UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, DC 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d) of the
Securities Exchange Act of 1934
Date of report (Date of earliest event reported): January 7, 2026
REZOLUTE, INC.
(Exact Name of Registrant as Specified in Charter)
| Nevada | 001-39683 | 27-3440894 | ||
|
(State or Other Jurisdiction of Incorporation) |
(Commission File Number) |
(I.R.S. Employer Identification No.) |
275 Shoreline Drive, Suite 500, Redwood City, CA 94065
(Address of Principal Executive Offices, and Zip Code)
650-206-4507
Registrant’s Telephone Number, Including Area Code
Not Applicable
(Former Name or Former Address, if Changed Since Last Report)
Check the appropriate box below if the Form 8-K filing is intended to simultaneously satisfy the filing obligation of the registrant under any of the following provisions (see General Instruction A.2. below):
| ¨ | Written communication pursuant to Rule 425 under the Securities Act (17 CFR 230.425) |
| ¨ | Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12) |
| ¨ | Pre-commencement communication pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)) |
| ¨ | Pre-commencement communication pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section 12(b) of the Act:
| Title of each class | Trading Symbol(s) | Name of each exchange on which registered |
| Common Stock, par value $0.001 per share | RZLT | Nasdaq Capital Market |
Indicate by check mark whether the registrant is an emerging growth company as defined in Rule 405 of the Securities Act of 1933 (17 CFR §230.405 of this chapter) or Rule 12b-2 of the Securities Exchange Act of 1934 (17 CFR §240.12b-2 of this chapter).
Emerging growth company ¨
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ¨
| Item 7.01 | Regulation FD Disclosure |
On January 7, 2026, Rezolute, Inc. issued, (i) a press release announcing further insights into the sunRIZE trial, (ii) a cumulative table outlining data from the initial 9 tumor HI participants in the EAP, including patient characteristics, ersodetug dosing, and observed outcomes and (iii) an updated corporate deck.
The information in this Current Report on Form 8-K, including Exhibits 99.1, 99.2 and 99.3 shall not be deemed “filed” for purposes of Section 18 of the Securities Exchange Act of 1934, as amended (the “Exchange Act”), or otherwise subject to the liability of that section, nor shall it be deemed incorporated by reference in any filing under the Securities Act of 1933, as amended, or the Exchange Act, whether made before or after the date hereof, except as expressly set forth by specific reference in such filing to this Current Report on Form 8-K.
| Item 9.01 | Financial Statements and Exhibits. |
(d) Exhibits.
| Exhibit No. | Description |
| 99.1 | Press Release, dated January 7, 2026 |
| 99.2 | EAP Data |
| 99.3 | Corporate Deck |
| 104 | Cover Page Interactive Data File (formatted as inline XBRL) |
SIGNATURES
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
| REZOLUTE, INC. | ||
| DATE: January 7, 2026 | By: | /s/ Nevan Charles Elam |
| Nevan Charles Elam | ||
| Chief Executive Officer | ||
Exhibit 99.1

Rezolute Provides Insights from its Phase 3 sunRIZE Study in Congenital Hyperinsulinism and Shares Findings from its Expanded Access Program in Tumor Hyperinsulinism
Company believes that data from sunRIZE and the Expanded Access Program (EAP) provide evidence of activity of ersodetug in both indications
Company plans to meet with FDA to align on path forward for congenital HI
REDWOOD CITY, Calif., January 7, 2025 – Rezolute, Inc. (Nasdaq: RZLT) (“Rezolute” or the “Company”), a late-stage rare disease company focused on treating hypoglycemia caused by all forms of hyperinsulinism (HI), today shared observations from the Phase 3 sunRIZE study in patients with congenital HI and provided details on the treatment of tumor HI patients with ersodetug under the Company’s EAP.
Congenital HI
While sunRIZE did not meet its primary (hypoglycemia events) or key secondary (time in hypoglycemia) endpoints, the Company believes that the totality of the data further supports previous clinical evidence that ersodetug is active against hypoglycemia in patients. Specifically, there was evidence of pharmacologic activity as target therapeutic drug concentrations were achieved in both treatment groups (5 mg/kg and 10 mg/kg) with highly sensitive biomarker responses (increases in circulating insulin) in the active treatment groups that are indicative of reduced insulin activity at its receptor. Notably, these responses were consistent with those of the Company’s Phase 2 RIZE study (see Figure 1).

