Galectin Therapeutics Presented NAVIGATE Trial Results at the American Association for the Study of Liver Diseases (AASLD) 2025 Annual Meeting
|
• |
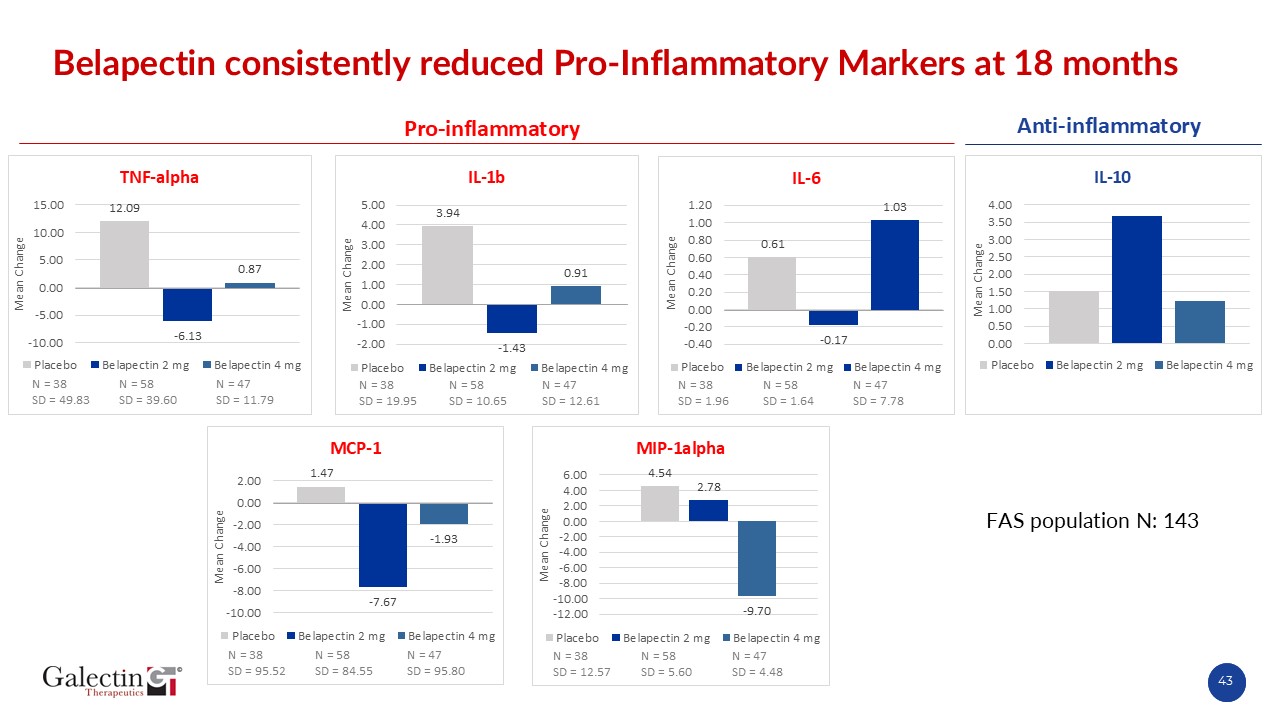
New biomarker analyses from the NAVIGATE trial demonstrated consistent antifibrotic effects of belapectin 2 mg/kg
|
|
• |
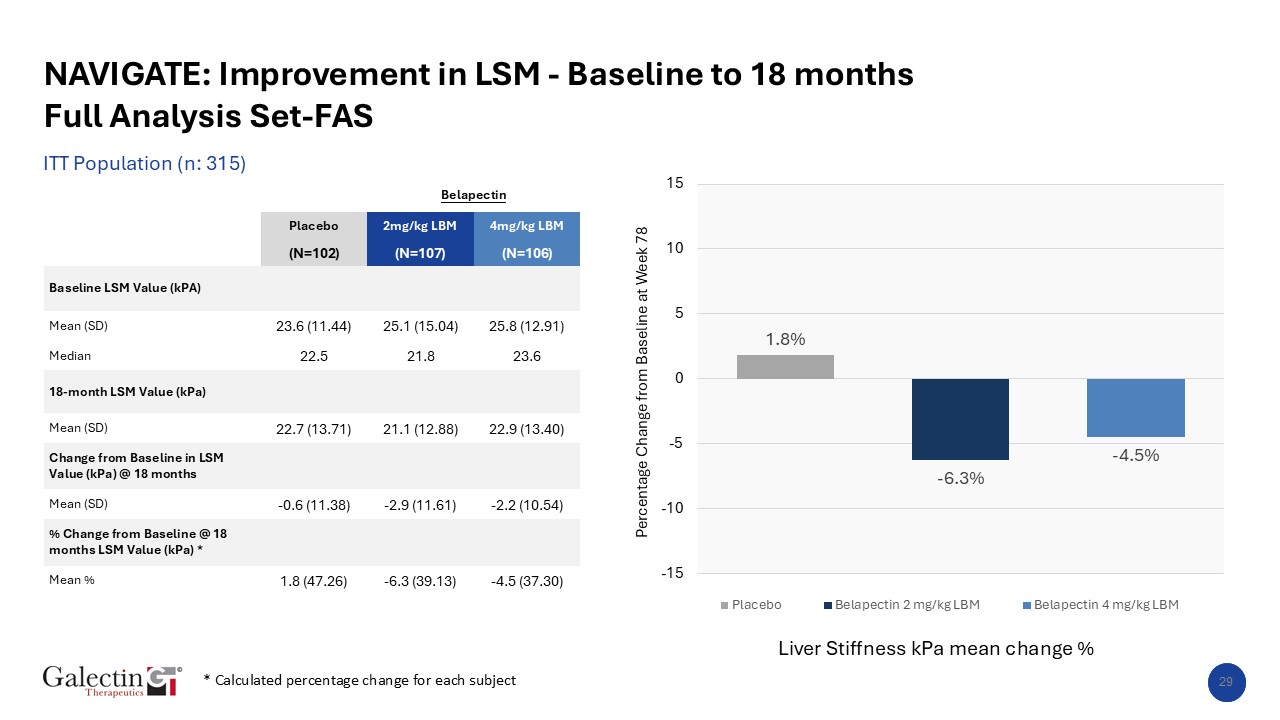
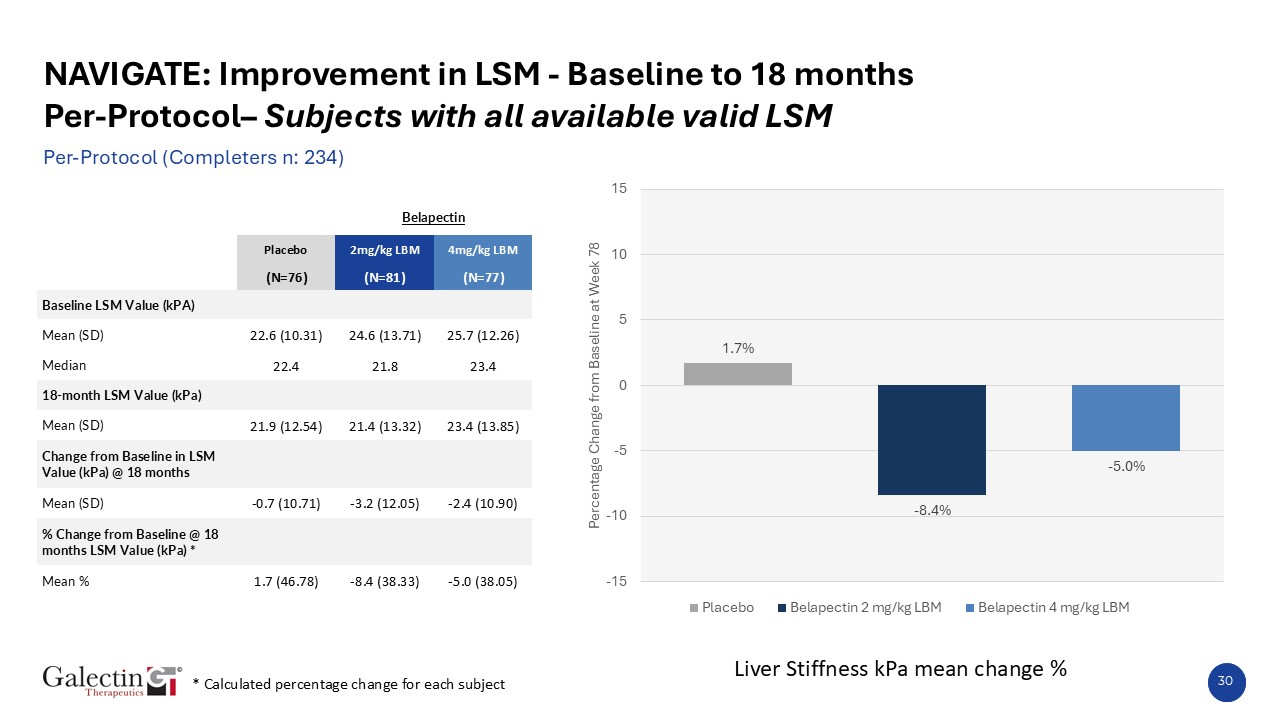
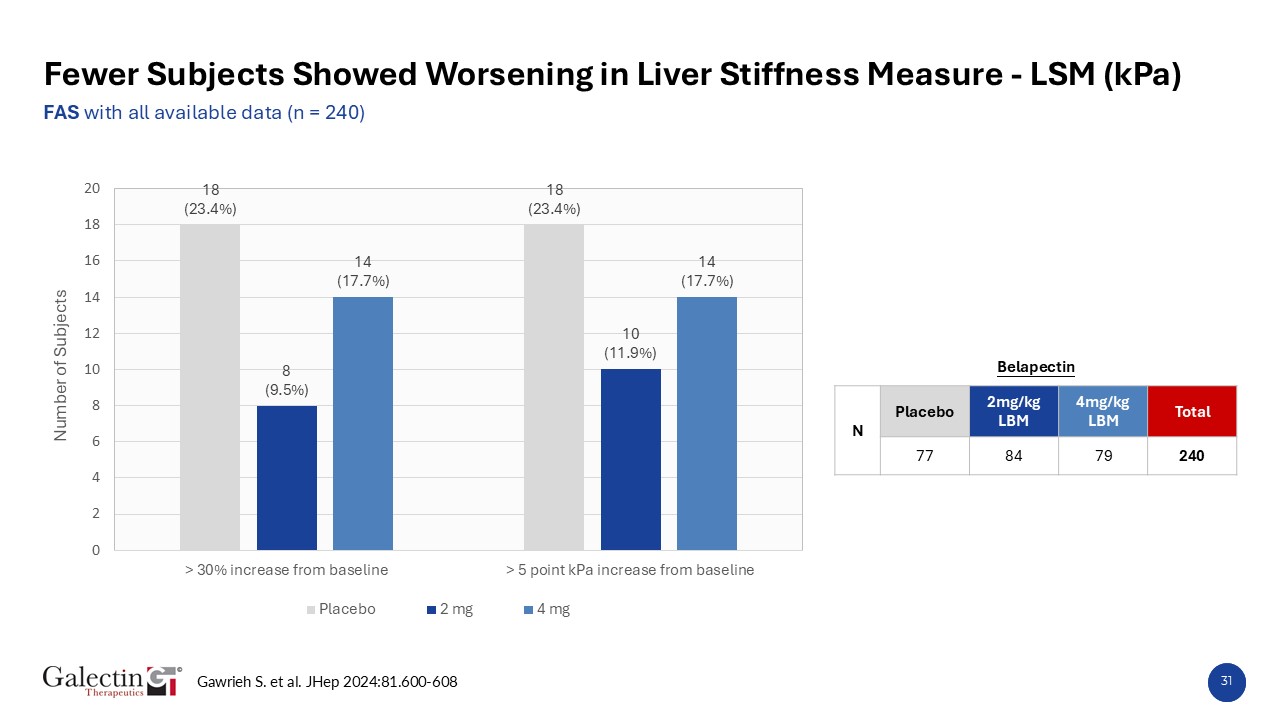
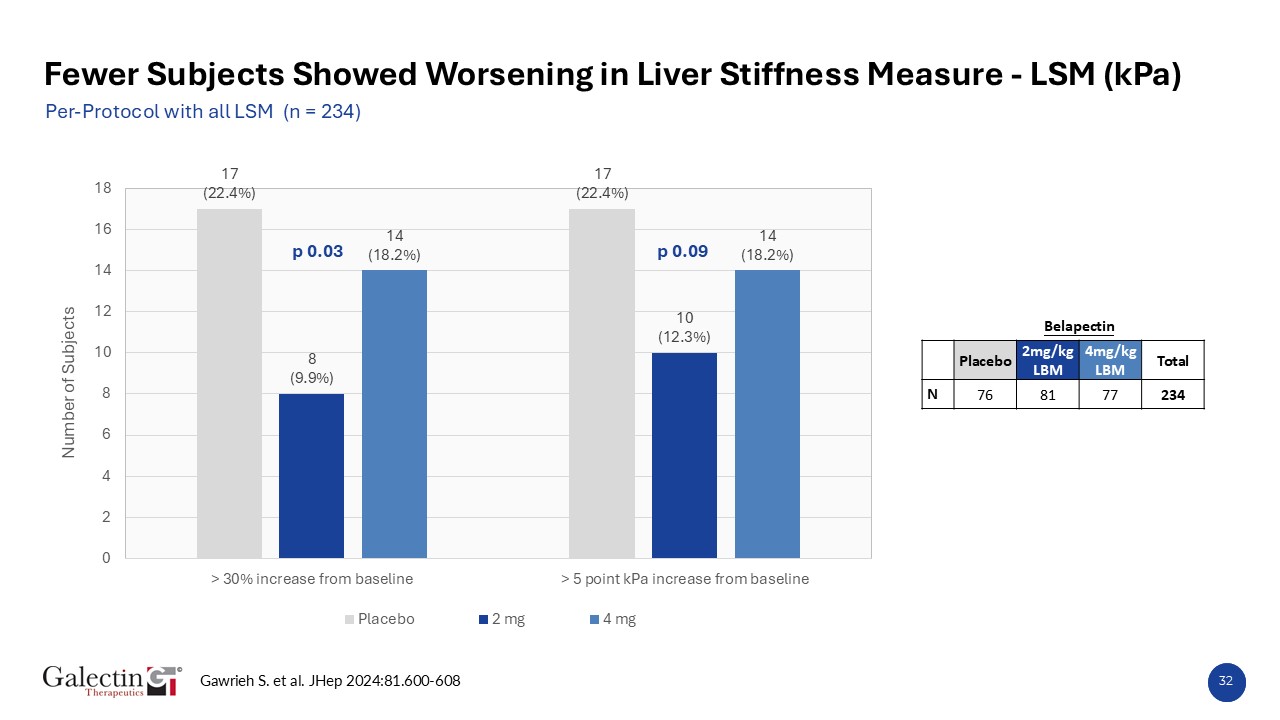
Using established criteria for clinically meaningful worsening, a lower proportion of patients treated with belapectin 2 mg/kg experienced ≥30% or ≥5 kPa increases in liver stiffness (LSM) by FibroScan®
