UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d)
of the Securities Exchange Act of 1934
Date of Report (Date of earliest event reported): December 11, 2023
DISC MEDICINE, INC.
(Exact name of registrant as specified in its charter)
| Delaware | 001-39438 | 85-1612845 | ||
| (State or other jurisdiction of incorporation) |
(Commission File Number) |
(IRS Employer Identification No.) |
| 321 Arsenal Street, Suite 101 Watertown, MA 02472 |
02472 | |
| (Address of principal executive offices) | (Zip Code) |
Registrant’s telephone number, including area code: (617) 674-9274
N/A
(Former Name or Former Address, if Changed Since Last Report)
Check the appropriate box below if the Form 8-K filing is intended to simultaneously satisfy the filing obligation of the registrant under any of the following provisions (see General Instruction A.2. below):
| ☐ | Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425) |
| ☐ | Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12) |
| ☐ | Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)) |
| ☐ | Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section 12(b) of the Act:
| Title of each class |
Trading Symbol |
Name of each exchange on which registered |
||
| Common Stock, par value $0.0001 per share | IRON | The Nasdaq Global Market |
Indicate by check mark whether the registrant is an emerging growth company as defined in Rule 405 of the Securities Act of 1933 (§230.405 of this chapter) or Rule 12b-2 of the Securities Exchange Act of 1934 (§240.12b-2 of this chapter).
Emerging growth company ☒
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
| Item 7.01 | Regulation FD Disclosure. |
On December 11, 2023, Disc Medicine, Inc. (the “Company”) issued a press release announcing the Company’s data presented at the 65th American Society of Hematology (“ASH”) Annual Meeting and Exposition. The Company will host a conference call on December 11 at 9:30 p.m. ET to review such data and the Company’s operational plans. An archived webcast will be available following the call for 30 days on the Events & Presentations section of the Company’s website at https://ir.discmedicine.com. Information contained on the Company’s website is not incorporated by reference into this Current Report on Form 8-K, and you should not consider any information on, or that can be accessed from, the Company’s website as part of this Current Report on Form 8-K. A copy of the press release is attached as Exhibit 99.1 to this Current Report on Form 8-K.
The information contained in Item 7.01 of this Current Report on Form 8-K, including Exhibit 99.1, is intended to be furnished and shall not be deemed “filed” for purposes of Section 18 of the Securities Exchange Act of 1934, as amended (the “Exchange Act”), or otherwise subject to the liabilities of that section, nor shall it be deemed incorporated by reference in any filing under the Securities Act of 1933, as amended, or the Exchange Act, except as expressly provided by specific reference in such filing. The Company undertakes no obligation to update, supplement or amend the material attached hereto as Exhibit 99.1.
| Item 8.01 | Other Events. |
Phase 2 BEACON Study Data Release
On December 11, 2023, the Company presented updated results from its ongoing Phase 2 BEACON study evaluating bitopertin in patients with erythropoietic protoporphyria (“EPP”).
The BEACON study (ACTRN12622000799752) is a randomized, open-label, parallel-arm study that enrolled 22 adult subjects with EPP or X-linked protoporphyria in Australia, and has been expanded to include adolescents. This trial was designed to assess changes in levels of Protoporphyrin IX (“PPIX”), as well as measures of photosensitivity, quality of life, and safety and tolerability. Subjects are randomized to receive either 20 mg or 60 mg of bitopertin once-daily for 24 weeks, after which patients have the option of continuing in an open-label extension of the trial for up to an additional 24 weeks. The updated data presented reflects results from all 22 adults, with a data cutoff of September 18, 2023 for PPIX data and October 20, 2023 for all other endpoints. The data are consistent with the initial positive results presented in June 2023.
| • | PPIX levels: Significant, dose-dependent, and sustained reductions in whole blood PPIX levels; mean reduction > 40% (p<0.001 versus baseline) |
| • | Demonstrated substantial and consistent improvements in sunlight tolerance across all study measures |
| • | Highlights of the data: |
| • | Average time to prodrome: Greater than 3x improvement vs. baseline (p<0.001) |
| • | Increased proportion of days without symptoms: 78% vs. 33% (baseline) |
| • | Increased proportion of sunlight challenges without prodromes: 54% vs. 7% (baseline) |
| • | Phototoxic reactions: 92% reduction in patient-reported reactions while on treatment compared to baseline |
| • | Nearly all participants reported improvements in multiple quality-of-life measures at the end of study |
| • | Mean cumulative total time in light on days without pain observed over the 6-month treatment period (precedented pivotal endpoint): 222.6 ± 129.3 hours |
| • | Bitopertin-treated participants had a >3x increase relative to historical control |
| • | Bitopertin was generally well tolerated at both dose levels with no serious adverse events, stable mean hemoglobin levels, and no anemia adverse events (“AEs”) reported. |
| • | The most common AEs were dizziness, lightheadedness, headache, and nausea. |
Updated Corporate Presentation
On December 11, 2023, the Company updated its corporate presentation for use on the Company’s conference call on December 11 at 9:30 p.m. ET. A copy of the corporate presentation is filed as Exhibit 99.2 for purposes of Section 18 of the Exchange Act and is incorporated herein by reference.
Cautionary Statement Regarding Forward-Looking Statements
This Current Report on Form 8-K contains “forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995, as amended, including, but not limited to, express or implied statements regarding the Company’s expectations, hopes, beliefs, intentions or strategies with respect to its AURORA Phase 2 and BEACON Phase 2 clinical studies of bitopertin and the results thereof, its Phase 1b/2 clinical studies of DISC-0974 in patients with myelofibrosis and non-dialysis dependent chronic kidney disease patients with anemia, its Phase 1 clinical study of DISC-3405 in healthy volunteers, projected timelines for the initiation and completion of its clinical trials, anticipated timing of release of data and other clinical activities, the Company’s business plans and objectives, the Company’s analysis of market potential for patients with EPP, and the Company’s beliefs about operating expenses and that it will have capital to fund the Company well into 2026. The use of words such as, but not limited to, “anticipate,” “believe,” “contemplate,” “continue,” “could,” “estimate,” “expect,” “future,” “intends,” “may,” “might,” “plan,” “possible,” “potential,” “predict,” “project,” “should,” “seek,” “suggest,” “will,” or “would” or the negative of these terms and other similar words or expressions that are intended to identify forward-looking statements. Forward-looking statements are neither historical facts nor assurances of future performance. Instead, they are based on the Company’s current beliefs, expectations and assumptions regarding the future of the Company’s business, future plans and strategies, clinical results and other future conditions. New risks and uncertainties may emerge from time to time, and it is not possible to predict all risks and uncertainties. No representations or warranties (expressed or implied) are made about the accuracy of any such forward-looking statements.
The Company may not actually achieve the plans, intentions or expectations disclosed in these forward-looking statements, and investors should not place undue reliance on these forward-looking statements. Actual results or events could differ materially from the plans, intentions and expectations disclosed in the forward-looking statements as a result of a number of material risks and uncertainties including but not limited to: the adequacy of the Company’s capital to support its future operations and its ability to successfully initiate and complete clinical trials; the nature, strategy and focus of the Company; the difficulty in predicting the time and cost of development of the Company’s product candidates; the Company’s plans to research, develop and commercialize its current and future product candidates; the timing of initiation of the Company’s planned preclinical studies and clinical trials; the timing of the availability of data from the Company’s clinical trials; the Company’s ability to identify additional product candidates with significant commercial potential and to expand its pipeline in hematological diseases; the timing and anticipated results of the Company’s preclinical studies and clinical trials and the risk that the results of the Company’s preclinical studies and clinical trials may not be predictive of future results in connection with future studies or clinical trials and may not support further development and marketing approval; the other risks and uncertainties described in the “Risk Factors” section of our Quarterly Report on Form 10-Q for the quarter ended September 30, 2023, and other documents filed by the Company from time to time with the Securities and Exchange Commission (“SEC”), as well as discussions of potential risks, uncertainties, and other important factors in the Company’s subsequent filings with the SEC. Any forward-looking statement speaks only as of the date on which it was made. None of the Company, nor its affiliates, advisors or representatives, undertake any obligation to publicly update or revise any forward-looking statement, whether as result of new information, future events or otherwise, except as required by law.
| Item 9.01 | Financial Statements and Exhibits. |
(d) Exhibits
| Exhibit No. |
Description |
|
| 99.1 | Press Release issued by Disc Medicine, Inc. on December 11, 2023. | |
| 99.2 | Disc Medicine, Inc. Investor Presentation. | |
| 104 | Cover Page Interactive Data File (embedded within the Inline XBRL document). | |
SIGNATURE
Pursuant to the requirements of the Securities Exchange Act of 1934, as amended, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
| DISC MEDICINE, INC. | ||||||
| Date: December 11, 2023 | By: | /s/ John Quisel |
||||
| Name: | John Quisel, J.D. Ph.D. | |||||
| Title: | Chief Executive Officer | |||||
Exhibit 99.1

Disc Presents Positive Updated Results from Phase 2 BEACON Study of Bitopertin and Other Programs at the 65th American Society of Hematology (ASH) Annual Meeting
| • | Updated data from BEACON continued to demonstrate significant, consistent reductions in protoporphyrin IX (PPIX) > 40% and improvements in sunlight tolerance |
| • | Robust and consistent improvements across all measures of sunlight tolerance, including >3x improvement over historical control of precedented pivotal endpoint |
| • | Bitopertin was generally well-tolerated with stable hemoglobin at both dose levels |
| • | Earlier today, Disc also announced initial positive data from the phase 1b study of DISC-0974 in myelofibrosis patients with anemia, demonstrating improvements in hemoglobin and reductions in transfusion burden |
WATERTOWN, Mass. (December 11, 2023) – Disc Medicine, Inc. (NASDAQ:IRON), a clinical-stage biopharmaceutical company focused on the discovery, development, and commercialization of novel treatments for patients suffering from serious hematologic diseases, today presented updated results from the phase 2 open-label BEACON study of bitopertin, an orally administered glycine transporter 1 (GlyT1) inhibitor, in patients with erythropoietic protoporphyria (EPP) as an oral presentation at the 65th ASH Annual Meeting. The updated data are consistent with and confirm the initial positive results presented in June, demonstrating significant decreases in PPIX, robust and consistent improvements in sunlight tolerance across all study measures, including the precedented pivotal endpoint, and improvements in patient quality of life.
“This has been a tremendous ASH meeting for Disc, as we presented data across our two most advanced programs. We are especially proud and excited to present the updated results from BEACON, which reflect a more robust open label data set and clearly indicate that reducing PPIX with bitopertin has the potential to result in dramatic benefits for patients with EPP. Importantly, this improvement was observed across every efficacy measure of the study, including our analysis of the precedented pivotal endpoint, cumulative time in light over 6 months, which we debuted at this meeting,” said John Quisel, J.D., Ph.D., President and Chief Executive Officer. “With these results and the positive initial efficacy data from the DISC-0974 myelofibrosis study that we presented earlier today, Disc is preparing to enter its next stage of growth. We look forward to next year as we advance our full portfolio and obtain the readouts from AURORA and other studies.”
The BEACON study (ACTRN12622000799752) is a randomized, open-label, parallel-arm study that enrolled 22 adult subjects with EPP or X-linked protoporphyria (XLP) in Australia, and has been expanded to include adolescents. This trial was designed to assess changes in levels of PPIX, as well as measures of photosensitivity, quality of life, and safety and tolerability. Subjects are randomized to receive either 20 mg or 60 mg of bitopertin once-daily for 24 weeks, after which patients have the option of continuing in an open-label extension of the trial for up to an additional 24 weeks. The updated data presented reflects results from all 22 adults, with a data cutoff of September 18, 2023 for PPIX data and October 20, 2023 for all other endpoints. The data are consistent with and confirm the initial positive results presented in June 2023.
| • | Protoporphyrin IX (PPIX) levels: Significant, dose-dependent, and sustained reductions in whole blood PPIX levels; mean reduction > 40% (p<0.001 versus baseline) |
| • | Demonstrated substantial and consistent improvements in sunlight tolerance across all study measures |
| • | Highlights of the data presented: |
| • | Average time to prodrome: Greater than 3x improvement vs. baseline (p<0.001) |
| • | Increased proportion of days without symptoms: 78% vs. 33% (baseline) |
| • | Increased proportion of sunlight challenges without prodromes: 54% vs. 7% (baseline) |
| • | Phototoxic reactions: 92% reduction in patient-reported reactions while on treatment compared to baseline |
| • | Nearly all participants reported improvements in multiple quality-of-life measures at the end of study |
| • | Mean cumulative total time in light on days without pain observed over the 6-month treatment period (precedented pivotal endpoint): 222.6 + 129.3 hours |
| • | Bitopertin-treated participants had a >3x increase relative to historical control |
| • | Bitopertin was generally well tolerated at both dose levels with no serious adverse events, stable mean hemoglobin levels, and no anemia adverse events (AEs) reported. |
| • | The most common AEs were dizziness, lightheadedness, headache, and nausea. |
Earlier today, Disc also presented initial positive data from the ongoing phase 1b study of DISC-0974 in myelofibrosis (MF) patients with anemia. The data were presented as a poster during the ASH meeting and demonstrated suppression of hepcidin, increased iron levels and improvements in hematologic parameters, including increased hemoglobin and reduction in transfusion burden. The presentation was announced in a separate press release issued earlier today and will be reviewed again during the management call, as well as initial data from the first dose-escalation cohort of the ongoing phase 1b/2 study in non-dialysis dependent chronic kidney disease (NDD-CKD) patients with anemia.