The study also demonstrated reductions from baseline in events and time in hypoglycemia in both treatment groups, but not enough to be statistically significant compared to the pronounced study effect in the placebo arm. While in the early stages of evaluating study data and understanding the results, learnings in the field of glycemic control and initial observations from sunRIZE inform the Company’s belief that the pharmacologic response can translate to clinical efficacy. The magnitude of the placebo response observed for hypoglycemia events reveals a significant challenge in studying glucose in an ambulatory setting, where factors such as intensive monitoring where caregivers receive alerts regarding hypoglycemic events and frequent clinical interactions can independently influence outcomes.
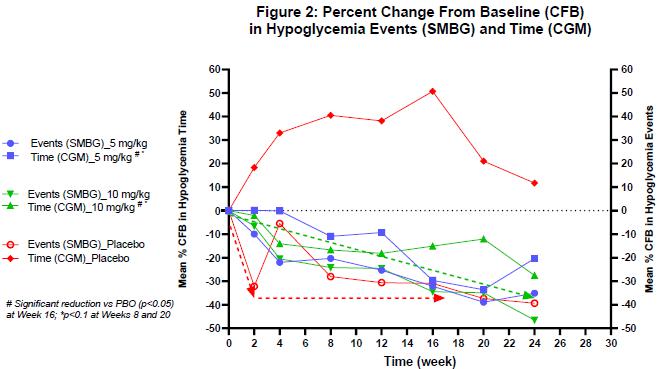
The Company believes that the extent of reduction from baseline in hypoglycemia events and time in hypoglycemia relative to placebo (see Figure 2) may have been impacted by the prolonged treatment duration of six months and the fact that glucose monitoring is necessary for safe patient management while also serving as the key endpoint in the study. This sentiment has been shared with the Company by investigator physicians as well as study participants. The Company is currently exploring how to characterize the overall study dynamic including evaluating patient-reported quality of life outcomes.
In light of these limitations, assessing the potential benefit in the ongoing open-label extension (OLE) portion of the study will be important. All 59 participants who completed the study elected to continue to receive ersodetug in the OLE. To date, 57 participants remain in the OLE, with an exposure duration ranging from ~6 weeks for the most recently entered patients, to ~18 months. The Company believes that a potential indicator of ersodetug’s underlying efficacy is that several children in the OLE have been able to stop taking all other therapies and are now receiving ersodetug as monotherapy.
The Company looks forward to interacting with FDA in Q1 2026 under its Breakthrough Therapy Designation to further characterize these and other clinical outcomes to inform a review of the full sunRIZE dataset with the intent of exploring options for this indication.
Tumor HI
Over the past two years, Rezolute has collaborated with investigators across the United States and in Europe to provide ersodetug to more than a dozen patients with severe and refractory hypoglycemia due to tumor HI, including malignant pancreatic neuroendocrine tumors (insulinomas) and non-islet cell tumors. The Company has previously reported that the therapy was generally well-tolerated, and that patients experienced substantial improvement in hypoglycemia, which led to a reduction in the rate of glucose infusion in the hospital (GIR) or the complete discontinuation of infusion and discharge from the hospital.
Presented in a table filed today on Form 8-K with the U.S. Securities and Exchange Commission are cumulative data from the initial 9 participants in the EAP, including patient characteristics, ersodetug dosing, and observed outcomes. This same data cohort was provided to FDA last year in support of the Company’s request for Breakthrough Therapy Designation and subsequently informed the discussion with FDA that led to revision of the Phase 3 upLIFT study in tumor HI to a single arm, open-label study. In summary, 75% of the patients receiving IV dextrose/total parental nutrition (TPN) in the EAP achieved a complete discontinuation of IV dextrose/TPN.
This outcome is highly relevant to the ongoing upLIFT study and provides additional evidence of the activity and potential efficacy of ersodetug across various forms of HI. Notably, the GIR assessment in the EAP is the primary endpoint in upLIFT, which measures the number of participants (out of ~16) who achieve at least a 50% reduction in GIR, an objective endpoint in a highly controlled hospital setting. For statistical significance, 9 of 16 open-label participants need to achieve this threshold. Topline results are anticipated in the second half of 2026.
About sunRIZE
The Phase 3 sunRIZE study (RZ358-301) was a multi-center, randomized, double-blind, placebo-controlled, parallel arm study designed to evaluate the efficacy and safety of ersodetug in patients with congenital hyperinsulinism (HI), ages 3 months to 45 years old, who were experiencing continued hypoglycemia on currently available standard of care (SOC). Eligible participants were randomized to one of three treatment arms to receive either ersodetug (5 or 10 mg/kg) or matched placebo-control as add on to existing SOC. Study drug was administered every other week during an initial loading phase, and then every 4 weeks during the 6-month controlled pivotal treatment period. Following the pivotal treatment phase of the study, participants could roll-over into an optional open-label extension phase to continue to receive ersodetug.
The study enrolled 63 participants in more than a dozen countries around the world, inclusive of U.S. patients. The primary and key secondary efficacy endpoints in the study were the change from baseline in the average number of hypoglycemia events per week and the average percent time in hypoglycemia, respectively, over six months of treatment.
About Ersodetug
Ersodetug is a fully human monoclonal antibody that binds allosterically to the insulin receptor to decrease receptor over-activation by insulin and related substances (such as IGF-2) in the setting of hyperinsulinism (HI), thereby improving hypoglycemia. Because ersodetug acts downstream from the pancreas, it has the potential to be universally effective at treating hypoglycemia due to any congenital or acquired form of HI.
About Rezolute, Inc.
Rezolute is a late-stage rare disease company focused on treating hypoglycemia caused by hyperinsulinism (HI). The Company’s antibody therapy, ersodetug, is designed to treat all forms of HI and has been studied in clinical trials and used in real-world cases for the treatment of both congenital and tumor HI. For more information, visit www.rezolutebio.com.
Forward-Looking Statements
This release, like many written and oral communications presented by Rezolute and our authorized officers, may contain certain forward-looking statements regarding our prospective performance and strategies within the meaning of Section 27A of the Securities Act and Section 21E of the Securities Exchange Act of 1934, as amended. We intend such forward-looking statements to be covered by the safe harbor provisions for forward-looking statements contained in the Private Securities Litigation Reform Act of 1995 and are including this statement for purposes of said safe harbor provisions. Forward-looking statements, which are based on certain assumptions and describe future plans, strategies, and expectations of Rezolute, are generally identified by use of words such as "anticipate," "believe," "estimate," "expect," "intend," "plan," "project," "seek," "strive," "try," or future or conditional verbs such as "could," "may," "should," "will," "would," or similar expressions. These forward-looking statements include, but are not limited to, the potential efficacy of ersodetug in treating hypoglycemia associated with either congenital or tumor HI, the possibility of FDA agreeing to a streamlined path for advancing the congenital HI program notwithstanding the lack of statistical significance in the sunRIZE study, or the timing of the release of topline results for upLIFT. Our ability to predict results or the actual effects of our plans or strategies is inherently uncertain. Accordingly, actual results may differ materially from anticipated results. Readers are cautioned not to place undue reliance on these forward-looking statements, which speak only as of the date of this release. Except as required by applicable law or regulation, Rezolute undertakes no obligation to update these forward-looking statements to reflect events or circumstances that occur after the date on which such statements were made. Important factors that may cause such a difference include any other factors discussed in our filings with the SEC, including the Risk Factors contained in Rezolute’s Annual Report on Form 10-K and Quarterly Reports on Form 10-Q, which are available at the U.S. Securities and Exchange Commission’s website at www.sec.gov. You are urged to consider these factors carefully in evaluating the forward-looking statements in this release and are cautioned not to place undue reliance on such forward-looking statements, which are qualified in their entirety by this cautionary statement.
Rezolute Contacts:
Christen Baglaneas
cbaglaneas@rezolutebio.com
508-272-6717
Carrie McKim
cmckim@rezolutebio.com
336-608-9706
Exhibit 99.2
Tumor HI EAP Patient Profiles
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | Patient 7 | Patient 8# | Patient 9 | |
| Gender (M/F) / Age (Years) | M / 55 | F / 50 | F / 50 | F / 43 | M / 74 | M / 62 | M / 74 | M / 53 | M / 24 |
| Diagnosis | Metastatic Insulinoma | Metastatic Insulinoma | Neuroendocrine Carcinoma of the Cervix | Metastatic Insulinoma | Metastatic Insulinoma | Metastatic Insulinoma |
Metastatic Insulinoma |
Metastatic Proinsulinoma | Metastatic Insulinoma |
| # of Anti-hypoglycemic therapies at enrollment | 4 | 3 | 3 | 4 | 4 | 3 | 5 | 2 | 4 |
| Glucose Infusion Rate (GIR, mg/kg/min) at ersodetug initiation | 6.0 |
7.0 (home TPN) |
5.1 | 6.2 | 4.9 | n/a (ambulatory) | 5.6 | Unknown amount | 3.1 |
| Ersodetug Dose Regimen (dose/frequency) | 6-9 mg/kg every 1-4 weeks | 6-9 mg/kg every 1-2 weeks | 9 mg/kg, every 1-2 weeks | 9-12 mg/kg every 1-2 weeks | 9 mg/kg every 1-3 weeks | 9 mg/kg every 1-2 weeks | 6-9 mg/kg every 1-2 weeks | 9 mg/kg every 1-2 weeks | 9 mg/kg every 1-3 weeks |
| Percent Reduction in GIR by 8 weeks of Ersodetug treatment (duration of Phase 3 upLIFT study) | >50%, then 100% by 9 weeks | <50% | 100% | 100% | 100% | n/a | 100% | Unknown amount | 100% |
| Time to IV Glucose discontinuation (days) | 74 | 139 (achieved 50% reduction) |
4 | 5 | 2 | n/a | 3 | n/a | 42 |
| Length of Hospitalization prior to ersodetug (days) | 28 | n/a (ambulatory) | 15 | 49 | 34 | n/a (ambulatory) | 4 | Unknown duration | 16 |
| # of Hospitalized Days in the 30-day period following ersodetug initiation | 30 | 0 | 7 | 8 | 8 | 0 | 16 | 30 | 1 |
| Baseline ECOG * | 3 | 2 | 3 | 3 | 3 | 1 | 1 | 3 | 1 |
| ECOG, Month 3 on ersodetug | 0 | 2 | 0 | 0 | 0 | 0 | 1 | 5 | 0 |
| Total Duration of ersodetug therapy (months) | 13 | 5 | 5 | 14 | 22 (ongoing) | 18 (ongoing) | 6 | 1.5 | 10 |
| Overall Survival (months) | 14 | 5 | 5 | 14 | 22 (living) | 18 (living) | 6 | 1.5 | 10 |
# Patient was critically ill when treatment commenced and died of sepsis prior to determination of whether there was a therapeutic effect
*Eastern Cooperative Oncology Group (ECOG) Performance Status is a standardized measure of functional status ranging from 0 (fully active) to 5 (death), with increasing scores indicating greater disability and reduced ability to perform daily activities
Exhibit 99.3