compared with placebo, indicating slowing of fibrosis progression and stabilization of liver function
|
|
• |
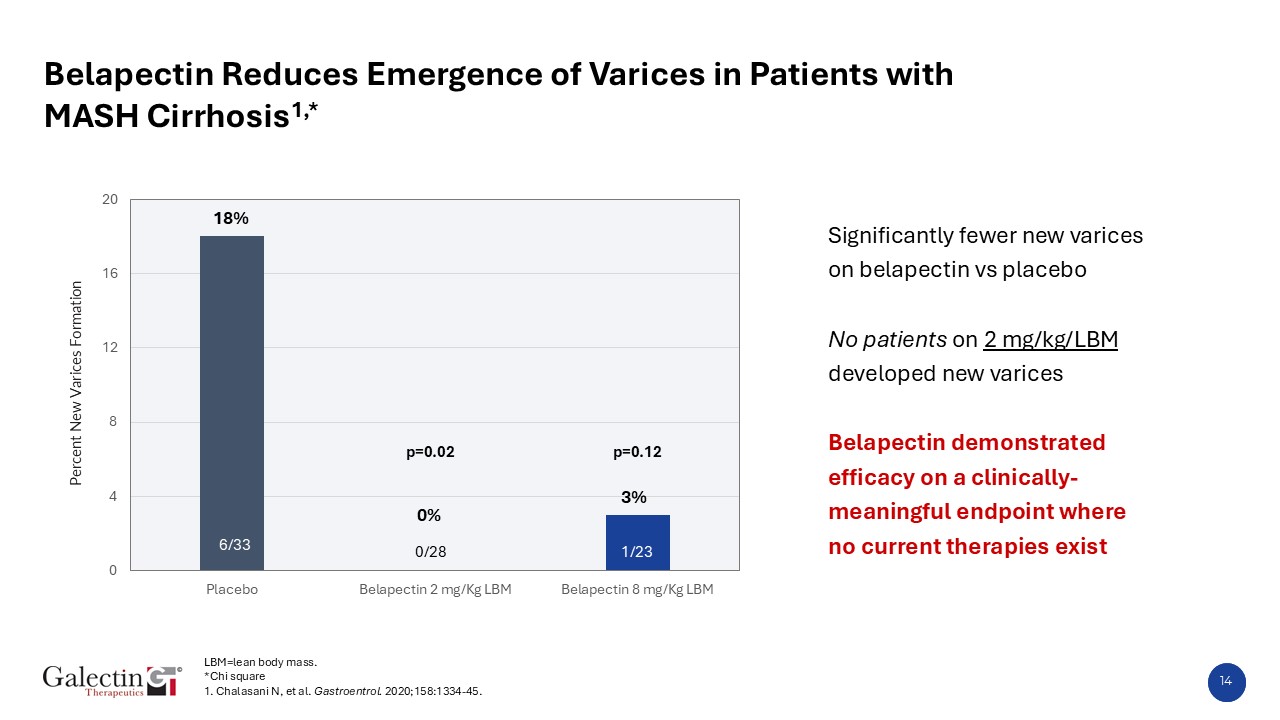
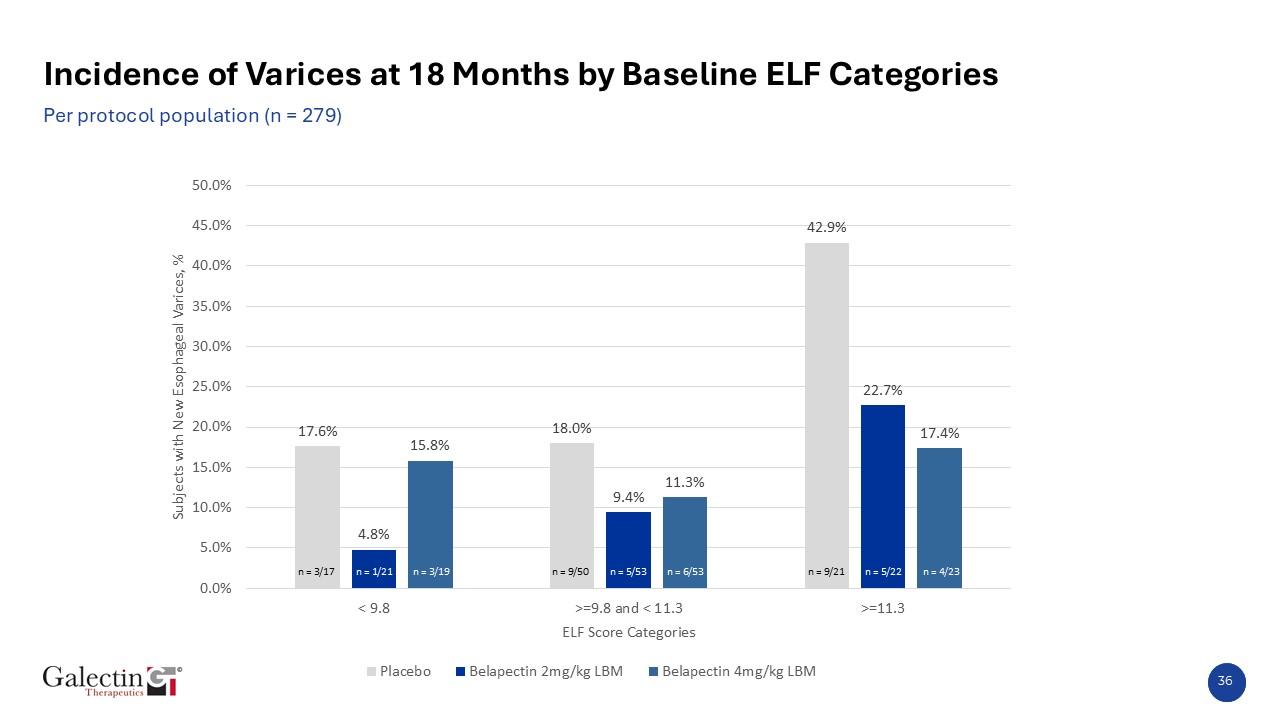
Across all ELF fibrosis risk categories, belapectin 2 mg/kg showed a lower incidence of new varices compared with placebo, with the largest benefit in patients with ELF > 11.3 (22.7% vs 42.9%),
representing those at highest risk for liver complications
|
|
• |
Pro-C3 biomarker analysis demonstrated a >50% reduction from baseline at 18 months with belapectin 2 mg/kg versus placebo, supporting the therapy’s antifibrotic and disease-modifying potential in
compensated MASH cirrhosis with portal hypertension.