Bitopertin and DISC-0974 are investigational agents and are not approved for use as a therapy in any jurisdiction worldwide.
Webcast Conference Call Information
Management will host a call on Monday, December 11th at 9:30 pm ET / 6:30 pm PT to review data and operational plans. Please register for management’s webcast on the Events and Presentations page of Disc’s website (https://ir.discmedicine.com/).
About Disc Medicine
Disc Medicine is a clinical-stage biopharmaceutical company committed to discovering, developing, and commercializing novel treatments for patients who suffer from serious hematologic diseases. We are building a portfolio of innovative, potentially first-in-class therapeutic candidates that aim to address a wide spectrum of hematologic diseases by targeting fundamental biological pathways of red blood cell biology, specifically heme biosynthesis and iron homeostasis. For more information, please visit www.discmedicine.com.
Disc Medicine Cautionary Statement Regarding Forward-Looking Statements
This press release contains “forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995, as amended, including, but not limited to, express or implied statements regarding Disc’s expectations, hopes, beliefs, intentions or strategies with respect to its AURORA Phase 2 and BEACON Phase 2 clinical studies of bitopertin and the results thereof, its Phase 1b/2 clinical studies of DISC-0974 in patients with MF and NDD-CKD patients with anemia, its Phase 1 clinical study of DISC-3405 in healthy volunteers, projected timelines for the initiation and completion of its clinical trials, anticipated timing of release of data and other clinical activities, Disc’s business plans and objectives, Disc’s analysis of market potential for patients with EPP, and Disc’s beliefs about operating expenses and that it will have capital to fund Disc well into 2026. The use of words such as, but not limited to, “anticipate,” “believe,” “contemplate,” “continue,” “could,” “estimate,” “expect,” “future,” “intends,” “may,” “might,” “plan,” “possible,” “potential,” “predict,” “project,” “should,” “seek,” “suggest,” “will,” or “would” or the negative of these terms and other similar words or expressions that are intended to identify forward-looking statements. Forward-looking statements are neither historical facts nor assurances of future performance. Instead, they are based on Disc’s current beliefs, expectations and assumptions regarding the future of Disc’s business, future plans and strategies, clinical results and other future conditions. New risks and uncertainties may emerge from time to time, and it is not possible to predict all risks and uncertainties. No representations or warranties (expressed or implied) are made about the accuracy of any such forward-looking statements.
Disc may not actually achieve the plans, intentions or expectations disclosed in these forward-looking statements, and investors should not place undue reliance on these forward-looking statements. Actual results or events could differ materially from the plans, intentions and expectations disclosed in the forward-looking statements as a result of a number of material risks and uncertainties including but not limited to: the adequacy of Disc’s capital to support its future operations and its ability to successfully initiate and complete clinical trials; the nature, strategy and focus of Disc; the difficulty in predicting the time and cost of development of Disc’s product candidates; Disc’s plans to research, develop and commercialize its current and future product candidates; the timing of initiation of Disc’s planned preclinical studies and clinical trials; the timing of the availability of data from Disc’s clinical trials; Disc’s ability to identify additional product candidates with significant commercial potential and to expand its pipeline in hematological diseases; the timing and anticipated results of Disc’s preclinical studies and clinical trials and the risk that the results of Disc’s preclinical studies and clinical trials may not be predictive of future results in connection with future studies or clinical trials and may not support further development and marketing approval; the other risks and uncertainties described in the “Risk Factors” section of our Quarterly Report on Form 10-Q for the quarter ended September 30, 2023, and other documents filed by Disc from time to time with the Securities and Exchange Commission (SEC), as well as discussions of potential risks, uncertainties, and other important factors in Disc’s subsequent filings with the SEC. Any forward-looking statement speaks only as of the date on which it was made. None of Disc, nor its affiliates, advisors or representatives, undertake any obligation to publicly update or revise any forward-looking statement, whether as result of new information, future events or otherwise, except as required by law.
Media Contact
Peg Rusconi
Verge Scientific Communications
prusconi@vergescientific.com
Investor Relations Contact
Christina Tartaglia
Stern Investor Relations
christina.tartaglia@sternir.com

Exhibit 99.2 2023 ASH Management Call Clinical Data Updates: Bitopertin and DISC-0974 December 11, 2023
Disclaimer and FLS This presentation includes “forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995, as amended. These forward-looking statements include express or implied statements relating to Disc's management team's expectations, hopes, beliefs, intentions or strategies regarding Disc’s expectations with respect to its AURORA Phase 2 and BEACON Phase 2 clinical studies of bitopertin and the results thereof, its Phase 1b/2 clinical studies of DISC-0974 in patients with MF and NDD-CKD patients with anemia, its Phase 1 clinical study of DISC-3405 in healthy volunteers; projected timelines for the initiation and completion of its clinical trials, anticipated timing of release of data, and other clinical activities; Disc’s business plans and objectives; Disc's analysis of market potential for patients with EPP; and Disc’s beliefs about operating expenses and that it will have capital to fund Disc well into 2026. In addition, any statements that refer to projections, forecasts or other characterizations of future events or circumstances, including any underlying assumptions, are forward-looking statements. The words “anticipate,” “believe,” “contemplate,” “continue,” “could,” “estimate,” “expect,” “intends,” “may,” “might,” “plan,” “possible,” “potential,” “predict,” “project,” “should,” “suggest,” “will,” “would” and similar expressions may identify forward-looking statements, but the absence of these words does not mean that a statement is not forward-looking. Forward-looking statements are neither historical facts nor assurances of future performance. Instead, they are based on Disc's current beliefs, expectations and assumptions regarding the future of Disc's business, future plans and strategies, clinical results and other future conditions. New risks and uncertainties may emerge from time to time, and it is not possible to predict all risks and uncertainties. No representations or warranties (expressed or implied) are made about the accuracy of any such forward-looking statements. Disc may not actually achieve the plans, intentions or expectations disclosed in these forward-looking statements, and investors should not place undue reliance on these forward-looking statements. These forward-looking statements involve a number of risks, uncertainties (some of which are beyond Disc's control) or other assumptions that may cause actual results or performance to be materially different from those expressed or implied by these forward-looking statements. These risks and uncertainties include, but are not limited to: the adequacy of Disc's capital to support its future operations and its ability to successfully initiate and complete clinical trials; the nature, strategy and focus of Disc; the difficulty in predicting the time and cost of development of Disc's product candidates; Disc's plans to research, develop and commercialize its current and future product candidates; the timing of initiation of Disc's planned preclinical studies and clinical trials; the timing of the availability of data from Disc's clinical trials; Disc's ability to identify additional product candidates with significant commercial potential and to expand its pipeline in hematological diseases; the timing and anticipated results of Disc's preclinical studies and clinical trials and the risk that the results of Disc's preclinical studies and clinical trials may not be predictive of future results in connection with future studies or clinical trials and may not support further development and marketing approval; the other risks and uncertainties described in our Annual Report on Form 10-K for the year ended December 31, 2022, Quarterly Reports on Form 10-Q for the quarters ended March 31, 2023, June 30, 2023 and September 30, 2023, and other documents filed by Disc from time to time with the Securities and Exchange Commission. Any forward-looking statement speaks only as of the date on which it was made. None of Disc, nor its affiliates, advisors or representatives, undertake any obligation to publicly update or revise any forward-looking statement, whether as result of new information, future events or otherwise, except as required by law.
Bitopertin and DISC-0974 are investigational agents and are not approved for use as therapies in any jurisdiction worldwide CONFIDENTIAL 3
Agenda Introduction and Data Summary 01 John Quisel, JD, PhD, Chief Executive Officer Bitopertin in EPP 02 • Updated BEACON Data Bruce Wang, MD, Professor of Gastroenterology, University of California San Francisco Will Savage, MD, PhD, Chief Medical Officer • EPP Commercial Opportunity Jonathan Yu, Chief Business Officer DISC-0974 03 • Initial Data in Anemia of Myelofibrosis Will Savage, MD, PhD, Chief Medical Officer • Initial Data in NDD-CKD and Anemia Will Savage, MD, PhD, Chief Medical Officer Closing Remarks 04 John Quisel, JD, PhD, Chief Executive Officer Q&A Session 05 4
Bitopertin: Summary of Phase 2 BEACON Data Update Data presented at ASH established proof of concept and demonstrated functional benefit for EPP patients. Key findings: Significant, dose- Significant Improved patients’ Generally well dependent increases in reported quality tolerated with stable reductions in sunlight tolerance of life mean hemoglobin PPIX levels levels 5
DISC-0974: Summary of Initial Data from Phase 1b Studies in MF and CKD Initial data from both Phase 1b studies in MF and CKD demonstrated proof of concept and improvement in anemia. Key findings: Substantial Corresponding Positive impact on Generally well reductions in increases in iron tolerated at all hematologic hepcidin levels levels parameters across evaluated dose a broad range of levels MF patients 6
Agenda Introduction and Data Summary 01 John Quisel, JD, PhD, Chief Executive Officer Bitopertin in EPP 02 • Updated BEACON Data Bruce Wang, MD, Professor of Gastroenterology, University of California San Francisco Will Savage, MD, PhD, Chief Medical Officer • EPP Commercial Opportunity Jonathan Yu, Chief Business Officer DISC-0974 03 • Initial Data in Anemia of Myelofibrosis Will Savage, MD, PhD, Chief Medical Officer • Initial Data in NDD-CKD and Anemia Will Savage, MD, PhD, Chief Medical Officer Closing Remarks 04 John Quisel, JD, PhD, Chief Executive Officer Q&A Session 05 7
Bruce Wang, MD Disclosures • Alnylam (consultant, investigator in clinical trial, grant funding) Principal • Disc Medicine (consultant, Investigator in investigator in clinical trial) Professor at UCSF • US Porphyrias Mitsubishi-Tanabe (consultant, investigator in clinical trial, grant Consortium funding) • Recordati Rare Diseases (consultant) 8
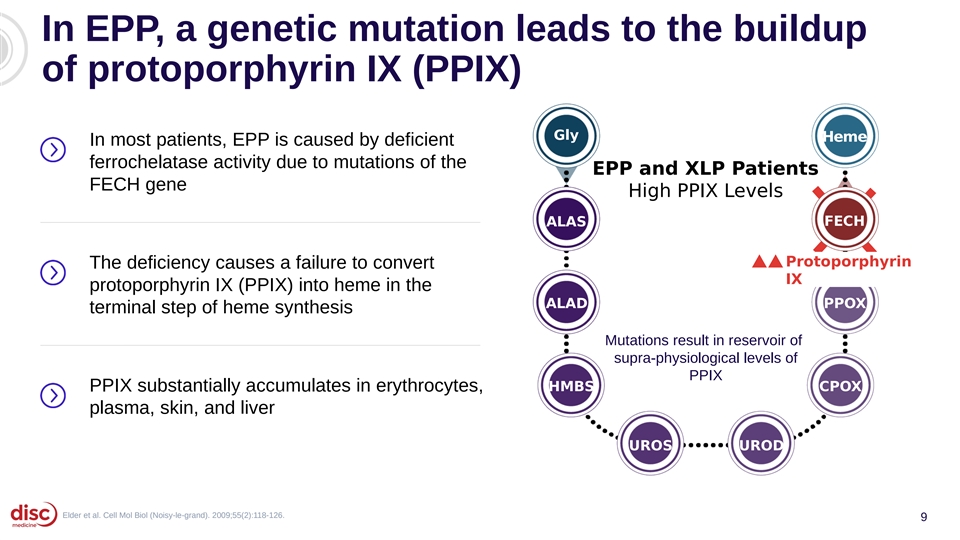
In EPP, a genetic mutation leads to the buildup of protoporphyrin IX (PPIX) Gly Heme In most patients, EPP is caused by deficient ferrochelatase activity due to mutations of the EPP and XLP Patients FECH gene High PPIX Levels ALAS FECH Protoporphyrin The deficiency causes a failure to convert IX protoporphyrin IX (PPIX) into heme in the ALAD PPOX terminal step of heme synthesis Mutations result in reservoir of supra-physiological levels of PPIX PPIX substantially accumulates in erythrocytes, HMBS CPOX plasma, skin, and liver UROS UROD Elder et al. Cell Mol Biol (Noisy-le-grand). 2009;55(2):118-126. 9
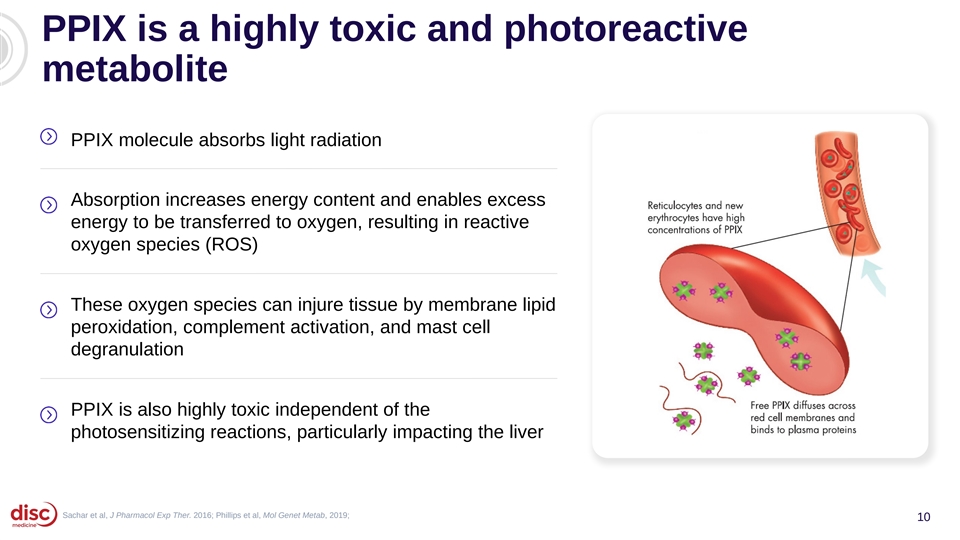
PPIX is a highly toxic and photoreactive metabolite PPIX molecule absorbs light radiation Absorption increases energy content and enables excess energy to be transferred to oxygen, resulting in reactive oxygen species (ROS) These oxygen species can injure tissue by membrane lipid peroxidation, complement activation, and mast cell degranulation PPIX is also highly toxic independent of the photosensitizing reactions, particularly impacting the liver Sachar et al, J Pharmacol Exp Ther. 2016; Phillips et al, Mol Genet Metab, 2019; 10
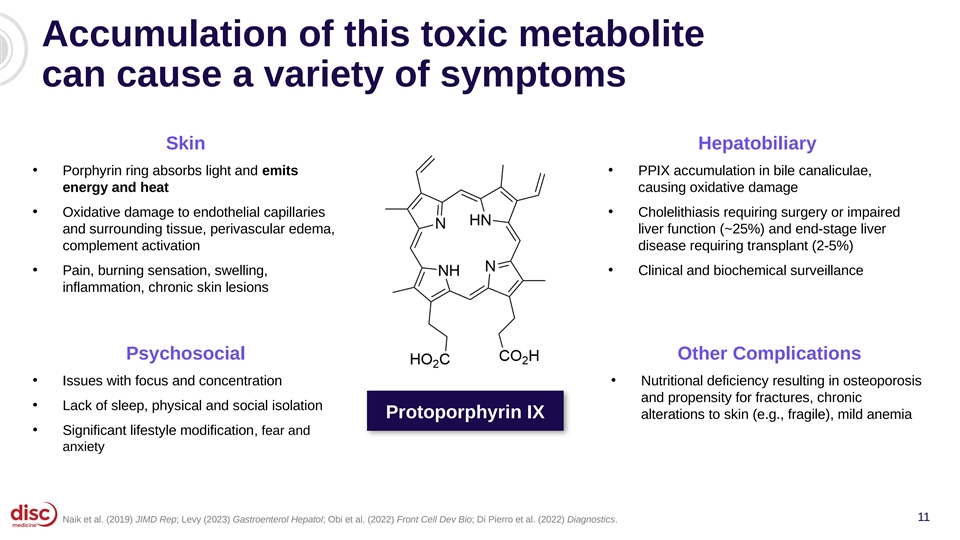
Accumulation of this toxic metabolite can cause a variety of symptoms Skin Hepatobiliary • • Porphyrin ring absorbs light and emits PPIX accumulation in bile canaliculae, energy and heat causing oxidative damage • • Oxidative damage to endothelial capillaries Cholelithiasis requiring surgery or impaired and surrounding tissue, perivascular edema, liver function (~25%) and end-stage liver complement activation disease requiring transplant (2-5%) • Pain, burning sensation, swelling, • Clinical and biochemical surveillance inflammation, chronic skin lesions Psychosocial Other Complications • Issues with focus and concentration • Nutritional deficiency resulting in osteoporosis and propensity for fractures, chronic • Lack of sleep, physical and social isolation Protoporphyrin IX alterations to skin (e.g., fragile), mild anemia • Significant lifestyle modification, fear and anxiety 11 Naik et al. (2019) JIMD Rep; Levy (2023) Gastroenterol Hepatol; Obi et al. (2022) Front Cell Dev Bio; Di Pierro et al. (2022) Diagnostics.
