UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d)
of the Securities Exchange Act of 1934
Date of Report (Date of earliest event reported): March 5, 2024
Apogee Therapeutics, Inc.
(Exact Name of Registrant as Specified in Its Charter)
| Delaware | 001-41740 | 88-0588063 |
| (State of Incorporation or Organization) |
(Commission File Number) | (I.R.S. Employer Identification No.) |
221 Crescent Street, Building 17, Suite 102b,
Waltham, MA, 02453
(Address of Principal Executive Offices, including Zip Code)
(650) 394-5230
(Registrant’s telephone number, including area code)
Check the appropriate box below if the Form 8-K filing is intended to simultaneously satisfy the filing obligation of the registrant under any of the following provisions:
| ¨ | Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425) |
| ¨ | Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12) |
| ¨ | Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)) |
| ¨ | Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section 12(b) of the Act:
| Title of each class | Trading Symbol(s) |
Name of each exchange on which registered |
||
| Common Stock, par value $0.00001 per share | APGE | The Nasdaq Global Market |
Indicate by check mark whether the registrant is an emerging growth company as defined in Rule 405 of the Securities Act of 1933 (§230.405 of this chapter) or Rule 12b-2 of the Securities Exchange Act of 1934 (§240.12b-2 of this chapter).
Emerging growth company x
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ¨
| Item 7.01 | Regulation FD Disclosure. |
On March 5, 2024, Apogee Therapeutics, Inc. (the “Company”) made available a presentation regarding its initial Phase 1 data from its first-in-human study of APG777 on the Company’s website.
A copy of the data presentation is furnished as Exhibit 99.1 to this Current Report on Form 8-K and is incorporated by reference herein. The exhibit furnished under Item 7.01 of this Current Report on Form 8-K shall not be deemed to be “filed” for purposes of Section 18 of the Securities Exchange Act of 1934, as amended (the “Exchange Act”), or otherwise subject to the liabilities of that section, nor shall it be deemed incorporated by reference in any filing under the Exchange Act or the Securities Act of 1933, as amended, regardless of any general incorporation language in such filing.
| Item 9.01 | Financial Statements and Exhibits. |
(d) Exhibits.
EXHIBIT INDEX
| Exhibit No. |
Description | |
| 99.1 | Data Presentation, dated March 2024 | |
| 104 | Cover Page Interactive Data File (embedded within the Inline XBRL document). | |
SIGNATURES
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
| Apogee Therapeutics, Inc. | ||
| Date: March 5, 2024 | By: | /s/ Michael Henderson, M.D. |
| Michael Henderson, M.D. | ||
| Chief Executive Officer | ||
|
APG777 PHASE 1 DATA March 2024 |
|
© Apogee Therapeutics, Inc. 2 Disclaimers and Forward-looking statements This presentation contains certain "forward-looking statements" within the meaning of applicable securities laws. Other than statements of historical facts, all statements included in this presentation are forward-looking statements, including statements about our plans, objectives, goals, strategies and future events, the efficacy, safety, tolerability, PK and PD profile of APG777, the potential dosing regimen of APG777, the potential superiority of APG777 compared to current therapies, our expectations regarding plans for our current and future product candidates and programs, our plans for our current and future clinical trials, our plans for clinical trial design, the anticipated timing of the initiation of and results from our clinical trials, the potential clinical benefit and half-life of APG777, APG808, APG990, APG222 and any other potential programs, our expected timing for future pipeline updates and estimates of market size. In some cases, you can identify forward-looking statements by terms such as “anticipate,” “believe,” “can,” “could,” “design,” “estimate,” “expect,” “intend,” “likely,” “may,” “might,” “plan,” “potential,” “predict,” “suggest,” “target,” “will,” “would,” or the negative of these terms, and similar expressions intended to identify forward-looking statements. The forward-looking statements are based on our beliefs, assumptions and expectations of future