Roivant Announces Positive Results for Batoclimab Myasthenia Gravis (MG) and Chronic Inflammatory
Demyelinating Polyneuropathy (CIDP) Studies
|
• |
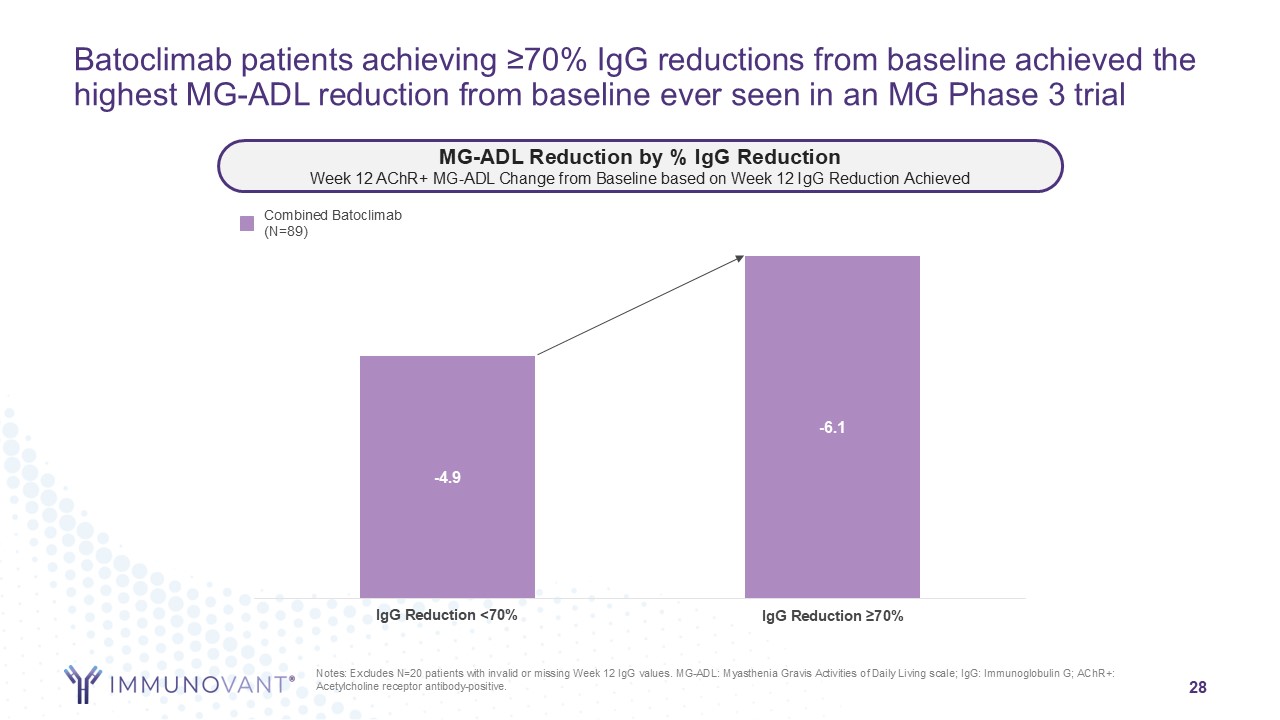
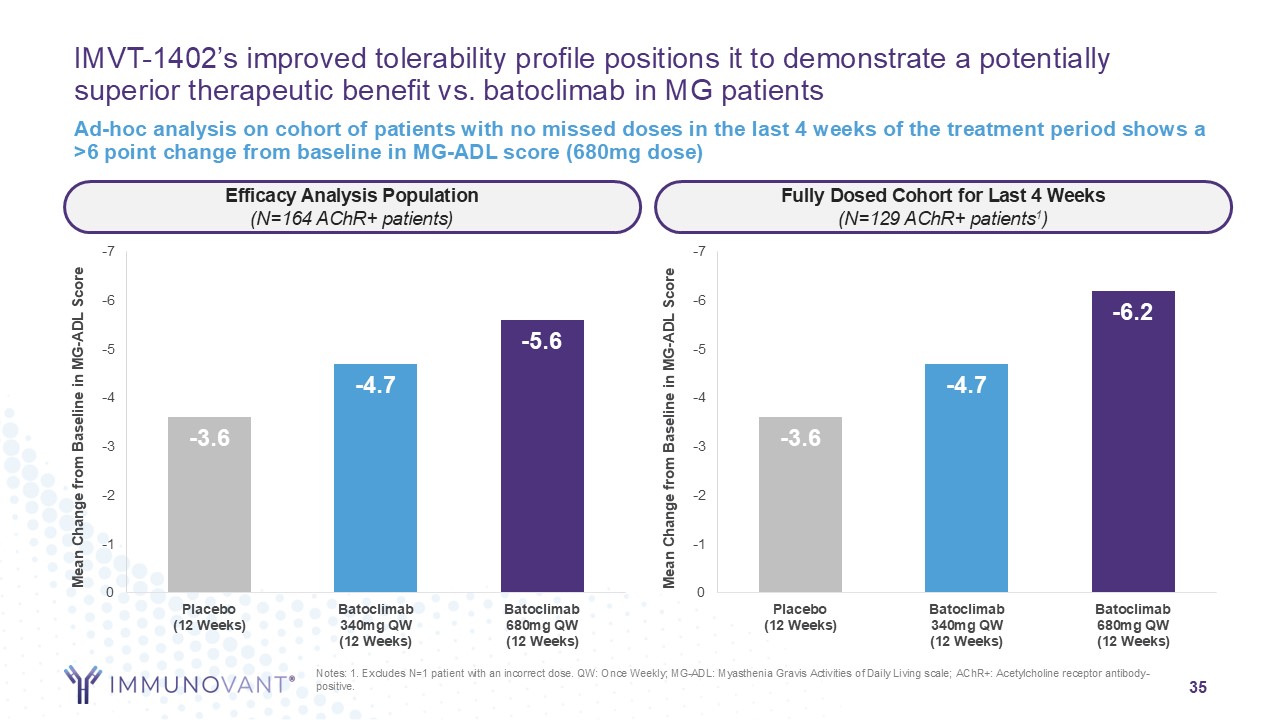
Pivotal study in MG met primary endpoint of change from baseline in MG-ADL in AChR+ population at 12 weeks, with a 5.6 point improvement in the higher dose arm (with 74% mean IgG reduction) and a
4.7 point improvement in the lower dose arm (with 64% mean IgG reduction)
|
|
• |
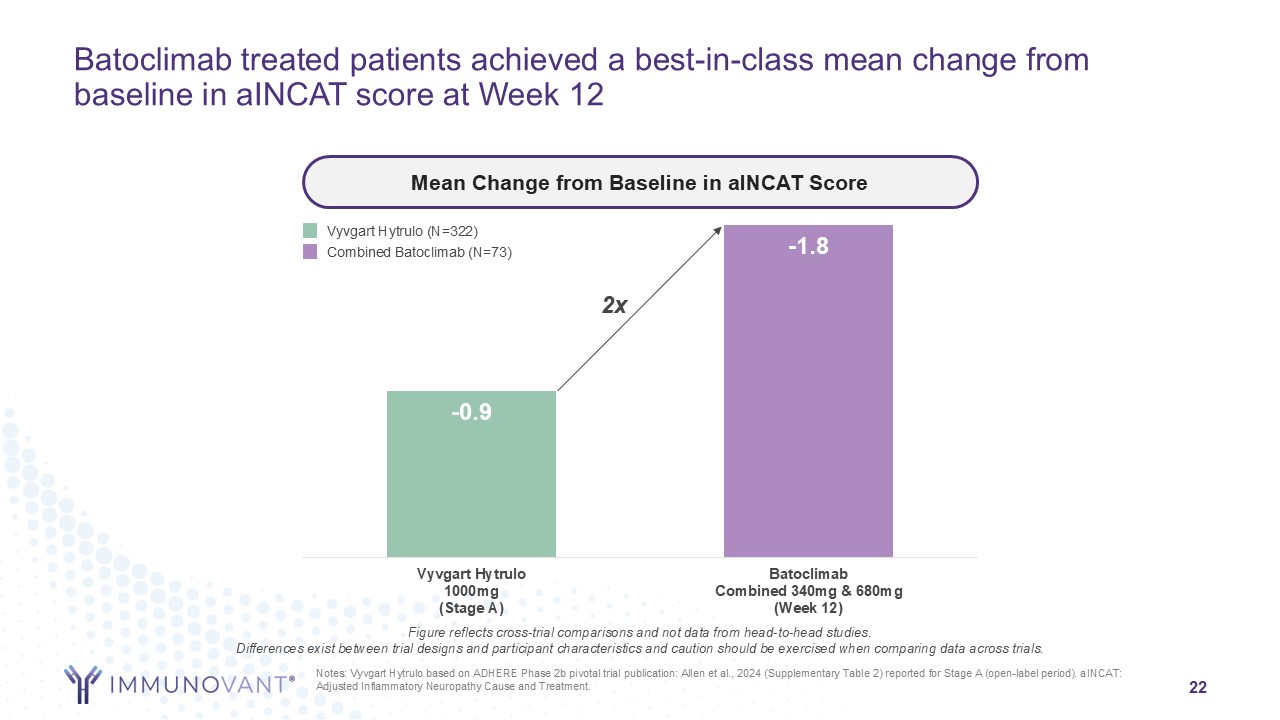
Initial CIDP results from Period 1, following standard of care washout, demonstrate a mean improvement in the adjusted INCAT disability score of 1.8 across batoclimab arms and an 84% responder rate
in those patients who achieved an IgG lowering greater than 70%
|
|
• |
In both batoclimab studies, deeper IgG reductions correlated with better clinical outcomes across a range of assessments and timepoints
|
|
• |
INDs active for both MG and CIDP with pivotal study initiations for lead asset IMVT-1402 in these indications expected imminently
|
|
• |
Immunovant and Roivant to host combined investor call to discuss these updates today, March 19, 2025 at 8 a.m. EDT
|
NEW YORK, March 19, 2025 (GLOBE NEWSWIRE) -- Immunovant, Inc. (Nasdaq: IMVT), a clinical-stage immunology company dedicated to enabling normal lives for people with
autoimmune diseases, today reported topline results from its Phase 3 study of batoclimab in MG and initial results from Period 1 of its Phase 2b study in CIDP.
