|
Delaware
|
001-39990
|
11-3430072
|
|
(State or other jurisdiction of incorporation or organization)
|
(Commission File Number)
|
(IRS Employer Identification No.)
|
| ☐ |
Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425)
|
| ☐ |
Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12)
|
| ☐ |
Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b))
|
| ☐ |
Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c))
|
|
(Title of each class)
|
(Trading Symbol)
|
(Name of exchange on which registered)
|
| Common Stock, $0.01 par value per share |
ELTX
|
The Nasdaq Global Select Market |
| Item 8.01 |
Other Events.
|
| Item 9.01. |
Financial Statements and Exhibits.
|
| (d) |
Exhibits.
|
|
Exhibit
Number
|
Exhibit
Description
|
|
|
Press Release of Elicio Therapeutics, Inc., dated January 9, 2024
|
||
|
Corporate presentation dated January 9, 2024
|
||
|
104
|
Cover Page Interactive Data File (embedded within the Inline XBRL document)
|
|
|
Elicio Therapeutics, Inc.
|
|
|
|
|
|
|
|
By:
|
/s/ ROBERT CONNELLY
|
|
|
|
Robert Connelly
President and Chief Executive Officer
(Principal Executive Officer)
|
|
Date: January 9, 2024
|
||

|
|
● |
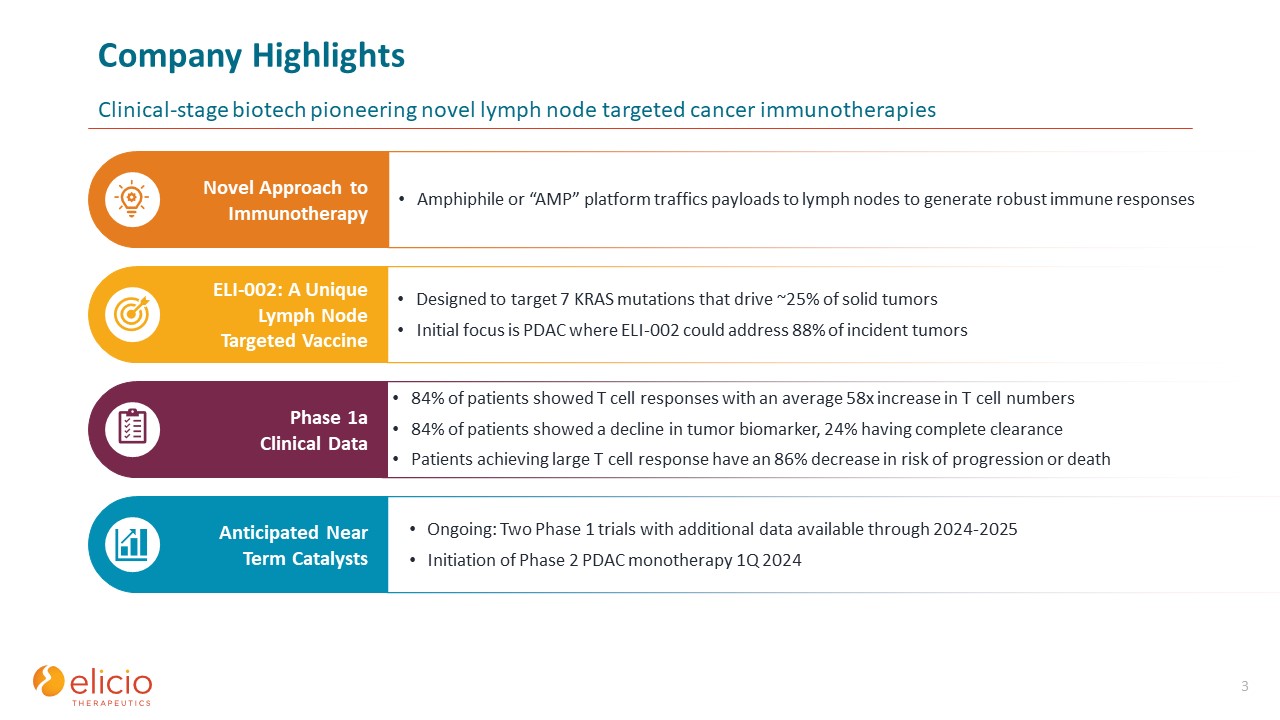
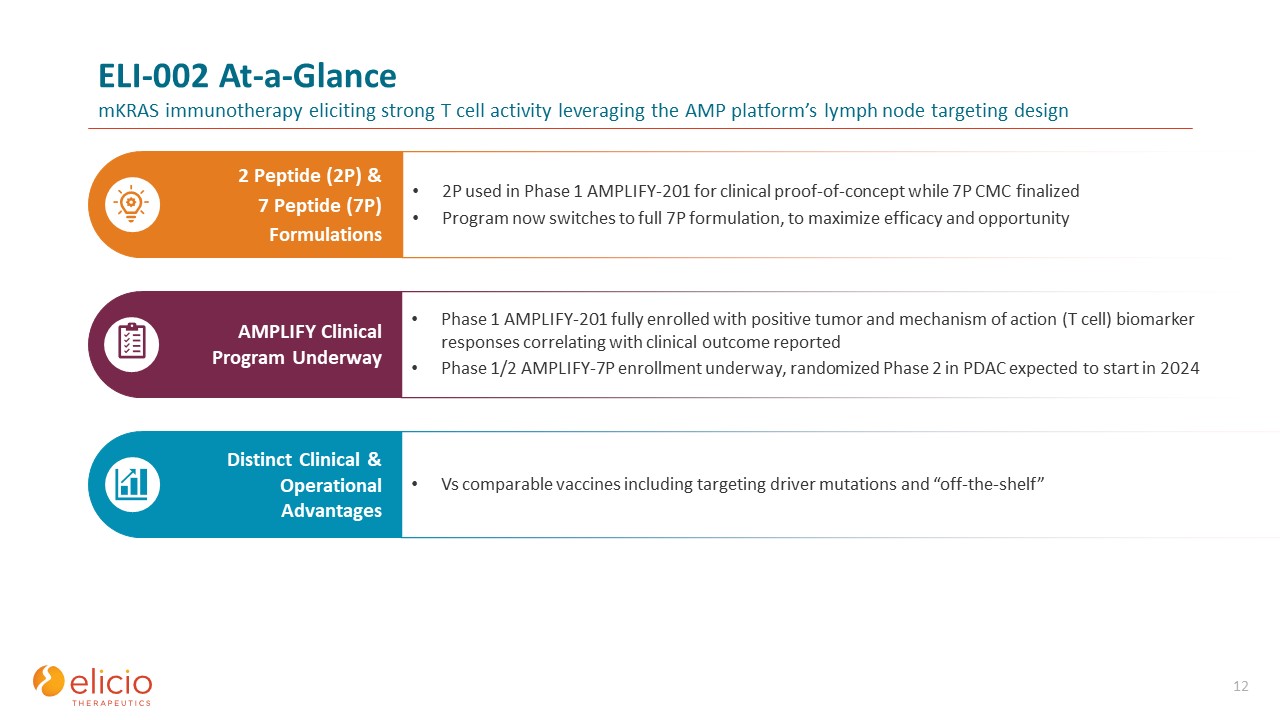
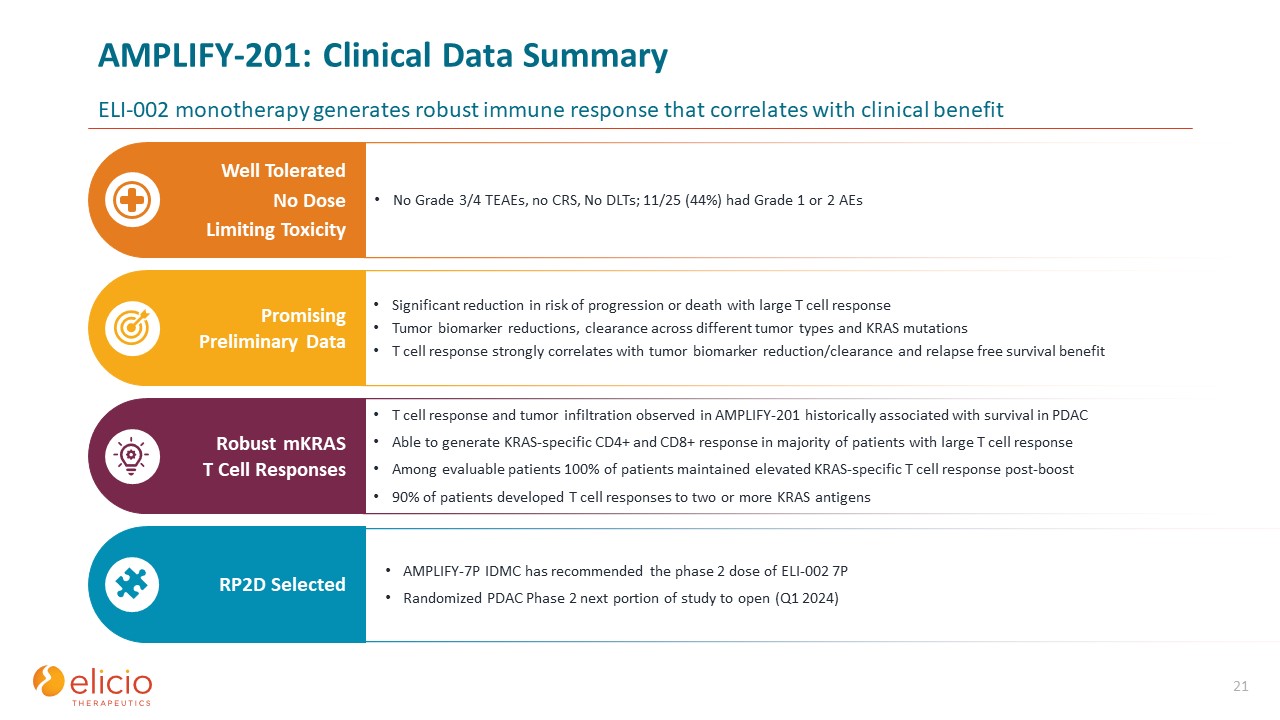
