UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934
Date of Report (Date of earliest event reported): October 10, 2025
ADAGIO MEDICAL HOLDINGS, INC.
(Exact name of registrant as specified in its charter)
| Delaware | 001-42199 | 99-1151466 |
| (State or other jurisdiction of incorporation) | (Commission File Number) | (I.R.S. Employer Identification No.) |
|
26051 Merit Circle, Suite 102 Laguna Hills, CA |
92653 | |
| (Address of principal executive offices) | (Zip Code) |
(949) 348-1188
(Registrant’s telephone number, including area code)
Not Applicable
(Former name or former address, if changed since last report)
Check the appropriate box below if the Form 8-K filing is intended to simultaneously satisfy the filing obligation of the registrant under any of the following provisions:
| ¨ | Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425) |
| ¨ | Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12) |
| ¨ | Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)) |
| ¨ | Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section 12(b) of the Act:
| Title of each class |
Trading Symbol(s) |
Name of each exchange on which registered |
| Common Stock, par value $0.0001 per share | ADGM | The Nasdaq Stock Market LLC |
Indicate by check mark whether the registrant is an emerging growth company as defined in Rule 405 of the Securities Act of 1933 or Rule 12b-2 of the Securities Exchange Act of 1934.
Emerging growth company x
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Item 8.01. Other Events.
Press Release
On October 10, 2025, Adagio Medical Holdings, Inc. (the “Company”) issued a press release announcing preliminary acute (within 7 days) safety and efficacy results from the Company’s FULCRUM-VT Study evaluating its Ultralow Temperature Cryoablation (ULTC) technology for the treatment of Sustained Monomorphic Ventricular Tachycardia (SMVT). The data was presented at the 20th Annual International Symposium on Ventricular Arrhythmias held in Philadelphia on October 10, 2025.
A copy of the press release is attached as Exhibit 99.1 to this Current Report on Form 8-K and is incorporated herein by reference.
Study Update Presentation
On October 10, 2025, the Company also made available a presentation to be used to discuss the preliminary acute (within 7 days) safety and efficacy results from the Company’s FULCRUM-VT Study. A copy of the presentation is attached as Exhibit 99.2 to this Current Report on Form 8-K and is incorporated herein by reference.
Item 9.01. Financial Statements and Exhibits.
(d) Exhibits.
| Exhibit No. | Description | |
| 99.1 | Press Release, dated October 10, 2025 | |
| 99.2 | Late Breaking Clinical Trials Presentation, dated October 10, 2025 | |
| 104 | Cover Page Interactive Data File (embedded within the Inline XBRL document) |
SIGNATURE
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
Dated: October 10, 2025
| Adagio Medical Holdings, Inc. | ||
| By: | /s/ Todd Usen | |
| Name: | Todd Usen | |
| Title: | Chief Executive Officer | |
Exhibit 99.1
Adagio Medical Unveils Preliminary Acute Results from FULCRUM-VT U.S. Pivotal Study in Late Breaking Session at VT Symposium
97% Acute Effectiveness and Favorable Safety Results from Proprietary ULTC for Ventricular Tachycardia
LAGUNA HILLS, CA, October 10, 2025 – Adagio Medical Holdings, Inc. (Nasdaq: ADGM) (“Adagio” or “the Company”), a leading innovator in catheter ablation technologies for the treatment of cardiac arrhythmias, today announced preliminary acute (within 7 days) safety and efficacy results from the Adagio’s FULCRUM-VT Study evaluating Ultralow Temperature Cryoablation (“ULTC”) for the treatment of Sustained Monomorphic Ventricular Tachycardia (“SMVT”) in patients with both ischemic and nonischemic cardiomyopathy. The data are being presented by Travis Richardson, MD, Assistant Professor of Medicine, Clinical Cardiac Electrophysiology, Vanderbilt University Medical Center, in a Late Breaking Clinical Trials Session at the 20th Annual International Symposium on Ventricular Arrhythmias being held in Philadelphia on October 10, 2025.
A total of 207 patients underwent ventricular tachycardia (“VT”) ablation using Adagio’s ULTC system at 19 sites in the United States and Canada. The study included patients with both ischemic (“ICM”) and non-ischemic (“NICM”) cardiomyopathies (LVEF=35+/-10%, 33% NICM, 75% with congestive heart failure). Mean procedure duration was 206+/- 68 minutes and acute clinical success, defined as non-inducibility of target ventricular arrhythmias, was 97.4%, with all clinically-relevant ventricular tachycardias eliminated in 96.7% of patients tested by post-ablation programmed electrical stimulation. Key safety findings included a 2.5% rate of major adverse events including four (1.9%) peri-procedural deaths, of which one (0.5%) was adjudicated by an independent clinical events committee as definitely related to the investigational device.
A presentation with additional details and accompanying figures are available on a Current Report on Form 8-K, which is being filed concurrently with this press release and available on the SEC’s website at www.sec.gov.