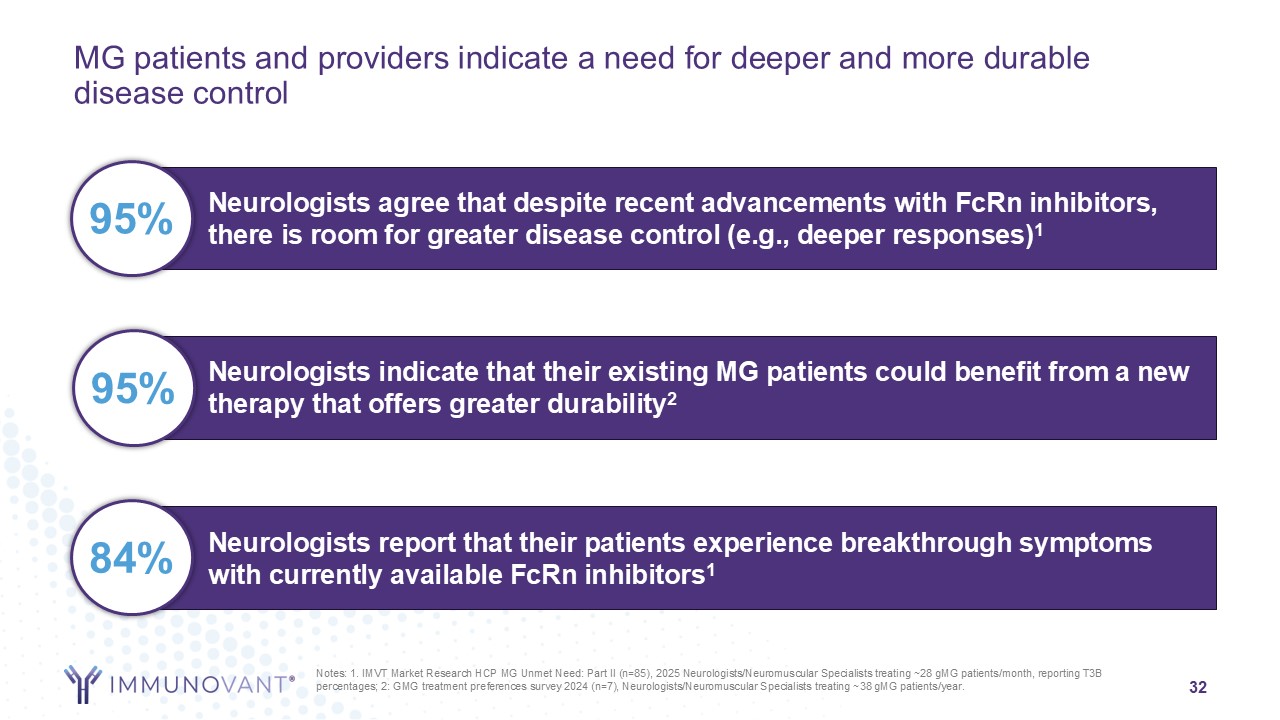
“We are excited to share positive results from our MG and CIDP studies. While neurologists and patients are very enthusiastic about currently
approved FcRn inhibitors, they tell us that they also see a lot of potential for a next-generation FcRn inhibitor that can offer deeper and more durable responses for patients whose disease is still affecting their daily function. Today’s results
show that deeper IgG reduction leads to deeper responses in MG and CIDP. Beyond the results in MG and CIDP, we believe that our core thesis - that deeper IgG reduction, at the levels achieved by high dose batoclimab and high dose IMVT-1402, leads
to improved clinical outcomes - will apply to a wide range of auto-antibody mediated conditions,” said Pete Salzmann, M.D., chief executive officer of Immunovant.
About the Phase 3 Study in MG
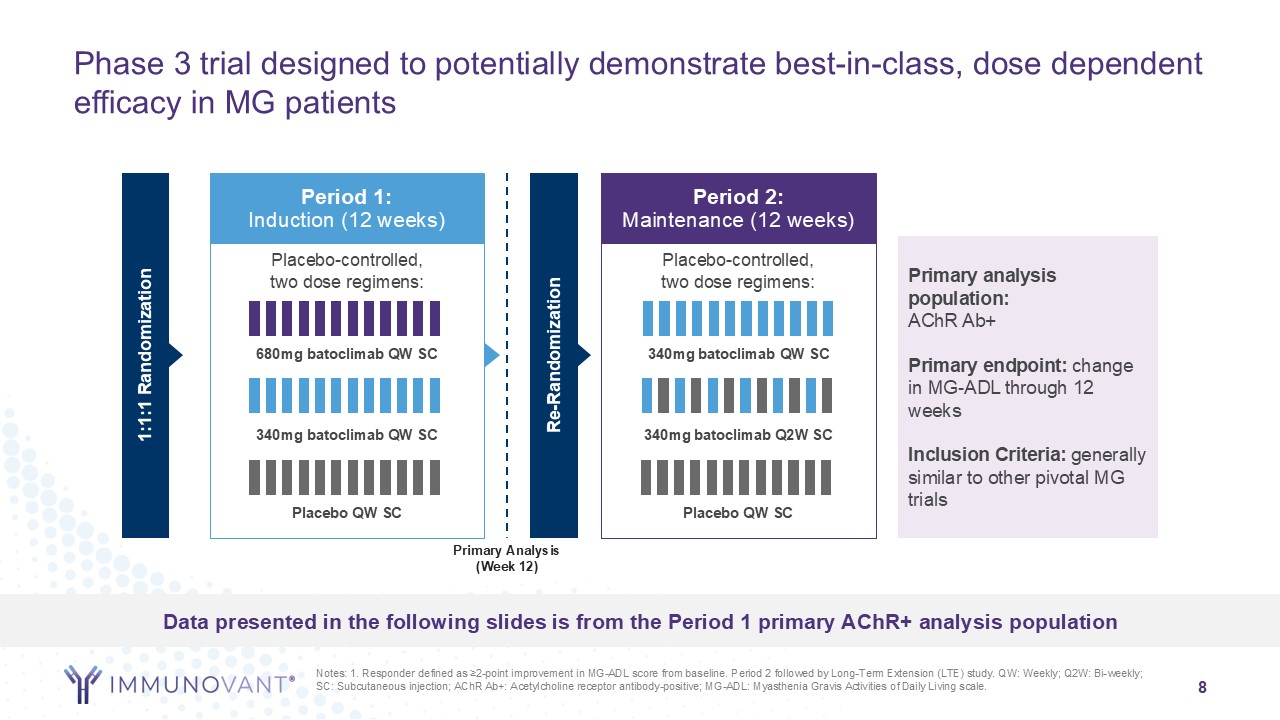
The Phase 3 study in MG is a randomized, quadruple-blind, placebo-controlled study designed to assess the efficacy and safety of batoclimab in
adults with MG. Following screening, participants with moderate to severe MG were randomized into Period 1 where they received high dose batoclimab (680mg weekly) or lower dose batoclimab (340mg weekly) or placebo for 12 weeks. Responders to
batoclimab in Period 1, defined as ≥2-point improvement in Myasthenia Gravis Activities of Daily Living (MG-ADL) score from baseline, were re-randomized 1:1:1 to batoclimab (340mg weekly or 340mg every other week) or placebo for 12 weeks (Period
2). The primary endpoint of the study was mean change from baseline in MG-ADL in acetylcholine receptor antibody positive (AChR+) participants at Week 12 (end of Period 1).
