UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d)
of the Securities Exchange Act of 1934
Date of Report (Date of earliest event reported): December 10, 2023
Poseida Therapeutics, Inc.
(Exact name of Registrant as Specified in Its Charter)
| Delaware | 001-39376 | 47-2846548 | ||
| (State or Other Jurisdiction of Incorporation) |
(Commission File Number) |
(IRS Employer Identification No.) |
| 9390 Towne Centre Drive, Suite 200 | ||
| San Diego, California | 92121 | |
| (Address of Principal Executive Offices) | (Zip Code) |
Registrant’s Telephone Number, Including Area Code: (858) 779-3100
(Former Name or Former Address, if Changed Since Last Report)
Check the appropriate box below if the Form 8-K filing is intended to simultaneously satisfy the filing obligation of the registrant under any of the following provisions:
| ☐ | Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425) |
| ☐ | Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12) |
| ☐ | Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)) |
| ☐ | Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section 12(b) of the Act:
|
|
Trading |
Name of each exchange on which registered |
||
| Common Stock, par value $0.0001 per share | PSTX | Nasdaq Global Select Market |
Indicate by check mark whether the registrant is an emerging growth company as defined in Rule 405 of the Securities Act of 1933 (§ 230.405 of this chapter) or Rule 12b-2 of the Securities Exchange Act of 1934 (§ 240.12b-2 of this chapter).
Emerging growth company ☒
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
| Item 7.01 | Regulation FD Disclosure. |
On December 10, 2023, Poseida Therapeutics, Inc. (the “Company”) issued a press release announcing that members of its scientific research team and external advisors are providing an update on the Company’s research and development programs, including the Company’s Phase 1 clinical trial of P-BCMA-ALLO1. The Company presented several posters at the 65th American Society of Hematology (ASH) Annual Meeting and Exposition, taking place in San Diego, California from December 9-12, 2023. A copy of the press release and one of the posters that was presented are attached as Exhibit 99.1 and Exhibit 99.2, respectively, to this report.
The information in this Item 7.01 of this report (including Exhibit 99.1 and Exhibit 99.2) is furnished and shall not be deemed “filed” for purposes of Section 18 of the Securities Exchange Act of 1934, as amended, or subject to the liabilities of that section or Sections 11 and 12(a)(2) of the Securities Act of 1933, as amended. The information shall not be deemed incorporated by reference into any other filing with the Securities and Exchange Commission made by the Company, whether made before or after today’s date, regardless of any general incorporation language in such filing, except as shall be expressly set forth by specific references in such filing.
| Item 9.01 | Financial Statements and Exhibits. |
(d) Exhibits.
| Exhibit No. |
Description | |
| 99.1 | Press Release of Poseida Therapeutics, Inc., dated December 10, 2023. | |
| 99.2 | Poster: Early Safety and Efficacy Results of P-BCMA-ALLO1, A Fully Allogeneic Chimeric Antigen Receptor T-cell (CAR-T), in Patients with Relapsed / Refractory Multiple Myeloma (RRMM). | |
| 104 | Cover Page Interactive Data File (embedded within the Inline XBRL document) | |
SIGNATURES
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
| Poseida Therapeutics, Inc. | ||||||
| Date: December 11, 2023 | By: | /s/ Harry J. Leonhardt, Esq. |
||||
| Name: Title: |
Harry J. Leonhardt, Esq. General Counsel, Chief Compliance Officer & |
|||||
Exhibit 99.1

Poseida Therapeutics Presents Positive Early Results from its Phase 1 Trial of Allogeneic CAR-T P-BCMA-ALLO1 in Relapsed-Refractory Multiple Myeloma at the 65th American Society of Hematology (ASH) Annual Meeting
82% ORR and deep clinical responses from off-the-shelf, allogeneic BCMA-targeted CAR-T in heavily pretreated patients receiving adequate lymphodepletion
100% ORR in these patients who were not previously treated with a BCMA-targeted bispecific T cell-engaging antibody
Favorable emerging safety and reliability profile, with all (100%) intent-to-treat (ITT) patients receiving therapy, no GvHD or dose-limiting toxicities and low incidences of CRS and neurotoxicity observed (all ≤ Grade 2)
Preliminary data show allogeneic TSCM-rich CAR-T cells trafficking to bone marrow, differentiating to cell-killing effector T cells and persisting at least 6 weeks
Two additional poster presentations highlight advancements across the Company’s cell and gene therapy programs and platforms
Company to host webcast and conference call today at 11:00 AM PST
SAN DIEGO, December 10, 2023—Poseida Therapeutics, Inc. (Nasdaq: PSTX), a clinical-stage cell and gene therapy company advancing a new class of treatments for patients with cancer and rare diseases, today announced early efficacy and safety results from its Phase 1 study of P-BCMA-ALLO1, its BCMA-targeted allogeneic, T stem cell memory (TSCM)-rich chimeric antigen receptor (CAR)-T therapy candidate. The Company is investigating P-BCMA-ALLO1 in partnership with Roche for the treatment of relapsed/refractory multiple myeloma (RRMM). Detailed study findings, along with two additional Company poster presentations in cell and gene therapy, are being featured at the 65th ASH Annual Meeting and Exposition being held in San Diego on December 9-12, 2023.
