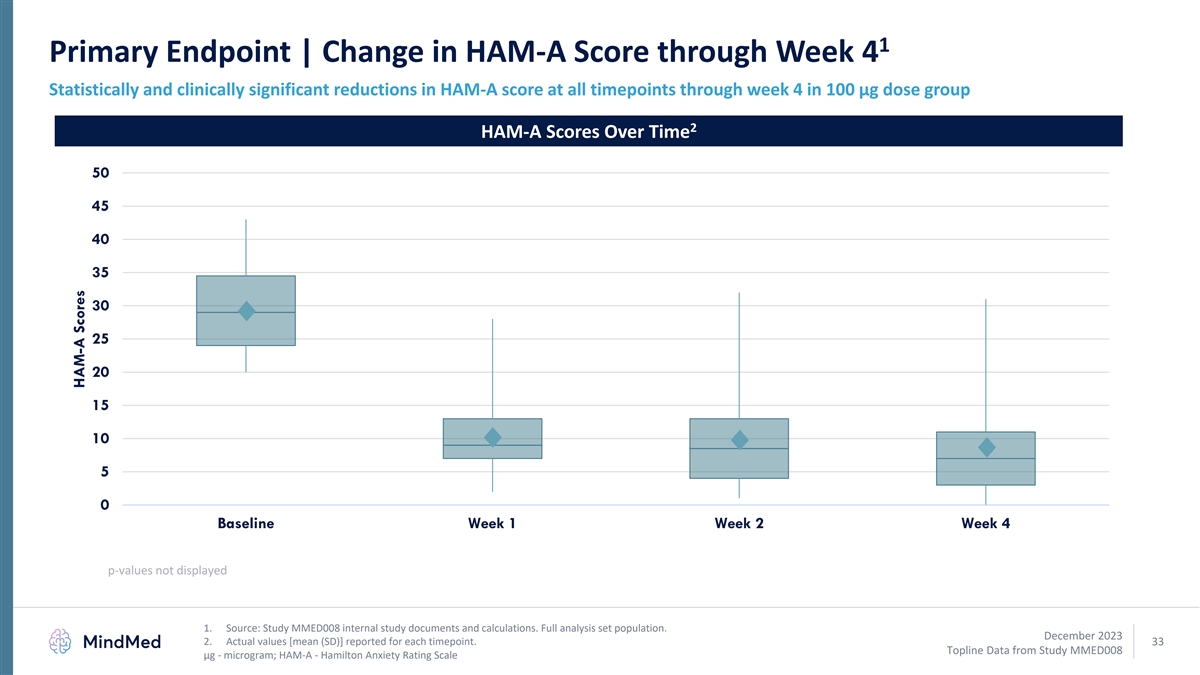
1 Primary Endpoint | Change in HAM-A Score through Week 4 Statistically and clinically significant reductions in HAM-A score at all timepoints through week 4 in 100 µg dose group 2 HAM-A Scores Over Time 50 45 40 35 30 25 20 15 10 5 0 Baseline Week 1 Week 2 Week 4 p-values not displayed 1. Source: Study MMED008 internal study documents and calculations. Full analysis set population. December 2023 2. Actual values [mean (SD)] reported for each timepoint. 33 Topline Data from Study MMED008 µg - microgram; HAM-A - Hamilton Anxiety Rating Scale HAM-A Scores
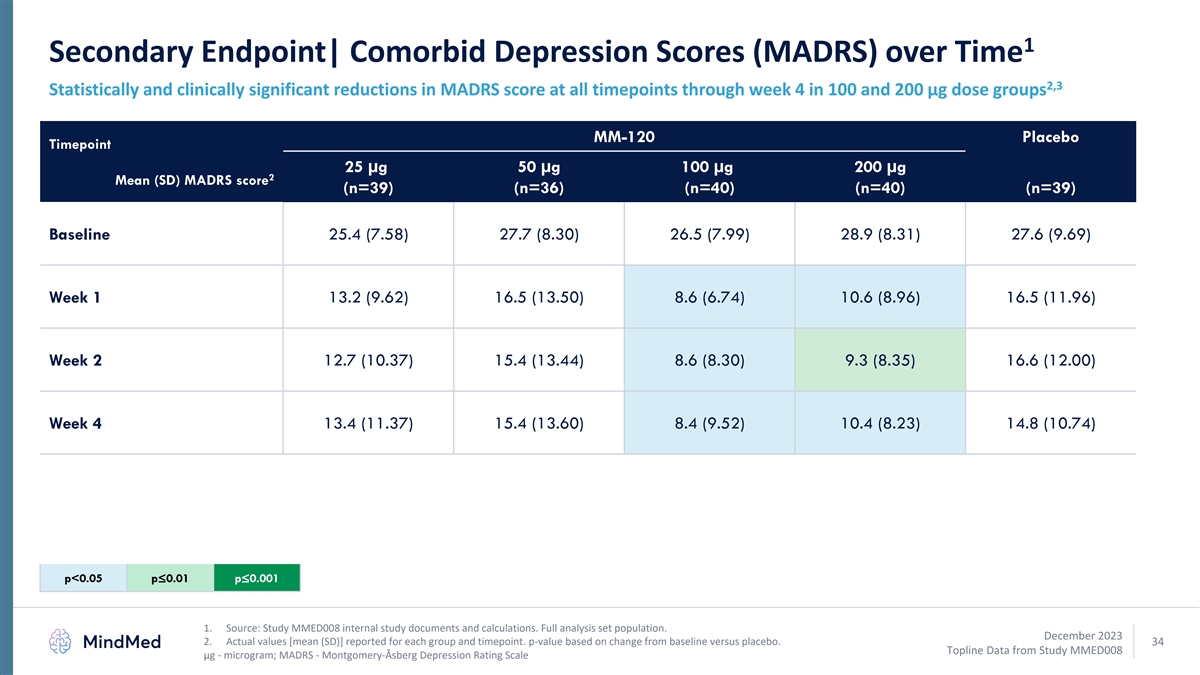
1 Secondary Endpoint| Comorbid Depression Scores (MADRS) over Time 2,3 Statistically and clinically significant reductions in MADRS score at all timepoints through week 4 in 100 and 200 µg dose groups MM-120 Placebo Timepoint 25 µg 50 µg 100 µg 200 µg 2 Mean (SD) MADRS score (n=39) (n=36) (n=40) (n=40) (n=39) Baseline 25.4 (7.58) 27.7 (8.30) 26.5 (7.99) 28.9 (8.31) 27.6 (9.69) Week 1 13.2 (9.62) 16.5 (13.50) 8.6 (6.74) 10.6 (8.96) 16.5 (11.96) Week 2 12.7 (10.37) 15.4 (13.44) 8.6 (8.30) 9.3 (8.35) 16.6 (12.00) Week 4 13.4 (11.37) 15.4 (13.60) 8.4 (9.52) 10.4 (8.23) 14.8 (10.74) p<0.05p≤0.01p≤0.001 1. Source: Study MMED008 internal study documents and calculations. Full analysis set population. December 2023 2. Actual values [mean (SD)] reported for each group and timepoint. p-value based on change from baseline versus placebo. 34 Topline Data from Study MMED008 µg - microgram; MADRS - Montgomery-Åsberg Depression Rating Scale