Data showed ELI-002 administered as a monotherapy induced robust, polyfunctional
and durable KRAS specific CD4+ and CD8+ T cell responses
|
|
|
● |
Tumor biomarker reduction was observed in 84% of patients correlating with a median relapse-free survival of 16.3 months
|
|
|
● |
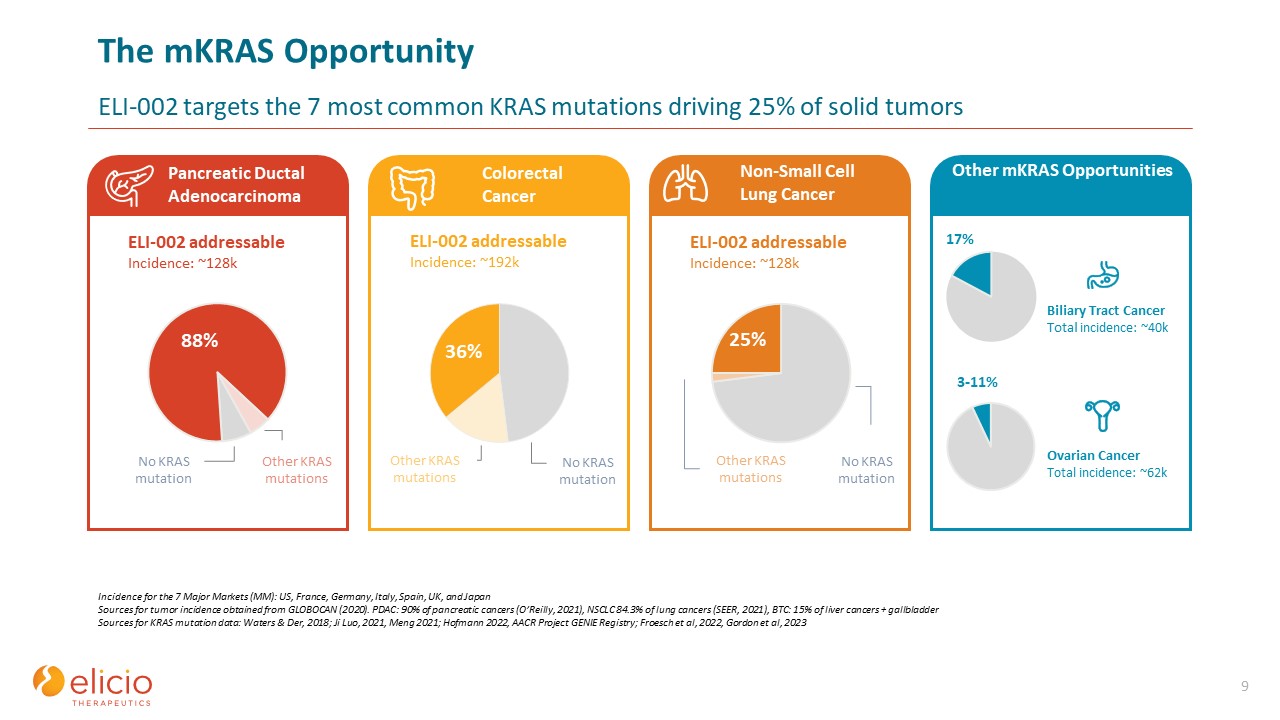
Phase 2 trial of ELI-002 monotherapy in pancreatic ductal adenocarcinoma (“PDAC”) planned to initiate in early 2024