“Today, far too many patients are unable to benefit from autologous CAR-T therapy due to its limited supply, lengthy timelines, complex logistics, and cost,” said Kristin Yarema, Ph.D., President, Cell Therapy at Poseida. “We have long believed that readily produced, off-the-shelf allogeneic, TSCM-rich CAR-T products have the potential to offer a compelling efficacy and safety profile while also supporting patient access. TSCM-rich CAR-T products can be difficult to produce with older virus-based technology, but we are able to create a portfolio of such products using Poseida’s unique, non-viral set of technologies. We see these early P-BCMA-ALLO1 results in multiple myeloma, in which all enrolled patients received CAR-T therapy and most patients receiving adequate lymphodepletion achieved a stringent complete response (sCR) or very good partial response (VGPR), as validating our vision and eagerly await additional data yet to come from this study. This is also the first known publicly presented data set that provides clear clinical evidence supporting the hypothesis that TSCM cells are the ideal cell type for allogeneic CAR-T, extending our previous findings with autologous TSCM cells to the allogeneic setting.
We hope that TSCM-rich allogeneic CAR-T therapies may potentially offer the optimal combination of clinical results, on-demand availability and high-volume production, while supporting broader access to CAR-T therapies. We are excited to have taken this first step with our early P-BCMA-ALLO1 clinical results. They inspire us to further develop P-BCMA-ALLO1 in partnership with Roche, and to continue advancing our entire allogeneic TSCM cell-based CAR-T portfolio.”
P-BCMA-ALLO1 program data presentations
At the time of the October 23, 2023 data cut off, 39 patients were enrolled as an intent-to-treat (ITT) population in the ongoing Phase 1 multicenter, open-label dose-escalation study (NCT04960579). Enrolled patients had previously failed protease inhibitor, immunomodulatory drug (IMiD), and anti-CD38 antibody treatments or were otherwise triple-refractory. Previous treatment with B cell maturation antigen (BCMA)-targeted therapy was allowed including autologous BCMA CAR-T and bispecific T cell-engaging (TCE) antibodies. All enrolled patients completed lymphodepletion and went on to receive P-BCMA-ALLO1 a median of 7 days after enrollment for a 100% ITT treatment rate with no use of bridging therapy. Six patient cohorts varying in size (n=1 to n=6) received one of three fludarabine/cyclophosphamide (flu/cy) lymphodepleting conditioning regimens including 3 days of fludarabine at 30 mg/m2/day for all patients and, depending upon the patient cohort, 3 days of cyclophosphamide at 300, 500, or 1,000 mg/m2/day followed by infusion of P-BCMA-ALLO1 cells at cell doses varying by cohort up to 6x106 cells/kg to date.
Evaluable patients with at least 4 weeks of follow up (n=33) were heavily pretreated with a median of 7 prior lines of therapy. Additionally, 30% of these patients had high risk disease by cytogenetics and nearly 2 in 5 (39%) had received previous BCMA-targeted therapy. 11 of the 33 evaluable patients were in the two cohorts receiving 2x106 cells/kg of P-BCMA-ALLO1 and higher cyclophosphamide preconditioning doses at either 500 mg/m2 (‘P1 arm’; n=5) or 1,000 mg/m2 (‘P2 arm’; n=6).
An overall objective response rate (ORR) of 82% (9/11 total patients) was reached among patients in the pooled P1 and P2 arms. ORR in the P2 arm was 83% (5/6) with 100% (5/5) of the responding P2 patients achieving a VGPR or better and 40% (2/5) achieving sCR. 80% ORR was obtained in the P1 arm (4/5) with 50% of responding patients achieving VGPR. Both nonresponding patients, one in each of the P1 and P2 arms, had received and not achieved clinical response with the BCMAxCD3 bispecific TCE antibody therapy teclistamab prior to receiving P-BCMA-ALLO1.
A 100% ORR (9/9) was achieved among patients in P1 and P2 arms who had not received a prior BCMA-targeting bispecific TCE antibody as well as 100% ORR (2/2) in patients who had received prior autologous CAR-T BCMA targeted therapy.
P-BCMA-ALLO1 was very well tolerated, with no graft-vs-host disease (GvHD) at any dose and low rates of cytokine release syndrome (CRS) and neurotoxicity, all Grade 2 or less, found among all evaluable patients.
Expansion and persistence of the CAR-T cells in patients after infusion was found to be highly dependent upon the conditioning dose of cyclophosphamide, with P-BCMA-ALLO1 levels measured in the blood much higher in patient cohorts in the P1 and P2 arms receiving the 500 mg/m2 and 1,000 mg/m2 conditioning doses than in any of the 300 mg/m2 (arm ‘S’, n=20) cohorts. Clinical responses in patients receiving arm S conditioning treatment were inferior to those achieved by patients in P1 or P2.
Analysis of P-BCMA-ALLO1 cellular kinetics in two patients with high CAR-T expansion showed CAR-T cells persisted and were measurable in the peripheral blood of one patient for at least 4 weeks and engrafted and persisted at a high level in the bone marrow of the other for at least 6 weeks. Moreover, in both cases cells in the TSCM-rich CAR-T infused drug product underwent differentiation after infusion to generate a much more effector T cell-rich population, particularly among the important CD8+ ‘killer T cell’ subpopulation. These findings are the first known direct clinical evidence supporting the theory that allogeneic TSCM-based CAR-T cells can act as effective prodrugs because they can expand, traffic to the relevant tissues, differentiate into effector cells and persist, all of which may contribute to driving deep clinical responses in patients while also being well-tolerated.