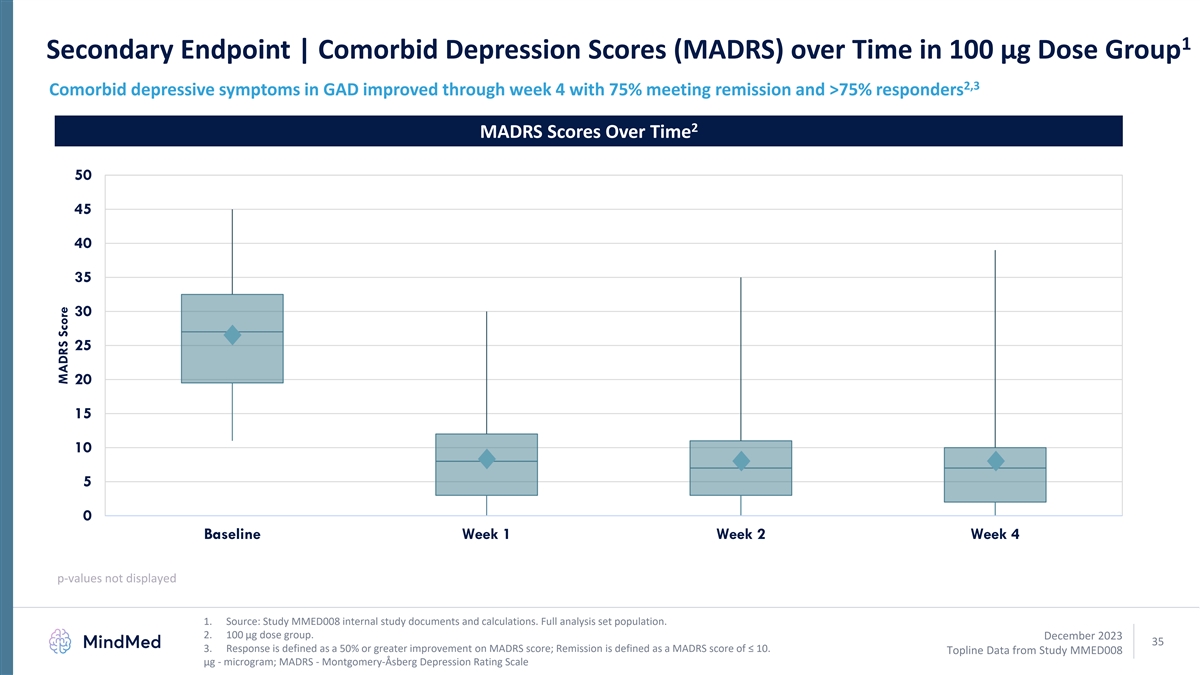
1 Secondary Endpoint | Comorbid Depression Scores (MADRS) over Time in 100 µg Dose Group 2,3 Comorbid depressive symptoms in GAD improved through week 4 with 75% meeting remission and >75% responders 2 MADRS Scores Over Time 50 45 40 35 30 25 20 15 10 5 0 Baseline Week 1 Week 2 Week 4 p-values not displayed 1. Source: Study MMED008 internal study documents and calculations. Full analysis set population. 2. 100 µg dose group. December 2023 35 3. Response is defined as a 50% or greater improvement on MADRS score; Remission is defined as a MADRS score of ≤ 10. Topline Data from Study MMED008 µg - microgram; MADRS - Montgomery-Åsberg Depression Rating Scale MADRS Score
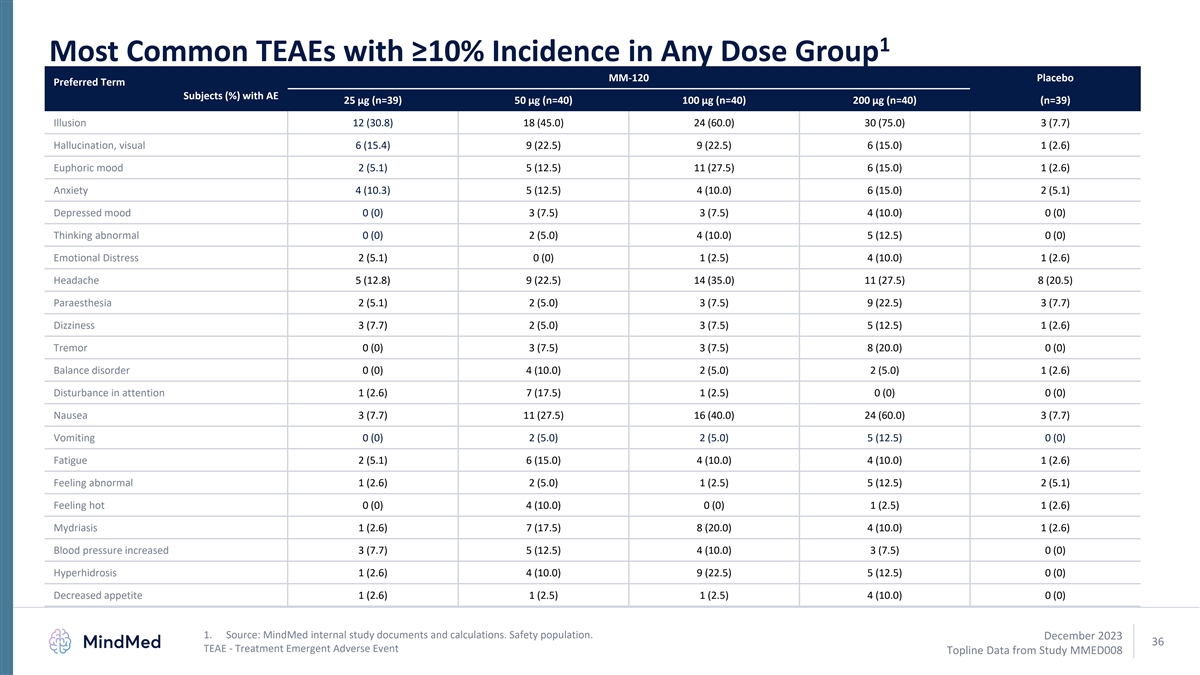
1 Most Common TEAEs with ≥10% Incidence in Any Dose Group MM-120 Placebo Preferred Term Subjects (%) with AE 25 µg (n=39) 50 µg (n=40) 100 µg (n=40) 200 µg (n=40) (n=39) Illusion 12 (30.8) 18 (45.0) 24 (60.0) 30 (75.0) 3 (7.7) Hallucination, visual 6 (15.4) 9 (22.5) 9 (22.5) 6 (15.0) 1 (2.6) Euphoric mood 2 (5.1) 5 (12.5) 11 (27.5) 6 (15.0) 1 (2.6) Anxiety 4 (10.3) 5 (12.5) 4 (10.0) 6 (15.0) 2 (5.1) Depressed mood 0 (0) 3 (7.5) 3 (7.5) 4 (10.0) 0 (0) Thinking abnormal 0 (0) 2 (5.0) 4 (10.0) 5 (12.5) 0 (0) Emotional Distress 2 (5.1) 0 (0) 1 (2.5) 4 (10.0) 1 (2.6) Headache 5 (12.8) 9 (22.5) 14 (35.0) 11 (27.5) 8 (20.5) Paraesthesia 2 (5.1) 2 (5.0) 3 (7.5) 9 (22.5) 3 (7.7) Dizziness 3 (7.7) 2 (5.0) 3 (7.5) 5 (12.5) 1 (2.6) Tremor 0 (0) 3 (7.5) 3 (7.5) 8 (20.0) 0 (0) Balance disorder 0 (0) 4 (10.0) 2 (5.0) 2 (5.0) 1 (2.6) Disturbance in attention 1 (2.6) 7 (17.5) 1 (2.5) 0 (0) 0 (0) Nausea 3 (7.7) 11 (27.5) 16 (40.0) 24 (60.0) 3 (7.7) Vomiting 0 (0) 2 (5.0) 2 (5.0) 5 (12.5) 0 (0) Fatigue 2 (5.1) 6 (15.0) 4 (10.0) 4 (10.0) 1 (2.6) Feeling abnormal 1 (2.6) 2 (5.0) 1 (2.5) 5 (12.5) 2 (5.1) Feeling hot 0 (0) 4 (10.0) 0 (0) 1 (2.5) 1 (2.6) Mydriasis 1 (2.6) 7 (17.5) 8 (20.0) 4 (10.0) 1 (2.6) Blood pressure increased 3 (7.7) 5 (12.5) 4 (10.0) 3 (7.5) 0 (0) Hyperhidrosis 1 (2.6) 4 (10.0) 9 (22.5) 5 (12.5) 0 (0) Decreased appetite 1 (2.6) 1 (2.5) 1 (2.5) 4 (10.0) 0 (0) 1. Source: MindMed internal study documents and calculations. Safety population. December 2023 36 TEAE - Treatment Emergent Adverse Event Topline Data from Study MMED008
Appendix – Intellectual Property December 2023 37 Topline Data from Study MMED008
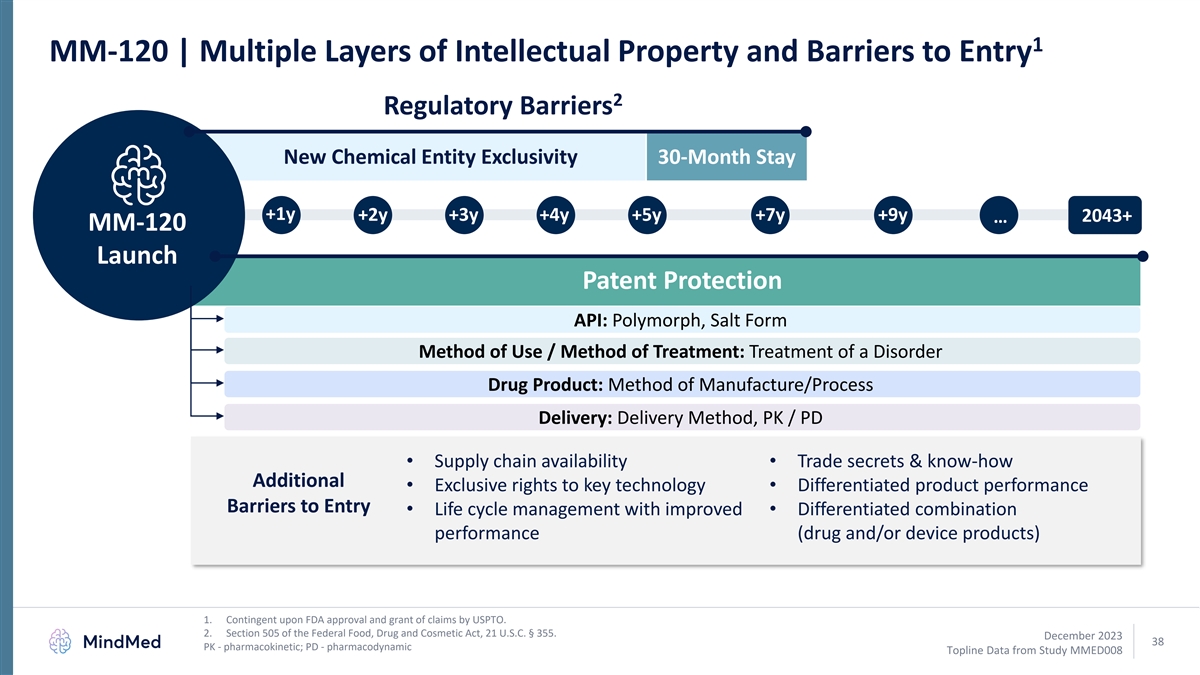
1 MM-120 | Multiple Layers of Intellectual Property and Barriers to Entry 2 Regulatory Barriers New Chemical Entity Exclusivity 30-Month Stay +1y +2y +3y +4y +5y +7y +9y … 2043+ MM-120 Launch Patent Protection API: Polymorph, Salt Form Method of Use / Method of Treatment: Treatment of a Disorder Drug Product: Method of Manufacture/Process Delivery: Delivery Method, PK / PD • Supply chain availability• Trade secrets & know-how