|
|
|
● |
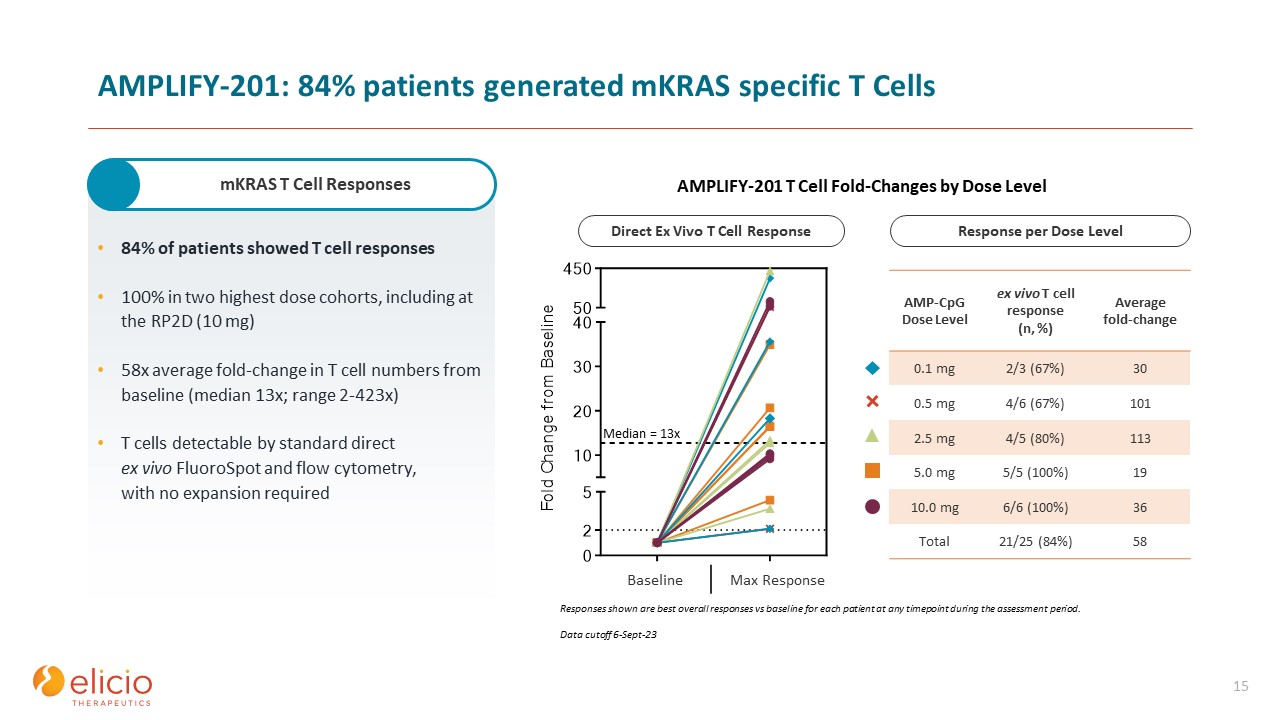
The data is as of September 6, 2023, based on 25 patients with solid tumors (20 pancreatic, 5 colorectal) who were positive for minimal residual mKRAS disease after locoregional
treatment.
|
|
|
● |
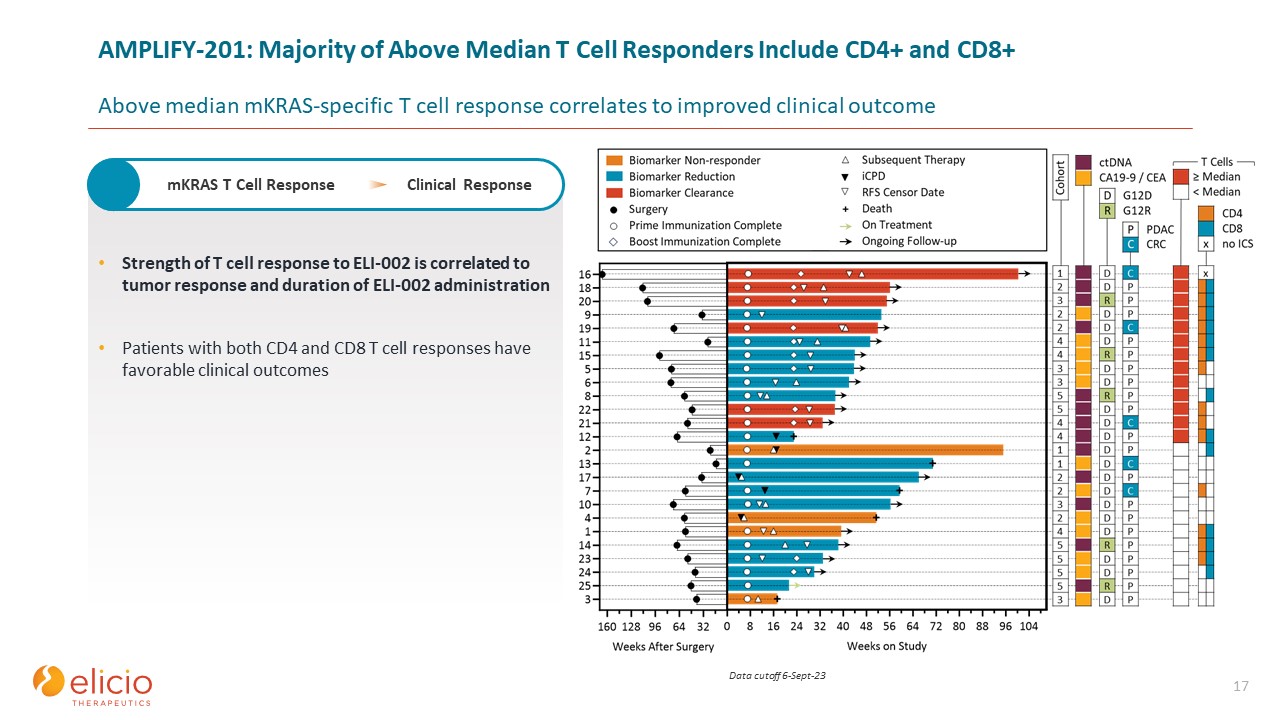
Direct ex vivo mKRAS-specific T cell responses were observed in 21/25 patients (84%; 59% both CD4+ and
CD8+).