“Despite the emergence of autologous BCMA-targeted therapies, multiple myeloma remains an incurable malignancy. Autologous CAR-T therapies may be associated with numerous challenges for patients and physicians, including prolonged manufacturing times, inconsistent drug quality and serious safety issues,” said Bhagirathbhai Dholaria, M.D., Associate Professor of Medicine (Hematology/Oncology) at the Vanderbilt-Ingram Cancer Center. “Allogeneic CAR-T therapies have the potential to overcome many of these challenges. Today’s data demonstrate that P-BCMA-ALLO1 is a well-tolerated off-the-shelf therapy with a favorable emerging safety profile and encouraging evidence of early clinical activity. In addition, the data show that P-BCMA-ALLO1 can achieve deep clinical responses in patients with high-risk disease and those who have previously received BCMA targeting therapies. Importantly, P-BCMA-ALLO1 was delivered to all patients in the ITT population with all drug product meeting all quality specifications. We look forward to continuing to enroll patients in this study.”
Enrollment is ongoing including additional exploration of dose regimens and lymphodepleting conditioning regimens. While still early to assess durability, at the time of the data cut off 8 of the 9 responding patients in P1 and P2 arms remained in response. The Company, together with Roche, plans to present additional clinical data updates for P-BCMA-ALLO1 at scientific meetings in 2024, subject to coordination with Roche.
A second Poseida-sponsored poster highlights the development of an in vivo bioassay for assessing BCMA CAR-T final product potency and presents data suggesting P-BCMA-ALLO1 drug product may have greater potency than drug products produced in the Company’s earlier, autologous P-BCMA-101 CAR-T program.
P-FVIII-101 program data presentation
The Company has also presented a third poster describing P-FVIII-101, a fully non-viral liver-directed gene therapy combining Poseida’s proprietary piggyBac® DNA Delivery System with nanoparticle delivery for the treatment of Hemophilia A. This poster demonstrates the capabilities of the piggyBac DNA insertion system and non-viral approach in providing stable Factor VIII (FVIII) transgene expression through genomic integration, along with the potential for redosing. The poster highlights 52-week durability in an adult Hemophilia A model along with a favorable tolerability profile of Poseida’s liver-targeted non-viral delivery platform providing further proof-of-principle toward developing an effective and durable treatment for Hemophilia A.
Company-Hosted Webcast and Conference Call Information:
Poseida will host a webcast and conference call today, December 10th at 11:00 AM PST / 2:00 PM EST. The conference call can be accessed by dialing 800-225-9448 (United States) or 203-518-9708 (International) with the conference ID PSTX23. A live webcast may be accessed using the link here, or by visiting the Events and Presentations section of the Poseida website at investors.poseida.com. After the live webcast, the event will remain archived on the Poseida site for 90 days.
Poster Presentation Details:
Title: Early Safety Results of P-BCMA-ALLO1, a Fully Allogeneic Chimeric Antigen Receptor T-Cell (CAR-T), in Patients with Relapsed/Refractory Multiple Myeloma (RRMM)
| • | Presenting Author: Bhagirathbhai Dholaria, M.D., Associate Professor of Medicine (Hematology/Oncology) at the Vanderbilt-Ingram Cancer Center |
| • | Session Date & Time: Sunday, December 10, 2023, at 6:00 – 8:00 PM PT |
| • | Publication Number: 3479 |
| • | Session Title: 704. Cellular Immunotherapies: Early Phase and Investigational Therapies: Poster II |
| • | Location: Halls G-H |
Title: A Tumor-Bearing Murine Xenograft Model as a Bioassay for Assessing CAR-T Product Potency Shows Positive Predictive Value for Clinical Performance
| • | Presenting Author: Stacey Cranert, Ph.D., Poseida Therapeutics |
| • | Session Date & Time: Saturday, December 9, 2023, at 5:30 – 7:30 PM PT |
| • | Publication Number: 2293 |
| • | Session Title: 803. Emerging Tools, Techniques and Artificial Intelligence in Hematology: Poster I |
| • | Location: Halls G-H |
Title: Effective Gene Therapy for Hemophilia A: Novel Re-Dosable Non-Viral Formulation That Provides Stable, and Durable FVIII Expression with Improved Tolerability
| • | Presenting Author: Brian Truong, Ph.D., Poseida Therapeutics |
| • | Session Date & Time: Saturday, December 9, 2023, at 5:30 – 7:30 PM PT |
| • | Publication Number: 1232 |
| • | Session Title: 321. Coagulation and Fibrinolysis: Basic and Translational: Poster I |
| • | Location: Halls G-H |
About P-BCMA-ALLO1
P-BCMA-ALLO1 is an allogeneic CAR-T product candidate licensed to Roche targeting B-cell maturation antigen (BCMA) for the treatment of relapsed/refractory multiple myeloma in Phase 1 development. This allogeneic program includes a VH-based binder that targets BCMA and has shown early evidence of encouraging safety and efficacy. Additional information about the Phase 1 study is available at www.clinicaltrials.gov using identifier: NCT04960579.