Additional • Exclusive rights to key technology• Differentiated product performance Barriers to Entry • Life cycle management with improved • Differentiated combination performance (drug and/or device products) 1. Contingent upon FDA approval and grant of claims by USPTO. 2. Section 505 of the Federal Food, Drug and Cosmetic Act, 21 U.S.C. § 355. December 2023 38 PK - pharmacokinetic; PD - pharmacodynamic Topline Data from Study MMED008
MM-120 | Multipronged Market Protection Strategies 1 • Highlights of Patent Protection Strategy o Methods of treating GAD o Stability and methods of manufacturing for API (salt form and polymorphs) o Improved product performance with faster absorption, less variability and potential shorter duration o Methods of use related to ODT formulation, treatment of GAD and other patient outcomes o Additional claims related to dose identification, patient monitoring, digital technology and others • Highlights of Non-Patent Protection Strategy o FDA-granted NCE exclusivity o 30-month stay against generic applicants (with Paragraph IV claims) o Limited supply chain availability 2 o Exclusive rights to key technology (e.g. Catalent Zydis® ODT) o Trade secrets and know-how 1. Source: US Patent and Trade Office (https://ppubs.uspto.gov/). 2. Catalent has granted exclusive rights to intellectual property for Zydis® for lysergide (LSD). December 2023 39 FDA - U.S. Food and Drug Administration; API – active pharmaceutical ingredient; ODT – orally disintegrating tablet; NCE – new chemical entity Topline Data from Study MMED008