|
|
• |
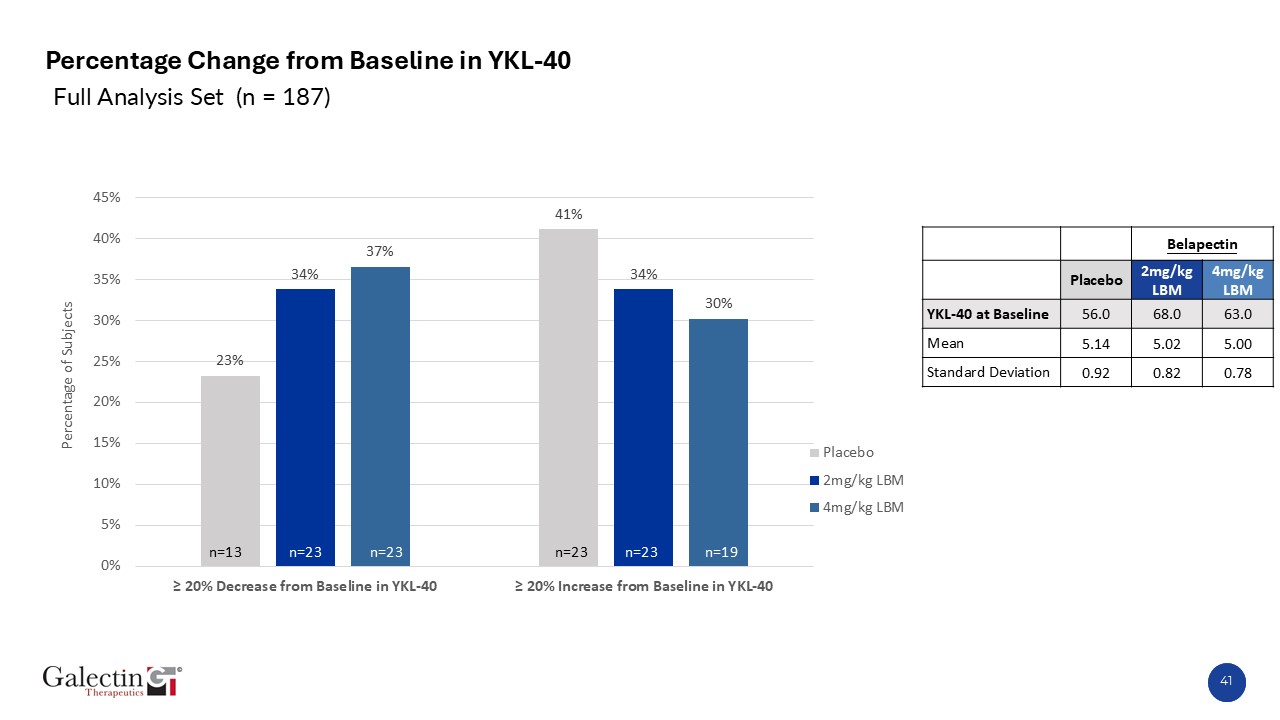
Analysis of YKL-40, a biomarker associated with Galectin-3 upregulation in fibrotic liver disease, demonstrated a ≥20% reduction in a higher proportion of patients treated with belapectin 2 mg/kg compared
with placebo, providing additional mechanistic evidence of belapectin’s antifibrotic activity.
|
|
• |
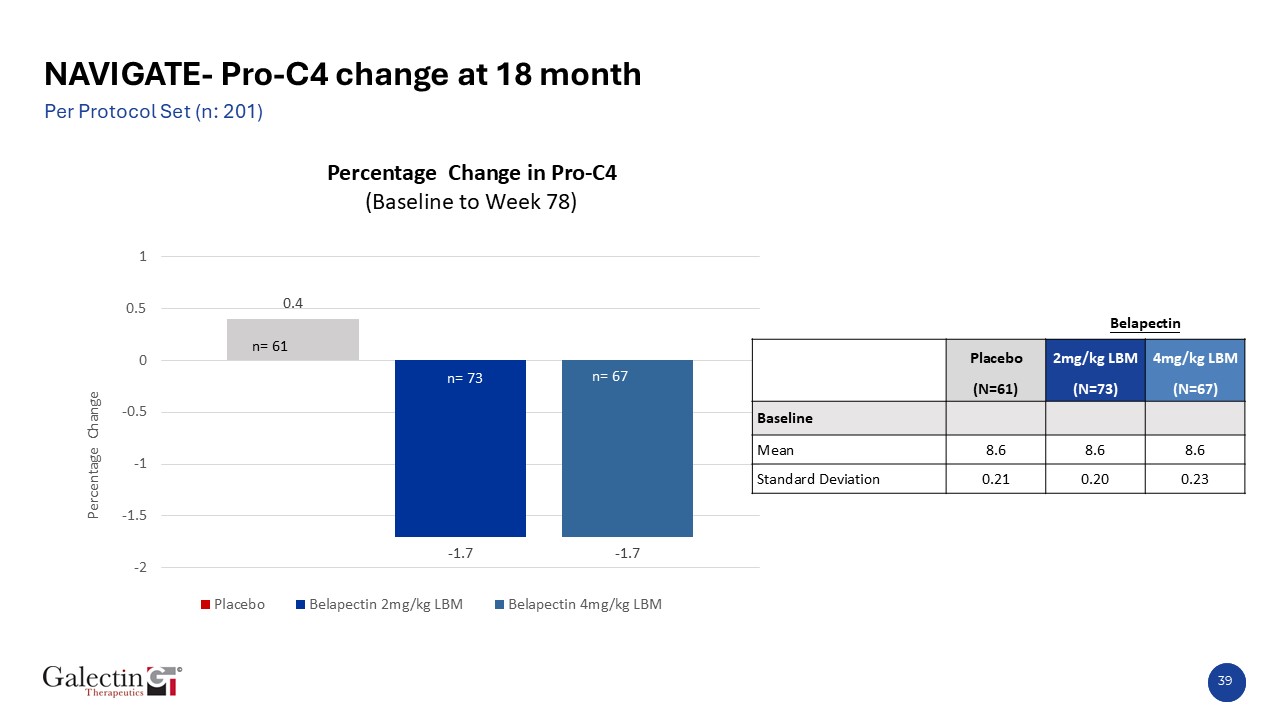
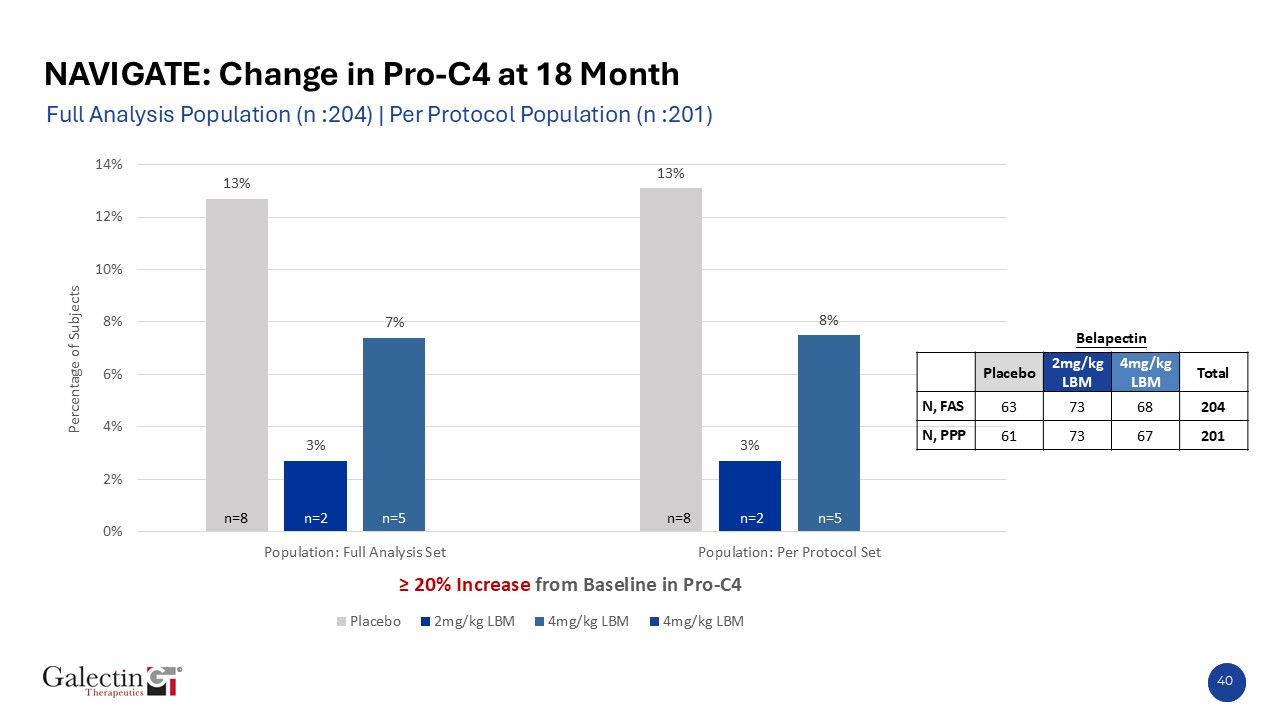
Analysis of PRO-C4, a key biomarker of liver injury and fibrogenesis, showed a ≥20% increase in a higher proportion of placebo-treated patients compared with those receiving belapectin 2 mg/kg, consistent