|
|
|
● |
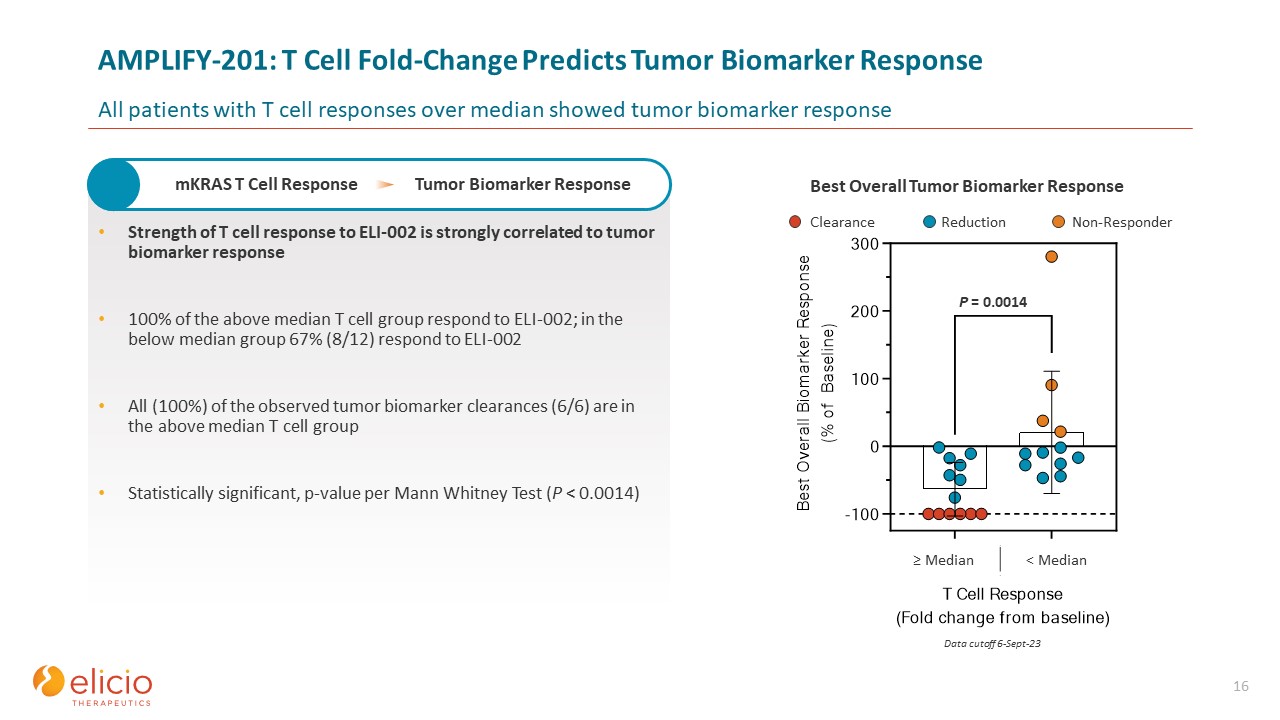
Tumor biomarker responses were observed in 21/25 patients (84%) and biomarker clearance in 6/25 patients, as determined by tumor-informed circulating tumor DNA (24%; 3
pancreatic, 3 colorectal).