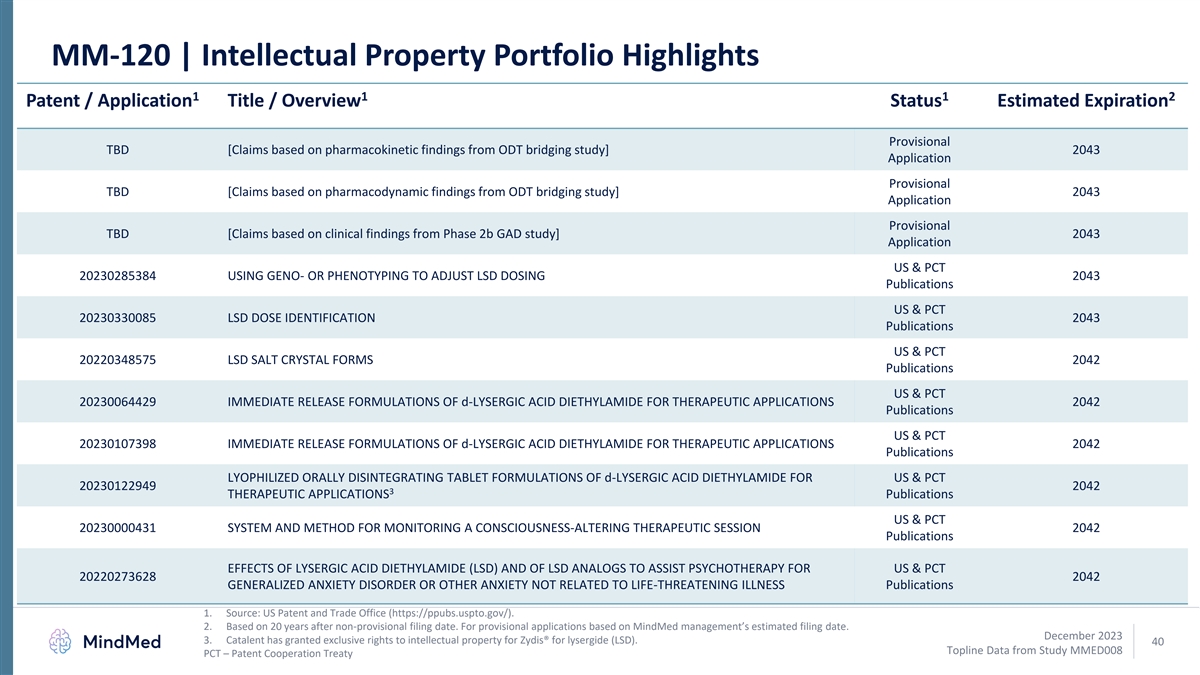
MM-120 | Intellectual Property Portfolio Highlights 1 1 1 2 Patent / Application Title / Overview Status Estimated Expiration Provisional TBD [Claims based on pharmacokinetic findings from ODT bridging study] 2043 Application Provisional TBD [Claims based on pharmacodynamic findings from ODT bridging study] 2043 Application Provisional TBD [Claims based on clinical findings from Phase 2b GAD study] 2043 Application US & PCT 20230285384 USING GENO- OR PHENOTYPING TO ADJUST LSD DOSING 2043 Publications US & PCT 20230330085 LSD DOSE IDENTIFICATION 2043 Publications US & PCT 20220348575 LSD SALT CRYSTAL FORMS 2042 Publications US & PCT 20230064429 IMMEDIATE RELEASE FORMULATIONS OF d-LYSERGIC ACID DIETHYLAMIDE FOR THERAPEUTIC APPLICATIONS 2042 Publications US & PCT 20230107398 IMMEDIATE RELEASE FORMULATIONS OF d-LYSERGIC ACID DIETHYLAMIDE FOR THERAPEUTIC APPLICATIONS 2042 Publications LYOPHILIZED ORALLY DISINTEGRATING TABLET FORMULATIONS OF d-LYSERGIC ACID DIETHYLAMIDE FOR US & PCT 20230122949 2042 3 THERAPEUTIC APPLICATIONS Publications US & PCT 20230000431 SYSTEM AND METHOD FOR MONITORING A CONSCIOUSNESS-ALTERING THERAPEUTIC SESSION 2042 Publications EFFECTS OF LYSERGIC ACID DIETHYLAMIDE (LSD) AND OF LSD ANALOGS TO ASSIST PSYCHOTHERAPY FOR US & PCT 20220273628 2042 GENERALIZED ANXIETY DISORDER OR OTHER ANXIETY NOT RELATED TO LIFE-THREATENING ILLNESS Publications 1. Source: US Patent and Trade Office (https://ppubs.uspto.gov/). 