with ongoing fibrotic progression and further supporting belapectin’s disease-modifying potential
|
|
• |
For available patients who completed 36 months of therapy, belapectin maintained the sustained reduction in new variceal development seen at 18 months
|
NORCROSS, Ga., Nov 10, 2025 (GLOBE NEWSWIRE) -- Galectin Therapeutics Inc. (NASDAQ:GALT), the leading developer of galectin-3-targeted therapeutics for patients with MASH cirrhosis and
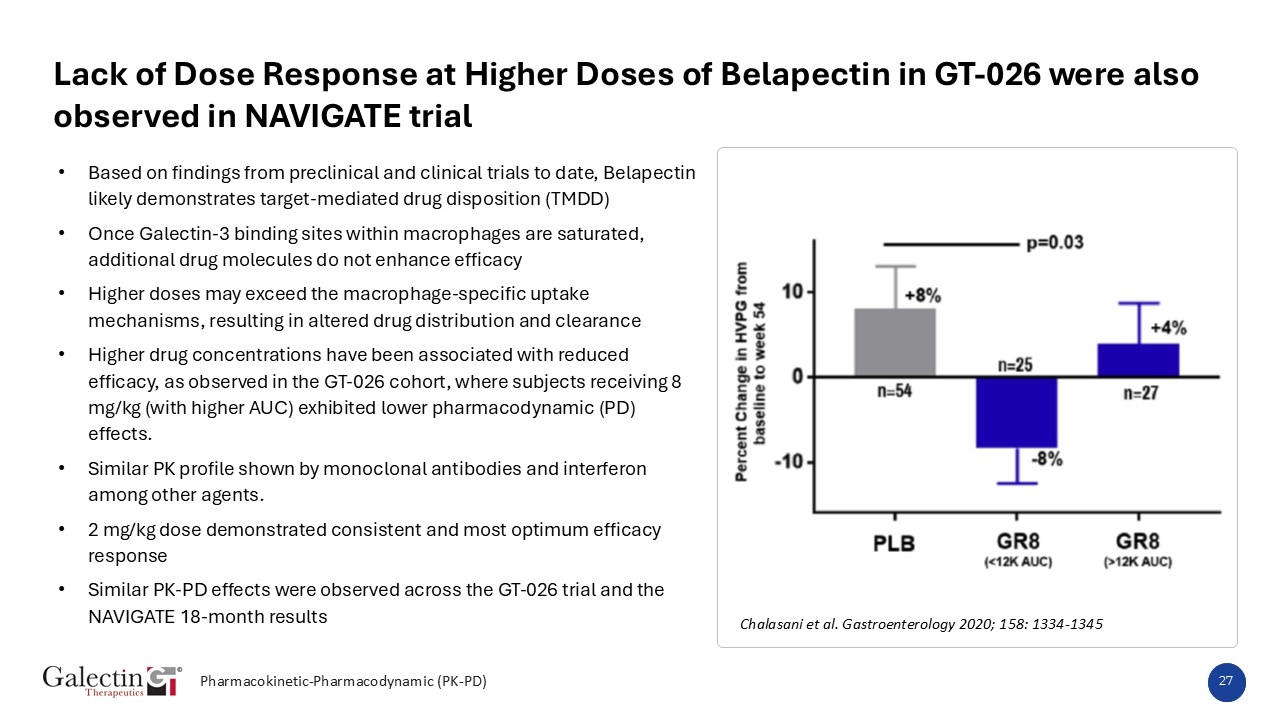
portal hypertension, presented a poster and will deliver an oral presentation of the NAVIGATE study analysis at the AASLD 2025 Annual Meeting. The Phase 2 NAVIGATE trial evaluated belapectin, a proprietary galectin-3 inhibitor, in patients with