About P-FVIII-101
P-FVIII-101 is a liver-directed gene therapy combining Poseida’s non-viral piggyBac platform and nanoparticle delivery technologies for the in vivo treatment of Hemophilia A. Hemophilia A is a bleeding disorder caused by a deficiency in Factor VIII production with a high unmet need. P-FVIII-101 utilizes the piggyBac gene integration system delivered via lipid nanoparticle, which has demonstrated stable and sustained Factor VIII expression in juvenile and adult animal models.
About Poseida Therapeutics, Inc.
Poseida Therapeutics is a clinical-stage biopharmaceutical company advancing differentiated cell and gene therapies with the capacity to cure certain cancers and rare diseases. The Company’s pipeline includes allogeneic CAR-T cell therapy product candidates for both solid and liquid tumors as well as in vivo gene therapy product candidates that address patient populations with high unmet medical need. The Company’s approach to cell and gene therapies is based on its proprietary genetic editing platforms, including its non-viral piggyBac® DNA Delivery System, Cas-CLOVER™ Site-Specific Gene Editing System, and nanoparticle and hybrid gene delivery technologies as well as in-house GMP cell therapy manufacturing. The Company has formed a global strategic collaboration with Roche to unlock the promise of cell therapies for patients with hematological malignancies. Learn more at www.poseida.com and connect with us on X and LinkedIn.
Forward-Looking Statements
Statements contained in this press release regarding matters that are not historical facts are “forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995. Such forward-looking statements include statements regarding, among other things, expected plans with respect to clinical trials, including timing of regulatory submissions and approvals and clinical data updates; anticipated timelines and milestones with respect to the Company’s development programs and manufacturing activities and capabilities; the potential capabilities and benefits of the Company’s technology platforms and product candidates, including the efficacy and safety profile of such product candidates; the quotes from Dr. Yarema and Dr. Dholaria; and the Company’s plans and strategy with respect to developing its technologies and product candidates.
Because such statements are subject to risks and uncertainties, actual results may differ materially from those expressed or implied by such forward-looking statements. These forward-looking statements are based upon the Company’s current expectations and involve assumptions that may never materialize or may prove to be incorrect. Actual results could differ materially from those anticipated in such forward-looking statements as a result of various risks and uncertainties, which include, without limitation, the Company’s reliance on third parties for various aspects of its business; risks and uncertainties associated with development and regulatory approval of novel product candidates in the biopharmaceutical industry; the Company’s ability to retain key scientific or management personnel; and the other risks described in the Company’s filings with the Securities and Exchange Commission. All forward-looking statements contained in this press release speak only as of the date on which they were made. The Company undertakes no obligation to update such statements to reflect events that occur or circumstances that exist after the date on which they were made, except as required by law.
###
| Investor Contact: | Media Contact: | |
| Alex Lobo | Sarah Thailing | |
| Stern Investor Relations | Senior Director, Corporate Communications and IR | |
| IR@poseida.com | Poseida Therapeutics, Inc. | |
| PR@poseida.com |
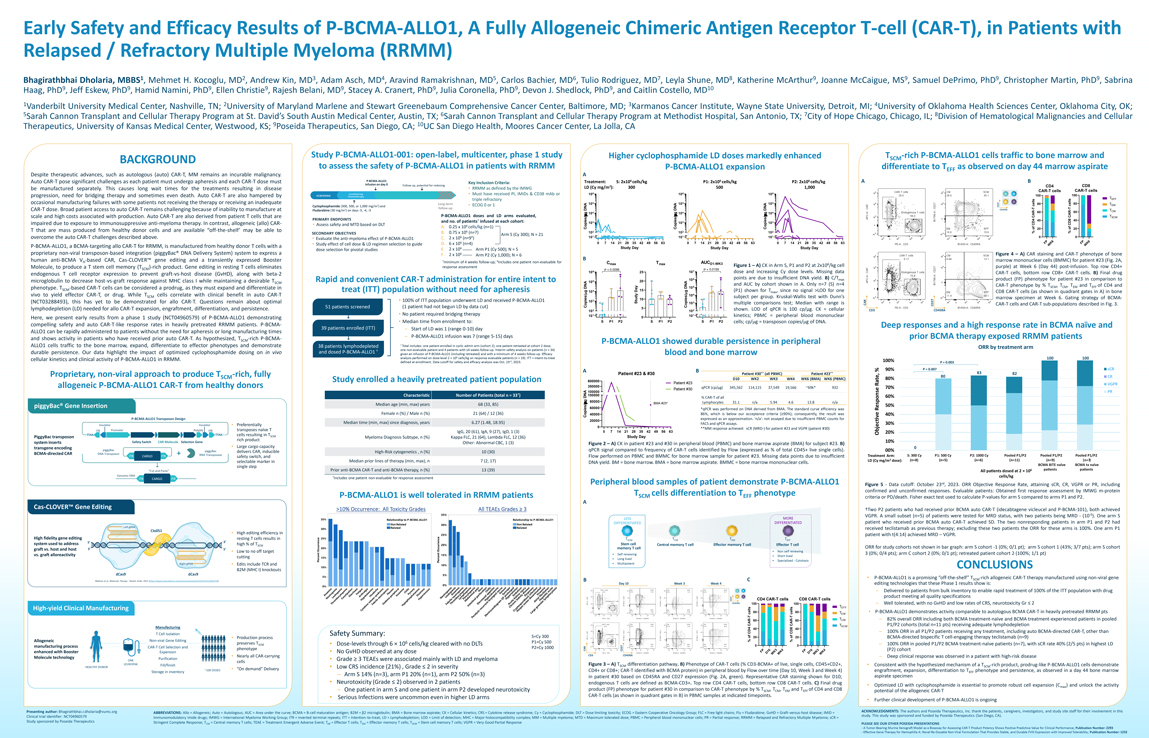
Exhibit 99.2