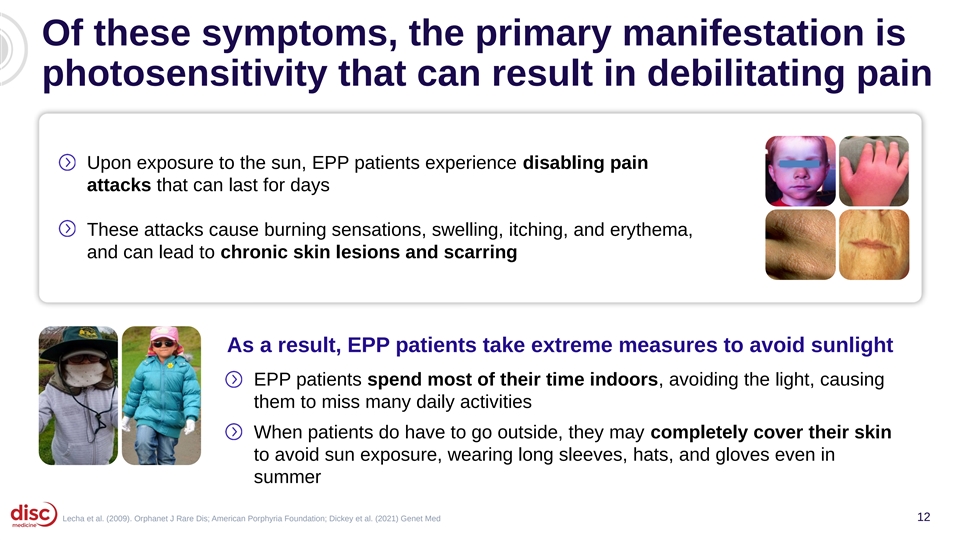
Of these symptoms, the primary manifestation is photosensitivity that can result in debilitating pain Upon exposure to the sun, EPP patients experience disabling pain attacks that can last for days These attacks cause burning sensations, swelling, itching, and erythema, and can lead to chronic skin lesions and scarring As a result, EPP patients take extreme measures to avoid sunlight EPP patients spend most of their time indoors, avoiding the light, causing them to miss many daily activities When patients do have to go outside, they may completely cover their skin to avoid sun exposure, wearing long sleeves, hats, and gloves even in summer Lecha et al. (2009). Orphanet J Rare Dis; American Porphyria Foundation; Dickey et al. (2021) Genet Med 12
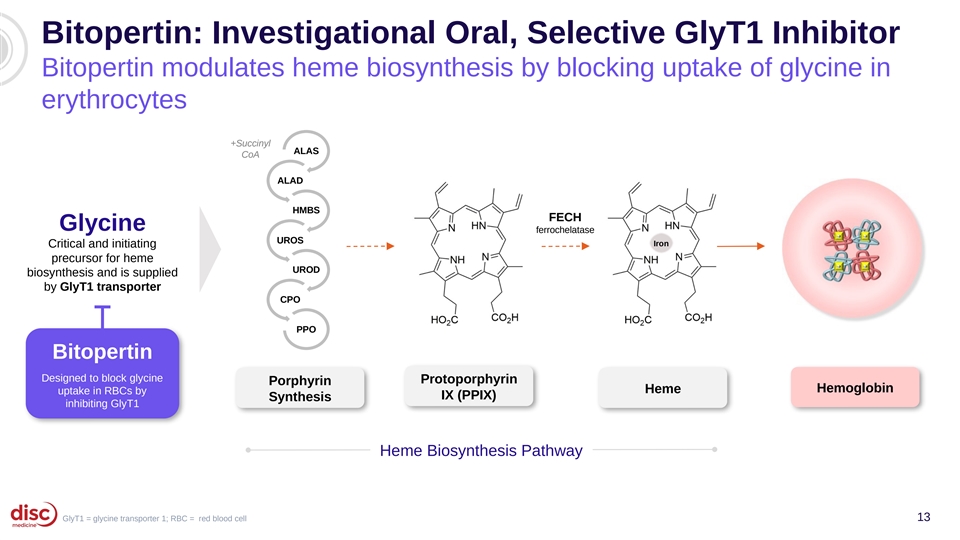
Bitopertin: Investigational Oral, Selective GlyT1 Inhibitor Bitopertin modulates heme biosynthesis by blocking uptake of glycine in erythrocytes +Succinyl ALAS CoA ALAD HMBS FECH Glycine ferrochelatase UROS Iron Critical and initiating precursor for heme UROD biosynthesis and is supplied by GlyT1 transporter CPO PPO Bitopertin Designed to block glycine Protoporphyrin Porphyrin Hemoglobin Heme uptake in RBCs by IX (PPIX) Synthesis inhibiting GlyT1 Heme Biosynthesis Pathway GlyT1 = glycine transporter 1; RBC = red blood cell 13
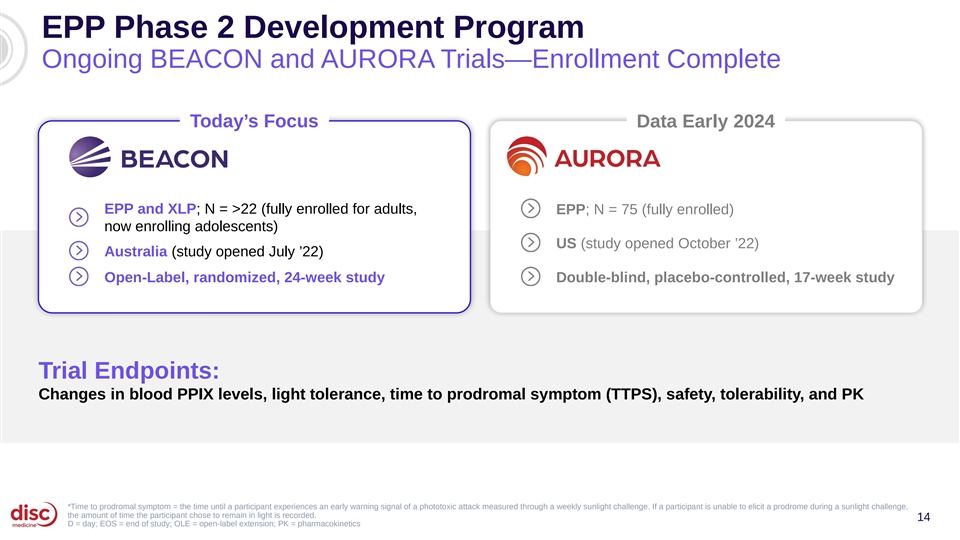
EPP Phase 2 Development Program Ongoing BEACON and AURORA Trials—Enrollment Complete Today’s Focus Data Early 2024 EPP and XLP; N = >22 (fully enrolled for adults, EPP; N = 75 (fully enrolled) now enrolling adolescents) US (study opened October ’22) Australia (study opened July ’22) Open-Label, randomized, 24-week study Double-blind, placebo-controlled, 17-week study Trial Endpoints: Changes in blood PPIX levels, light tolerance, time to prodromal symptom (TTPS), safety, tolerability, and PK *Time to prodromal symptom = the time until a participant experiences an early warning signal of a phototoxic attack measured through a weekly sunlight challenge. If a participant is unable to elicit a prodrome during a sunlight challenge, the amount of time the participant chose to remain in light is recorded. 14 D = day; EOS = end of study; OLE = open-label extension; PK = pharmacokinetics
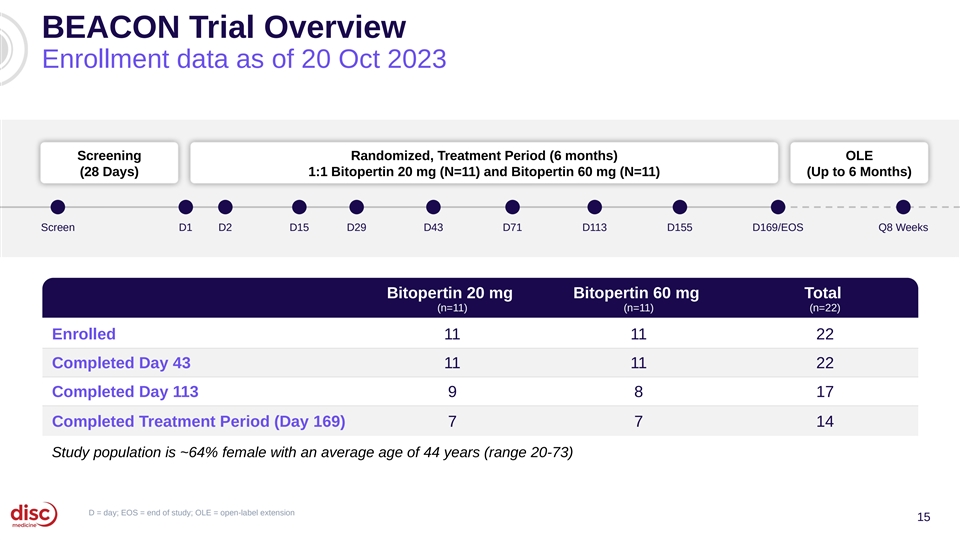
BEACON Trial Overview Enrollment data as of 20 Oct 2023 Screening Randomized, Treatment Period (6 months) OLE (28 Days) 1:1 Bitopertin 20 mg (N=11) and Bitopertin 60 mg (N=11) (Up to 6 Months) Screen D1 D2 D15 D29 D43 D71 D113 D155 D169/EOS Q8 Weeks Bitopertin 20 mg Bitopertin 60 mg Total (n=11) (n=11) (n=22) Enrolled 11 11 22 Completed Day 43 11 11 22 Completed Day 113 9 8 17 Completed Treatment Period (Day 169) 7 7 14 Study population is ~64% female with an average age of 44 years (range 20-73) D = day; EOS = end of study; OLE = open-label extension 15
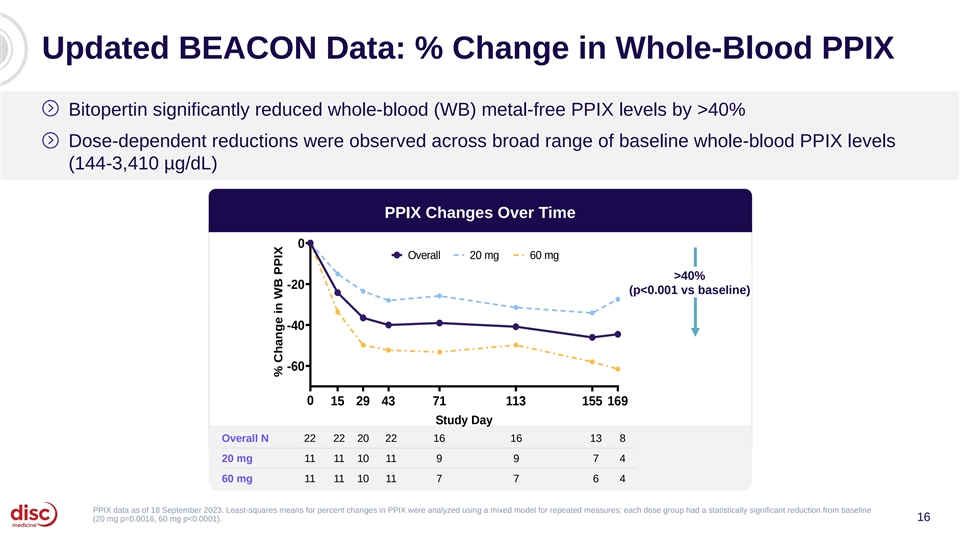
Updated BEACON Data: % Change in Whole-Blood PPIX Bitopertin significantly reduced whole-blood (WB) metal-free PPIX levels by >40% Dose-dependent reductions were observed across broad range of baseline whole-blood PPIX levels (144-3,410 µg/dL) PPIX Changes Over Time 0 Overall 20 mg 60 mg >40% -20 (p<0.001 vs baseline) -40 -60 0 15 29 43 71 113 155 169 Study Day Overall N 22 22 20 22 16 16 13 8 20 mg 11 11 10 11 9 9 7 4 60 mg 11 11 10 11 7 7 6 4 PPIX data as of 18 September 2023. Least-squares means for percent changes in PPIX were analyzed using a mixed model for repeated measures; each dose group had a statistically significant reduction from baseline (20 mg p=0.0016, 60 mg p<0.0001). 16 % Change in WB PPIX
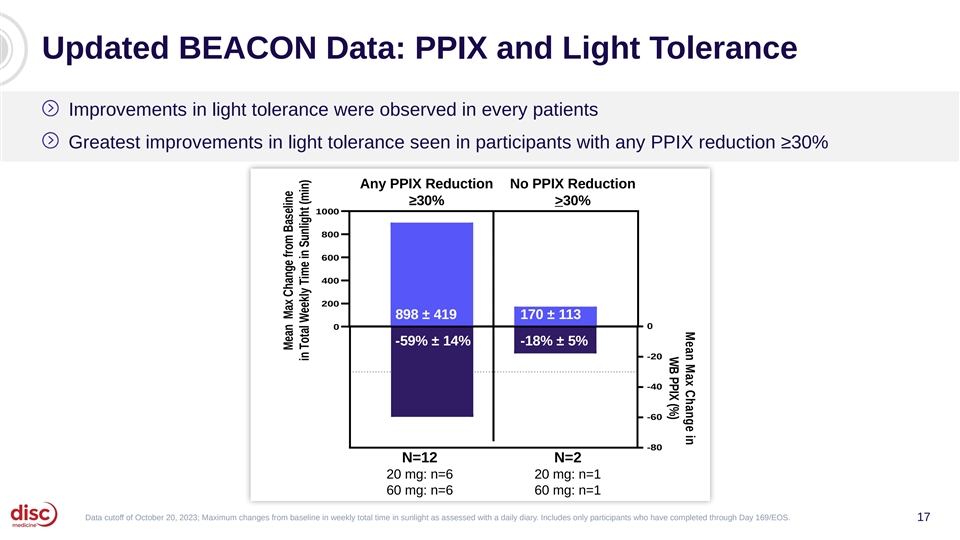
Mean Max Change in WB PPIX (%) Updated BEACON Data: PPIX and Light Tolerance Improvements in light tolerance were observed in every patients Greatest improvements in light tolerance seen in participants with any PPIX reduction ≥30% Any PPIX Reduction No PPIX Reduction ≥30% >30% 1000 800 600 400 N=11 200 898 ± 419 170 ± 113 0 0 -59% ± 14% -18% ± 5% -20 -40 -60 -80 N=12 N=2 20 mg: n=6 20 mg: n=1 60 mg: n=6 60 mg: n=1 Data cutoff of October 20, 2023; Maximum changes from baseline in weekly total time in sunlight as assessed with a daily diary. Includes only participants who have completed through Day 169/EOS. 17 Mean Max Change from Baseline in Total Weekly Time in Sunlight (min)
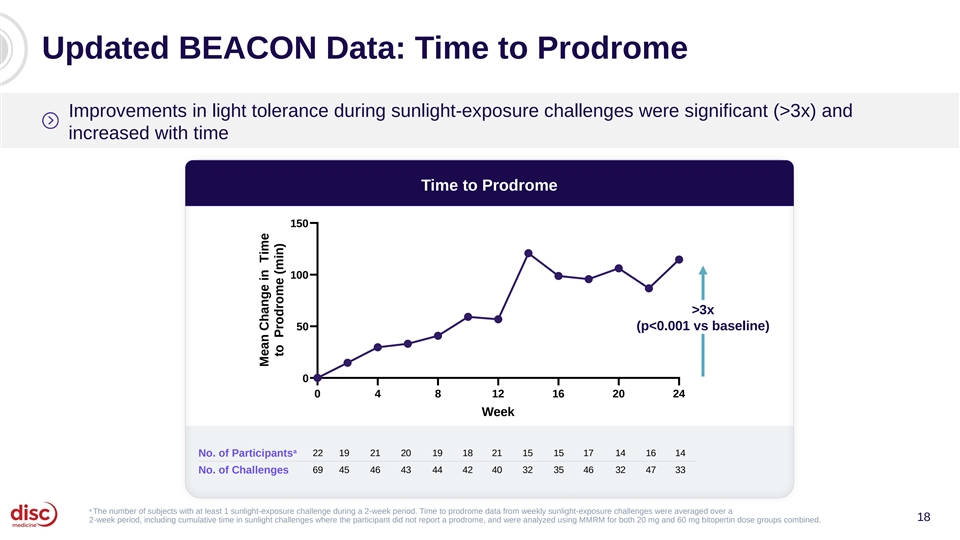