A Late - stage Rare Disease Company Treating Hyperinsulinism Corporate Presentation Forward Looking Statements 2 This presentation, like many written and oral communications presented by Rezolute and our authorized officers, may contain certain forward - looking statements regarding our prospective performance and strategies within the meaning of Section 27 A of the Securities Act and Section 21 E of the Securities Exchange Act of 1934 , as amended . We intend such forward - looking statements to be covered by the safe harbor provisions for forward - looking statements contained in the Private Securities Litigation Reform Act of 1995 and are including this statement for purposes of said safe harbor provisions . Forward - looking statements, which are based on certain assumptions and describe future plans, strategies, and expectations of Rezolute, are generally identified by use of words such as "anticipate," "believe," "estimate," "expect," "intend," "plan," "project," "prove," "potential," "seek," "strive," "try," or future or conditional verbs such as "predict," "could," "may," "likely," "should," "will," "would," or similar expressions . These Forward - Looking statements include, but are not limited to, statements regarding the sunRIZE clinical study, the RIZE study, the upLIFT study, the complete removal of the partial clinical holds on RZ 358 for the treatment of hypoglycemia, the Investigational New Drug (IND) application for RZ 358 ( ersodetug ), the ability of RZ 358 to become an effective treatment, the effectiveness or future effectiveness of RZ 358 as a treatment, statements regarding clinical trial timelines for the treatment . Our ability to predict results or the actual effects of our plans or strategies is inherently uncertain . Accordingly, actual results may differ materially from anticipated results . Readers are cautioned not to place undue reliance on these forward - looking statements, which speak only as of the date of this release . Except as required by applicable law or regulation, Rezolute undertakes no obligation to update these forward - looking statements to reflect events or circumstances that occur after the date on which such statements were made . Important factors that may cause such a difference include any other factors discussed in our filings with the SEC, including the Risk Factors contained in the Rezolute’s Annual Report on Form 10 - K and Quarterly Reports on Form 10 - Q, which are available at the SEC’s website at www . sec . gov . You are urged to consider these factors carefully in evaluating the forward - looking statements in this release and are cautioned not to place undue reliance on such forward - looking statements, which are qualified in their entirety by this cautionary statement . This presentation shall not constitute an offer to sell or the solicitation of an offer to buy, nor shall there be any sale of these securities in any state or other jurisdiction in which such offer, solicitation or sale would be unlawful prior to registration or qualification under the securities laws of any such state or other jurisdiction . @2026 Rezolute, Inc. All Rights Reserved.

A Rare Disease Company Treating Hyperinsulinism 3 Well - capitalized for execution – $152 million in cash with runway to mid - 2027 Seasoned management team with demonstrated success from early development through commercialization Total $1B+ global market opportunity with additional upside through expansion Compelling ev idence that ersodetug is active against hypoglycemia in patients under the Company’s Expanded Access Program Two rare disease programs evaluating ersodetug to treat hypoglycemia in congenital HI and tumor HI RZ358 ( ersodetug ) is an antibody designed to treat hypoglycemia caused by all forms of hyperinsulinism (HI) @2026 Rezolute, Inc. All Rights Reserved.

Two Phase 3 Indications Targeting Hyperinsulinism 4 Milestone Expected Next Milestone Phase 3 Phase 2 Phase 1 IND - Enabling Target Program Q1 2026 FDA Engagement Congenital Hyperinsulinism Ersodetug 2H 2026 Topline data Tumor Hyperinsulinism Ersodetug @2026 Rezolute, Inc. All Rights Reserved.