Early Safety and Efficacy Results of P-BCMA-ALLO1, A Fully Allogeneic Chimeric Antigen Receptor T-cell (CAR-T), in Patients with Relapsed / Refractory Multiple Myeloma (RRMM) Bhagirathbhai Dholaria, MBBS1, Mehmet H. Kocoglu, MD2, Andrew Kin, MD3, Adam Asch, MD4, Aravind Ramakrishnan, MD5, Carlos Bachier, MD6, Tulio Rodriguez, MD7, Leyla Shune, MD8, Katherine McArthur9, Joanne McCaigue, MS9, Samuel DePrimo, PhD9, Christopher Martin, PhD9, Sabrina Haag, PhD9, Jeff Eskew, PhD9, Hamid Namini, PhD9, Ellen Christie9, Rajesh Belani, MD9, Stacey A. Cranert, PhD9, Julia Coronella, PhD9, Devon J. Shedlock, PhD9, and Caitlin Costello, MD10 1Vanderbilt University Medical Center, Nashville, TN; 2University of Maryland Marlene and Stewart Greenebaum Comprehensive Cancer Center, Baltimore, MD; 3Karmanos Cancer Institute, Wayne State University, Detroit, MI; 4University of Oklahoma Health Sciences Center, Oklahoma City, OK; 5Sarah Cannon Transplant and Cellular Therapy Program at St. David’s South Austin Medical Center, Austin, TX; 6Sarah Cannon Transplant and Cellular Therapy Program at Methodist Hospital, San Antonio, TX; 7City of Hope Chicago, Chicago, IL; 8Division of Hematological Malignancies and Cellular Therapeutics, University of Kansas Medical Center, Westwood, KS; 9Poseida Therapeutics, San Diego, CA; 10UC San Diego Health, Moores Cancer Center, La Jolla, CA Study P-BCMA-ALLO1-001: open-label, multicenter, phase 1 study Higher cyclophosphamide LD doses markedly enhanced T -rich P-BCMA-ALLO1 cells traffic to bone marrow and BACKGROUND SCM to assess the safety of P-BCMA-ALLO1 in patients with RRMM P-BCMA-ALLO1 expansion differentiate to T as observed on day 44 marrow aspirate EFF Despite therapeutic advances, such as autologous (auto) CAR-T, MM remains an incurable malignancy. A Auto CAR-T pose significant challenges as each patient must undergo apheresis and each CAR-T dose must P-BCMA-ALLO1 Treatment: S: 2x106 cells/kg P1: 2x106 cells/kg P2: 2x106 cells/kg A B Key Inclusion Criteria: infusion on day 0 Follow up, potential for redosing CD8 • LD (Cy mg/m2): 300 500 1,000 CD4 be manufactured separately. This causes long wait times for the treatments resulting in disease RRMM as defined by the IMWG CAR-T cells CAR-T cells Conditioning • Must have received PI, IMiDs & CD38 mAb or 106 106 106 progression, need for bridging therapy and sometimes even death. Auto CAR-T are also hampered by SCREENING FOLLOW UP 100 100 Chemotherapy T triple refractory EFF occasional manufacturing failures with some patients not receiving the therapy or receiving an inadequate Long-term 105 105 105 80 80 T 2 • ECOG 0 or 1 A A cells cells EM Cyclophosphamide (300, 500, or 1,000 mg/m ) and NA CD27 T follow-up T—CAR-T dose. Broad patient access to auto CAR-T remains challenging because of inability to manufacture at Fludarabine (30 mg/m2) on days -5, -4, -3 D DN DN CD45RA—T R 60 60 CM g 104 g 104 g 104 scale and high costs associated with production. Auto CAR-T are also derived from patient T cells that are P-BCMA-ALLO1 doses and LD arms evaluated, mmm CA CAR T SCM PRIMARY ENDPOINTS and no. of patients† infused at each cohort: i es/ es/ i es/ i 40 40 impaired due to exposure to immunosuppressive anti-myeloma therapy. In contrast, allogeneic (allo) CAR- 103 103 103 CD4 CD8 • Assess safety and MTD based on DLT 6 A. 0.25 x 10 cells/kg (n=1) Cop Cop Cop f o of 20 20 T that are mass produced from healthy donor cells and are available “off-the-shelf’ may be able to B. 0.75 x 106 (n=7) 102 102 102 % % SECONDARY OBJECTIVES Arm S (Cy 300); N = 21 overcome the auto CAR-T challenges described above. C. 2 x 106 (n=9‡) 101 101 101 0 0 • Evaluate the anti-myeloma effect of P-BCMA-ALLO1 6 0 7 14 21 28 35 42 49 56 63 0 7 14 21 28 35 42 49 56 63 0 7 14 21 28 35 42 49 56 63 P 6 P 6 • Study effect of cell dose & LD regimen selection to guide D. 6 x 10 (n=4) F W K F W K P-BCMA-ALLO1, a BCMA-targeting allo CAR-T for RRMM, is manufactured from healthy donor T cells with a Study Day dose selection for pivotal studies E. 2 x 106 Arm P1 (Cy 500); N = 5 Study Day Study Day proprietary non-viral transposon-based integration (piggyBac® DNA Delivery System) system to express a F. 2 x 106 Arm P2 (Cy 1,000); N = 6 Figure 4 – A) CAR staining and CAR-T phenotype of bone human anti-BCMA V -based CAR, Cas-CLOVER™ gene editing and a transiently expressed Booster B marrow mononuclear cells (BMMC) for patient #23 (Fig. 2A, H †minimum of 4 weeks follow-up; ‡Includes one patient non-evaluable for C T AUCD1-WK3 max max