Updated BEACON Data: Time to Prodrome Improvements in light tolerance during sunlight-exposure challenges were significant (>3x) and increased with time Time to Prodrome 150 100 >3x 50 (p<0.001 vs baseline) 0 0 4 8 12 16 20 24 Week a 22 19 21 20 19 18 21 15 15 17 14 16 14 No. of Participants No. of Challenges 69 45 46 43 44 42 40 32 35 46 32 47 33 a The number of subjects with at least 1 sunlight-exposure challenge during a 2-week period. Time to prodrome data from weekly sunlight-exposure challenges were averaged over a 18 2-week period, including cumulative time in sunlight challenges where the participant did not report a prodrome, and were analyzed using MMRM for both 20 mg and 60 mg bitopertin dose groups combined. Mean Change in Time to Prodrome (min)
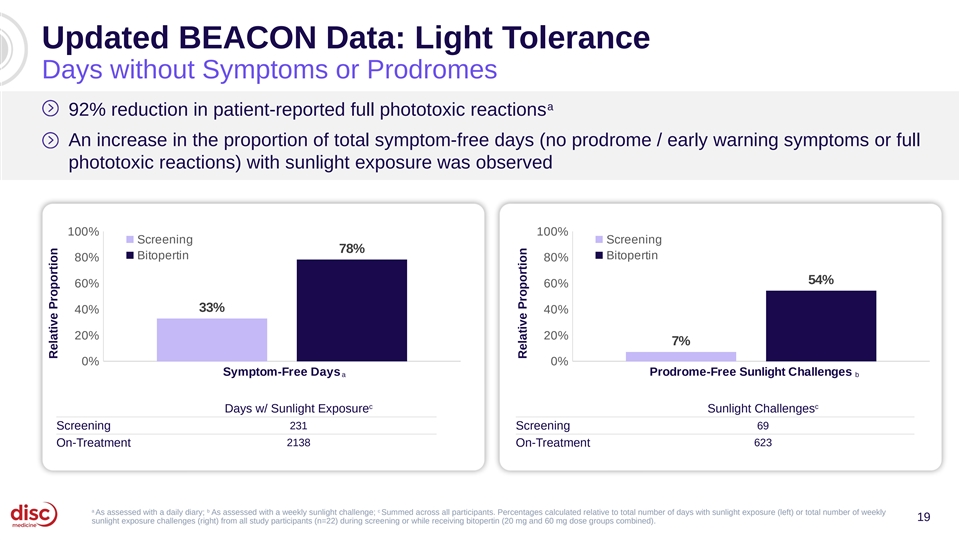
Updated BEACON Data: Light Tolerance Days without Symptoms or Prodromes a 92% reduction in patient-reported full phototoxic reactions An increase in the proportion of total symptom-free days (no prodrome / early warning symptoms or full phototoxic reactions) with sunlight exposure was observed 100% 100% Screening Screening 78% Bitopertin Bitopertin 80% 80% 54% 60% 60% 33% 40% 40% 20% 20% 7% 0% 0% Symptom-Free Days Prodrome-Free Sunlight Challenges a b c c Days w/ Sunlight Exposure Sunlight Challenges Screening 231 Screening 69 On-Treatment 2138 On-Treatment 623 a b c As assessed with a daily diary; As assessed with a weekly sunlight challenge; Summed across all participants. Percentages calculated relative to total number of days with sunlight exposure (left) or total number of weekly 19 sunlight exposure challenges (right) from all study participants (n=22) during screening or while receiving bitopertin (20 mg and 60 mg dose groups combined). Relative Proportion Relative Proportion
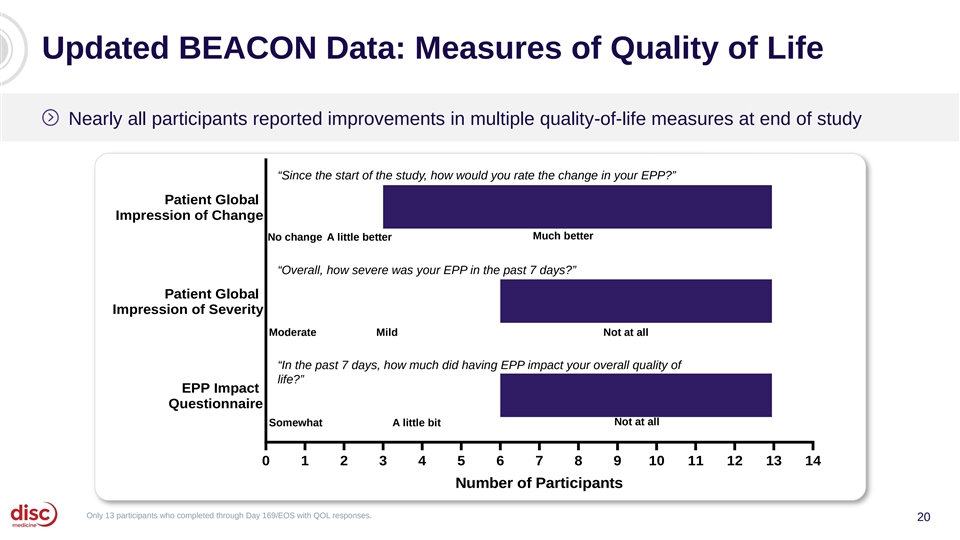
Updated BEACON Data: Measures of Quality of Life Nearly all participants reported improvements in multiple quality-of-life measures at end of study “Since the start of the study, how would you rate the change in your EPP?” Patient Global Impression of Change Much better No change A little better “Overall, how severe was your EPP in the past 7 days?” Patient Global Impression of Severity Moderate Mild Not at all “In the past 7 days, how much did having EPP impact your overall quality of life?” EPP Impact Questionnaire Not at all Somewhat A little bit 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Number of Participants Only 13 participants who completed through Day 169/EOS with QOL responses. 20

Updated BEACON Data: Precedented Pivotal Endpoint Cumulative Time in Light on Days without Pain Cumulative total time in light observed over 6-month treatment period with bitopertin represents >3x increase relative to historical control Improvements in average daily light tolerance with bitopertin increased with time Cumulative Time in Light Without Pain Over 6 Months (hours) ± 129.3 222.6 Mean ± 60.6 60.6 +SD 178.2 Median 40.8 0 50 100 150 200 250 b a Bitopertin (n=14) Historical Control (n=43) a b Placebo arm from prior Phase 3 study in EPP (Langendonk et al. [2015] NEJM). Includes data from participants who completed EOS visit (D169). Cumulative time in light measured via daily diary, adding all time in light between the hours of 10 am and 6 pm on days without any pain or prodrome; SD = standard deviation 21
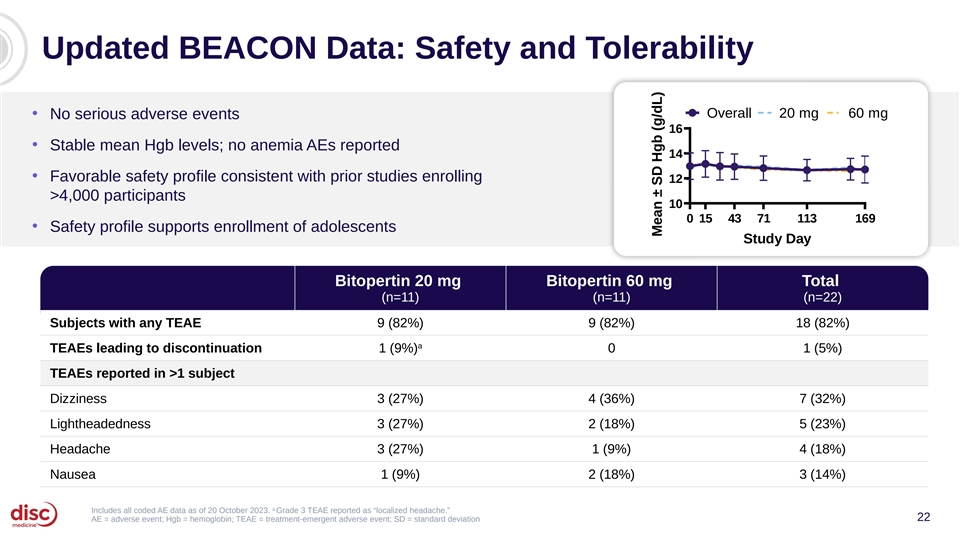
Updated BEACON Data: Safety and Tolerability Overall 20 mg 60 mg • No serious adverse events 16 • Stable mean Hgb levels; no anemia AEs reported 14 • Favorable safety profile consistent with prior studies enrolling 12 >4,000 participants 10 0 15 43 71 113 169 • Safety profile supports enrollment of adolescents Study Day Bitopertin 20 mg Bitopertin 60 mg Total (n=11) (n=11) (n=22) Subjects with any TEAE 9 (82%) 9 (82%) 18 (82%) a TEAEs leading to discontinuation 1 (9%) 0 1 (5%) TEAEs reported in >1 subject Dizziness 3 (27%) 4 (36%) 7 (32%) Lightheadedness 3 (27%) 2 (18%) 5 (23%) Headache 3 (27%) 1 (9%) 4 (18%) Nausea 1 (9%) 2 (18%) 3 (14%) a Includes all coded AE data as of 20 October 2023. Grade 3 TEAE reported as “localized headache.” 22 AE = adverse event; Hgb = hemoglobin; TEAE = treatment-emergent adverse event; SD = standard deviation Mean ± SD Hgb (g/dL)
Key Takeaways from Updated BEACON Data Proof of Functional Quality of Life Safety Concept Outcomes Impact Significant Significant Patients reported Generally well reduction in PPIX improvement in an improved tolerated and no at low and high sunlight tolerance, quality of life meaningful doses including on change in precedented hemoglobin pivotal endpoint observed with bitopertin 23