compensated MASH cirrhosis and portal hypertension.
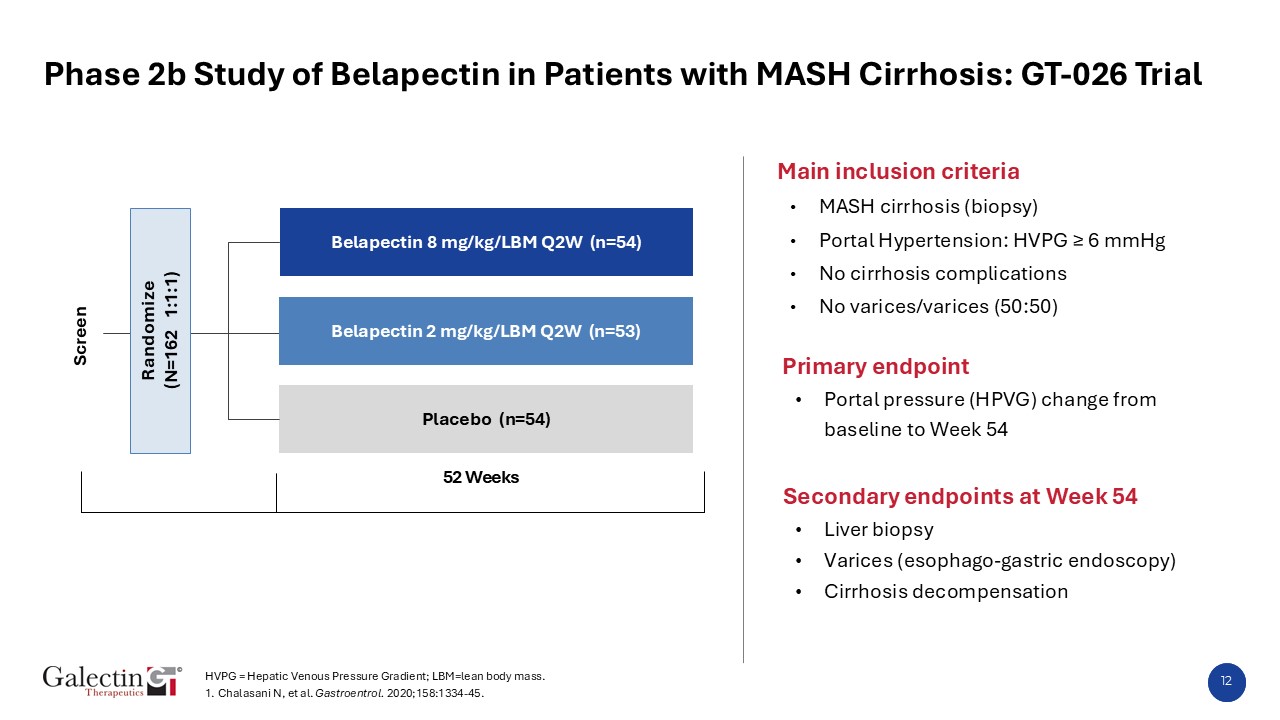
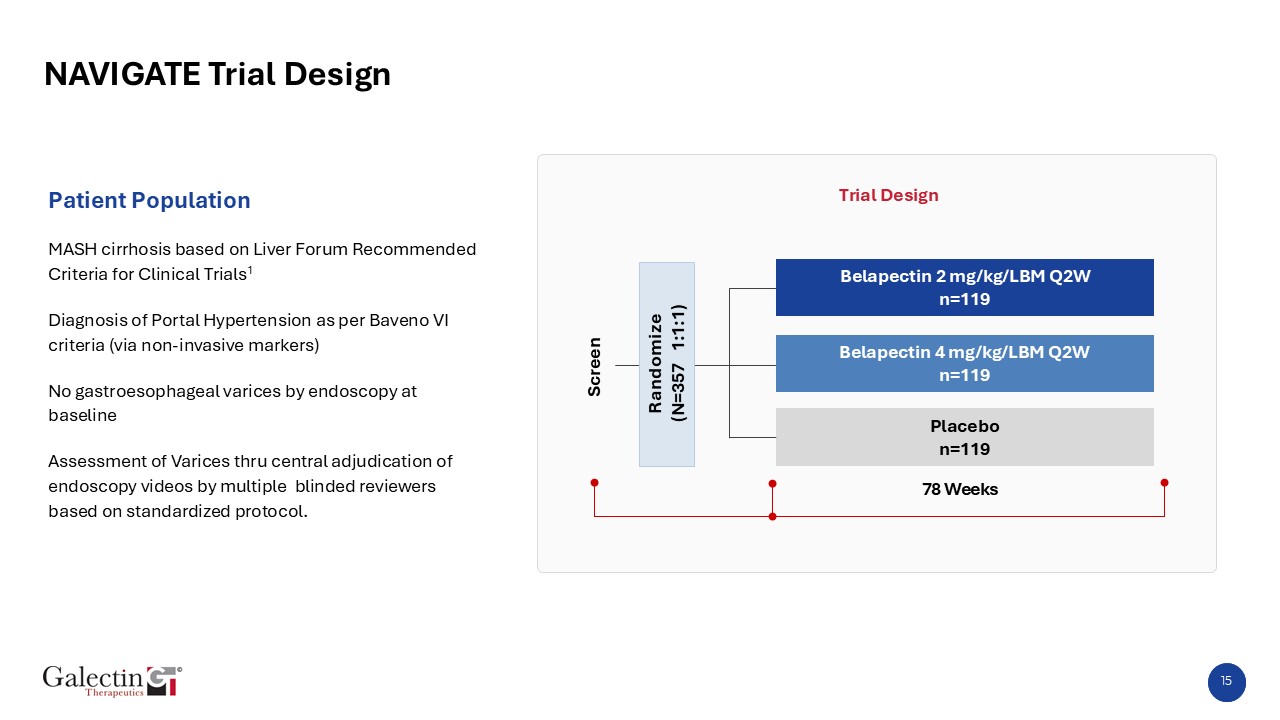
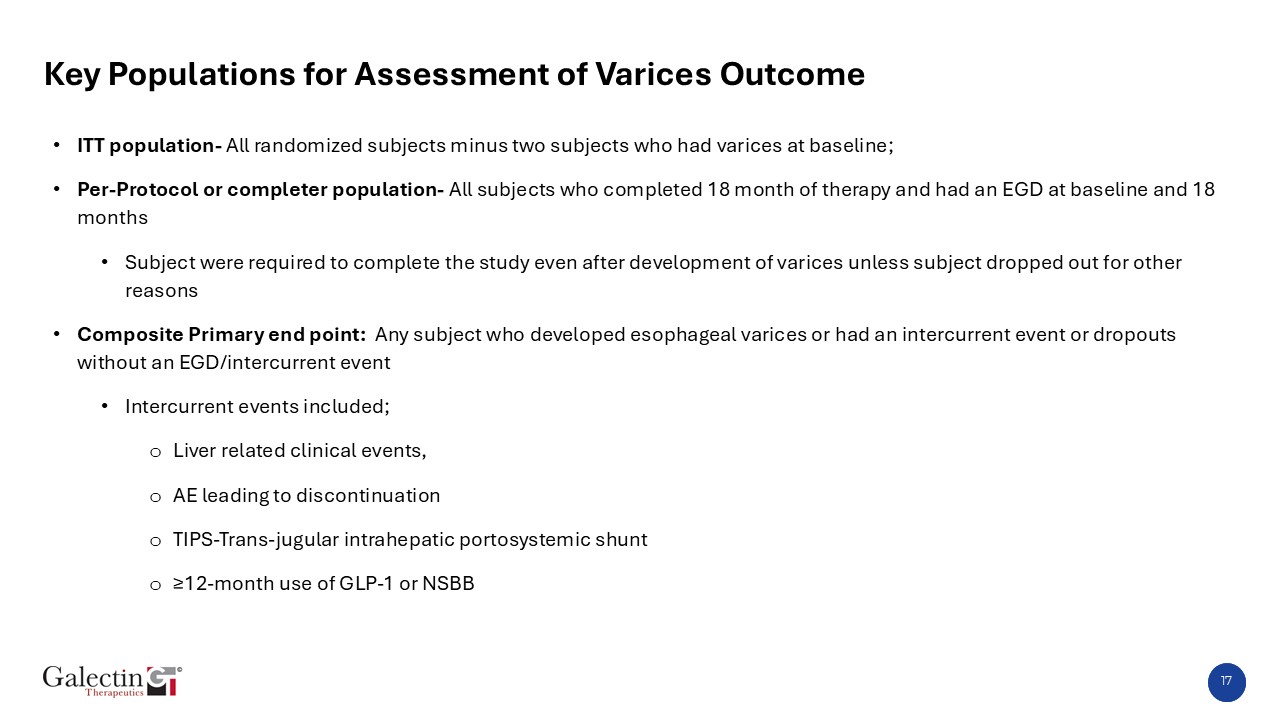
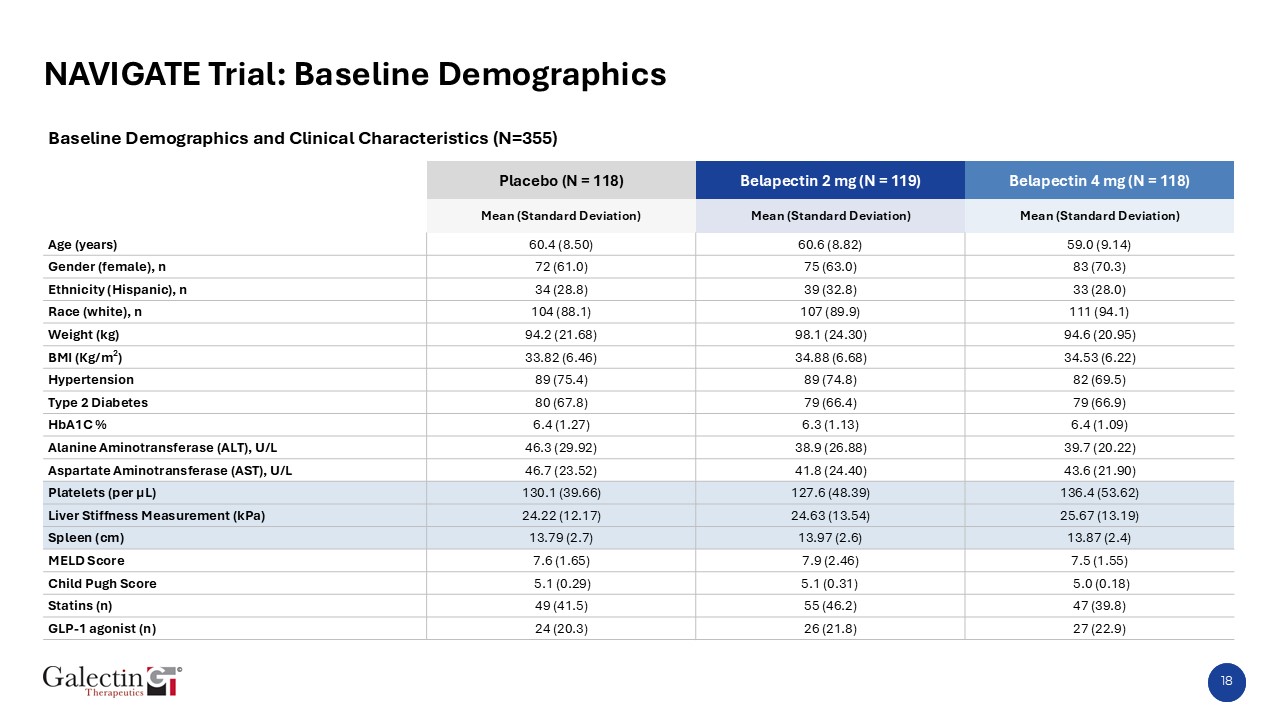
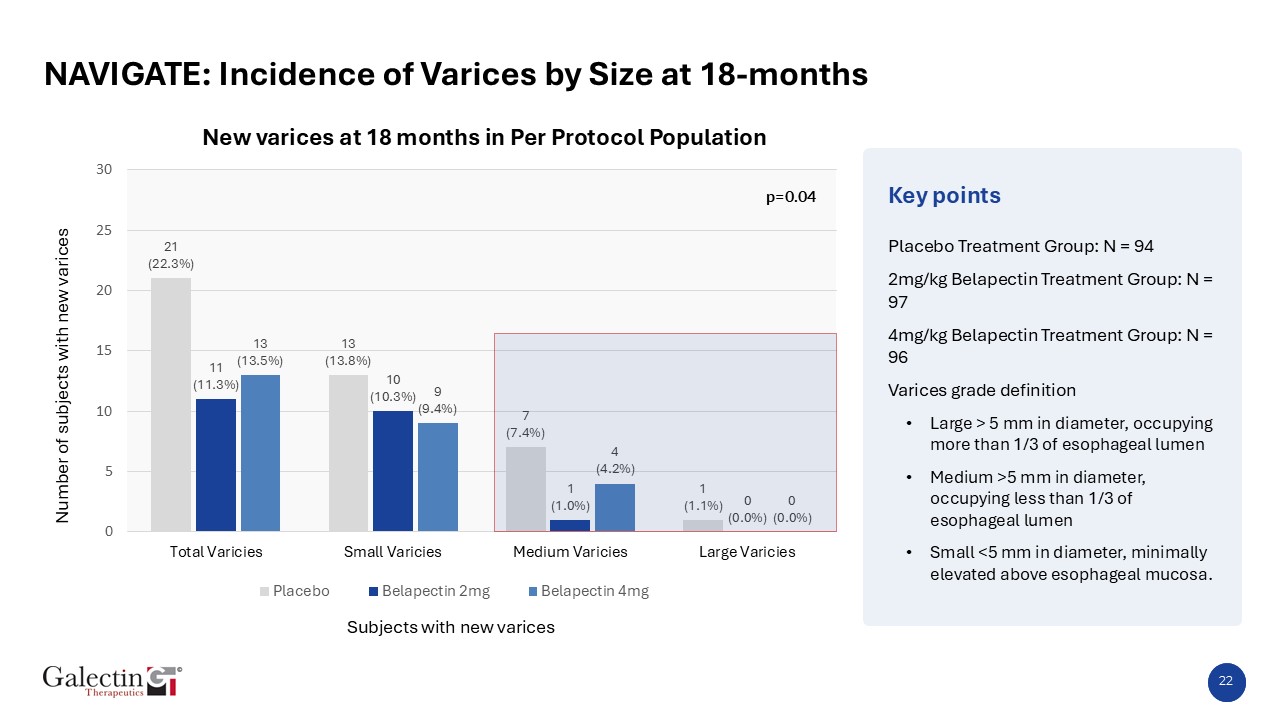
The global Phase 2b NAVIGATE trial (NCT04365868) was a randomized, double-blind, placebo-controlled study evaluating the galectin-3 inhibitor belapectin in 355 patients with compensated MASH
cirrhosis and portal hypertension confirmed by non-invasive markers and baseline endoscopy. Patients were randomized 1:1:1 to receive intravenous belapectin at 2 mg/kg or 4 mg/kg of lean body mass or placebo every other week for 18 months (78
weeks).