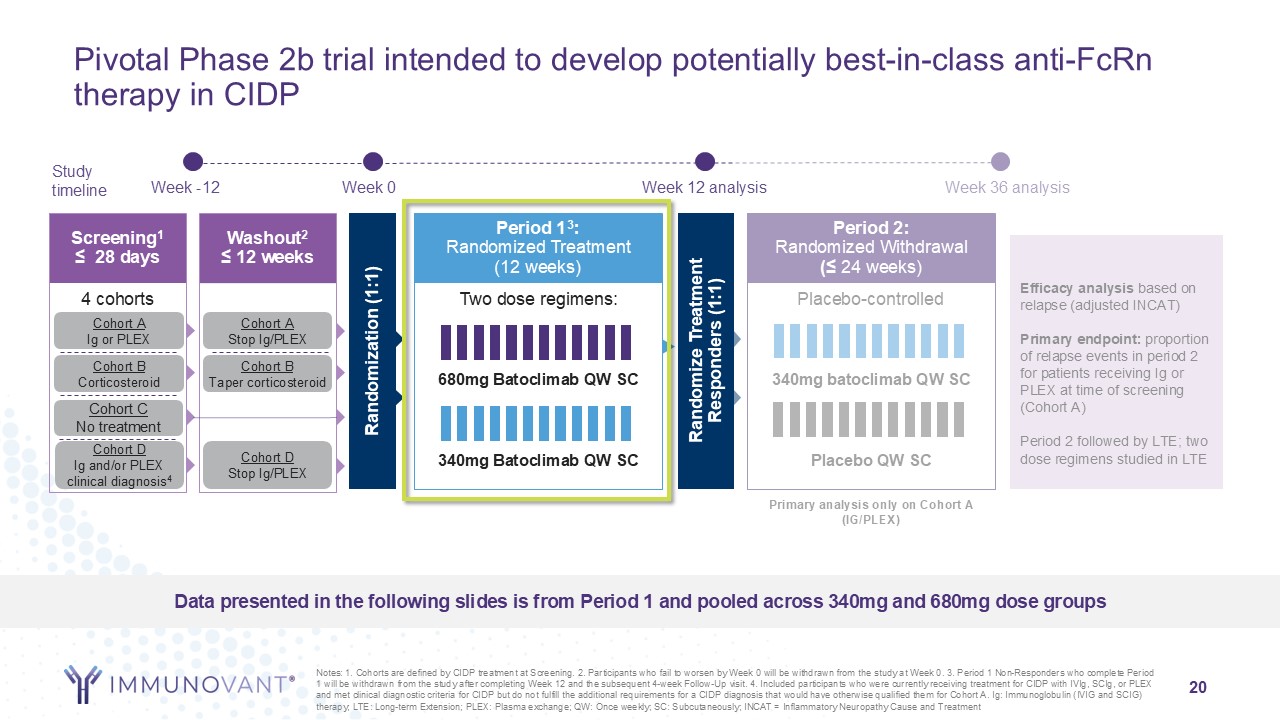
About the Phase 2b Study in CIDP
The Phase 2b study in CIDP is a randomized, quadruple-blind, placebo-controlled study designed to assess the efficacy and safety of batoclimab in adult participants with
active CIDP.
Similar to other recent studies, this Phase 2b study in CIDP begins with a non-placebo controlled run-in (Period 1), during which participants
whose disease had worsened during standard of care washout then receive either 340 mg or 680 mg batoclimab weekly by subcutaneous injection. Participants who respond to batoclimab therapy in Period 1 (responders are defined as those achieving a ≥1
point improvement from Period 1 baseline in adjusted Inflammatory Neuropathy Cause and Treatment (aINCAT) disability score), are then randomized 1:1 to receive either 340 mg batoclimab or placebo weekly in a 24-week withdrawal period (Period 2).
The primary endpoint will assess the percentage of participants who remain relapse-free at Week 36, at the end of Period 2. The study is ongoing and has not yet been unblinded. Therefore, pooled data are currently available from Period 1 and no
data are available for the primary endpoint at the end of Period 2.