Agenda Introduction and Data Summary 01 John Quisel, JD, PhD, Chief Executive Officer Bitopertin in EPP 02 • Updated BEACON Data Bruce Wang, MD, Professor of Gastroenterology, University of California San Francisco Will Savage, MD, PhD, Chief Medical Officer • EPP Commercial Opportunity Jonathan Yu, Chief Business Officer DISC-0974 03 • Initial Data in Anemia of Myelofibrosis Will Savage, MD, PhD, Chief Medical Officer • Initial Data in NDD-CKD and Anemia Will Savage, MD, PhD, Chief Medical Officer Closing Remarks 04 John Quisel, JD, PhD, Chief Executive Officer Q&A Session 05 24
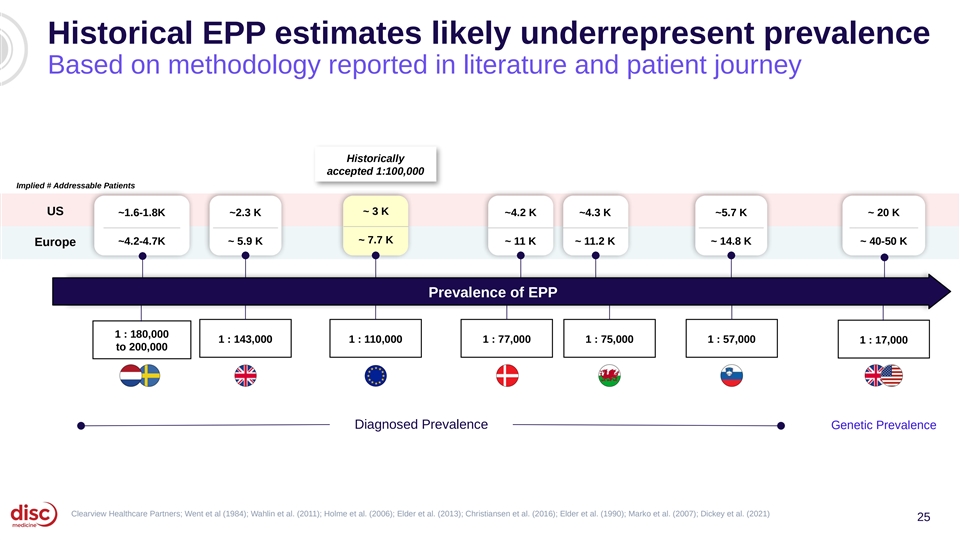
Historical EPP estimates likely underrepresent prevalence Based on methodology reported in literature and patient journey Historically accepted 1:100,000 Implied # Addressable Patients ~ 3 K US ~1.6-1.8K ~2.3 K ~4.2 K ~4.3 K ~5.7 K ~ 20 K ~ 7.7 K ~4.2-4.7K ~ 5.9 K ~ 11 K ~ 11.2 K ~ 14.8 K ~ 40-50 K Europe Prevalence of EPP 1 : 180,000 1 : 143,000 1 : 110,000 1 : 77,000 1 : 75,000 1 : 57,000 1 : 17,000 to 200,000 Diagnosed Prevalence Genetic Prevalence Clearview Healthcare Partners; Went et al (1984); Wahlin et al. (2011); Holme et al. (2006); Elder et al. (2013); Christiansen et al. (2016); Elder et al. (1990); Marko et al. (2007); Dickey et al. (2021) 25
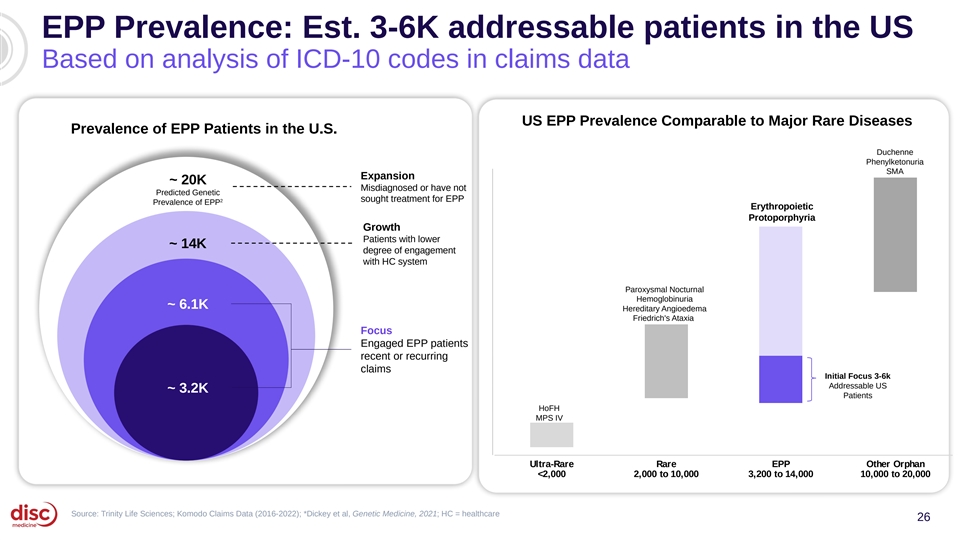
EPP Prevalence: Est. 3-6K addressable patients in the US Based on analysis of ICD-10 codes in claims data US EPP Prevalence Comparable to Major Rare Diseases Prevalence of EPP Patients in the U.S. Duchenne Phenylketonuria SMA Expansion ~ 20K Misdiagnosed or have not Predicted Genetic 2 sought treatment for EPP Prevalence of EPP Erythropoietic Protoporphyria Growth Patients with lower ~ 14K degree of engagement with HC system Paroxysmal Nocturnal Hemoglobinuria ~ 6.1K Hereditary Angioedema Friedrich's Ataxia Focus Engaged EPP patients recent or recurring claims Initial Focus 3-6k Addressable US ~ 3.2K Patients HoFH MPS IV Ultra-Rare Rare EPP Other Orphan <2,000 2,000 to 10,000 3,200 to 14,000 10,000 to 20,000 Source: Trinity Life Sciences; Komodo Claims Data (2016-2022); *Dickey et al, Genetic Medicine, 2021; HC = healthcare 26
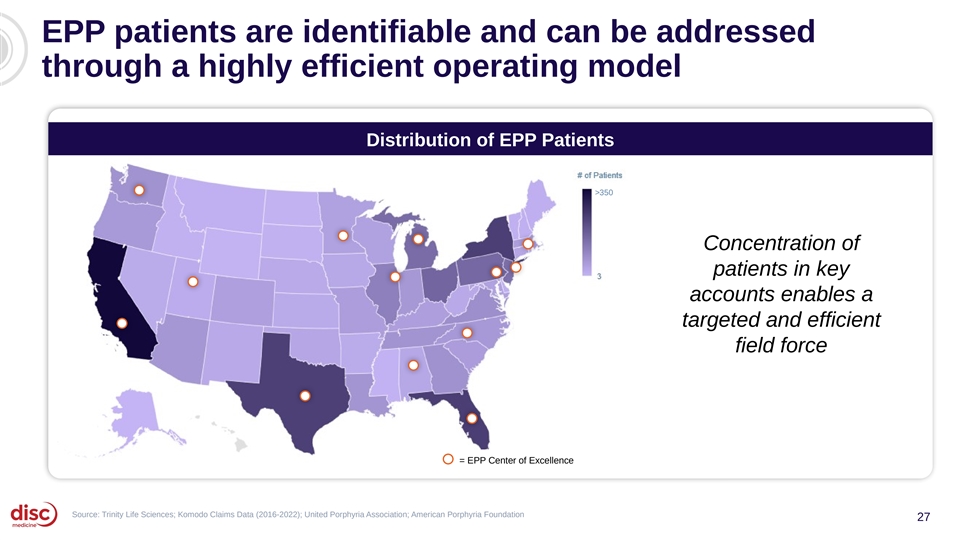
EPP patients are identifiable and can be addressed through a highly efficient operating model Distribution of EPP Patients >350 Concentration of patients in key accounts enables a targeted and efficient field force = EPP Center of Excellence Source: Trinity Life Sciences; Komodo Claims Data (2016-2022); United Porphyria Association; American Porphyria Foundation 27
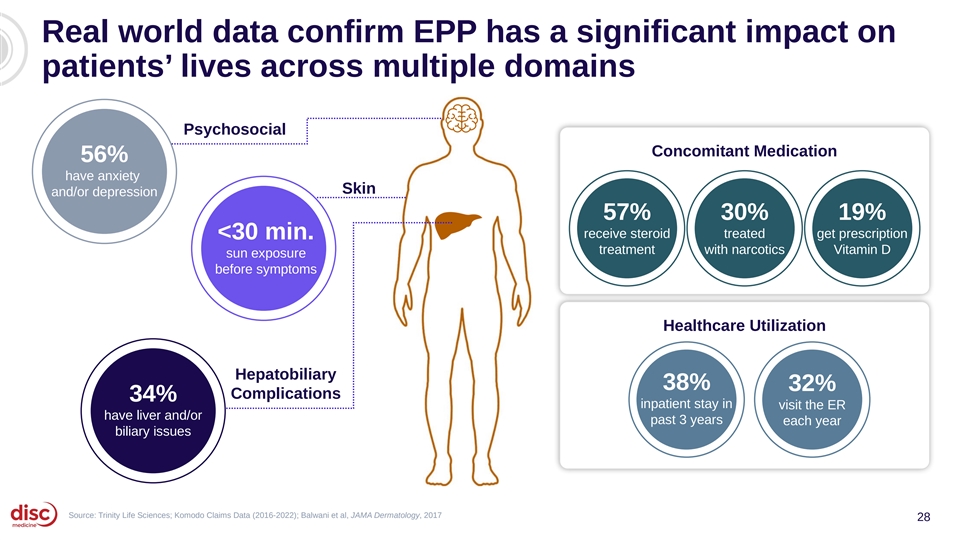
Real world data confirm EPP has a significant impact on patients’ lives across multiple domains Psychosocial Concomitant Medication 56% have anxiety Skin and/or depression 57% 30% 19% receive steroid treated get prescription <30 min. treatment with narcotics Vitamin D sun exposure before symptoms Healthcare Utilization Hepatobiliary 34% 38% 32% Complications 34% have liver and/or inpatient stay in visit the ER have liver and/or biliary issues past 3 years each year biliary issues Source: Trinity Life Sciences; Komodo Claims Data (2016-2022); Balwani et al, JAMA Dermatology, 2017 28
Agenda Introduction and Data Summary 01 John Quisel, JD, PhD, Chief Executive Officer Bitopertin in EPP 02 • Updated BEACON Data Bruce Wang, MD, Professor of Gastroenterology, University of California San Francisco Will Savage, MD, PhD, Chief Medical Officer • EPP Commercial Opportunity Jonathan Yu, Chief Business Officer DISC-0974 03 • Initial Data in Anemia of Myelofibrosis Will Savage, MD, PhD, Chief Medical Officer • Initial Data in NDD-CKD and Anemia Will Savage, MD, PhD, Chief Medical Officer Closing Remarks 04 John Quisel, JD, PhD, Chief Executive Officer Q&A Session 05 29
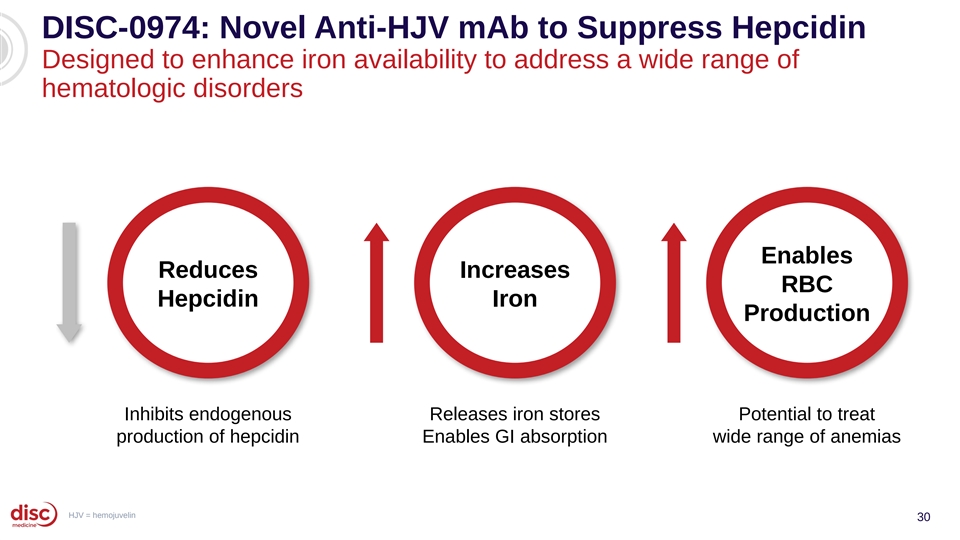
DISC-0974: Novel Anti-HJV mAb to Suppress Hepcidin Designed to enhance iron availability to address a wide range of hematologic disorders Enables Reduces Increases RBC Hepcidin Iron Production Inhibits endogenous Releases iron stores Potential to treat production of hepcidin Enables GI absorption wide range of anemias HJV = hemojuvelin 30
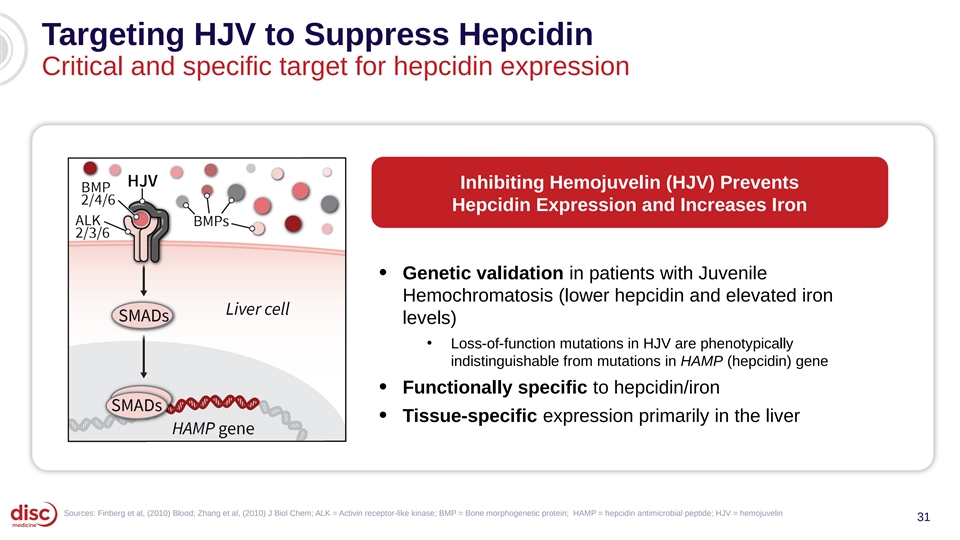