“The patient profile in FULCRUM-VT is representative of what we see in real-world practice. The ability of Adagio’s ULTC system to produce deep, titratable endocardial lesions without irrigation and without concerns for catheter stability make it a promising tool for a broad patient population. These factors, along with the broad inclusion criteria for the study, fueled swift enrollment,” said Dr. Richardson. “FULCRUM-VT not only included patients with ischemic myopathy, but also a large number with nonischemic disease, whose VT is often more difficult to treat due to deep substrate. Despite this, the acute effectiveness across the study population was excellent. This, along with the favorable safety profile of the ULTC System, is encouraging. VT is a largely undertreated condition, partially because the available treatment tools make ablation procedures challenging, and I have hope that ULTC will help to change that. We look forward to the six-month primary efficacy endpoint results of the FULCRUM-VT trial, which the company currently plans to share at the Heart Rhythm 2026 conference.”
The FULCRUM-VT Study is a prospective, multi-center investigation of ULTC evaluating acute safety and effectiveness in patients with scar-related VT refractory to antiarrhythmic drug therapy and a left ventricular ejection fraction greater than 20%. Long-term outcomes as well as analysis of the effectiveness in different myocardial substrates will be reported in the future.
“We are pleased with the preliminary FULCRUM-VT acute data, which highlight the potential of Adagio’s proprietary ULTC technology to transform treatment for patients with ventricular tachycardia,” said Todd Usen, Chief Executive Officer of Adagio Medical. “On behalf of the entire Adagio Medical team, I want to thank all of the investigators, research coordinators and patients who have supported this study and whose commitment to serving this underserved population of patients will bring us one step closer to a purpose-built solution for VT. We thank the VT Symposium for this opportunity to share our results as part of a Late Breaking Session in Philadelphia.”
About Adagio Medical Holdings, Inc.
Adagio is a medical device company focused on developing and commercializing products for the treatment of cardiac arrhythmias utilizing its novel, proprietary, catheter-based Ultra-Low Temperature Cryoablation (ULTC) technology. ULTC is designed to create large, durable lesions extending through the depth of both diseased and healthy cardiac tissue. The Company is currently focused on the treatment of ventricular tachycardia (VT) with its purpose-built vCLAS™ Cryoablation System, which is CE Marked and is currently under evaluation in the Company’s FULCRUM-VT U.S. IDE Pivotal Study.
About FULCRUM VT
FULCRUM-VT (Feasibility of Ultra-Low Temperature Cryoablation in Recurring Monomorphic Ventricular Tachycardia) is a prospective, multi-center, open-label, single-arm study, enrolling 206 patients with structural heart disease of both ischemic and non-ischemic cardiomyopathy, indicated for catheter ablation of drug refractory VT in accordance with current treatment guidelines. The results of the study will be used to apply for FDA premarket approval (PMA) for Adagio’s vCLAS™ Cryoablation System, potentially leading to the broadest industry indication for purely endocardial ablation of scar-mediated VT.
Adagio’s vCLAS™ Cryoablation System is commercially available for the treatment of monomorphic ventricular tachycardia in Europe and select other geographies but is limited to investigational use in the United States.
Forward-Looking Statements
This press release contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. Words such as “anticipates,” “believes,” “expects,” “intends,” “projects,” “plans,” and “future” or similar expressions are intended to identify forward-looking statements. Forward-looking statements include statements concerning: the reproducibility of any favorable results initially seen in Adagio’s preliminary FULCRUM-VT acute data; the ability of Adagio’s proprietary ULTC system to become a tool for a broad patient population; Adagio’s research, development and regulatory plans for its product candidates; and the ability of Adagio’s proprietary ULTC technology to transform treatment for patients with VT. Forward-looking statements are based on management’s current expectations and are subject to various risks and uncertainties that could cause actual results to differ materially and adversely from those expressed or implied by such forward-looking statements. Accordingly, these forward-looking statements do not constitute guarantees of future performance, and you are cautioned not to place undue reliance on these forward-looking statements. Risks regarding Adagio’s business are described in detail in Adagio’s Securities and Exchange Commission (“SEC”) filings, including in its Annual Report on Form 10-K for the full-year ended December 31, 2024 and Quarterly Report on Form 10-Q for the quarter ended June 30, 2025, which are available on the SEC’s website at www.sec.gov. Additional information will be made available in other filings that Adagio makes from time to time with the SEC. These forward-looking statements speak only as of the date hereof, and Adagio disclaims any obligation to update these statements except as may be required by law.