|
|
|
● |
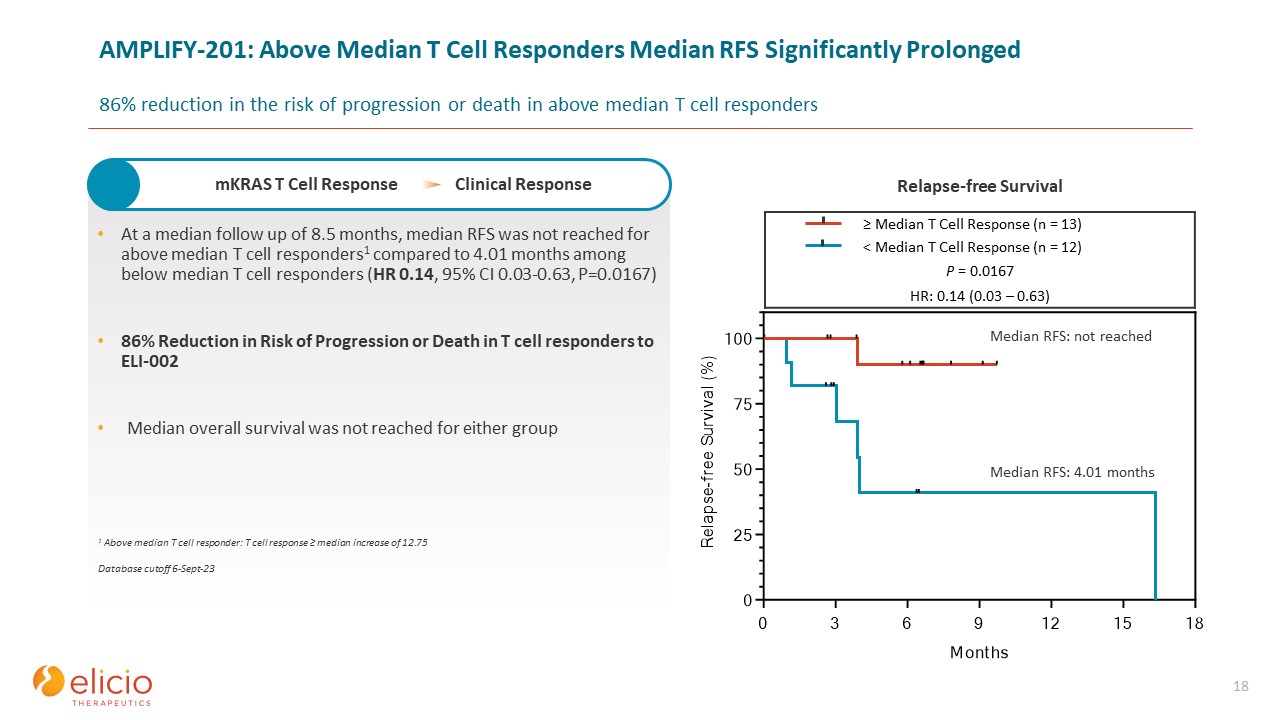
At 8.5 months median follow-up the median RFS of the 25-patient cohort was 16.33 months.
|
|
|
● |
Efficacy correlated with T cell response (≥ versus < median: 12.75-fold over baseline):
|
|
|
o |
Median tumor biomarker reduction was -76.0% compared to -10.2% in above versus below median T cell responders, respectively (p<0.0014).
|
|
|
o |
Median RFS was not reached compared to 4.01 months in above versus below median T cell responders, respectively (HR 0.14, 95% CI 0.03 to 0.63, p=0.0167).
|
|
|
o |
Patients with greater than median T cell response had an 86% reduction in the risk of progression or death.
|
|
|
● |
The association of RFS with T cell response was not correlated to baseline prognostic variables including tumor stage, recovery from prior cytotoxic therapy as assessed by
absolute neutrophil count or immune system subsets such as %CD4+ or %CD8+ of CD3+ lymphocytes.
|
|
|
● |
RFS was shorter in patients who began treatment with a low absolute lymphocyte count.
|
|
|
● |
No safety concerns were identified, and no dose limiting toxicities and no ≥ grade 3 treatment related adverse events were observed.
|