Targeting HJV to Suppress Hepcidin Critical and specific target for hepcidin expression Inhibiting Hemojuvelin (HJV) Prevents Hepcidin Expression and Increases Iron • Genetic validation in patients with Juvenile Hemochromatosis (lower hepcidin and elevated iron levels) • Loss-of-function mutations in HJV are phenotypically indistinguishable from mutations in HAMP (hepcidin) gene Functionally specific to hepcidin/iron • • Tissue-specific expression primarily in the liver Sources: Finberg et al, (2010) Blood; Zhang et al, (2010) J Biol Chem; ALK = Activin receptor-like kinase; BMP = Bone morphogenetic protein; HAMP = hepcidin antimicrobial peptide; HJV = hemojuvelin 31
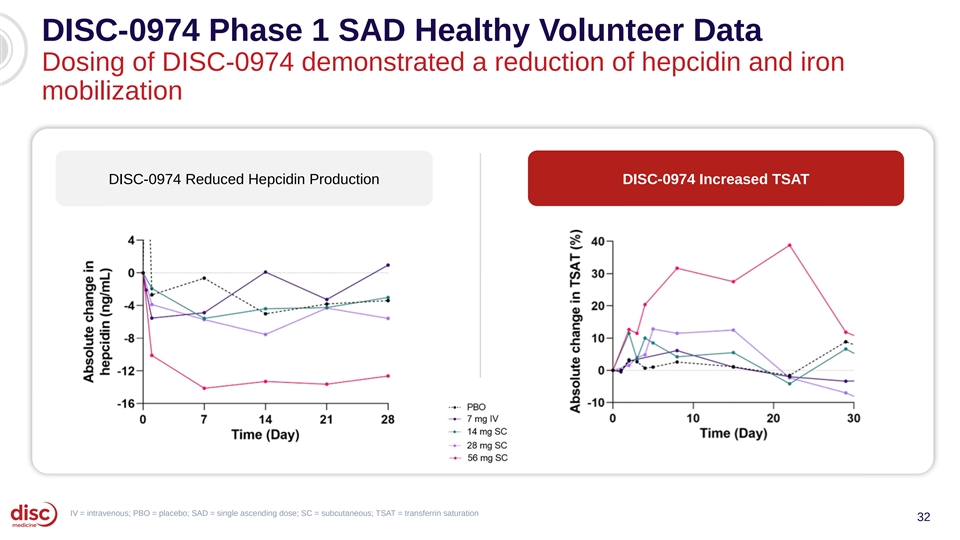
DISC-0974 Phase 1 SAD Healthy Volunteer Data Dosing of DISC-0974 demonstrated a reduction of hepcidin and iron mobilization DISC-0974 Reduced Hepcidin Production DISC-0974 Increased TSAT IV = intravenous; PBO = placebo; SAD = single ascending dose; SC = subcutaneous; TSAT = transferrin saturation 32
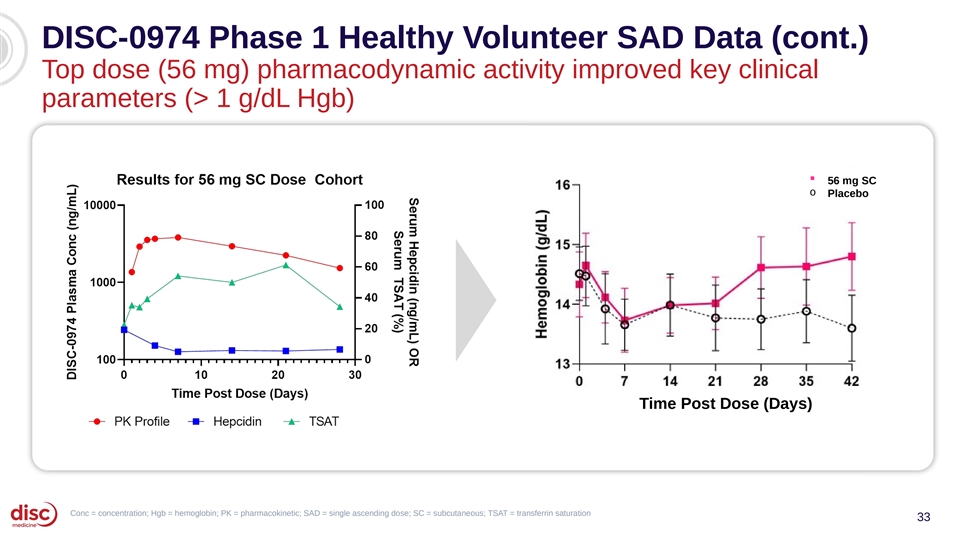
DISC-0974 Phase 1 Healthy Volunteer SAD Data (cont.) Top dose (56 mg) pharmacodynamic activity improved key clinical parameters (> 1 g/dL Hgb) § 56 mg SC o Placebo Time Post Dose (Days) Conc = concentration; Hgb = hemoglobin; PK = pharmacokinetic; SAD = single ascending dose; SC = subcutaneous; TSAT = transferrin saturation 33
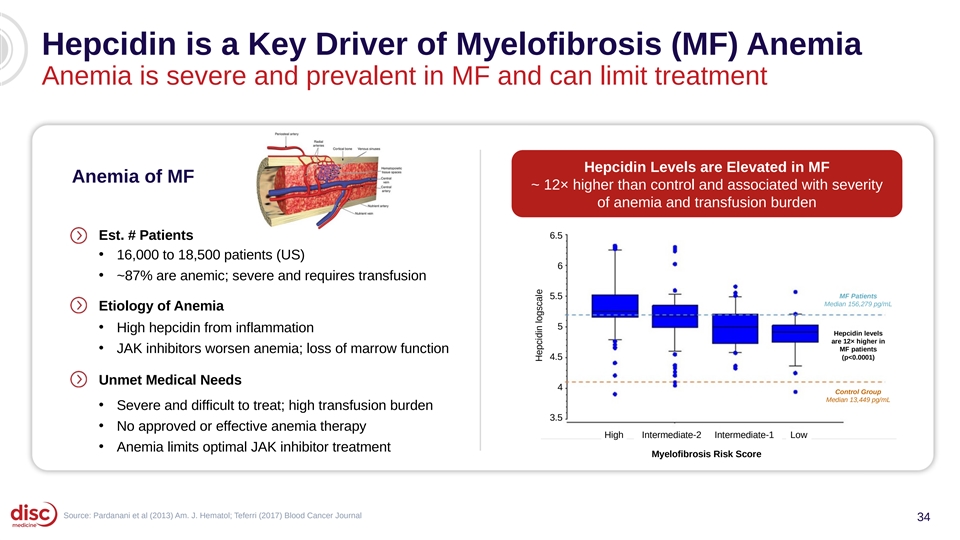
Hepcidin is a Key Driver of Myelofibrosis (MF) Anemia Anemia is severe and prevalent in MF and can limit treatment Hepcidin Levels are Elevated in MF Anemia of MF ~ 12× higher than control and associated with severity of anemia and transfusion burden 6.5 Est. # Patients • 16,000 to 18,500 patients (US) 6 • ~87% are anemic; severe and requires transfusion MF Patients 5.5 Median 156,279 pg/mL Etiology of Anemia 5 • High hepcidin from inflammation Hepcidin levels are 12× higher in • MF patients JAK inhibitors worsen anemia; loss of marrow function 4.5 (p<0.0001) Unmet Medical Needs 4 Control Group Median 13,449 pg/mL • Severe and difficult to treat; high transfusion burden 3.5 • No approved or effective anemia therapy High Intermediate-2 Intermediate-1 Low • Anemia limits optimal JAK inhibitor treatment Myelofibrosis Risk Score Source: Pardanani et al (2013) Am. J. Hematol; Teferri (2017) Blood Cancer Journal 34 Hepcidin logscale
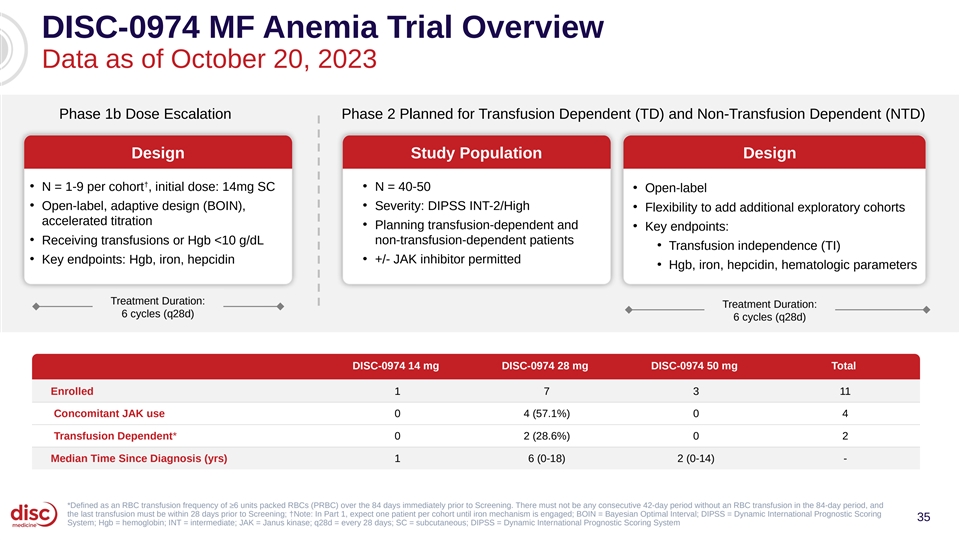
DISC-0974 MF Anemia Trial Overview Data as of October 20, 2023 Phase 1b Dose Escalation Phase 2 Planned for Transfusion Dependent (TD) and Non-Transfusion Dependent (NTD) Design Study Population Design † • N = 1-9 per cohort , initial dose: 14mg SC • N = 40-50 • Open-label • • Open-label, adaptive design (BOIN), Severity: DIPSS INT-2/High • Flexibility to add additional exploratory cohorts accelerated titration • Planning transfusion-dependent and • Key endpoints: • Receiving transfusions or Hgb <10 g/dL non-transfusion-dependent patients • Transfusion independence (TI) • • Key endpoints: Hgb, iron, hepcidin +/- JAK inhibitor permitted • Hgb, iron, hepcidin, hematologic parameters Treatment Duration: Treatment Duration: 6 cycles (q28d) 6 cycles (q28d) DISC-0974 14 mg DISC-0974 28 mg DISC-0974 50 mg Total Enrolled 1 7 3 11 Concomitant JAK use 0 4 (57.1%) 0 4 Transfusion Dependent* 0 2 (28.6%) 0 2 Median Time Since Diagnosis (yrs) 1 6 (0-18) 2 (0-14) - *Defined as an RBC transfusion frequency of ≥6 units packed RBCs (PRBC) over the 84 days immediately prior to Screening. There must not be any consecutive 42-day period without an RBC transfusion in the 84-day period, and the last transfusion must be within 28 days prior to Screening; †Note: In Part 1, expect one patient per cohort until iron mechanism is engaged; BOIN = Bayesian Optimal Interval; DIPSS = Dynamic International Prognostic Scoring 35 System; Hgb = hemoglobin; INT = intermediate; JAK = Janus kinase; q28d = every 28 days; SC = subcutaneous; DIPSS = Dynamic International Prognostic Scoring System
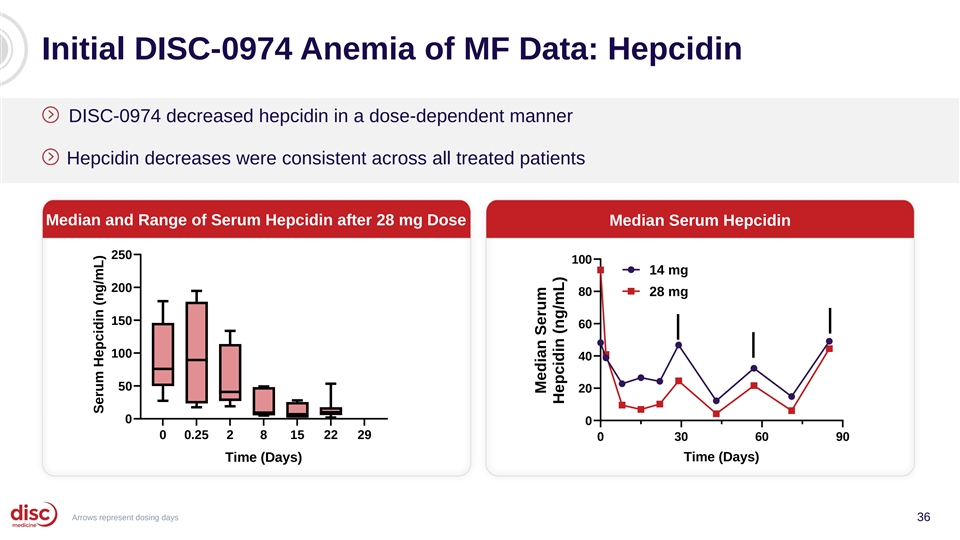
Initial DISC-0974 Anemia of MF Data: Hepcidin DISC-0974 decreased hepcidin in a dose-dependent manner Hepcidin decreases were consistent across all treated patients Median and Range of Serum Hepcidin after 28 mg Dose Median Serum Hepcidin 250 100 14 mg 200 80 28 mg 150 60 100 40 50 20 0 0 0 0.25 2 8 15 22 29 0 30 60 90 Time (Days) Time (Days) Arrows represent dosing days 36 Serum Hepcidin (ng/mL) Median Serum Hepcidin (ng/mL)
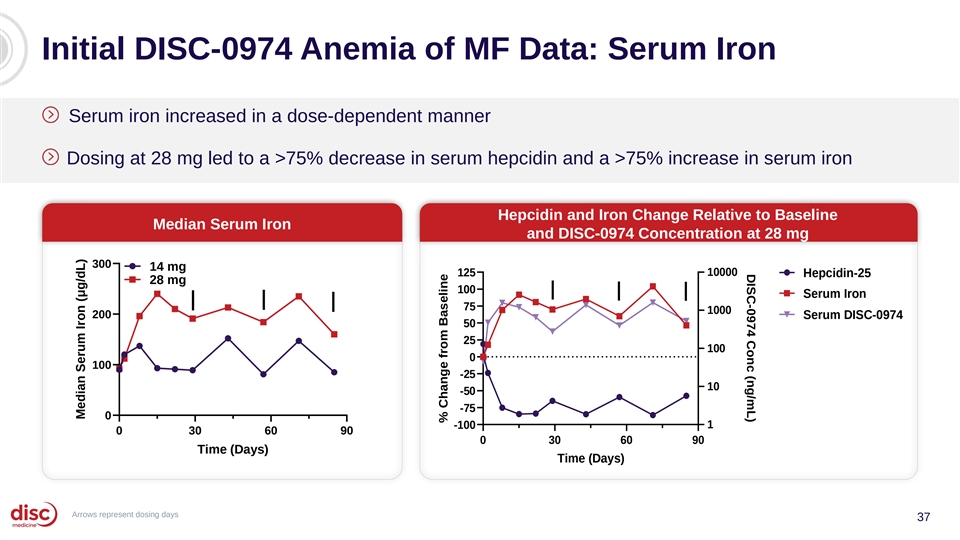