Ersodetug Treatment for Hyperinsulinism (HI)

Hypoglycemia as a Result of HI 6 Rare disease caused by tumors that produce insulin or insulin - like substances such as IGF - 2 Rare pediatric genetic disease characterized by excessive insulin production Congenital HI Tumor HI Ersodetug has been studied in clinical trials and used in real - world cases for the treatment of HI Hypoglycemia o Severe, persistent, life - threatening complication of over activation of the insulin receptor o Lack of effective treatment options @2026 Rezolute, Inc. All Rights Reserved.

Antibody Designed to Treat All Forms of HI 7 INSULIN or IGF - 2 GLUCOSE Ersodetug Reduces Insulin Binding & Signaling Ersodetug Increases Available Blood Glucose Reduced Glucose Uptake • Fully human monoclonal antibody with a novel mechanism acting downstream from production source (e.g. pancreas) • Allosterically binds to the insulin receptor to counteract excess signaling by insulin or related hormones (e.g. IGF) • Modulating effect helps maintain glucose values in a healthy range • Administered by IV infusion @2026 Rezolute, Inc. All Rights Reserved.

Congenital HI

Disease Background @2026 Rezolute, Inc. All Rights Reserved. 9 • 1 in 22,000 live births in the US 1 , translating to approximately 165 new patients per year • Often presents within first month of life • Most common cause of persistent hypoglycemia in infants and children • Requires constant monitoring as serious hypoglycemic lows are often missed • 50% of children with congenital HI have neurological deficiencies caused by hypoglycemic lows • Risk of coma, death, and other serious complications • No therapy has been developed and approved for chronic treatment 2 1 Based on the Forian and Compass claims data. 2 Based on the RIZE clinical trial outcomes and the evidence of benefit in this serious condition with substantial unmet medica l need, ersodetug was granted Breakthrough Therapy Designation by the US Food and Drug Administration (FDA), a priority medicines (PRIME) designation by th e E uropean Medicines Agency (EMA), an Innovation Passport designation by the U.K. Innovative Licensing and Access Pathway (ILAP) Steering Group, and Orphan Drug Designation in the US and EU for t he treatment of hypoglycemia due to congenital HI.

Inadequate Standard of Care 10 • Diazoxide (DZ) is first line treatment and the only approved medication for hypoglycemia caused by HI • 60% of patients do not respond to DZ • May experience frequent and serious adverse reactions including volume overload, heart failure, and pulmonary hypertension • Patients report 1 intolerable side effects including increased body hair (92%), loss of appetite (43%), swelling(27%), facial changes (27%), and gastrointestinal upset (26%) • Other available treatment options are suboptimal • Glucagon tends to be temporizing and short - term • Somatostatin analogs have marginal efficacy and potentially serious pediatric side effects • Pancreatectomy is an invasive option in DZ non - responsive patients, but frequently requires adjuvant medications until insulin - dependent diabetes eventually ensues • Intensive feeding regimens (e.g. tube feeding) often underlie all of these approaches • Each of these therapies can contribute to a cycle of poor appetite and feeding aversions 1 HI Global Registry 2024 Annual Report: 223 patients surveyed, 183 have taken DZ. @2026 Rezolute, Inc. All Rights Reserved.

Therapies in Development @2026 Rezolute, Inc. All Rights Reserved. 11 1 Formulation allows for subcutaneous dosing. 2 Phase 2 data supports potential use. SC: subcutaneous. SOC: standard of care. PBH: post - bariatric hypoglycemia. MOA: mechanism of action. Clinical Barriers HI Indication Dosing Stage Mechanism Asset N/A Congenital, Tumor, PBH 2 IV 1 , once monthly Phase 3 Insulin receptor allosteric modulator Ersodetug • Utility in chronic use unproven; likely need to combine with other therapies Congenital Continuous Infusion Pump Phase 3 Glucagon analogue Dasiglucagon (Zealand) • No plans to pursue cHI • MOA suited to PBH PBH IV, 1 - 2 times daily Phase 3 GLP - 1 receptor antagonist Avexitide (Amylyx) • Earlier in development • Similar drawbacks as dasiglucagon Congenital SC injection, once weekly Phase 2 Glucagon analogue HM - 15136 (Hanmi) Ersodetug has been studied in clinical trials and used in real - world cases for the treatment of HI Phase 2b RIZE Study Results 12 • 23 participants • Average age ~6.5 (16 participants were between 2 - 6 years of age) • Diverse group across gender and genetics • ~20% average daily time in hypoglycemia and 13 hypoglycemia events per week at baseline • Participants were on standard of care • Predictable and dose - dependent pharmacokinetics • Generally safe and well - tolerated • No adverse drug reactions • No study terminations • No clinically - significant hyperglycemia or hyperglycemia AEs • Study exceeded expectations for glucose correction: • Improvement in hypoglycemia time and events of up to ~90% at top doses • Nearly universal response rate at the top dose SOC: standard of care.