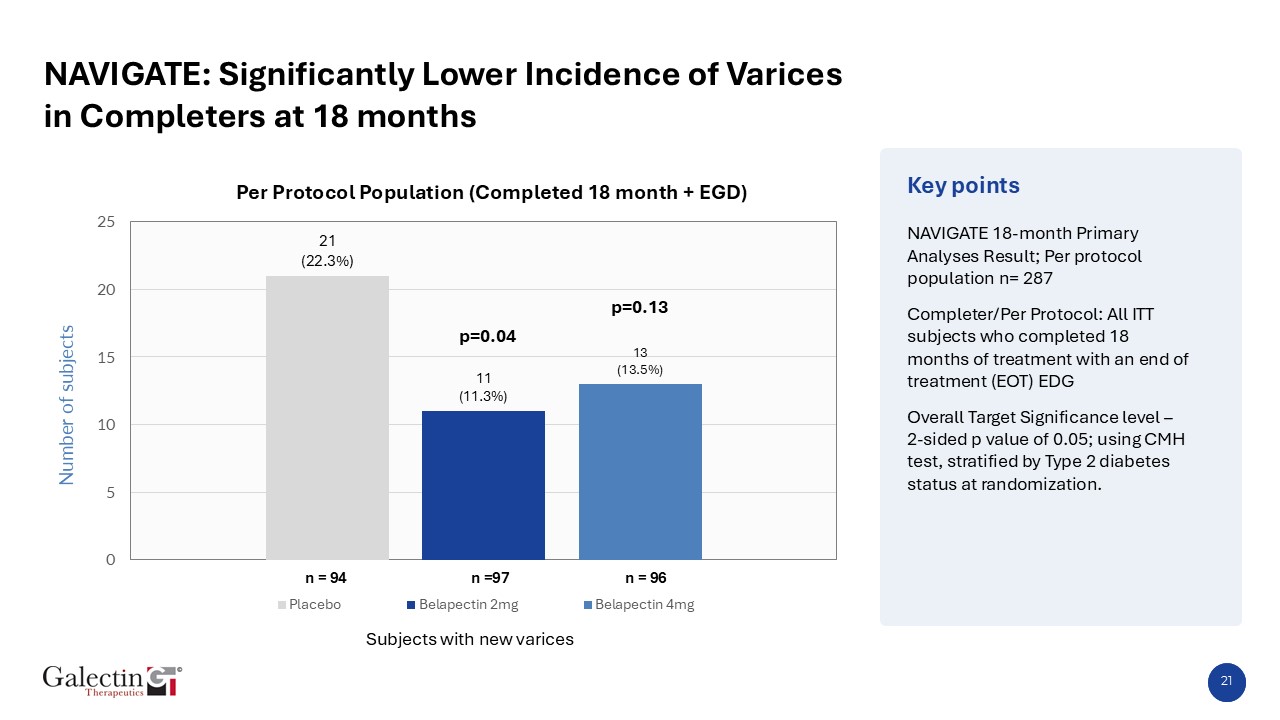
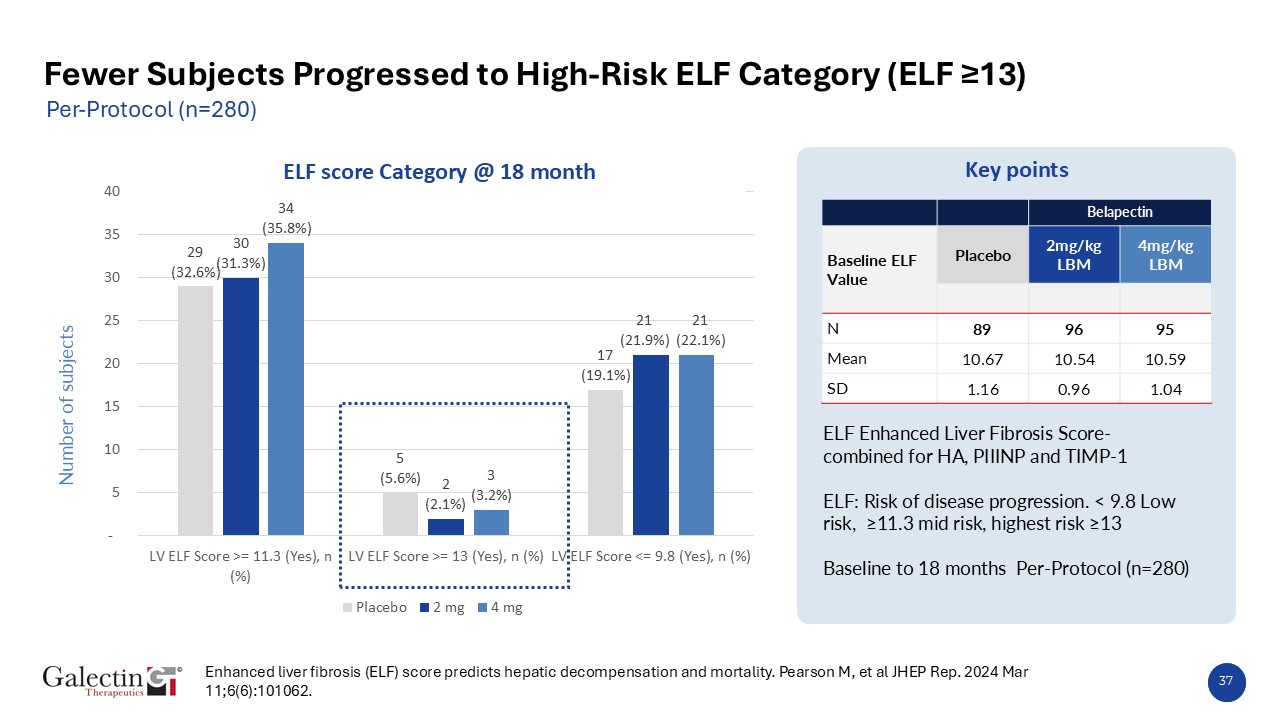
When patients were stratified using FDA-approved Enhanced Liver Fibrosis (ELF) score cutoffs, belapectin 2 mg/kg demonstrated a consistently lower incidence of new varices across all fibrosis
categories, with the largest reduction observed among patients with ELF >11.3, representing those at highest risk for liver complications (22.7% vs 42.9% for placebo). Incidences across ELF strata were as follows:
| |
Subjects with New Esophageal Varices by Baseline ELF Categories at 18 Months %, n=245
|
|
placebo
|
2 mg/kg
belapectin
|
4mg/kg
belapectin
|
| |
ELF score < 9.8
|
|
17.6% (3/17)
|
4.8% (1/21)
|
15.8% (3/19)
|
| |
|
|
|
|
|
| |
ELF score between < 9.8 and <11.3
|
|
18% (9/50)
|
9.4% (5/53)
|
11.3% (6/53)
|
| |
|
|
|
|
|
| |
ELF score > 11.3
|
|
42.9% (9/21)
|
22.7% (5/22)
|
17.4% (4/23)
|
Note: ELF: Risk of disease progression. < 9.8 Low risk, ≥11.3 mid risk, highest risk ≥13
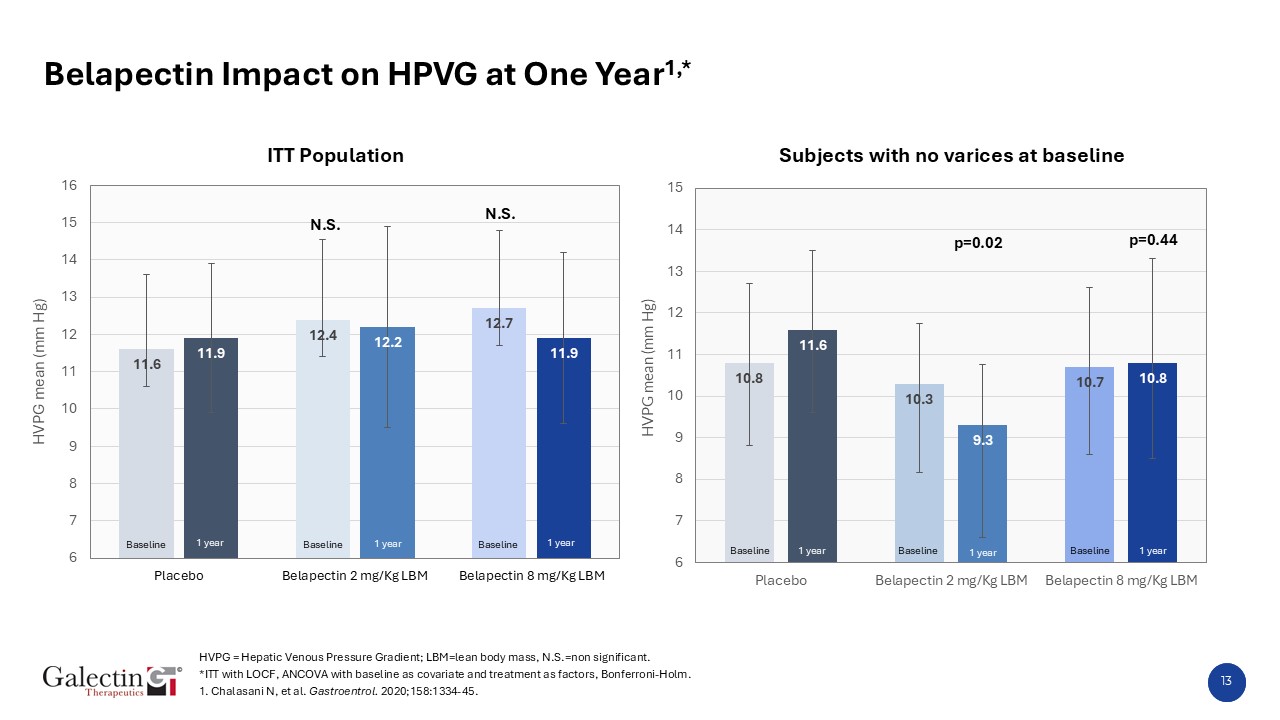
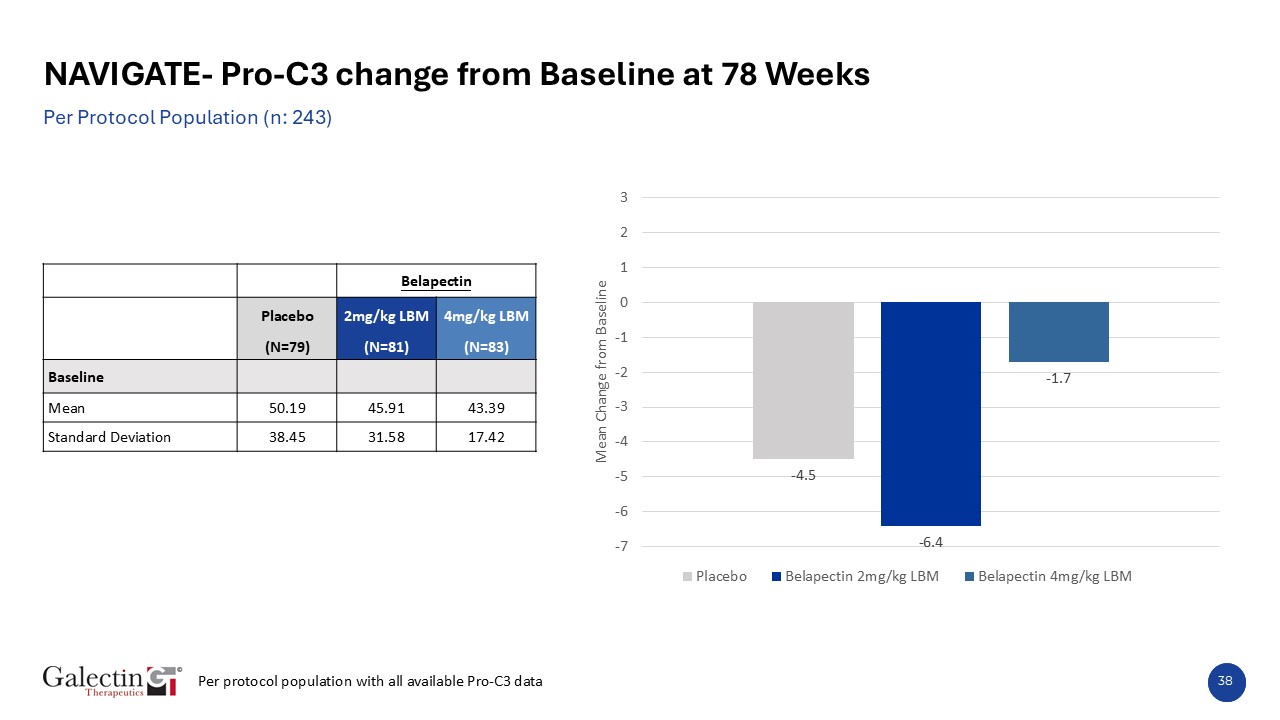
Additionally, analysis of the Pro-C3 fibrosis biomarker showed that baseline levels were comparable across all groups (placebo: 50.2 ng/mL; 2 mg/kg: 45.9 ng/mL; 4 mg/kg: 43.4 ng/mL). At 78 weeks,
patients receiving 2 mg/kg belapectin achieved a mean –6.4 ng/mL reduction in Pro-C3, representing >50% improvement from baseline compared with placebo (–4.5 ng/mL), while the 4 mg/kg dose showed a –1.7 ng/mL change. These biomarker findings
were consistent with the clinical outcome of reduction in development of new varices, further supporting the antifibrotic and disease-modifying potential of belapectin in patients with compensated MASH cirrhosis and portal hypertension.
Baseline YKL-40 levels were comparable across treatment groups (placebo: 5.11 ng/mL; 2 mg/kg: 4.95 ng/mL; 4 mg/kg: 4.92 ng/mL). At 18 months, a greater proportion of patients receiving belapectin
2 mg/kg achieved a ≥ 20% reduction in YKL-40 compared with placebo (33.8% vs 23.1%), while fewer belapectin-treated patients experienced increases from baseline. These findings provide additional mechanistic evidence of galectin-3 pathway
modulation and support belapectin’s antifibrotic biological activity in patients with MASH cirrhosis and portal hypertension.
Analysis of PRO-C4, a key biomarker associated with liver injury and fibrogenesis, showed that a ≥ 20% increase from baseline occurred at a higher rate in placebo-treated subjects compared with