Contact
Debbie Kaster
Chief Financial Officer and Chief Business Officer
dkaster@adagiomedical.com
|
Ultralow Temperature Cryoablation of Ventricular Tachycardia: Interim Analysis of Acute Outcomes of the FULCRUM-VT Trial Travis D. Richardson, MD Assistant Professor of Medicine Clinical Cardiac Electrophysiology on behalf of FULCRUM-VT Investigators |
|
DISCLOSURES • Consultant/honoraria for Medtronic Inc, Johnson & Johnson, Boston Scientific, and Abbott. |
|
DISCLAIMER This presentation describes a preliminary assessment;subject to study database lock, source data monitoring, and final analysis. Final data will be finalized for US FDA submission to support a pre-market approval (PMA) of this Investigational Device. US FDA has not reviewed these data. |
|
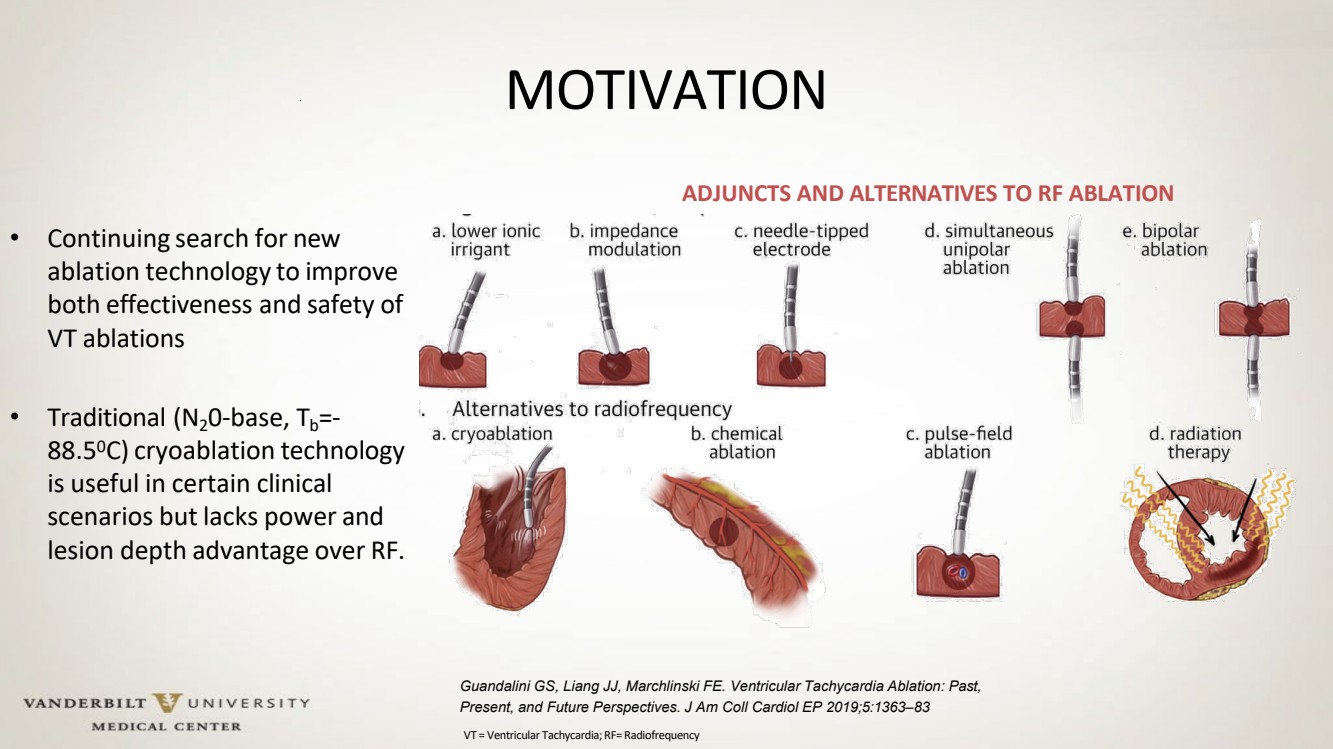
MOTIVATION • Continuing search for new ablation technology to improve both effectiveness and safety of VT ablations • Traditional (N20-base, Tb=- 88.50C) cryoablation technology is useful in certain clinical scenarios but lacks power and lesion depth advantage over RF. Guandalini GS, Liang JJ, Marchlinski FE. Ventricular Tachycardia Ablation: Past, Present, and Future Perspectives. J Am Coll Cardiol EP 2019;5:1363–83 ADJUNCTS AND ALTERNATIVES TO RF ABLATION VT = Ventricular Tachycardia;RF= Radiofrequency |
|
ULTRA-LOW TEMPERATURE CRYOABLATION VanderbiltHeart.com OPERATING POINT NEAR-CRITICAL (NC)-N2: combination of pressure and temperature suppresses liquid-gas phase transition • Viscosity of a gas • Density and heat capacity of a liquid • “Vapor