AEs: adverse events. @2026 Rezolute, Inc. All Rights Reserved.
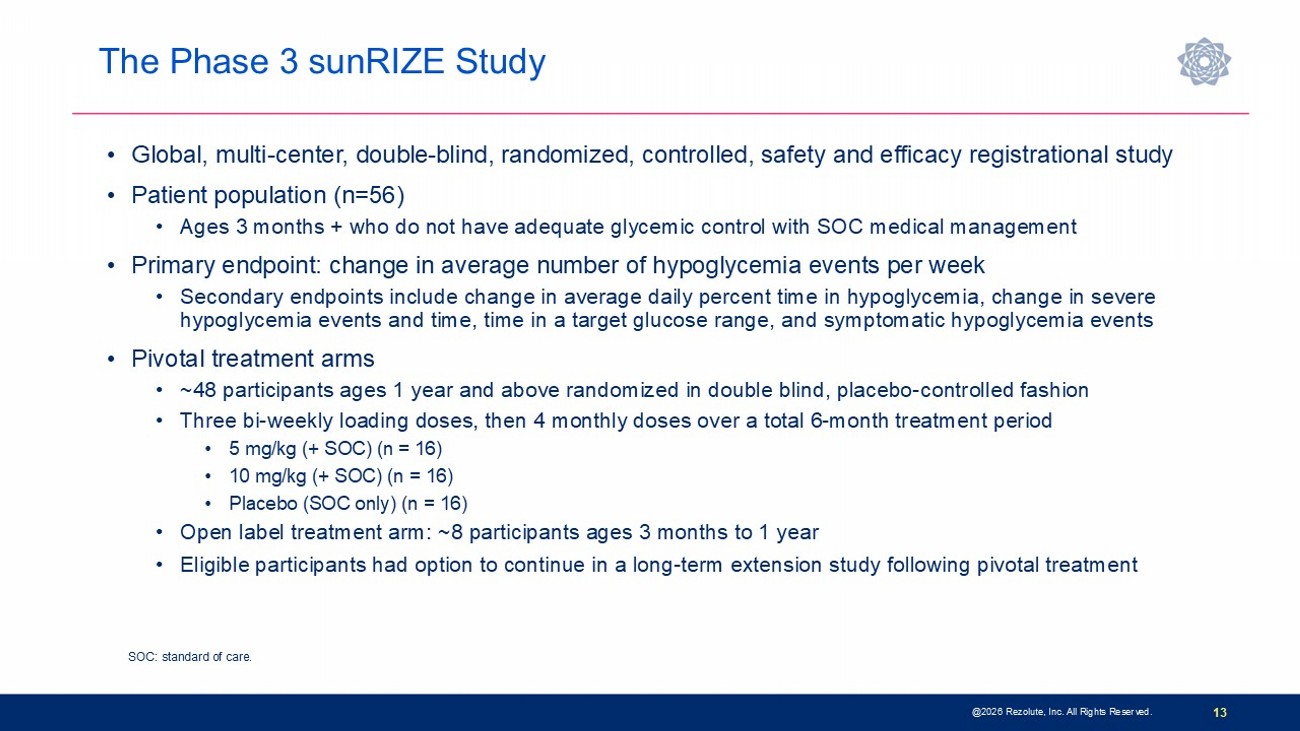
The Phase 3 sunRIZE Study @ 2026 Rezolute, Inc. All Rights Reserved. 13 • Global, multi - center, double - blind, randomized, controlled, safety and efficacy registrational study • Patient population (n=56) • Ages 3 months + who do not have adequate glycemic control with SOC medical management • Primary endpoint: change in average number of hypoglycemia events per week • Secondary endpoints include change in average daily percent time in hypoglycemia, change in severe hypoglycemia events and time, time in a target glucose range, and symptomatic hypoglycemia events • Pivotal treatment arms • ~48 participants ages 1 year and above randomized in double blind, placebo - controlled fashion • Three bi - weekly loading doses, then 4 monthly doses over a total 6 - month treatment period • 5 mg/kg (+ SOC) (n = 16) • 10 mg/kg (+ SOC) (n = 16) • Placebo (SOC only) (n = 16) • Open label treatment arm: ~8 participants ages 3 months to 1 year • Eligible participants had option to continue in a long - term extension study following pivotal treatment SOC: standard of care.

Phase 3 sunRIZE Study Results Highlights 14 • Study did not meet the primary or key secondary measured glucose endpoints • Up to 45% reduction in events by SMBG in treated groups; not significantly different from placebo (40%) • Reduction in hypoglycemia time by CGM did not reach statistical significance at end - of - treatment ( - 32%; p=0.3) • Reductions in hypoglycemia in ersodetug groups appears to be pharmacologically mediated • Predictable and dose - dependent target concentrations were achieved • Highly sensitive biomarker responses (increases in circulating insulin) indicate drug activity • Decreases in hypoglycemia progressed over course of study and were consistent between SMBG - measured events and CGM - measured hypoglycemia time • 100% roll - over to open - label extension and very high retention rate • Several patients have stopped other therapies and remain on ersodetug as monotherapy • No limiting safety findings • 4 early terminations due to adverse events (2 serious hypersensitivity reactions, 1 infusion reaction, 1 mild hypertrichosis) • Hypertrichosis was the only other commonly reported AE in ersodetug patients (n=14; 36%) • No liver safety signals @2026 Rezolute, Inc. All Rights Reserved.
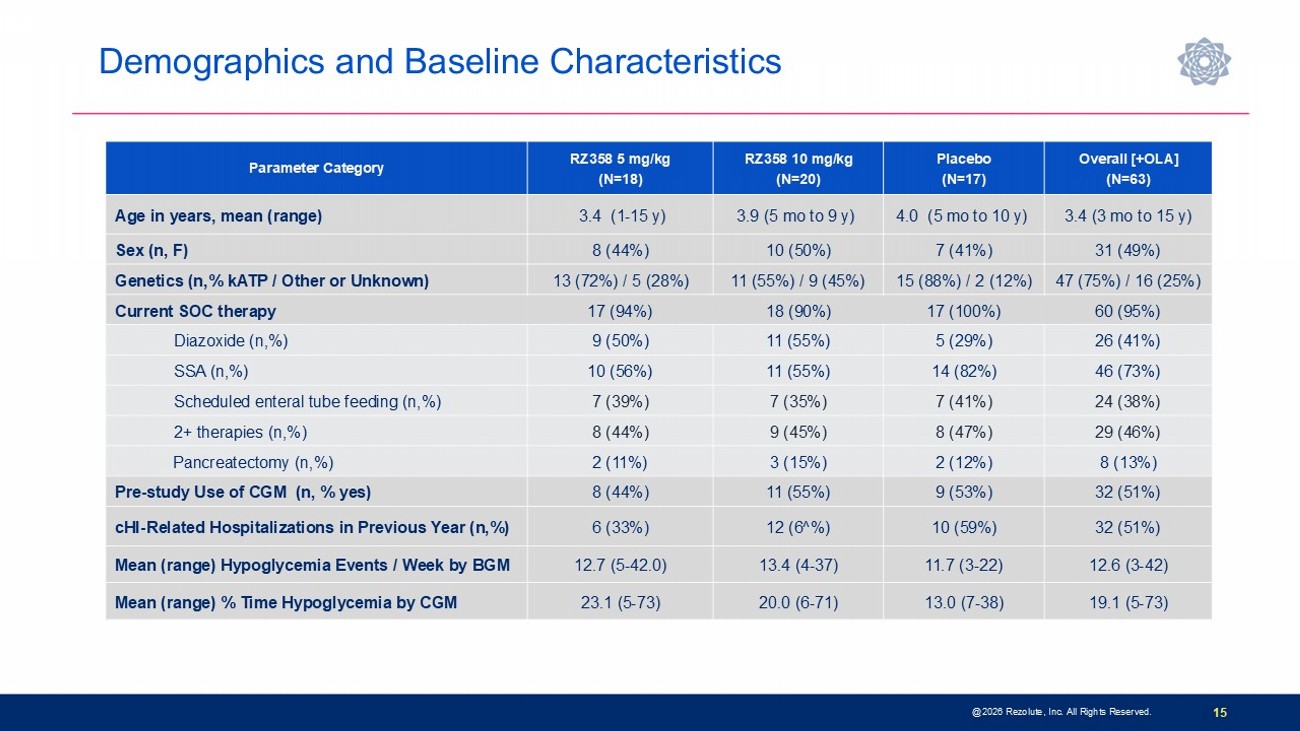
@2026 Rezolute, Inc. All Rights Reserved. 15 Overall [+OLA] (N=63) Placebo (N=17) RZ358 10 mg/kg (N=20) RZ358 5 mg/kg (N=18) Parameter Category 3.4 (3 mo to 15 y) 4.0 (5 mo to 10 y) 3.9 (5 mo to 9 y) 3.4 (1 - 15 y) Age in years, mean (range) 31 (49%) 7 (41%) 10 (50%) 8 (44%) Sex (n, F) 47 (75%) / 16 (25%) 15 (88%) / 2 (12%) 11 (55%) / 9 (45%) 13 (72%) / 5 (28%) Genetics (n,% kATP / Other or Unknown) 60 (95%) 17 (100%) 18 (90%) 17 (94%) Current SOC therapy 26 (41%) 5 (29%) 11 (55%) 9 (50%) Diazoxide (n,%) 46 (73%) 14 (82%) 11 (55%) 10 (56%) SSA (n,%) 24 (38%) 7 (41%) 7 (35%) 7 (39%) Scheduled enteral tube feeding (n,%) 29 (46%) 8 (47%) 9 (45%) 8 (44%) 2+ therapies (n,%) 8 (13%) 2 (12%) 3 (15%) 2 (11%) Pancreatectomy (n,%) 32 (51%) 9 (53%) 11 (55%) 8 (44%) Pre - study Use of CGM (n, % yes) 32 (51%) 10 (59%) 12 (6^%) 6 (33%) cHI - Related Hospitalizations in Previous Year (n,%) 12.6 (3 - 42) 11.7 (3 - 22) 13.4 (4 - 37) 12.7 (5 - 42.0) Mean (range) Hypoglycemia Events / Week by BGM 19.1 (5 - 73) 13.0 (7 - 38) 20.0 (6 - 71) 23.1 (5 - 73) Mean (range) % Time Hypoglycemia by CGM Demographics and Baseline Characteristics P reliminary PK: Therapeutic and Age - Comparable Concentrations @2026 Rezolute, Inc. All Rights Reserved. 16 0 2 4 6 8 10 12 14 16 18 20 22 24 10 100 1000 Study Week R Z 3 5 8 S e r u m C o n c e n t r a t i o n ( μ g / m l ) RZ358_10 mg/kg_DB RZ358_5 mg/kg_DB Ph2 (RIZE) [trough] at effective doses