Figure 1 – A) CK in Arm S, P1 and P2 at 2x106/kg cell Molecule, to produce a T stem cell memory (T )-rich product. Gene editing in resting T cells eliminates response assessment purple) at Week 6 (Day 44) post-infusion. Top row CD4+ SCM P = 0.0096 7 P = 0.0159 106 25 10 dose and increasing Cy dose levels. Missing data CAR-T cells, bottom row CD8+ CAR-T cells. B) Final drug endogenous T cell receptor expression to prevent graft-vs-host disease (GvHD), along with beta-2 106 points are due to insufficient DNA yield. B) C/Tmax product (FP) phenotype for patient #23 in comparison to microglobulin to decrease host-vs-graft response against MHC class I while maintaining a desirable T Rapid and convenient CAR-T administration for entire intent to 105 20 A SCM and AUC by cohort shown in A. Only n=7 (S) n=4 y 5 CAR-T phenotype by % TSCM, TCM, TEM and TEFF of CD4 and phenotype. T -based CAR-T cells can be considered a prodrug, as they must expand and differentiate in DNA DN 10 SCM 15 treat (ITT) population without need for apheresis g 104 Da g (P1) shown for Tmax, since no signal >LOD for one CD8 CAR-T cells (as shown in quadrant gates in A) in bone vivo to yield effector CAR-T, or drug. While T cells correlate with clinical benefit in auto CAR-T m m 104 SCM s/ es/ subject per group. Kruskal-Wallis test with Dunn’s marrow specimen at Week 6. Gating strategy of BCMA- 10 (NCT03288493), this has yet to be demonstrated for allo CAR-T. Questions remain about optimal • 100% of ITT population underwent LD and received P-BCMA-ALLO1 103 Study 103 51 patients screened (1 patient had not begun LD by data cut) Copie Copi multiple comparisons test; Median with range is CAR CAR-T cells and CAR-T sub-populations described in Fig. 3. lymphodepletion (LD) needed for allo CAR-T expansion, engraftment, differentiation, and persistence. 5 shown. LOD of qPCR is 100 cp/µg. CK = cellular 102 102 • No patient required bridging therapy 101 101 kinetics; PBMC = peripheral blood mononuclear Here, we present early results from a phase 1 study (NCT04960579) of P-BCMA-ALLO1 demonstrating 0 • Median time from enrollment to: S P1 P2 S P1 P2 S P1 P2 cells; cp/mg = transposon copies/mg of DNA. compelling safety and auto CAR-T-like response rates in heavily pretreated RRMM patients. P-BCMA- Deep responses and a high response rate in BCMA naïve and 39 patients enrolled (ITT) – Start of LD was 1 (range 0-10) day ALLO1 can be rapidly administered to patients without the need for apheresis or long manufacturing times and shows activity in patients who have received prior auto CAR-T. As hypothesized, T -rich P-BCMA- – P-BCMA-ALLO1 infusion was 7 (range 5-15) days prior BCMA therapy exposed RRMM patients SCM P-BCMA-ALLO1 showed durable persistence in peripheral ALLO1 cells traffic to the bone marrow, expand, differentiate to effector phenotypes and demonstrate 38 patients lymphodepleted † Total includes: one patient enrolled in cyclic admin arm (cohort 2); one patient retreated at cohort 2 dose; and dosed P-BCMA-ALLO1 † one non-evaluable patient and 4 patients with 4 weeks follow-up. Interim safety analysis on patients (n = 34) durable persistence. Our data highlight the impact of optimized cyclophosphamide dosing on in vivo given an infusion of P-BCMA-ALLO1 (including retreated) and with a minimum of 4 weeks follow-up. Efficacy blood and bone marrow cellular kinetics and clinical activity of P-BCMA-ALLO1 in RRMM. analysis performed on dose-level 2 × 106 cells/kg on response evaluable patients (n = 19). ITT = intent-to-treat defined at enrollment. Data cutoff for safety and efficacy analysis was Oct. 23rd, 2023. 3 A B sCR Proprietary, non-viral approach to produce T -rich, fully Patient #23 & #30 Patient #30** (all PBMC) Patient #23** 3 SCM CR Study enrolled a heavily pretreated patient population D10 WK2 WK3 WK4 WK6 (BMA) WK6 (PBMC) 600000 Patient #23 GPR allogeneic P-BCMA-ALLO1 CAR-T from healthy donors 350000 qPCR (cp/µg) 345,562 114,115 37,549 19,566 ~69k* 932 Patient #30 † 100000 PR Characteristic Number of Patients (total n = 33 ) DNA 100000 % CAR-T of all g 80000 Lymphocytes 31.1 n/a 5.94 4.6 13.8 n/a Median age (min, max) years 68 (33, 85)m BMA #23* piggyBac® Gene Insertion 5 60000 *qPCR was performed on DNA derived from BMA. The standard curve efficiency was Female n (%) / Male n (%) 21 (64) / 12 (36) Copies/ 40000 86%, which is below our acceptance criteria ( 90%); consequently, the result was P-BCMA-ALLO1 Transposon Design expressed as an approximation. ‘n/a’: not assayed due to insufficient PBMC counts for 20000 Median time (min, max) since diagnosis, years 6.27 (1.48, 18.95) FACS and qPCR assays. 