lock” – free flow OPERATING PRINCIPLE1 PHYSIOLOGY OF CRYOABLATION2,3,4,5,6 1Adopted with modifications from: Littrup P, Babkin A. Evolving Concepts: Near-Critical Cooling-Based Technologies. In: Cryoablation of Cardiac Arrhythmias. Elsevier Health Sciences 2011. 2 Erinjeri JP, Clark TWI.J Vasc Interv Radiol. 2010;21(8 Suppl): S187–S191 3 Baust JG, Bischof JC, et al. Prostate Cancer and Prostatic Disease (2015)18, 87–95 4 Choi J, Bischof J. Cryobiology 2017;78: 115-118 5 Petrova EV, Brecjt HP, et al. Phys. Med. Biol 2019;63(6):064002 6 Cox JL, Malaisrie SC, Churyla A, et al. Ann Thorac Surg 2021;112:354-62 ULTC TARGET |
|
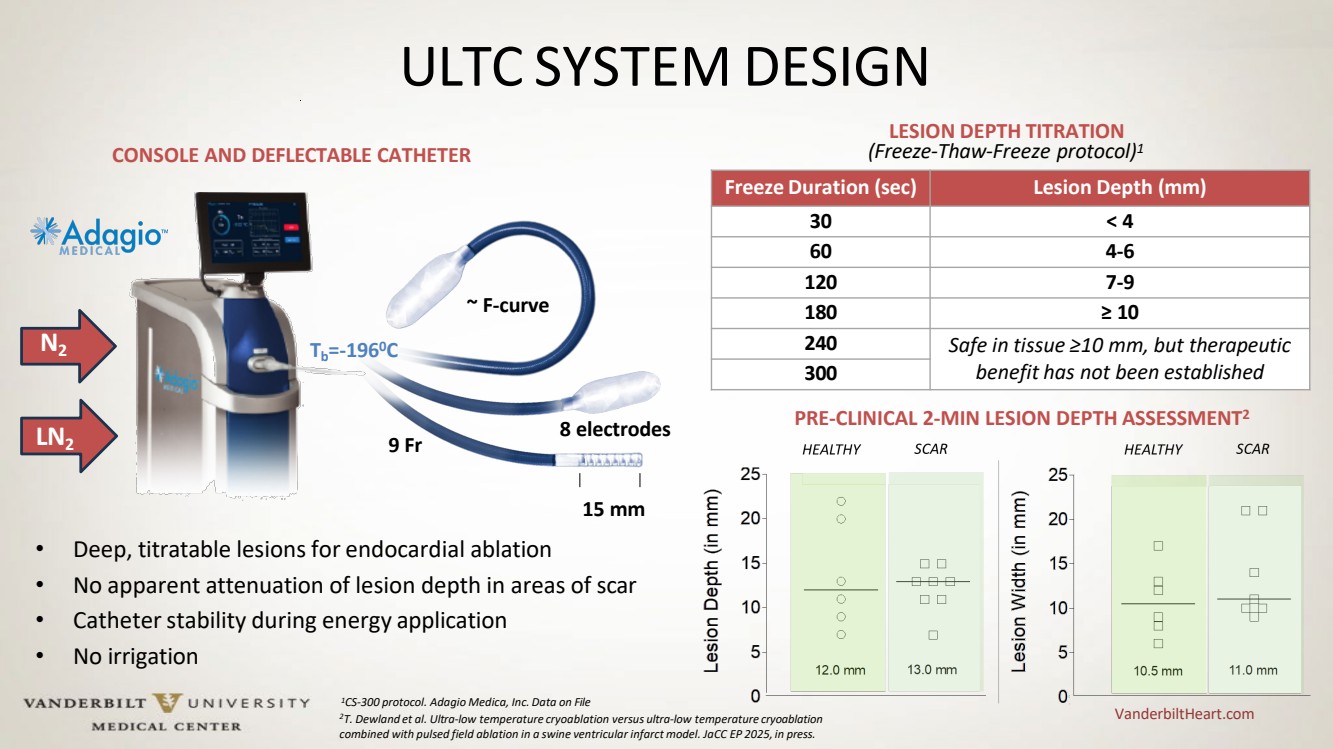
ULTC SYSTEM DESIGN VanderbiltHeart.com 15 mm • Deep, titratable lesions for endocardial ablation • No apparent attenuation of lesion depth in areas of scar • Catheterstability during energy application • No irrigation N2 LN2 Freeze Duration (sec) Lesion Depth (mm) 30 < 4 60 4-6 120 7-9 180 ≥ 10 240 Safe in tissue ≥10 mm, but therapeutic 300 benefit has not been established Tb=-1960C 9 Fr ~ F-curve 8 electrodes CONSOLE AND DEFLECTABLE CATHETER LESION DEPTH TITRATION (Freeze-Thaw-Freeze protocol)1 PRE-CLINICAL 2-MIN LESION DEPTH ASSESSMENT2 1CS-300 protocol. Adagio Medica, Inc. Data on File 2T. Dewland et al. Ultra-low temperature cryoablation versus ultra-low temperature cryoablation combined with pulsed field ablation in a swine ventricular infarct model. JaCC EP 2025, in press. |
|