Increase in Circulating Insulin Consistent With Ph2 (RIZE) @2026 Rezolute, Inc. All Rights Reserved. 17 Sensitive Biomarker of Drug Activity -4 -2 0 2 4 6 8 10 12 14 16 18 20 22 24 0 50 100 150 200 250 300 M e a n I n s u l i n C o n c e n t r a t i o n ( μ I U / m l ) Weeks sunRIZE_5 mg/kg_Trough sunRIZE_10 mg/kg_Trough sunRIZE_Placebo_Trough Dosing (sunRIZE) sunRIZE_5 mg/kg_Post-dose sunRIZE_10 mg/kg_Post-dose sunRIZE_Placebo_Post-dose RIZE_6 mg/kg_Trough RIZE_6 mg/kg_Post-dose RIZE_9 mg/kg_Trough RIZE_9 mg/kg_Post-dose Dosing (RIZE)

Percent Change in Average Weekly Hypoglycemia Events by Self - Monitored Blood Glucose (SMBG) @2026 Rezolute, Inc. All Rights Reserved.

18 0 4 8 12 16 20 24 5 10 15 Time (Week) H y p o g l y c e m i a E v e n t s ( M e a n ± S D ) RZ358_5 mg/kg RZ358_10 mg/kg Placebo -80 -60 -40 -20 0 % Change from BL to EOT (Week 24) Full Analysis Set % C h a n g e ( L S m e a n ± S E ) NS NS Percent Change in Average Daily Percent Time in Hypoglycemia by Continuous Glucose Measurement (CGM) @2026 Rezolute, Inc. All Rights Reserved.

19 -60 -40 -20 0 20 40 % Change from BL to Week 24 (Full Analysis Set) % C h a n g e ( L S M e a n ± S E ) p=0.44 p=0.30 -60 -40 -20 0 20 40 60 % Change from BL to Week 24 (Per Protocol Population) % C h a n g e ( L S M e a n ± S E ) p=0.28 p=0.18 n=15 n=14 n=12 0 4 8 12 16 20 24 10 15 20 25 Time (Week) % H y p o g l y c e m i a T i m e ( M e a n ± S D ) RZ358_5 mg/kg RZ358_10 mg/kg Placebo Hypoglycemia Reductions in Ersodetug Groups Appear Pharmacologically Mediated 20 • Target therapeutic concentrations achieved • Typical biomarker responses occurred • Decline of hypoglycemia was gradual and progressive • Concordant reduction in hypoglycemia by two different measurements (events [SMBG] and time [CGM]) • Sudden and discordant decrease in events in placebo suggests behavioral confounders influenced the response • Patient/Site reports, PRO/QoL outcomes, OLE may highlight these impacts @2026 Rezolute, Inc. All Rights Reserved.