DISC-0974 Conc (ng/mL) Initial DISC-0974 Anemia of MF Data: Serum Iron Serum iron increased in a dose-dependent manner Dosing at 28 mg led to a >75% decrease in serum hepcidin and a >75% increase in serum iron Hepcidin and Iron Change Relative to Baseline Median Serum Iron and DISC-0974 Concentration at 28 mg 300 14 mg 125 10000 Hepcidin-25 28 mg 100 Serum Iron 75 1000 200 Serum DISC-0974 50 25 100 0 100 -25 10 -50 -75 0 1 -100 0 30 60 90 0 30 60 90 Time (Days) Time (Days) Arrows represent dosing days 37 Median Serum Iron (μg/dL) % Change from Baseline
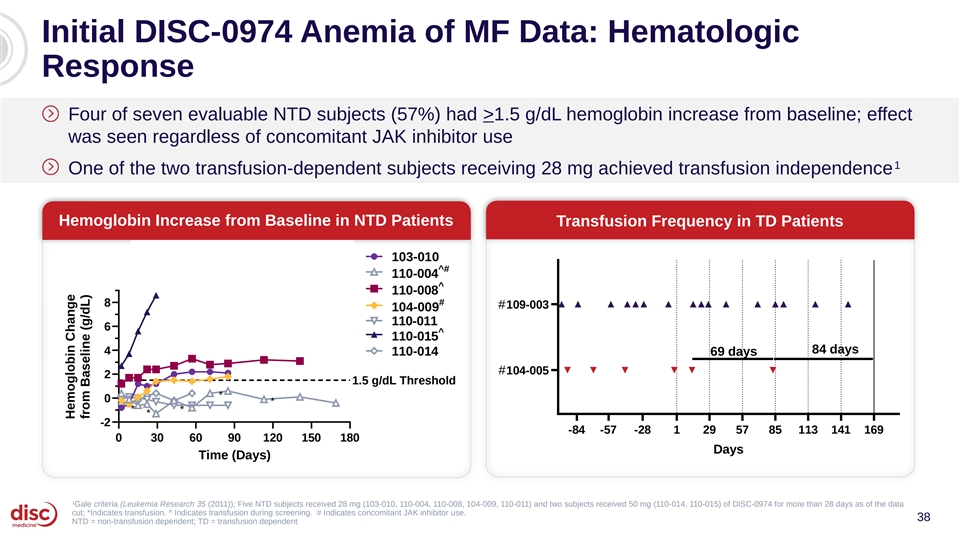
Initial DISC-0974 Anemia of MF Data: Hematologic Response Four of seven evaluable NTD subjects (57%) had >1.5 g/dL hemoglobin increase from baseline; effect was seen regardless of concomitant JAK inhibitor use 1 One of the two transfusion-dependent subjects receiving 28 mg achieved transfusion independence Hemoglobin Increase from Baseline in NTD Patients Transfusion Frequency in TD Patients Transfusion Frequency over time in TD subjects Hemoglobin Change from 103-010 Baseline in NTD subjects ^# 110-004 ^ 110-008 # 8 #109-003 104-009 110-011 6 ^ 110-015 84 days 4 110-014 69 days #104-005 2 1.5 g/dL Threshold * 0 * * * * -2 -84 -57 -28 1 29 57 85 113 141 169 0 30 60 90 120 150 180 Days Time (Days) 1 Gale criteria (Leukemia Research 35 (2011)); Five NTD subjects received 28 mg (103-010, 110-004, 110-008, 104-009, 110-011) and two subjects received 50 mg (110-014, 110-015) of DISC-0974 for more than 28 days as of the data cut; *Indicates transfusion. ^ Indicates transfusion during screening. # Indicates concomitant JAK inhibitor use. 38 NTD = non-transfusion dependent; TD = transfusion dependent Hemoglobin Change from Baseline (g/dL)
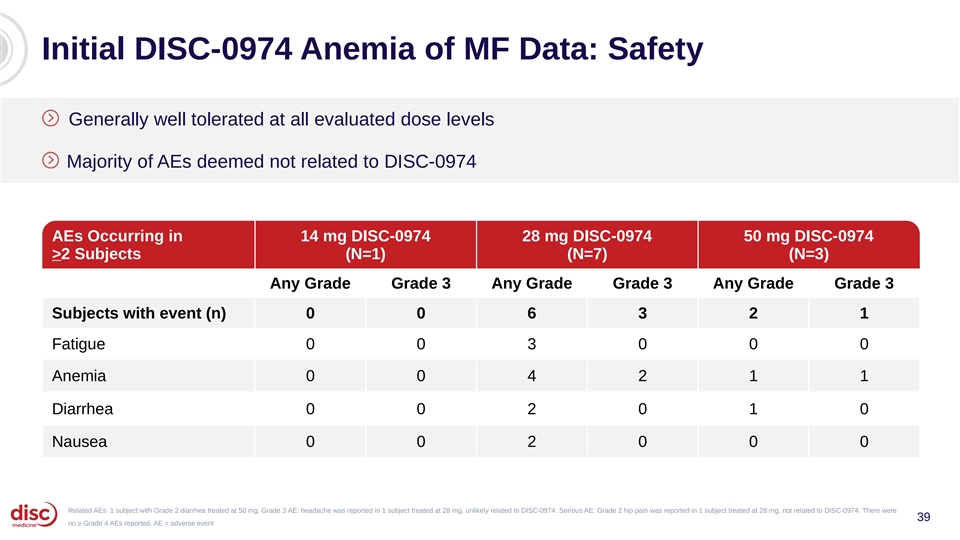
Initial DISC-0974 Anemia of MF Data: Safety Generally well tolerated at all evaluated dose levels Majority of AEs deemed not related to DISC-0974 AEs Occurring in 14 mg DISC-0974 28 mg DISC-0974 50 mg DISC-0974 >2 Subjects (N=1) (N=7) (N=3) Any Grade Grade 3 Any Grade Grade 3 Any Grade Grade 3 Subjects with event (n) 0 0 6 3 2 1 Fatigue 0 0 3 0 0 0 Anemia 0 0 4 2 1 1 Diarrhea 0 0 2 0 1 0 Nausea 0 0 2 0 0 0 Related AEs: 1 subject with Grade 2 diarrhea treated at 50 mg. Grade 3 AE: headache was reported in 1 subject treated at 28 mg, unlikely related to DISC-0974. Serious AE: Grade 2 hip pain was reported in 1 subject treated at 28 mg, not related to DISC-0974. There were 39 no ≥ Grade 4 AEs reported. AE = adverse event
Agenda Introduction and Data Summary 01 John Quisel, JD, PhD, Chief Executive Officer Bitopertin in EPP 02 • Updated BEACON Data Bruce Wang, MD, Professor of Gastroenterology, University of California San Francisco Will Savage, MD, PhD, Chief Medical Officer • EPP Commercial Opportunity Jonathan Yu, Chief Business Officer DISC-0974 03 • Initial Data in Anemia of Myelofibrosis Will Savage, MD, PhD, Chief Medical Officer • Initial Data in NDD-CKD and Anemia Will Savage, MD, PhD, Chief Medical Officer Closing Remarks 04 John Quisel, JD, PhD, Chief Executive Officer Q&A Session 05 40
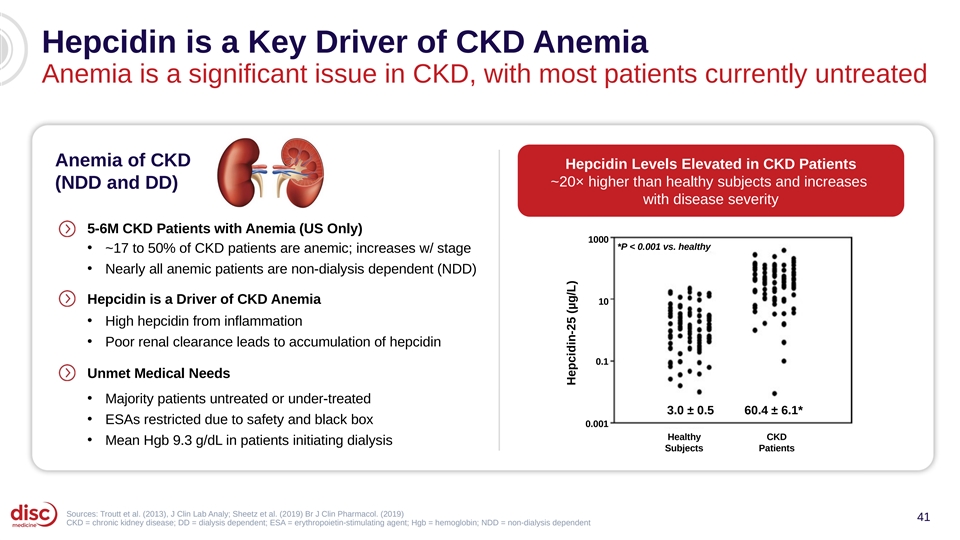
Hepcidin is a Key Driver of CKD Anemia Anemia is a significant issue in CKD, with most patients currently untreated Anemia of CKD Hepcidin Levels Elevated in CKD Patients ~20× higher than healthy subjects and increases (NDD and DD) with disease severity 5-6M CKD Patients with Anemia (US Only) 1000 *P < 0.001 vs. healthy • ~17 to 50% of CKD patients are anemic; increases w/ stage • Nearly all anemic patients are non-dialysis dependent (NDD) Hepcidin is a Driver of CKD Anemia 10 • High hepcidin from inflammation • Poor renal clearance leads to accumulation of hepcidin 0.1 Unmet Medical Needs • Majority patients untreated or under-treated 3.0 ± 0.5 60.4 ± 6.1* • ESAs restricted due to safety and black box 0.001 Healthy CKD • Mean Hgb 9.3 g/dL in patients initiating dialysis Subjects Patients Sources: Troutt et al. (2013), J Clin Lab Analy; Sheetz et al. (2019) Br J Clin Pharmacol. (2019) 41 CKD = chronic kidney disease; DD = dialysis dependent; ESA = erythropoietin-stimulating agent; Hgb = hemoglobin; NDD = non-dialysis dependent Hepcidin-25 (µg/L)
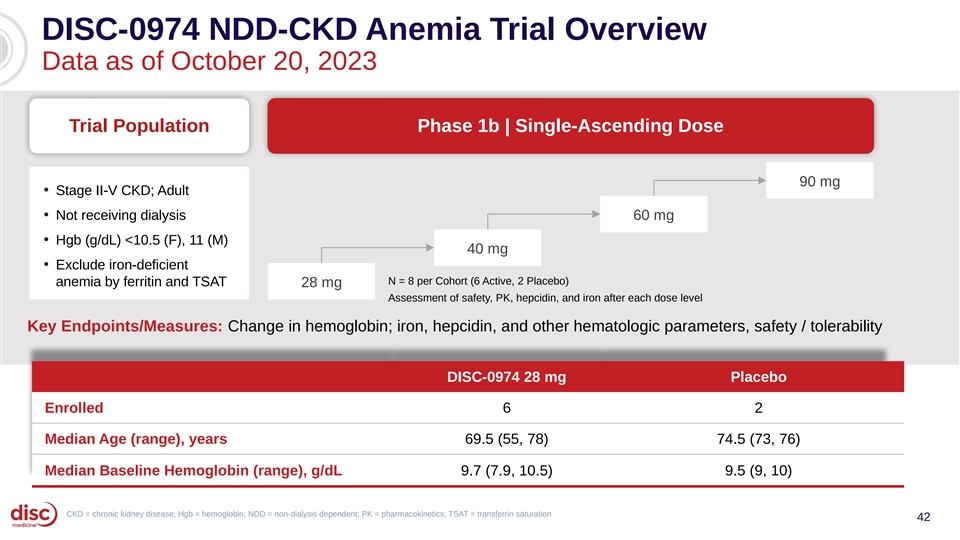