Phase 3 MG Study Results Highlights
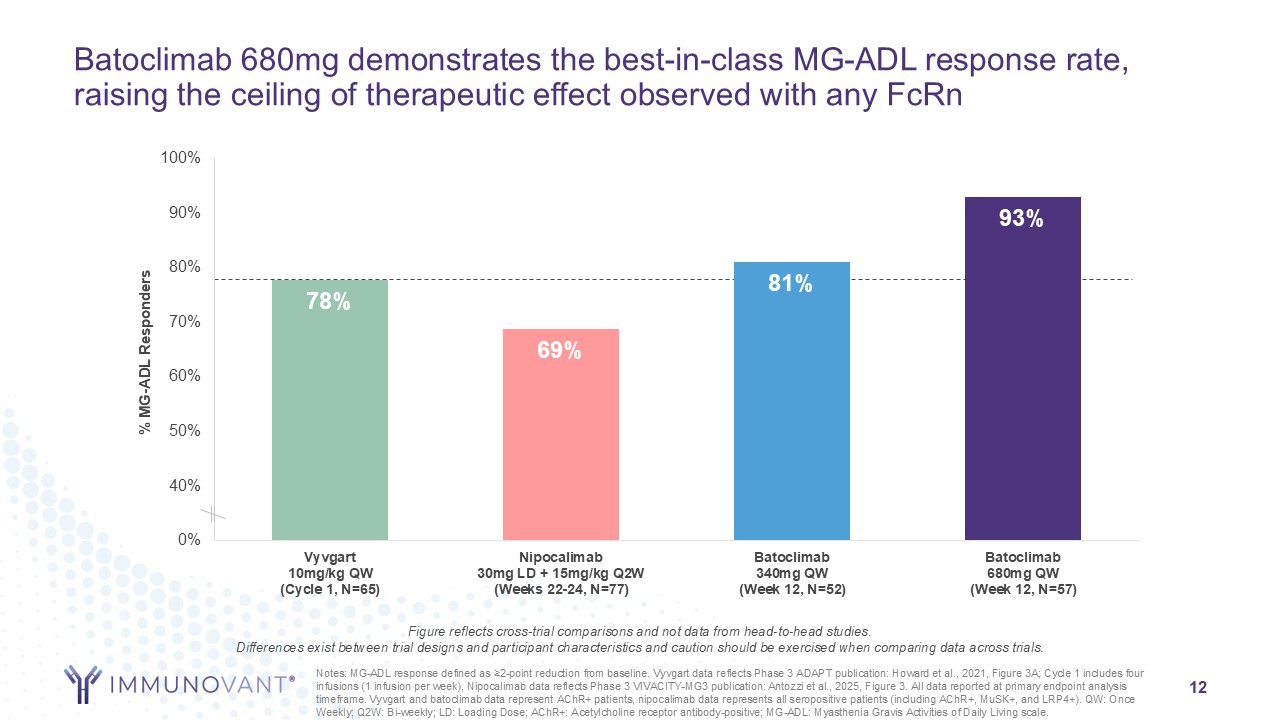
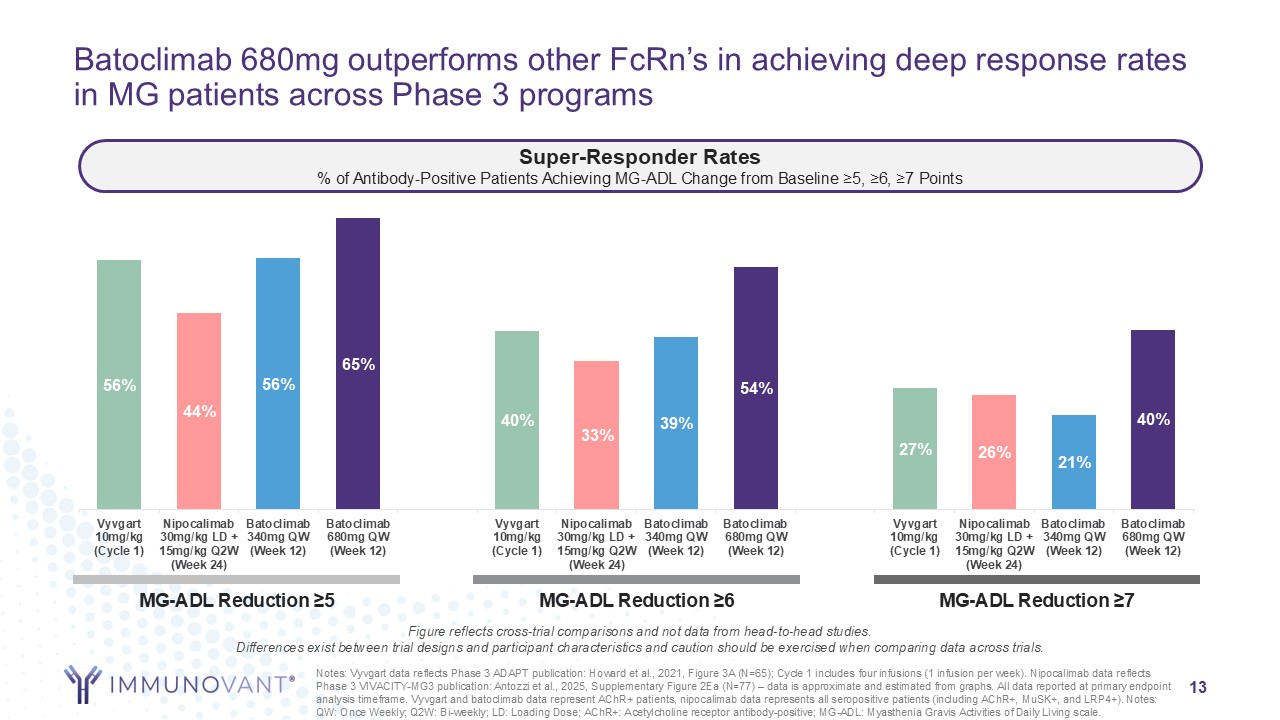
In the Phase 3 MG study, batoclimab met its primary endpoint of mean change from baseline in MG-ADL in AChR+ participants. Participants entering the study and randomized
to 680mg of batoclimab given weekly by subcutaneous injection achieved a 5.6 point improvement in MG-ADL at Week 12, while those randomized to 340mg of batoclimab given weekly by subcutaneous injection achieved a 4.7 point improvement in MG-ADL at
Week 12 and those randomized to placebo experienced a 3.6 point improvement in MG-ADL at Week 12. Large differences between the dosing arms were observed, especially for deeper response thresholds. Results in Period 2 (Weeks 12-24) were as
expected, with patients re-randomized to 340mg weekly outperforming those whose dose was reduced. Additional efficacy results are summarized in the table below:
| |
Snapshot of Efficacy Measures Observed
|
Placebo
|
Batoclimab
340mg
|
Batoclimab
680mg
|
| |
(% AChR+ Population)
|
|
(QW)^
|
(QW)^^
|
| |
|
|
|
|
| |
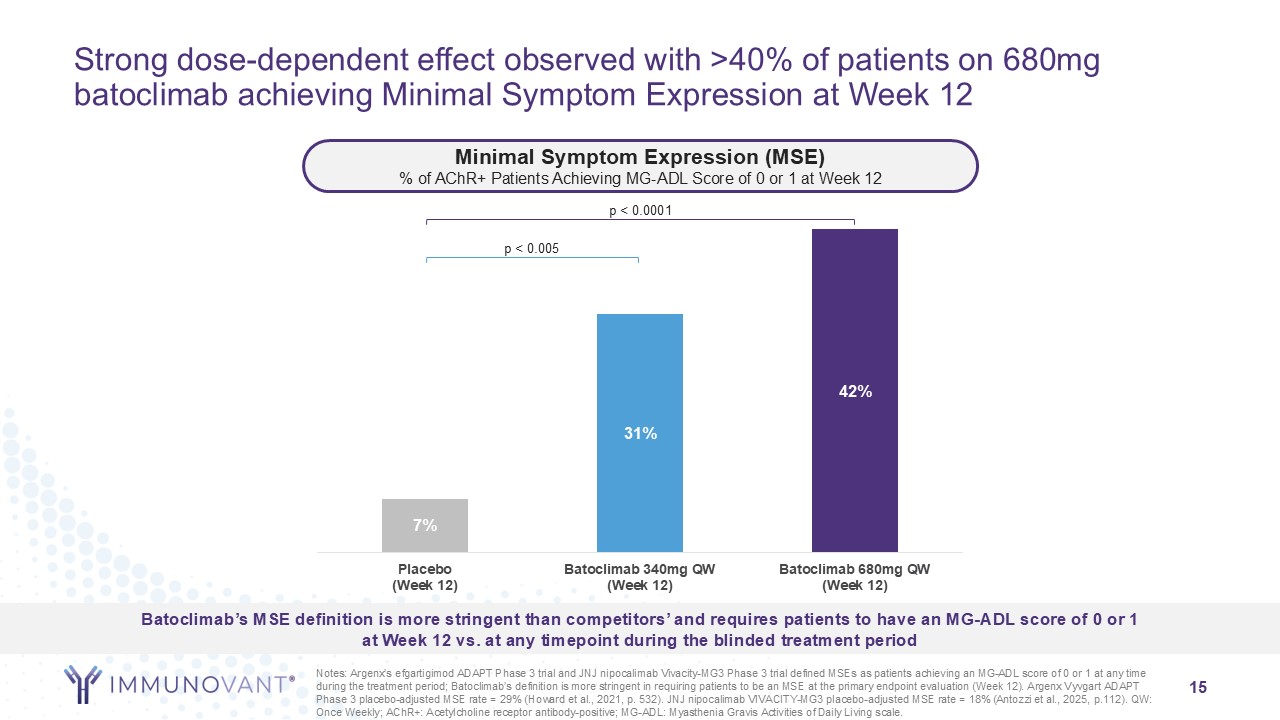
Minimal Symptom Expression (MSE*) at Wk 12
|
7%
|
31%
|
42%
|
| |
Durable MSE**
|
0%
|
39%
|
75%
|
| |
Early Super Responders (≥5 point reduction in MG-ADL score by Wk 2)
|
11%
|
25%
|
40%
|
| |
Early Super Responders (≥6 point reduction in MG-ADL score by Wk 2)
|
6%
|
17%
|
30%
|
| |
Early Super Responders (≥7 point reduction in MG-ADL score by Wk 2)
|
2%
|
10%
|
19%
|
| |