PRIOR CLINICAL DATA: CRYOCURE-VT STUDY A. Verma et al. Cryocure-VT: the safety and effectiveness of ultra-low-temperature cryoablation of monomorphic ventricular VanderbiltHeart.com tachycardia in patients with ischaemic and non-ischaemic cardiomyopathies Europace 2024, MAE = Major Adverse Event LVEF= Left Ventricular Ejection Fraction |
|
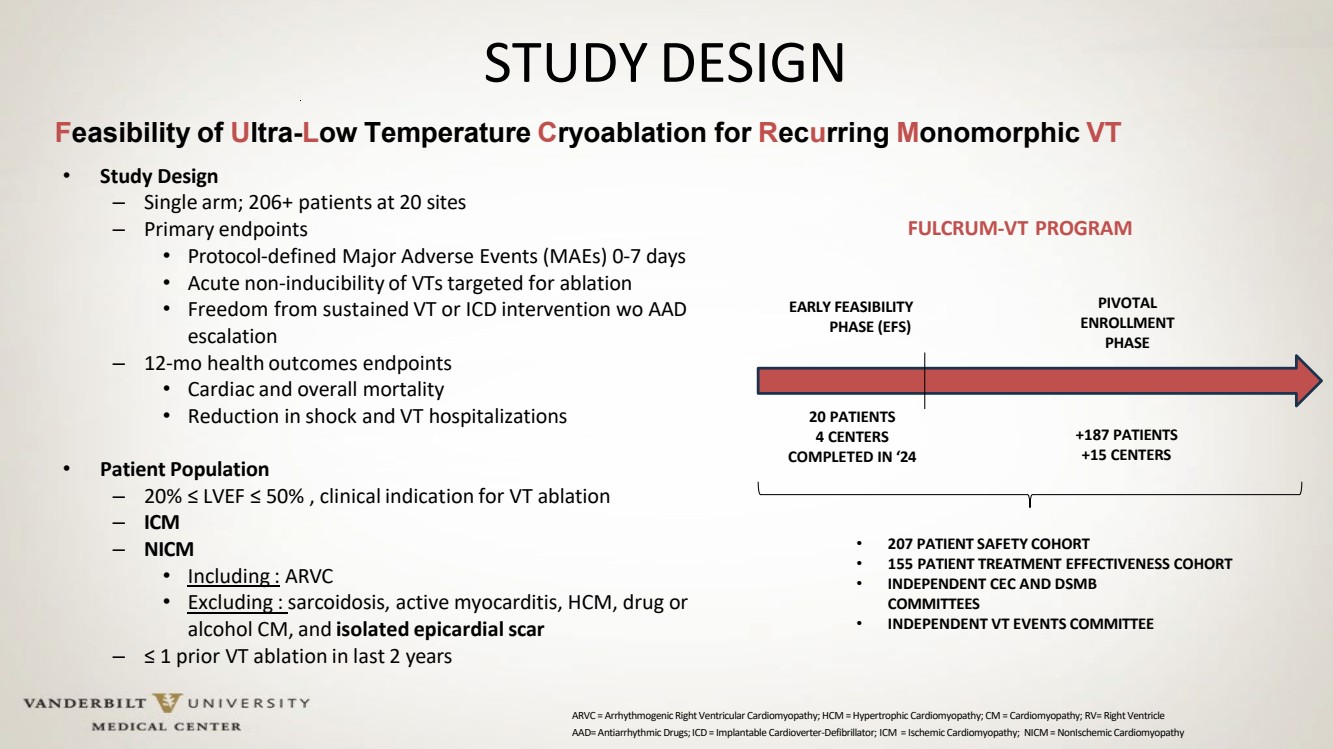
STUDY DESIGN • Protocol-defined Major Adverse Events (MAEs) 0-7 days • Acute non-inducibility of VTs targeted for ablation • Freedom from sustained VT or ICD intervention wo AAD escalation – 12-mo health outcomes endpoints • Cardiac and overall mortality • Reduction in shock and VT hospitalizations • Patient Population – 20% ≤ LVEF ≤ 50% , clinical indication for VT ablation – ICM – NICM • Including : ARVC • Excluding : sarcoidosis, active myocarditis, HCM, drug or alcohol CM, and isolated epicardialscar – ≤ 1 prior VT ablation in last 2 years EARLY FEASIBILITY PHASE (EFS) PIVOTAL ENROLLMENT PHASE 20 PATIENTS 4 CENTERS COMPLETED IN ‘24 +187 PATIENTS +15 CENTERS • 207 PATIENT SAFETY COHORT • 155 PATIENT TREATMENT EFFECTIVENESS COHORT • INDEPENDENT CEC AND DSMB COMMITTEES • INDEPENDENT VT EVENTS COMMITTEE Feasibility of Ultra-Low Temperature Cryoablation for Recurring Monomorphic VT • Study Design – Single arm; 206+ patients at 20 sites – Primary endpoints FULCRUM-VT PROGRAM AAD= Antiarrhythmic Drugs; ICD = Implantable Cardioverter-Defibrillator; ICM = Ischemic Cardiomyopathy; NICM = NonIschemic Cardiomyopathy ARVC = Arrhythmogenic Right Ventricular Cardiomyopathy; HCM = Hypertrophic Cardiomyopathy; CM = Cardiomyopathy; RV= Right Ventricle |
|