DISC-0974 NDD-CKD Anemia Trial Overview Data as of October 20, 2023 Trial Population Phase 1b | Single-Ascending Dose 90 mg • Stage II-V CKD; Adult • Not receiving dialysis 60 mg • Hgb (g/dL) <10.5 (F), 11 (M) 40 mg • Exclude iron-deficient N = 8 per Cohort (6 Active, 2 Placebo) anemia by ferritin and TSAT 28 mg Assessment of safety, PK, hepcidin, and iron after each dose level Key Endpoints/Measures: Change in hemoglobin; iron, hepcidin, and other hematologic parameters, safety / tolerability DISC-0974 28 mg Placebo Enrolled 6 2 Median Age (range), years 69.5 (55, 78) 74.5 (73, 76) Median Baseline Hemoglobin (range), g/dL 9.7 (7.9, 10.5) 9.5 (9, 10) CKD = chronic kidney disease; Hgb = hemoglobin; NDD = non-dialysis dependent; PK = pharmacokinetics; TSAT = transferrin saturation 42
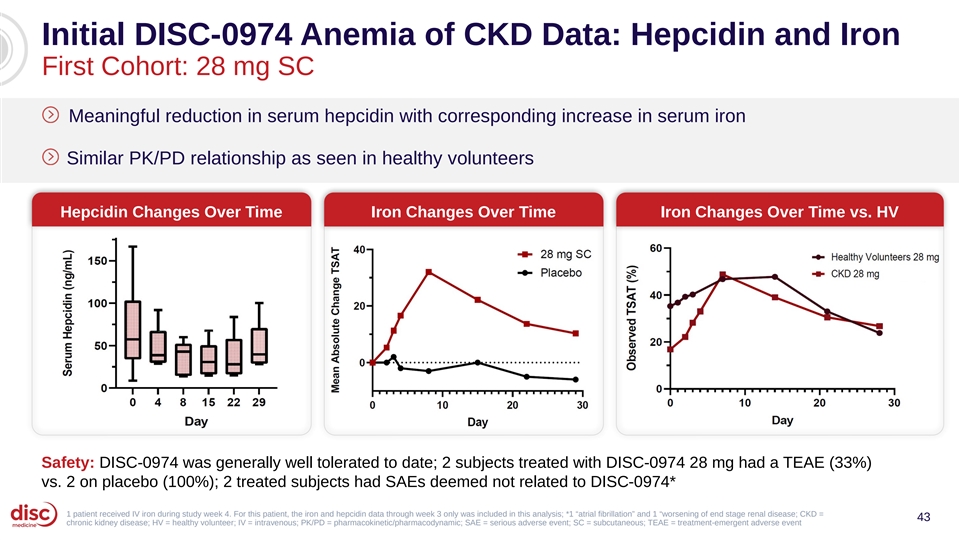
Initial DISC-0974 Anemia of CKD Data: Hepcidin and Iron First Cohort: 28 mg SC Meaningful reduction in serum hepcidin with corresponding increase in serum iron Similar PK/PD relationship as seen in healthy volunteers Hepcidin Changes Over Time Iron Changes Over Time Iron Changes Over Time vs. HV Safety: DISC-0974 was generally well tolerated to date; 2 subjects treated with DISC-0974 28 mg had a TEAE (33%) vs. 2 on placebo (100%); 2 treated subjects had SAEs deemed not related to DISC-0974* 1 patient received IV iron during study week 4. For this patient, the iron and hepcidin data through week 3 only was included in this analysis; *1 “atrial fibrillation” and 1 “worsening of end stage renal disease; CKD = 43 chronic kidney disease; HV = healthy volunteer; IV = intravenous; PK/PD = pharmacokinetic/pharmacodynamic; SAE = serious adverse event; SC = subcutaneous; TEAE = treatment-emergent adverse event
Key Takeaways from Initial DISC-0974 Data Signal of Initial Proof Hematologic Safety of Concept Response Dose-dependent, Improvements in Generally well meaningful hemoglobin and tolerated at all reductions in transfusion burden evaluated dose hepcidin and across broad range levels increases in iron of MF patients 44
Agenda Introduction and Data Summary 01 John Quisel, JD, PhD, Chief Executive Officer Bitopertin in EPP 02 • Updated BEACON Data Bruce Wang, MD, Professor of Gastroenterology, University of California San Francisco Will Savage, MD, PhD, Chief Medical Officer • EPP Commercial Opportunity Jonathan Yu, Chief Business Officer DISC-0974 03 • Initial Data in Anemia of Myelofibrosis Will Savage, MD, PhD, Chief Medical Officer • Initial Data in NDD-CKD and Anemia Will Savage, MD, PhD, Chief Medical Officer Closing Remarks 04 John Quisel, JD, PhD, Chief Executive Officer Q&A Session 05 45
Summary of Data Bitopertin DISC-0974 Heme Synthesis Modulator Hepcidin Suppression Phase 1b/2 in Myelofibrosis and Anemia • Consistent, significant reductions in PPIX; • Initial data demonstrated: >40% on average • Consistent decrease in serum hepcidin (>75%) • Significant improvement in sunlight tolerance and increase in iron across multiple measures: • Hematologic responses in a broad range of pts • >3x increase in time to prodrome Phase 1b/2 in NDD-CKD and Anemia • >3x increase in cumulative time in light vs. • Initial data from the 28 mg cohort demonstrated: historical controls • Meaningful reductions in hepcidin and • Increase in symptom-free days increase in iron, similar PK/PD as HVOL • Improvements in quality of life • Generally well tolerated • Generally well tolerated AE = adverse event; HVOL = healthy volunteers; PD = pharmacodynamics; PK = pharmacokinetics; PPIX = protoporphyrin IX; NTD = non-transfusion dependent; TD = transfusion dependent 46
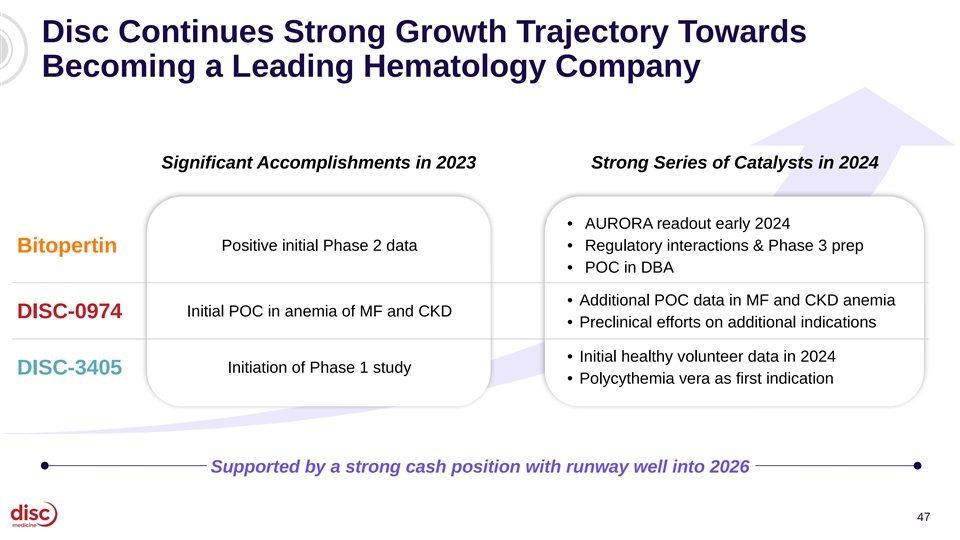
Disc Continues Strong Growth Trajectory Towards Becoming a Leading Hematology Company Significant Accomplishments in 2023 Strong Series of Catalysts in 2024 • AURORA readout early 2024 Positive initial Phase 2 data • Regulatory interactions & Phase 3 prep Bitopertin • POC in DBA • Additional POC data in MF and CKD anemia Initial POC in anemia of MF and CKD DISC-0974 • Preclinical efforts on additional indications • Initial healthy volunteer data in 2024 Initiation of Phase 1 study DISC-3405 • Polycythemia vera as first indication Supported by a strong cash position with runway well into 2026 47
Agenda Introduction and Data Summary 01 John Quisel, JD, PhD, Chief Executive Officer Bitopertin in EPP 02 • Updated BEACON Data Bruce Wang, MD, Professor of Gastroenterology, University of California San Francisco Will Savage, MD, PhD, Chief Medical Officer • EPP Commercial Opportunity Jonathan Yu, Chief Business Officer DISC-0974 03 • Initial Data in Anemia of Myelofibrosis Will Savage, MD, PhD, Chief Medical Officer • Initial Data in NDD-CKD and Anemia Will Savage, MD, PhD, Chief Medical Officer Closing Remarks 04 John Quisel, JD, PhD, Chief Executive Officer Q&A Session 05 48

Q&A