|
|
|
|
^ all p<0.05 except early super responders ≥7 where p=0.07;
^^ all p<=0.001
* MSE defined as patients that achieved an MG-ADL score of 0 or 1 at Week 12
** Durable MSE defined as patients maintaining MSE for >6 weeks, amongst those that achieved MSE
prior to or by Week 6
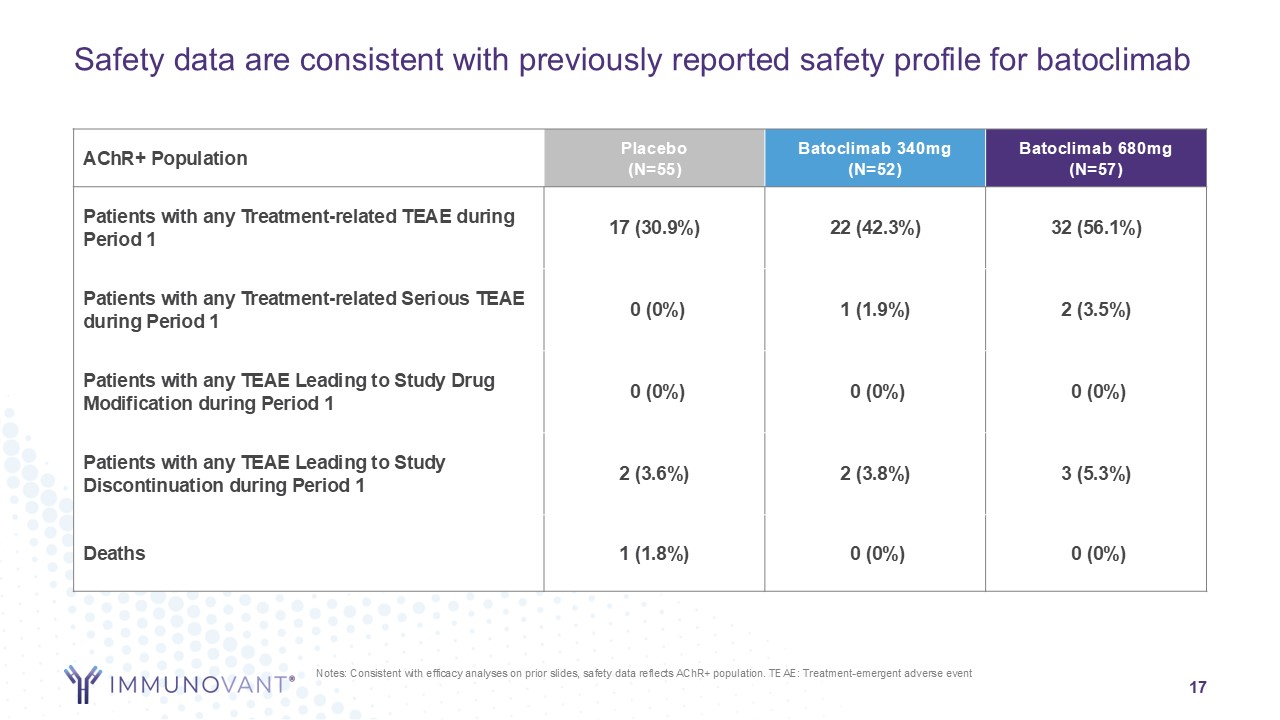
Safety and tolerability were observed to be consistent with prior batoclimab studies.
Phase 2b CIDP Study Results Highlights
Initial batoclimab data in 73 patients pooled across all cohorts for the run-in Period 1 of the Phase 2b CIDP study demonstrated a 1.8 point improvement in aINCAT
(compared to Period 1 baseline) at Week 12. An 84% responder rate (with response defined as an aINCAT improvement ≥ 1) was observed among all patients whose IgG was reduced by ≥ 70%. Other CIDP scales also demonstrated meaningful improvements for
pooled batoclimab cohorts, with an improvement in I-RODS of 15.3, an improvement in MRC-SS of 5.6, and an improvement in grip strength of 15.1 all at Week 12.
Safety and tolerability were observed to be consistent with prior batoclimab studies.
Path Forward in MG and CIDP
Immunovant plans to initiate potentially registrational studies in both MG and CIDP with lead asset IMVT-1402 and has received clearance for its
Investigational New Drug (IND) applications for both indications as previously disclosed. Despite meaningful improvement for patients with MG and CIDP to date with the anti-FcRn class, there continues to be significant unmet need. IMVT-1402 is a