3 Insulator Insulator • Preferentially 0 **MM response achieved: sCR (MRD-) for patient #23 and VGPR (patient #30) ITR Promoter Poly(A) ITR transposes naïve T IgG, 20 (61), IgA, 9 (27), IgD, 1 (3) 0 7 14 21 28 35 42 49 56 63 TTAA TTAA cells resulting in T PiggyBac transposon SCM Myeloma Diagnosis Subtype, n (%) Kappa FLC, 21 (64), Lambda FLC, 12 (36) Study Day rich product system inserts Safety Switch CAR Molecule Selection Gene Other: Abnormal CBC, 1 (3) Figure 2 – A) CK in patient #23 and #30 in peripheral blood (PBMC) and bone marrow aspirate (BMA) for subject #23. B) transgene encoding • Large cargo capacity piggyBac piggyBac delivers CAR, inducible High-Risk cytogenetics , n (%) 10 (30) qPCR signal compared to frequency of CAR-T cells identified by Flow (expressed as % of total CD45+ live single cells). BCMA-directed CAR DNA Transposon RNA Transposase ITR CARGO ITR safety switch, and Flow performed on PBMC and BMMC for bone marrow sample for patient #23. Missing data points due to insufficient 3 5 selectable marker in Median prior lines of therapy (min, max), n 7 (2, 17) 5 DNA yield. BM = bone marrow. BMA = bone marrow aspirate. BMMC = bone marrow mononuclear cells. single step Prior anti-BCMA CAR-T and anti-BCMA therapy, n (%) 13 (39) “Cut and Paste” Genomic DNA †Includes one patient non-evaluable for response assessment ITR CARGO ITR Peripheral blood samples of patient demonstrate P-BCMA-ALLO1 Figure 5—Data cutoff: October 23rd, 2023. ORR Objective Response Rate, attaining sCR, CR, VGPR or PR, including T cells differentiation to T phenotype confirmed and unconfirmed responses. Evaluable patients: Obtained first response assessment by IMWG m-protein P-BCMA-ALLO1 is well tolerated in RRMM patients SCM EFF criteria or PD/death. Fisher exact test used to calculate P-values for arm S compared to arms P1 and P2. Cas-CLOVER™ Gene Editing A †Two P2 patients who had received prior BCMA auto CAR-T (idecabtagene vicleucel and P-BCMA-101), both achieved VGPR. A small subset (n=5) of patients were tested for MRD status, with two patients being MRD—(10-5). One arm S LESS MORE patient who received prior BCMA auto CAR-T achieved SD. The two nonresponding patients in arm P1 and P2 had DIFFERENTIATED DIFFERENTIATED Left gRNA received teclistamab as previous therapy; excluding these two patients the ORR for these arms is 100%. One arm P1 Clo051 • High editing efficiency in patient with t(4:14) achieved MRD – VGPR. High fidelity gene editing resting T cells results in SCM CM EM EFF system used to address 5’ 3’ high % of T Stem cell Central memory T cell Effector memory T cell Effector T cell SCM ORR for study cohorts not shown in bar graph: arm S cohort -1 (0%; 0/1 pt); arm S cohort 1 (43%; 3/7 pts); arm S cohort graft vs. host and host 3’ 5’ memory T cell • Low to no off target • Non self renewing 3 (0%; 0/4 pts); arm C cohort 2 (0%; 0/1 pt); retreated patient cohort 2 (100%; 1/1 pt) vs. graft alloreactivity • Self renewing cutting • Short lived • Long lived • Specialized—Cytotoxic Right gRNA • Edits include TCR and • Multipotent CONCLUSIONS B2M (MHC I) knockouts dCas9 dCas9 C • P-BCMA-ALLO1 is a promising “off-the-shelf” TSCM-rich allogeneic CAR-T therapy manufactured using non-viral gene Madison et al., Molecular Therapy – Nucleic Acids, 2022. (https://www.sciencedirect.com/science/article/pii/S216225312200155X) B Day 10 Week 3 Week 4 editing technologies that these Phase 1 results show is: – Delivered to patients from bulk inventory to enable rapid treatment of 100% of the ITT population with drug product meeting all quality specifications CD27 CD4 CAR-T cells CD8 CAR-T cells CD45RA 100 100 – Well tolerated, with no GvHD and low rates of