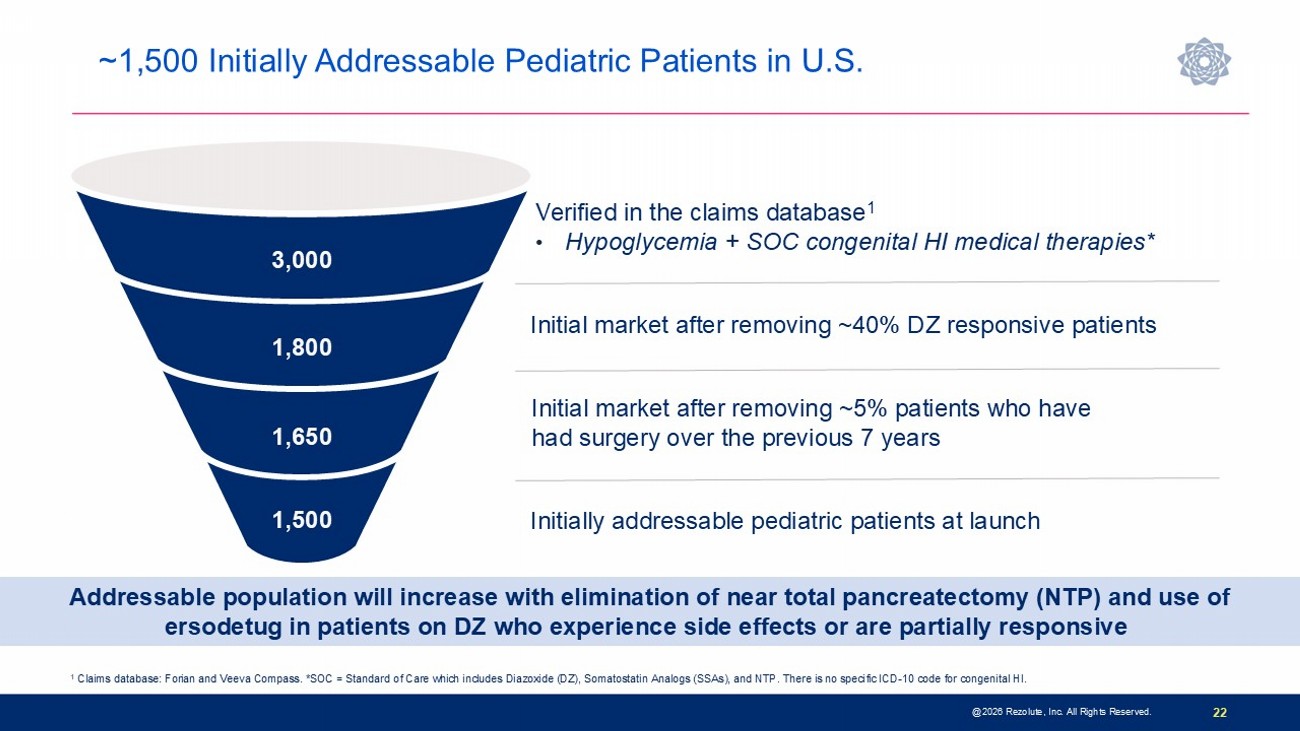
0 4 8 12 16 20 24 28 -60 -40 -20 0 20 40 60 -60 -40 -20 0 20 40 60 Percent Change From Baseline (CFB) in Hypoglycemia Events (SMBG) and Time (CGM) Time (week) M e a n % C F B i n H y p o g l y c e m i a T i m e M e a n % C F B i n H y p o g l y c e m i a E v e n t s Events (SMBG)_5 mg/kg Time (CGM)_5 mg/kg # * Time (CGM)_10 mg/kg # * Events (SMBG)_10 mg/kg Time (CGM)_Placebo Events (SMBG)_Placebo # Significant reduction vs PBO (p<0.05) at Week 16; *p<0.1 at Weeks 8 and 20 Study Conclusions and Next Steps @2026 Rezolute, Inc. All Rights Reserved. 21 • Study/placebo effect observed with primary endpoint (SMBG) • Previous precedent for this observation in this patient population • Glucose - related endpoints in an outpatient study are challenging and likely influenced by participant behaviors • Frequent visits and real - time glucose monitoring • Statistically significant reductions in hypoglycemia time by CGM observed at some time points • There is evidence of drug activity: • Therapeutic concentrations achieved • Gradual, progressive pattern of hypoglycemia reduction in both measurement types (events and time) • Trends if not significant hypoglycemia reduction at some time points, particularly in post - hoc analyses with more favorable populations or statistical approaches • Patient/site reports have been very favorable, supported by near universal participation/retention in OLE to date, with sites reporting discontinuation of background therapies/tube - feeding in their patients • Company believes that the totality of data supports a path forward and plans to initiate FDA discussions in Q1 of this year 22 @2026 Rezolute, Inc. All Rights Reserved. Verified in the claims database 1 • Hypoglycemia + SOC congenital HI medical therapies* 1 Claims database: Forian and Veeva Compass. *SOC = Standard of Care which includes Diazoxide (DZ), Somatostatin Analogs (SSAs), and NTP. There is no s pe cific ICD - 10 code for congenital HI. 1,500 1,650 1,800 3,000 Initial market after removing ~5% patients who have had surgery over the previous 7 years Initial market after removing ~40% DZ responsive patients Initially addressable pediatric patients at launch Addressable population will increase with elimination of near total pancreatectomy (NTP) and use of ersodetug in patients on DZ who experience side effects or are partially responsive ~1,500 Initially Addressable Pediatric Patients in U.S.

Tumor HI

Disease Background 24 • Hypoglycemia caused by two distinct tumor types: • Islet Cell Tumors (ICT) • Excessive secretion of insulin • Malignant insulinomas are the most common ICTs that cause hypoglycemia • Non - Islet Cell Tumors (NICT) • Produce and secrete insulin - like substances such as IGF - 2 that over activate the insulin receptor • Hepatocellular carcinomas (HCC) are the most common NICTs that cause hypoglycemia in addition to several other tumor types including fibrosarcomas and mesotheliomas • Significant unmet need across both tumor types • Resulting hypoglycemia is often severe and may have serious adverse outcomes • Limited treatment options with poor efficacy and safety profiles • High morbidity and mortality rates • Can require hospitalization (often prolonged and in ICU) and interferes with patient quality of life • May prevent adjuvant tumor treatment @2026 Rezolute, Inc. All Rights Reserved.

Treatment Options and Unmet Need 25 • Tumor - directed therapies do not directly treat hypoglycemia • Adequate hypoglycemia management is required prior to initiation of tumor - targeted therapies • Therapies to treat malignant insulinoma are often ineffective or poorly tolerated • Diazoxide (DZ) is the only approved treatment • Suboptimal response rates and serious side effects • Somatostatin analogs (SSAs) • Used off - label with limited success • May worsen hypoglycemia in tumor HI setting • mTOR - inhibitors • Used off - label and have potentially severe side effects • Limited and often ineffective treatment options for hepatocellular carcinoma (HCC) • Medical therapies directed at suppressing insulin secretion such as DZ and SSAs do not work in non - islet cell tumors (NICTs) where HI is caused by non - insulin substances such as IGF - 2 ICT: islet - cell tumor. NICT: non - islet cell tumor. SOC: standard of care. @2026 Rezolute, Inc. All Rights Reserved.