those receiving belapectin 2 mg/kg (13% vs 3%). This pattern, consistent across both the full analysis and per-protocol populations, indicates ongoing fibrotic progression in the placebo arm and further reinforces belapectin’s potential to modify
disease progression in compensated MASH cirrhosis with portal hypertension.
Separately, a poster presentation at AASLD over the weekend showed that reduction in the development of esophageal varices observed at 18 months was sustained through 36 months in patients with
MASH cirrhosis and portal hypertension. A total of 57 subjects completed 36 months of therapy in NAVIAGTE. At 36 months, the cumulative incidence of new varices in the study was 23.4%, 12.4% and 16.7% respectively, in placebo, 2 mg/kg, and 4 mg/kg
cohorts.
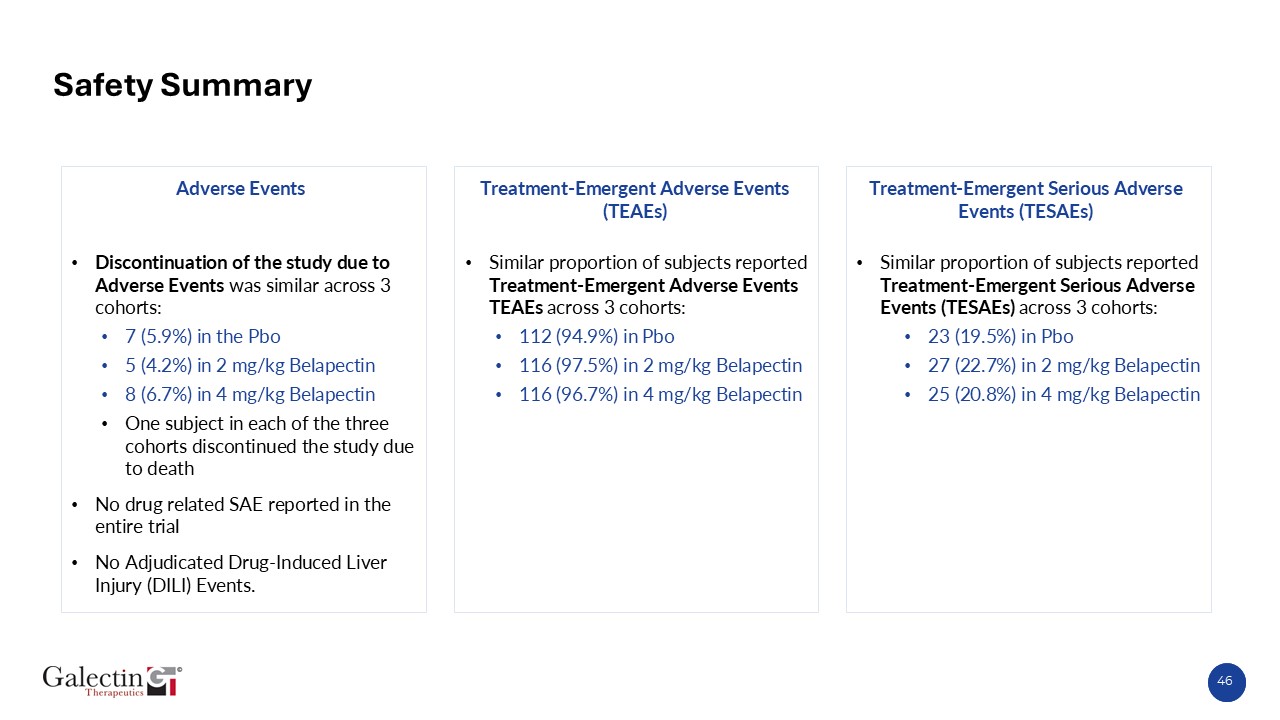
As in prior trials, the safety profile of belapectin remains highly encouraging with incidence of adverse events and serious adverse events comparable across the three cohorts. Rates of
discontinuation, adverse events (AEs), and serious adverse events (SAEs) were comparable to placebo, with no drug-related SAEs reported in the NAVIGATE trial.
Raj Vuppalanchi, M.D., serves as Professor of Medicine and Director of Hepatology at Indiana University School of Medicine, stated “The long-term NAVIGATE data presented at AASLD provide
important insights into the potential of Galectin-3 inhibition in advanced fibrosis. The sustained improvements in liver stiffness and multiple serum biomarkers, including ELF, PRO-C3, and YKL-40, are particularly noteworthy, as they collectively
suggest a consistent antifibrotic effect and stabilization of disease. These results are encouraging for patients with MASH cirrhosis and portal hypertension, a population with few effective therapeutic options.”
Dr. Khurram Jamil, Chief Medical Officer at Galectin Therapeutics, stated, “The consistency we observed across both clinical and biomarker endpoints reinforces belapectin’s potential as a
disease-modifying therapy for patients with compensated MASH cirrhosis and portal hypertension. The 2 mg/kg dose demonstrated a clear and clinically meaningful reduction in the incidence of new varices across all ELF risk categories, with the
strongest effect seen in patients at highest risk for liver complications. In addition, the more than 50% greater reduction in Pro-C3 levels versus placebo further supports belapectin’s antifibrotic activity and alignment between biomarker and
clinical outcomes.”