20 32 155 All patients Treatment Cohort Number of Patients 207 155 Age 68 ± 11 y.o. 69 ± 10 y.o. Male Sex 92.4% 95.5% BMI 30 ± 6 30 ± 6 Cardiomyopathy 93.6% 91.4% ICM 60.8% 61.8% NICM 27.5% 23.7% both ICM and NICM 5.4% 5.9% LVEF 35% ± 10% 35% ± 10% ≤ 30% 38.2% 36.6% 31-40% 33.3% 35.8% 41-50% 23.7% 24.6% >50% 4.8% 3.0% CAD 72.4% 74.3% Prior MI 55.7% 60.3% Diabetes Mellitus 37.8% 40.3% Congestive Heart Failure 74.9% 78.3% Hypertension 84.1% 83.9% Class I AADs 2.0% 2.1% Class III AADs 82.8% 82.0% Amiodarone 64.1% 64.4% PATIENT POPULATION PATIENT COHORT DETAILS EFS Cohort Roll-In Patients Treatment Cohort Roll-in patients (one per operator) are counted towards safety but not effectiveness endpoints. |
|
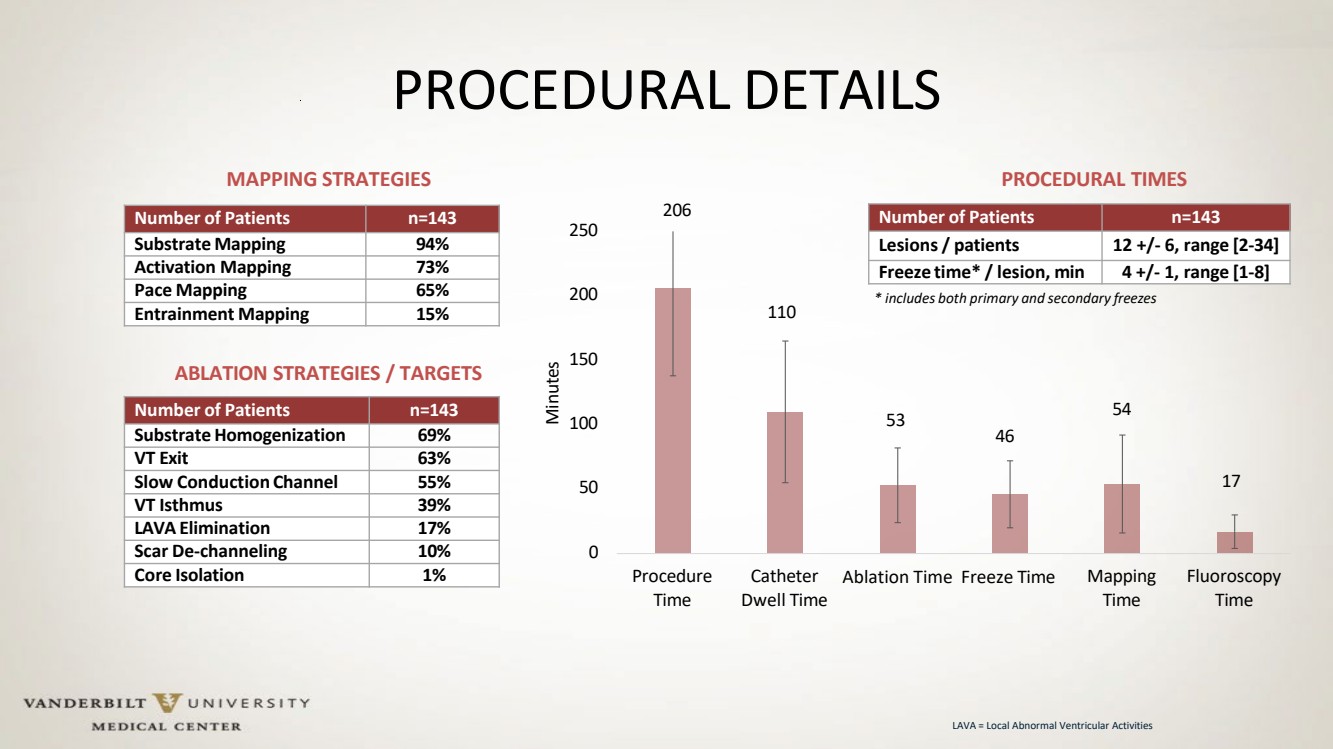
110 53 46 54 17 0 50 100 150 200 206 250 Procedure Time Catheter Dwell Time Ablation Time Freeze Time Mapping Time Fluoroscopy Time Minutes PROCEDURAL DETAILS Number of Patients n=143 Substrate Mapping 94% Activation Mapping 73% Pace Mapping 65% Entrainment Mapping 15% Number of Patients n=143 Substrate Homogenization 69% VT Exit 63% Slow Conduction Channel 55% VT Isthmus 39% LAVA Elimination 17% Scar De-channeling 10% Core Isolation 1% Number of Patients n=143 Lesions / patients 12 +/- 6, range [2-34] Freeze time* / lesion, min 4 +/- 1, range [1-8] MAPPING STRATEGIES ABLATION STRATEGIES / TARGETS PROCEDURAL TIMES * includes both primary and secondary freezes LAVA = Local Abnormal Ventricular Activities |
|
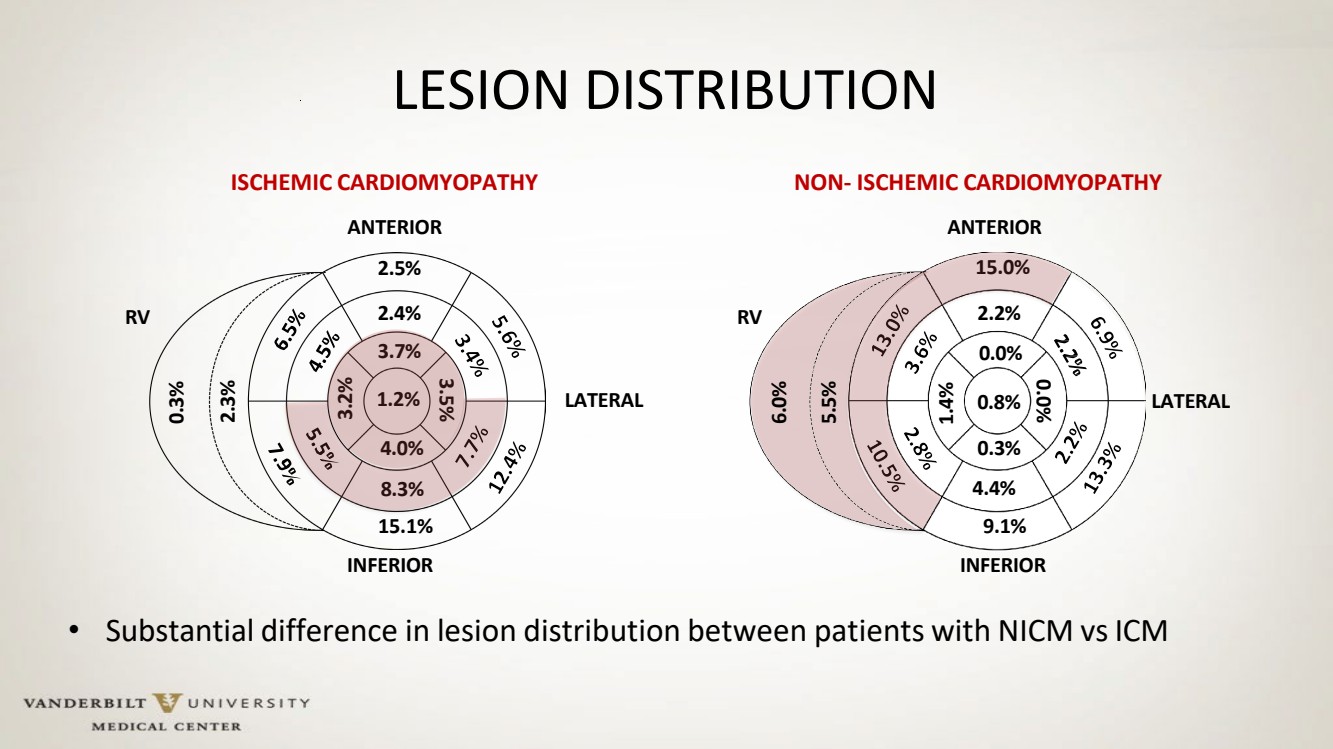