Real - world Patient Benefit in Expanded Access Program of Ersodetug 26 • Multiple tumor HI patients with severe refractory hypoglycemia • Hospitalized and in life - threatening or hospice - bound condition • Required continuous high volume/concentration intravenous dextrose or nutritional infusion • Tumor - directed therapies (e.g., embolization, radio therapy, chemotherapy) deferred because of hypoglycemia • Physician - requested use of ersodetug • Administration of ersodetug resulted in: • Substantial hypoglycemia improvement with no significant side effects 1 • Discontinuation of intravenous dextrose • Discharge from in - patient to out - patient care • Ability to resume regular activities (e.g., driving, walking dog) • Resumption of tumor - directed therapies 1 Based on real - world patient benefit demonstrated in Expanded Access Program the US Food and Drug Administration (FDA) granted Or phan Drug Designation to ersodetug for the treatment of hypoglycemia due to tumor HI. Sources: n engl j med 389;8 Aug24,2023 - https://www.nejm.org/doi/full/10.1056/NEJMc2307576?query=TOC&cid=NEJM+eToc%2C+August+24%2C+2023+DM2279684_NEJM_Non_Subscriber &bi d=1754093795 @2026 Rezolute, Inc. All Rights Reserved.
Phase 3: The upLIFT Study 27 • Global, multi - center, single - arm, open - label registrational study • Patient population (n=~16) • Adult ICT and NICT patients with HI who have not achieved adequate hypoglycemia control with SOC therapies • Primary endpoint: number of participants achieving ≥50% reduction from baseline IV glucose requirements (glucose infusion rate; GIR) • Additional endpoints include number of participants and time to discontinuation of GIR, time to discharge from the hospital, extent of hypoglycemia events and hypoglycemia time in the outpatient setting by self - monitored blood glucose and continuous glucose monitor, respectively, and patient reported quality of life • Treatment arms and dosing regimen • Once weekly administration over 8 - week pivotal treatment period • 9 mg/kg per week as add - on to SOC • All participants may receive ersodetug in long - term extension • Topline results expected second half of 2026 ICT: islet - cell tumor. NICT: non - islet cell tumor. SOC: standard of care. @2026 Rezolute, Inc. All Rights Reserved.

28 @2026 Rezolute, Inc. All Rights Reserved. Malignant insulinoma patients identified in claims (includes two or more C25.4 or E31.21 + ) ~ 40% patients refractory to surgery and medical management including DZ Initial commercial effort: refractory patient population at nationally recognized cancer institutes or academic centers 1,500 3,000 1,200 750 The ICD - 10 code C25.4 is for malignant neoplasm of the endocrine pancreas, which refers to cancer of the endocrine pancreas. The above analysis shows the unique patient count based on claims data from Forian and Veeva Compass; +The ICD - 10 code E31.21 is for multiple endocrine neoplasia [MEN] type I, also known as Wermer's syndrome. Included in the above analysis are MEN1 patients with hypoglycemia and treated for hypoglycemia; DZ = Diazoxide; * 60% of these patients respond to DZ ( https://www.ncbi.nlm.nih.gov/books/NBK544299/ ). Estimated treatment duration for ~750 patients is 2 years • 5 - year survival rate in this population is between ~24% to 67% • Entire refractory population = significant market expansion opportunity ~1,500 Initially Addressable Malignant Insulinoma Patients in U.S.

29 @2026 Rezolute, Inc. All Rights Reserved. * Analysis identified patients in the Forian and Veeva Compass claims database that matched phase 3 tumor HI clinical inclusion/exclusion criteria. Severe NICTH patients identified in claims* (Tumor Diagnosis + Hypoglycemia + Steroids + Hospitalization) ~40% patients refractory to SOC (tumor - directed and/or steroids) and requiring hospital stays + IV glucose* Initial commercial effort: refractory patient population at nationally recognized cancer institutes or academic centers 6,000 2,400 1,500 Estimated treatment duration of 1 year • 5 - year survival rates from 8% to 39% + • Entire refractory population = significant market expansion opportunity 1,500 ~1,500 Initially Addressable NICTH Patients in U.S.

Combined Commercial Opportunity

31 • Each vial is 80 mg/mL • Congenital HI maintenance dose: 10 mg/kg • Pediatric patient average weight: ~24 kg • Patients will use 3 vials per infusion • 39 vials per year per patient assuming infusion every four weeks • Tumor HI maintenance dose: 9 mg/kg • Adult patient average weight: ~80 kg • Patients will use 9 vials per infusion • 117 vials per year per patient assuming infusion every four weeks Tumor HI patients require ~3X more vials compared to congenital HI patients Weight - based Dosing Applies to Both Indications @2026 Rezolute, Inc. All Rights Reserved.

32 • Congenital HI Market • Pediatric ultra - rare disease pricing • Lead indication establishes clinical effectiveness and payer access pathway for ersodetug in HI • Addressable market of ~1,500 pediatric patients • Tumor HI Market • Malignant Insulinoma • Immediate opportunity with high awareness and concentration of patients among national cancer institutes • Addressable market of ~1,500 patients • NICTH • Nascent market with low disease awareness and underdiagnosis • Addressable market of ~1,500 patients • High prescriber overlap between the two indications among adult endocrinologists Tumor HI weight - based pricing at ~3X congenital HI represents significant revenue opportunity Initial Combined U.S. Market Opportunity: 4,500 Patients @2026 Rezolute, Inc. All Rights Reserved.

A Rare Disease Company Treating Hyperinsulinism 33 Well - capitalized for execution – $152 million in cash with runway to mid - 2027 Total $1B+ global market opportunity with additional upside through expansion RZ358 ( ersodetug ) is an antibody designed to treat hypoglycemia caused by all forms of hyperinsulinism (HI) Mission - driven to improve outcomes for individuals with severe hypoglycemia caused by hyperinsulinism (HI) Compelling evidence that ersodetug is active against hypoglycemia in patients under the Company’s Expanded Access Program @2026 Rezolute, Inc. All Rights Reserved.

Rezolutebio.com