2. Based on 20 years after non-provisional filing date. For provisional applications based on MindMed management’s estimated filing date. December 2023 3. Catalent has granted exclusive rights to intellectual property for Zydis® for lysergide (LSD). 40 Topline Data from Study MMED008 PCT – Patent Cooperation Treaty
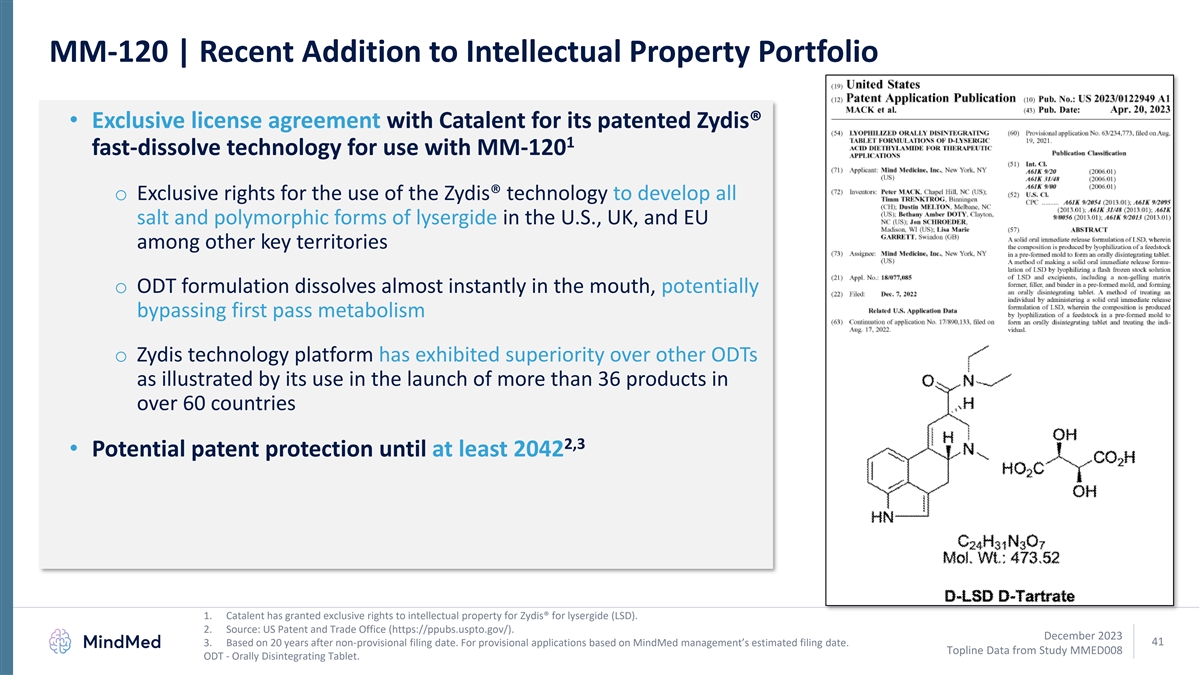
MM-120 | Recent Addition to Intellectual Property Portfolio • Exclusive license agreement with Catalent for its patented Zydis® 1 fast-dissolve technology for use with MM-120 o Exclusive rights for the use of the Zydis® technology to develop all salt and polymorphic forms of lysergide in the U.S., UK, and EU among other key territories o ODT formulation dissolves almost instantly in the mouth, potentially bypassing first pass metabolism o Zydis technology platform has exhibited superiority over other ODTs as illustrated by its use in the launch of more than 36 products in over 60 countries 2,3 • Potential patent protection until at least 2042 1. Catalent has granted exclusive rights to intellectual property for Zydis® for lysergide (LSD). 2. Source: US Patent and Trade Office (https://ppubs.uspto.gov/). December 2023 41 3. Based on 20 years after non-provisional filing date. For provisional applications based on MindMed management’s estimated filing date. Topline Data from Study MMED008 ODT - Orally Disintegrating Tablet.