LESION DISTRIBUTION • Substantial difference in lesion distribution between patients with NICM vs ICM ISCHEMIC CARDIOMYOPATHY NON- ISCHEMIC CARDIOMYOPATHY RV RV ANTERIOR 2.5% LATERAL LATERAL ANTERIOR 15.0% 15.1% INFERIOR 9.1% INFERIOR 2.4% 3.7% 2.2% 0.0% 3.2% 1.4% 4.0% 8.3% 0.3% 4.4% 3.5% 0.0% 1.2% 0.8% 0.3% 2.3% 6.0% 5.5% |
|
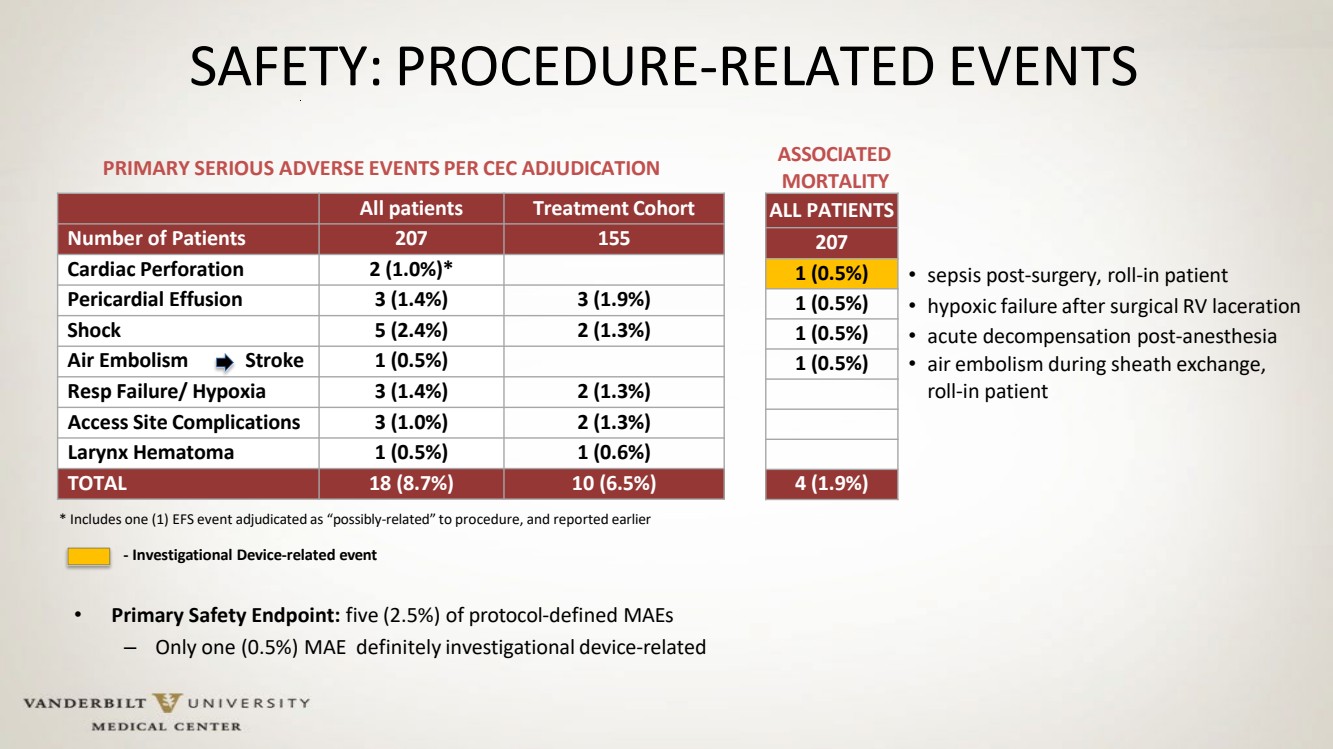
SAFETY: PROCEDURE-RELATED EVENTS All patients Treatment Cohort Number of Patients 207 155 Cardiac Perforation 2 (1.0%)* Pericardial Effusion 3 (1.4%) 3 (1.9%) Shock 5 (2.4%) 2 (1.3%) Air Embolism Stroke 1 (0.5%) Resp Failure/ Hypoxia 3 (1.4%) 2 (1.3%) Access Site Complications 3 (1.0%) 2 (1.3%) Larynx Hematoma 1 (0.5%) 1 (0.6%) TOTAL 18 (8.7%) 10 (6.5%) PRIMARY SERIOUS ADVERSE EVENTS PER CEC ADJUDICATION ALL PATIENTS 207 1 (0.5%) 1 (0.5%) 1 (0.5%) 1 (0.5%) 4 (1.9%) ASSOCIATED MORTALITY * Includes one (1) EFS event adjudicated as “possibly-related” to procedure, and reported earlier - Investigational Device-related event • Primary Safety Endpoint: five (2.5%) of protocol-defined MAEs – Only one (0.5%) MAE definitely investigational device-related • sepsis post-surgery, roll-in patient • hypoxic failure after surgical RV laceration • acute decompensation post-anesthesia • air embolism during sheath exchange, roll-in patient |
|
VT INDUCIBILITY AND ACUTE PROCEDURAL SUCCESS 154 patients 382 VTs 204 Clinical 135 Non-Clinical 43 Undetermined 201 Clinical 105 Non-Clinical 39 Undetermined 178 Clinical 93 Non-Clinical 28 Undetermined 298 Non-reinducible 8 Reinducible 39 No PES Done 5 Clinical 2 Non-Clinical 1 Undetermined 19 Clinical 10 