Joel Lewis, Chief Executive Officer at Galectin Therapeutics, added, “We are very encouraged to see the robust effects of belapectin maintained over 36 months of therapy. These results represent
an important milestone for the belapectin program and for patients living with MASH cirrhosis, a population with no approved therapeutic options today. With a solid foundation of clinical and biomarker evidence, we are focused on advancing
regulatory discussions and exploring strategic partnerships to accelerate the next phase of development. We are deeply encouraged by the potential of belapectin to make a meaningful difference for patients and families affected by this serious
disease.”
About Galectin Therapeutics
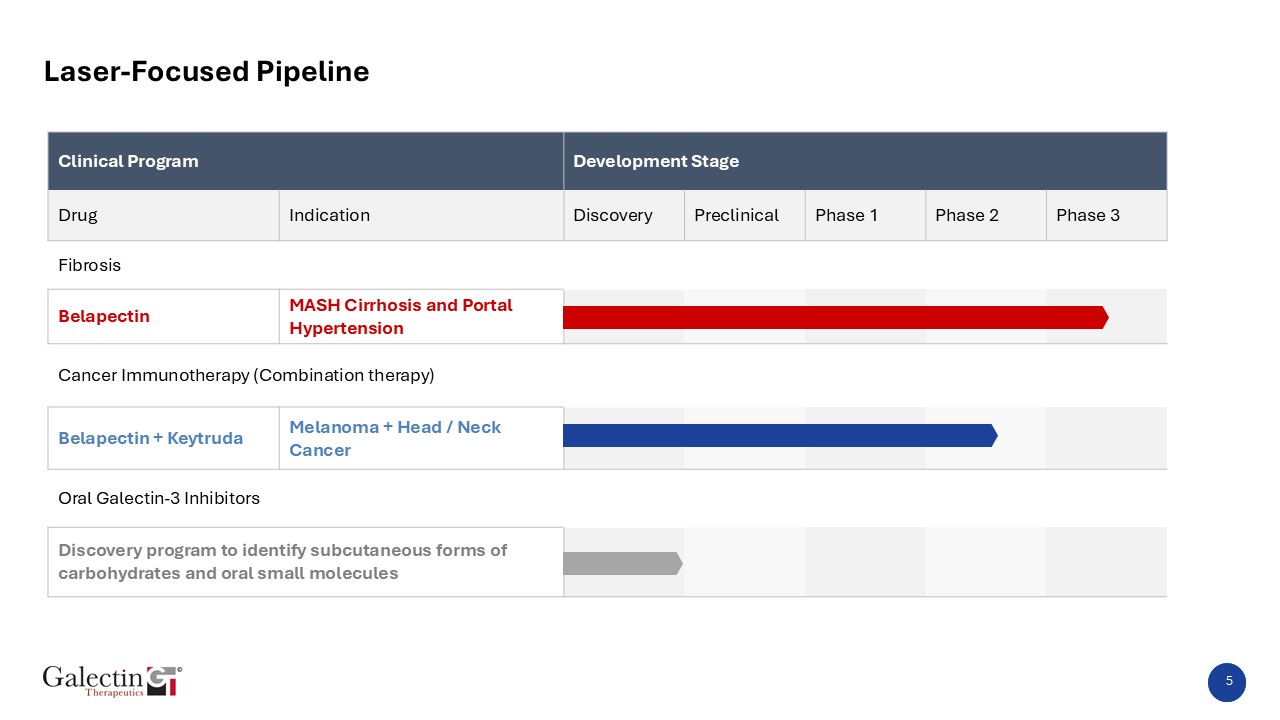
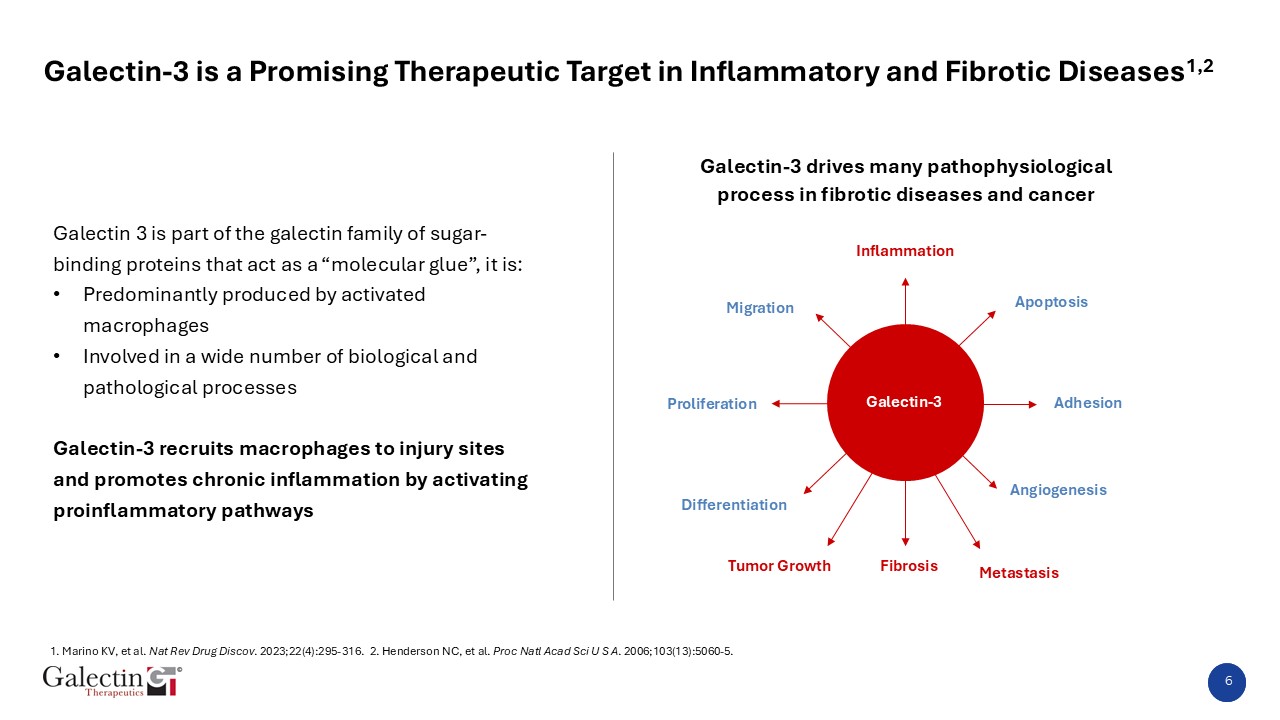
Galectin Therapeutics is dedicated to developing novel therapies to improve the lives of patients with chronic liver disease and cancer. Galectin’s lead drug belapectin is a carbohydrate-based drug that inhibits the
galectin-3 protein, which is directly involved in multiple inflammatory, fibrotic, and malignant diseases, for which it has Fast Track designation by the U.S. Food and Drug Administration. The lead development program is in metabolic
dysfunction-associated steatohepatitis (MASH, formerly known as nonalcoholic steatohepatitis, or NASH) with cirrhosis, the most advanced form of MASH-related fibrosis. Liver cirrhosis is one of the most pressing medical need and a significant drug
development opportunity. Additional development programs are in treatment of combination immunotherapy for advanced head and neck cancers and other malignancies. Advancement of these additional clinical programs is largely dependent on finding a
suitable partner. Galectin seeks to leverage extensive scientific and development expertise as well as established relationships with external sources to achieve cost-effective and efficient development. Additional information is available at www.galectintherapeutics.com.
Forward Looking Statements
This press release contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. These statements relate to future events or future financial performance, and use words
such as “may,” “estimate,” “could,” “expect”, “look forward”, “believe”, “hope” and others. They are based on management’s current expectations and are subject to factors and uncertainties that could cause actual results to differ materially from
those described in the statements. These statements include those regarding the hope that Galectin’s development program for belapectin will lead to the first therapy for the treatment of MASH, formerly known as NASH, with cirrhosis and those
regarding the hope that our lead compounds will be successful in cancer immunotherapy and in other therapeutic indications. Factors that could cause actual performance to differ materially from those discussed in the forward-looking statements
include, among others, full analysis of the NAVIGATE trial data may not produce positive data; Galectin may not be successful in developing effective treatments and/or obtaining the requisite approvals for the use of belapectin or any of its other
drugs in development; the Company may not be successful in scaling up manufacturing and meeting requirements related to chemistry, manufacturing and control matters; the Company’s current clinical trial and any future clinical studies may not produce
positive results in a timely fashion, if at all, and could require larger and longer trials, which would be time consuming and costly; plans regarding development, approval and marketing of any of Galectin’s drugs are subject to change at any time
based on the changing needs of the Company as determined by management and regulatory agencies; regardless of the results of any of its development programs, Galectin may be unsuccessful in developing partnerships with other companies or raising
additional capital that would allow it to further develop and/or fund any studies or trials. Galectin has incurred operating losses since inception, and its ability to successfully develop and market drugs may be impacted by its ability to manage
costs and finance continuing operations. For a discussion of additional factors impacting Galectin’s business, see the Company’s Annual Report on Form 10-K for the year ended December 31, 2024, and subsequent filings with the SEC. You should not
place undue reliance on forward-looking statements. Although subsequent events may cause its views to change, management disclaims any obligation to update forward-looking statements.
Jack Callicutt, Chief Financial Officer
(678) 620-3186
ir@galectintherapeutics.com
Investors Relations Contacts:
Kevin Gardner
kgardner@lifesciadvisors.com
Galectin Therapeutics and its associated logo is a registered trademark of Galectin Therapeutics Inc. Belapectin is the USAN assigned name for Galectin Therapeutics’ galectin-3 inhibitor belapectin.