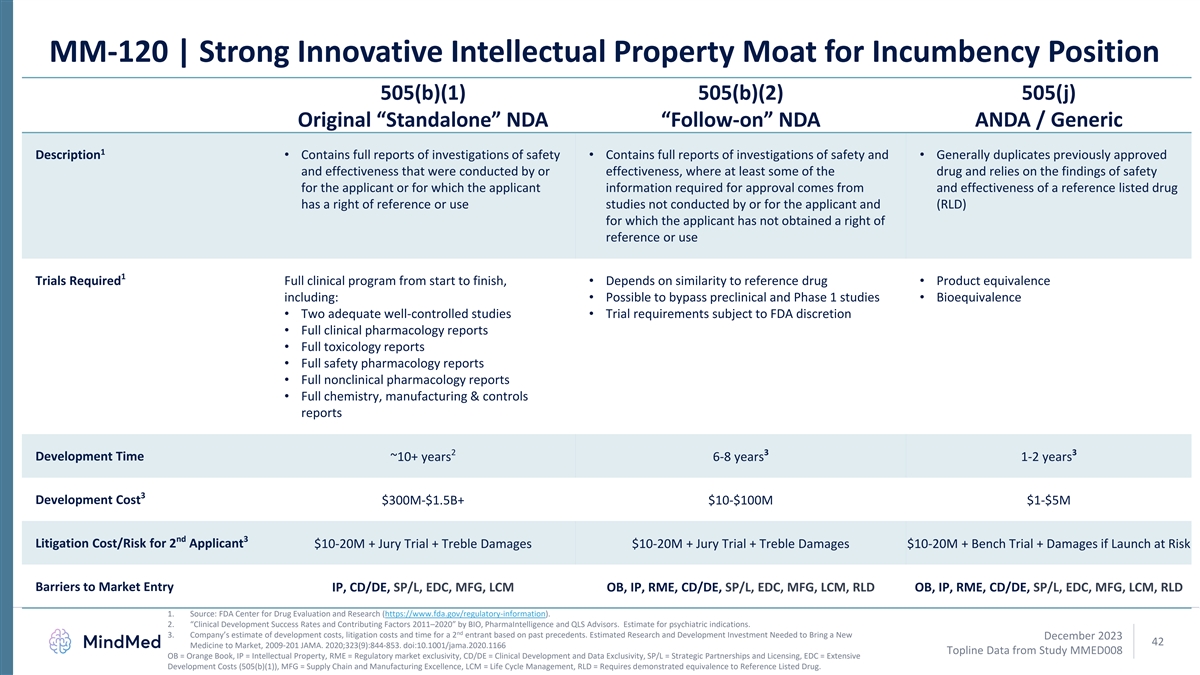
MM-120 | Strong Innovative Intellectual Property Moat for Incumbency Position 505(b)(1) 505(b)(2) 505(j) ANDA / Generic Original “Standalone” NDA “Follow-on” NDA 1 Description• Contains full reports of investigations of safety • Contains full reports of investigations of safety and • Generally duplicates previously approved and effectiveness that were conducted by or effectiveness, where at least some of the drug and relies on the findings of safety for the applicant or for which the applicant information required for approval comes from and effectiveness of a reference listed drug has a right of reference or use studies not conducted by or for the applicant and (RLD) for which the applicant has not obtained a right of reference or use 1 Trials Required Full clinical program from start to finish, • Depends on similarity to reference drug• Product equivalence including:• Possible to bypass preclinical and Phase 1 studies• Bioequivalence • Two adequate well-controlled studies• Trial requirements subject to FDA discretion • Full clinical pharmacology reports • Full toxicology reports • Full safety pharmacology reports • Full nonclinical pharmacology reports • Full chemistry, manufacturing & controls reports 2 3 3 Development Time ~10+ years 6-8 years 1-2 years 3 Development Cost $300M-$1.5B+ $10-$100M $1-$5M nd 3 Litigation Cost/Risk for 2 Applicant $10-20M + Jury Trial + Treble Damages $10-20M + Jury Trial + Treble Damages $10-20M + Bench Trial + Damages if Launch at Risk Barriers to Market Entry IP, CD/DE, SP/L, EDC, MFG, LCM OB, IP, RME, CD/DE, SP/L, EDC, MFG, LCM, RLD OB, IP, RME, CD/DE, SP/L, EDC, MFG, LCM, RLD 1. Source: FDA Center for Drug Evaluation and Research (https://www.fda.gov/regulatory-information). 2. “Clinical Development Success Rates and Contributing Factors 2011–2020” by BIO, PharmaIntelligence and QLS Advisors. Estimate for psychiatric indications. nd 3. Company’s estimate of development costs, litigation costs and time for a 2 entrant based on past precedents. Estimated Research and Development Investment Needed to Bring a New December 2023 42 Medicine to Market, 2009-201 JAMA. 2020;323(9):844-853. doi:10.1001/jama.2020.1166 Topline Data from Study MMED008 OB = Orange Book, IP = Intellectual Property, RME = Regulatory market exclusivity, CD/DE = Clinical Development and Data Exclusivity, SP/L = Strategic Partnerships and Licensing, EDC = Extensive Development Costs (505(b)(1)), MFG = Supply Chain and Manufacturing Excellence, LCM = Life Cycle Management, RLD = Requires demonstrated equivalence to Reference Listed Drug.