Non-Clinical 10 Undetermined 97.4% Acute Success Number of Patients n=154 VTs per patient 2.8 % Clinical 53.4% % Hemodynamically Stable 34.6% Average CL (ms) 365 +/- 84 345 VTs Targeted for Ablation BASELINE INDUCIBILE VTs STATISTICS |
|
117 2 4 No VTs reinduced in post-ablation PES Non-clinical VTs after post-ablation PES Clinical VTs in post-ablation PES PATIENT-LEVEL DATA: 96.7% CLINICAL SUCCESS 154 patients 17 patients 137 patients 14 patients 117 patients 2 patients 4 patients No VT induction after pre-ablation PES Clinical VTs(5) reinduced Neither clinical nor non-clinical VTs reinduced No clinical VTs, but non-clinical VTs are reinduced Post-ablation PES not performed Post-ablation PES 95.1% 96.7% - Full Success - Clinical Success PES = Programmed Electrical Stimulation |
|
CONCLUSIONS • In large, multi-center cohort of patients with both ischemic and non-ischemic cardiomyopathies the ULTC system demonstrated very promising acute performance for ablation of VT associated with structural heart disease. – Favorable safety profile • Low rate of intra- and peri-procedural complications, consistent with underlying morbidity of the treated population • No signal of incremental risk associated with the specific technology/novel energy source – Excellent acute effectiveness • 97.4% elimination of targeted VTs • 96.7% patient-level clinical success (elimination of clinical VTs) • 6-mo outcome data should be available by HRS’ 26 • Next-generation catheter design (8.5Fr, D/F, more flexible, colder and shorter ablations) is in the works |