potentially best-in-class anti-FcRn that may deliver deeper and more durable clinical responses for patients with MG, CIDP, and many other challenging autoimmune conditions.
At present, Immunovant does not intend to seek regulatory approval for batoclimab in MG or CIDP and is focused on leveraging data and learnings from
the batoclimab studies to inform and accelerate its programs with IMVT-1402. Immunovant will wait to make a final decision about regulatory submissions for batoclimab until the results of the ongoing Phase 3 studies of batoclimab in thyroid eye
disease are available.
Webcast Details
The company will host an investor call and webcast with Immunovant CEO Dr. Pete Salzmann, M.D., MBA and Roivant CEO Matt Gline at 8:00 a.m. EDT
today, March 19, 2025 to discuss these updates. Please click here to register for the event. The live webcast will also be available under “Events & Presentations” in the
Investors section of the Roivant website at https://investor.roivant.com/news-events/events. The archived webcast will be available on Roivant’s website after the conference call.
About Immunovant, Inc.
Immunovant, Inc. is a clinical-stage immunology company dedicated to enabling normal lives for people with autoimmune diseases. As a trailblazer in
anti-FcRn technology, the Company is developing innovative, targeted therapies to meet the complex and variable needs of people with autoimmune diseases. For additional information on the Company, please visit immunovant.com.