CRS, neurotoxicity Gr 2 High-yield Clinical Manufacturing TEFF cells 80 cells 80 T • P-BCMA-ALLO1 demonstrates activity comparable to autologous BCMA CAR-T in heavily pretreated RRMM pts EM T T—60—TCM – 82% overall ORR including both BCMA treatment-naïve and BCMA treatment-experienced patients in pooled CAR CAR 60 TSCM P1/P2 cohorts (total n=11 pts) receiving adequate lymphodepletion Manufacturing 40 40 CD4 CD8 – 100% ORR in all P1/P2 patients receiving any treatment, including auto BCMA-directed CAR-T, other than T Cell Isolation Safety Summary: S=Cy 300 of of • Production process 20 20 BCMA-directed bispecific T cell-engaging therapy teclistamab (n=9) Allogeneic Non-viral Gene Editing P1=Cy 500 % % preserves T • Dose-levels through 6 × 106 cells/kg cleared with no DLTs – 100% ORR in pooled P1/P2 BCMA treatment-naïve patients (n=7), with sCR rate 40% (2/5 pts) in highest LD SCM 0 0 phenotype P2=Cy 1000 CAR (P2) cohort P 0 3 4 P 0 3 4 • No GvHD observed at any dose F 1 K K F 1 K K CD3 CD45RA D W W D W W • Nearly all CAR-carrying • – Deep clinical response was observed in a patient with high-risk disease Grade 3 TEAEs were associated mainly with LD and myeloma cells Figure 3 – A) TSCM differentiation pathway. B) Phenotype of CAR-T cells (% CD3-BCMA+ of live, single cells, CD45+CD2+, • Consistent with the hypothesized mechanism of a T -rich product, prodrug-like P-BCMA-ALLO1 cells demonstrate ON • • Low CRS incidence (21%) , Grade 2 in severity SCM DOSES “On demand” Delivery CD4+ or CD8+; CAR-T identified with BCMA protein) in peripheral blood by Flow over time (Day 10, Week 3 and Week 4) engraftment, expansion, differentiation to T phenotype and persistence, as observed in a day 44 bone marrow Arm S 14% (n=3), arm P1 20% (n=1), arm P2 50% (n=3) EFF in patient #30 based on CD45RA and CD27 expression (Fig. 2A, green). Representative CAR staining shown for D10; aspirate specimen • Neurotoxicity (Grade 2) observed in 2 patients endogenous T cells are defined as BCMA-CD3+. Top row CD4 CAR-T cells, bottom row CD8 CAR-T cells. C) Final drug • Optimized LD with cyclophosphamide is essential to promote robust cell expansion (Cmax) and unlock the activity One patient in arm S and one patient in arm P2 developed neurotoxicity product (FP) phenotype for patient #30 in comparison to CAR-T phenotype by % TSCM, TCM, TEM and TEFF of CD4 and CD8 potential of the allogeneic CAR-T • Serious Infections were uncommon even in higher LD arms CAR-T cells (as shown in quadrant gates in B) in PBMC samples at indicated timepoints. • Further clinical development of P-BCMA-ALLO1 is ongoing vu ACKNOWLEDGMENTS: The authors and Poseida Therapeutics, Inc. thank the patients, caregivers, investigators, and study site staff for their involvement in this Auto = Autologous; AUC = Area under the curve; BCMA = B-cell maturation antigen; B2M = 2 microglobulin; BMA = Bone marrow aspirate; CK = Cellular kinetics; CRS = Cytokine release syndrome; Cy = Cyclophosphamide; DLT = Dose limiting toxicity; ECOG = Eastern Cooperative Oncology Group; FLC = Free light chains; Flu = Fludarabine; GvHD = Graft-versus-host disease; IMiD = study. This study was sponsored and funded by Poseida Therapeutics (San Diego, CA). MWG = International Myeloma Working Group; ITR = inverted terminal repeats; ITT = Intention-to-treat; LD = Lymphodepletion; LOD = Limit of detection; MHC = Major histocompatibility complex; MM = Multiple myeloma; MTD = Maximum tolerated dose; PBMC = Peripheral blood mononuclear cells; PR = Partial response; RRMM = Relapsed and Refractory Multiple Myeloma; sCR = = Central memory T cells; TEAE = Treatment Emergent Adverse Event; Teff = Effector T cells; TEM = Effector memory T cells; TSCM = Stem cell memory T cells; VGPR = Very Good Partial Response PLEASE SEE OUR OTHER POSEIDA PRESENTATIONS—A Tumor-Bearing Murine Xenograft Model as a Bioassay for Assessing CAR-T Product Potency Shows Positive Predictive Value for Clinical Performance; Publication Number: 2293—Effective Gene Therapy for Hemophilia A: Novel Re-Dosable Non-Viral Formulation That Provides Stable, and Durable FVIII Expression with Improved Tolerability; Publication Number: 1232