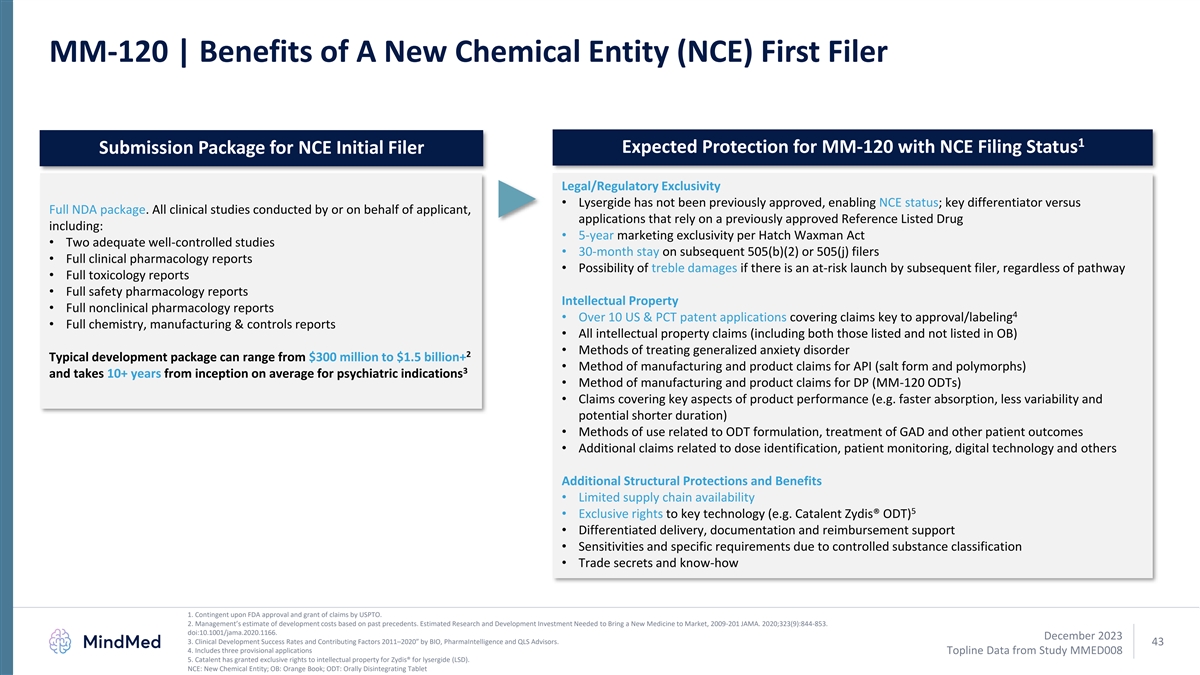
MM-120 | Benefits of A New Chemical Entity (NCE) First Filer 1 Expected Protection for MM-120 with NCE Filing Status Submission Package for NCE Initial Filer Legal/Regulatory Exclusivity • Lysergide has not been previously approved, enabling NCE status; key differentiator versus Full NDA package. All clinical studies conducted by or on behalf of applicant, applications that rely on a previously approved Reference Listed Drug including: • 5-year marketing exclusivity per Hatch Waxman Act • Two adequate well-controlled studies • 30-month stay on subsequent 505(b)(2) or 505(j) filers • Full clinical pharmacology reports • Possibility of treble damages if there is an at-risk launch by subsequent filer, regardless of pathway • Full toxicology reports • Full safety pharmacology reports Intellectual Property • Full nonclinical pharmacology reports 4 • Over 10 US & PCT patent applications covering claims key to approval/labeling • Full chemistry, manufacturing & controls reports • All intellectual property claims (including both those listed and not listed in OB) • Methods of treating generalized anxiety disorder 2 Typical development package can range from $300 million to $1.5 billion+ • Method of manufacturing and product claims for API (salt form and polymorphs) 3 and takes 10+ years from inception on average for psychiatric indications • Method of manufacturing and product claims for DP (MM-120 ODTs) • Claims covering key aspects of product performance (e.g. faster absorption, less variability and potential shorter duration) • Methods of use related to ODT formulation, treatment of GAD and other patient outcomes • Additional claims related to dose identification, patient monitoring, digital technology and others Additional Structural Protections and Benefits • Limited supply chain availability 5 • Exclusive rights to key technology (e.g. Catalent Zydis® ODT) • Differentiated delivery, documentation and reimbursement support • Sensitivities and specific requirements due to controlled substance classification • Trade secrets and know-how 1. Contingent upon FDA approval and grant of claims by USPTO. 2. Management’s estimate of development costs based on past precedents. Estimated Research and Development Investment Needed to Bring a New Medicine to Market, 2009-201 JAMA. 2020;323(9):844-853. doi:10.1001/jama.2020.1166. December 2023 3. Clinical Development Success Rates and Contributing Factors 2011–2020” by BIO, PharmaIntelligence and QLS Advisors. 43 4. Includes three provisional applications Topline Data from Study MMED008 5. Catalent has granted exclusive rights to intellectual property for Zydis® for lysergide (LSD). NCE: New Chemical Entity; OB: Orange Book; ODT: Orally Disintegrating Tablet