Cautionary Note Regarding Forward-Looking Statements
This press release contains forward-looking statements for the purposes of the safe harbor provisions under The Private Securities Litigation Reform Act of 1995 and other
federal securities laws. The use of words such as "can," “may,” “might,” “will,” “would,” “should,” “expect,” “believe,” “estimate,” “design,” “plan,” "intend," and other similar expressions are intended to identify forward-looking statements. Such
forward looking statements include Immunovant’s expectations relating to the results of its batoclimab clinical trials; Immunovant's plan to develop IMVT-1402 in MG and CIDP; and the potential benefits of IMVT-1402 and its potential best-in-class
profile. All forward-looking statements are based on estimates and assumptions by Immunovant’s management that, although Immunovant believes to be reasonable, are inherently uncertain. All forward-looking statements are subject to risks and
uncertainties that may cause actual results to differ materially from those that Immunovant expected. Such risks and uncertainties include, among others: initial results or other preliminary analyses or results of early clinical trials may not be
predictive final trial results or of the results of later clinical trials; the timing and availability of data from clinical trials; the timing of discussions with regulatory agencies, as well as regulatory submissions and potential approvals; the
continued development of Immunovant’s product candidates, including the timing of the commencement of additional clinical trials; Immunovant’s scientific approach, clinical trial design, indication selection, and general development progress;
future clinical trials may not confirm any safety, potency, or other product characteristics described or assumed in this press release; any product candidate that Immunovant develops may not progress through clinical development or receive
required regulatory approvals within expected timelines or at all; Immunovant’s product candidates may not be beneficial to patients, or even if approved by regulatory authorities, successfully commercialized; the potential impact of global
factors, geopolitical tensions, and adverse macroeconomic conditions on Immunovant’s business operations and supply chain, including its clinical development plans and timelines; Immunovant’s business is heavily dependent on the successful
development, regulatory approval and commercialization of IMVT-1402 and batoclimab; Immunovant is at an early stage of development for IMVT-1402 and in various stages of clinical development for batoclimab; and Immunovant will require additional
capital to fund its operations and advance batoclimab and IMVT-1402 through clinical development. These and other risks and uncertainties are more fully described in Immunovant’s periodic and other reports filed with the Securities and Exchange
Commission (SEC), including in the section titled “Risk Factors” in Immunovant’s Form 10-Q filed with the SEC on February 6, 2025, and Immunovant’s subsequent filings with the SEC. Any forward-looking statement speaks only as of the date on which
it was made. Immunovant undertakes no obligation to publicly update or revise any forward-looking statement, whether as a result of new information, future events, or otherwise.
About Roivant
Roivant (Nasdaq: ROIV) is a biopharmaceutical company that aims to improve the lives of patients by accelerating the development and
commercialization of medicines that matter. Roivant’s pipeline includes IMVT-1402 and batoclimab, fully human monoclonal antibodies targeting FcRn in development across several IgG-mediated autoimmune indications; brepocitinib, a potent small
molecule inhibitor of TYK2 and JAK1 in development for the treatment of dermatomyositis, non-infectious uveitis and cutaneous sarcoidosis; and mosliciguat, an inhaled sGC activator in development for pulmonary hypertension associated with
interstitial lung disease. We advance our pipeline by creating nimble subsidiaries or “Vants” to develop and commercialize our medicines and technologies. Beyond therapeutics, Roivant also incubates discovery-stage companies and health technology
startups complementary to its biopharmaceutical business. For more information, www.roivant.com.
Roivant-Forward Looking Statements
This press release contains forward-looking statements. Statements in this press release may include statements that are not historical facts and are considered
forward-looking within the meaning of Section 27A of the Securities Act of 1933, as amended (the “Securities Act”), and Section 21E of the Securities Exchange Act of 1934, as amended (the “Exchange Act”), which are usually identified by the use of
words such as “anticipate,” “believe,” “continue,” “could,” “estimate,” “expect,” “intends,” “may,” “might,” “plan,” “possible,” “potential,” “predict,” “project,” “should,” “would” and variations of such words or similar expressions. The words may
identify forward-looking statements, but the absence of these words does not mean that a statement is not forward-looking. We intend these forward-looking statements to be covered by the safe harbor provisions for forward-looking statements
contained in Section 27A of the Securities Act and Section 21E of the Exchange Act.
Our forward-looking statements include, but are not limited to, statements regarding our or our management team’s expectations, hopes, beliefs, intentions or strategies
regarding the future, and statements that are not historical facts, including statements about the clinical and therapeutic potential of our product candidates, the availability and success of topline results from our ongoing clinical trials and
any commercial potential of our product candidates following applicable regulatory approvals. In addition, any statements that refer to projections, forecasts or other characterizations of future events, results or circumstances, including any
underlying assumptions, are forward-looking statements. Actual results may differ materially from those contemplated in these statements due to a variety of risks, uncertainties and other factors.
Although we believe that our plans, intentions, expectations and strategies as reflected in or suggested by those forward-looking statements are reasonable, we can give
no assurance that the plans, intentions, expectations or strategies will be attained or achieved. Furthermore, actual results may differ materially from those described in the forward-looking statements and will be affected by a number of risks,
uncertainties and assumptions, including, but not limited to, those risks set forth in the Risk Factors section of our filings with the U.S. Securities and Exchange Commission. Moreover, we operate in a very competitive and rapidly changing
environment in which new risks emerge from time to time. These forward-looking statements are based upon the current expectations and beliefs of our management as of the date of this press release, and are subject to certain risks and uncertainties
that could cause actual results to differ materially from those described in the forward-looking statements. Except as required by applicable law, we assume no obligation to update publicly any forward-looking statements, whether as a result of new
information, future events or otherwise.
Roivant Contacts:
Investors:
Keyur Parekh
keyur.parekh@roivant.com
Media:
Stephanie Lee
stephanie.lee@roivant.com