performance, taking into account the information currently available to us. These statements are only predictions based upon our current expectations and projections about future events. Forward-looking statements are subject to known and unknown risks, uncertainties and other factors that may cause our actual results, level of activity, performance or achievements to be materially different from those expressed or implied by such forward-looking statements, including those risks described in “Risk Factors” and “Management’s Discussion and Analysis of Financial Condition and Results of Operations” in our Annual Report on Form 10-K for the year ended December 31, 2023, filed with the SEC on March 5, 2024, and subsequent disclosure documents we may file with the U.S. Securities and Exchange Commission. Although we have attempted to identify important factors that could cause actual results to differ materially from those contained in forward-looking statements, there may be other factors that cause results not to be as anticipated, estimated or intended. This presentation concerns drug candidates that are under clinical investigation, and which have not yet been approved by the U.S. Food and Drug Administration. These are currently limited by federal law to investigational use, and no representation is made as to their safety or effectiveness for the purposes for which they are being investigated. The assumptions used in the preparation of this presentation, although considered reasonable by us at the time of preparation, may prove to be incorrect. You are cautioned that the information is based on assumptions as to many factors and that actual results may vary from the results projected and such variations may be material. Accordingly, you should not place undue reliance on any forward-looking statements contained herein or rely on them as predictions of future events. All forward-looking statements in this presentation apply only as of the date made and are expressly qualified by the cautionary statements included in this presentation. We do not undertake to update any forward-looking statements, except in accordance with applicable securities laws. The trademarks, trade names and service marks appearing in this presentation are the property of their respective owners. Certain information contained in this presentation relate to or are based on studies, publications and other data obtained from third-party sources as well as our own internal estimates and research. While we believe these third-party sources to be reliable as of the date of this presentation, it has not independently verified, and makes no representation as to the adequacy, fairness, accuracy or completeness of, any information obtained from third-party sources. |
|
© Apogee Therapeutics, Inc. 3 Introduction & Executive Summary Michael Henderson, MD Chief Executive Officer APG777 Phase 1 Interim Results Carl Dambkowski, MD Chief Medical Officer APG777 Phase 2 Trial in Atopic Dermatitis Kristine Nograles, MD SVP, Clinical Development Building a Leading I&I Company Michael Henderson, MD Chief Executive Officer Analyst Q&A Michael Henderson, MD, CEO Carl Dambkowski, MD, CMO Jane Pritchett Henderson, CFO Agenda |
|
© Apogee Therapeutics, Inc. 4 People living with these diseases deserve the best possible treatment Significant unmet need continues Apogee plans to reshape the current standard of care for inflammatory and immune diseases Focus on developing differentiated biologics with known biologic drivers Refusing to stop at “good enough” Near term priority on treatments for atopic dermatitis (AD), asthma and chronic obstructive pulmonary disease (COPD) |
|
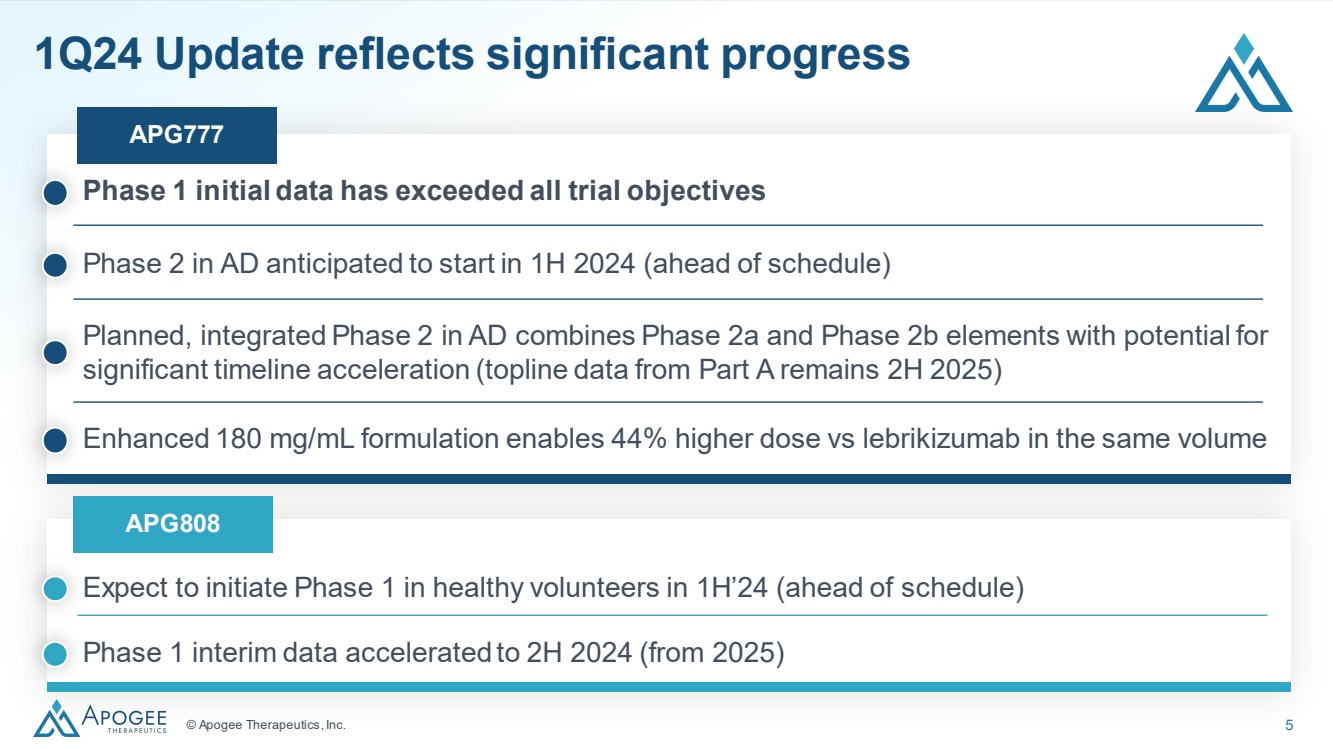
© Apogee Therapeutics, Inc. 5 1Q24 Update reflects significant progress Expect to initiate Phase 1 in healthy volunteers in 1H’24 (ahead of schedule) APG777 APG808 Phase 1 interim data accelerated to 2H 2024 (from 2025) Phase 1 initial data has exceeded all trial objectives Planned, integrated Phase 2 in AD combines Phase 2a and Phase 2b elements with potential for significant timeline acceleration (topline data from Part A remains 2H 2025) Phase 2 in AD anticipated to start in 1H 2024 (ahead of schedule) Enhanced 180 mg/mL formulation enables 44% higher dose vs lebrikizumab in the same volume |
|
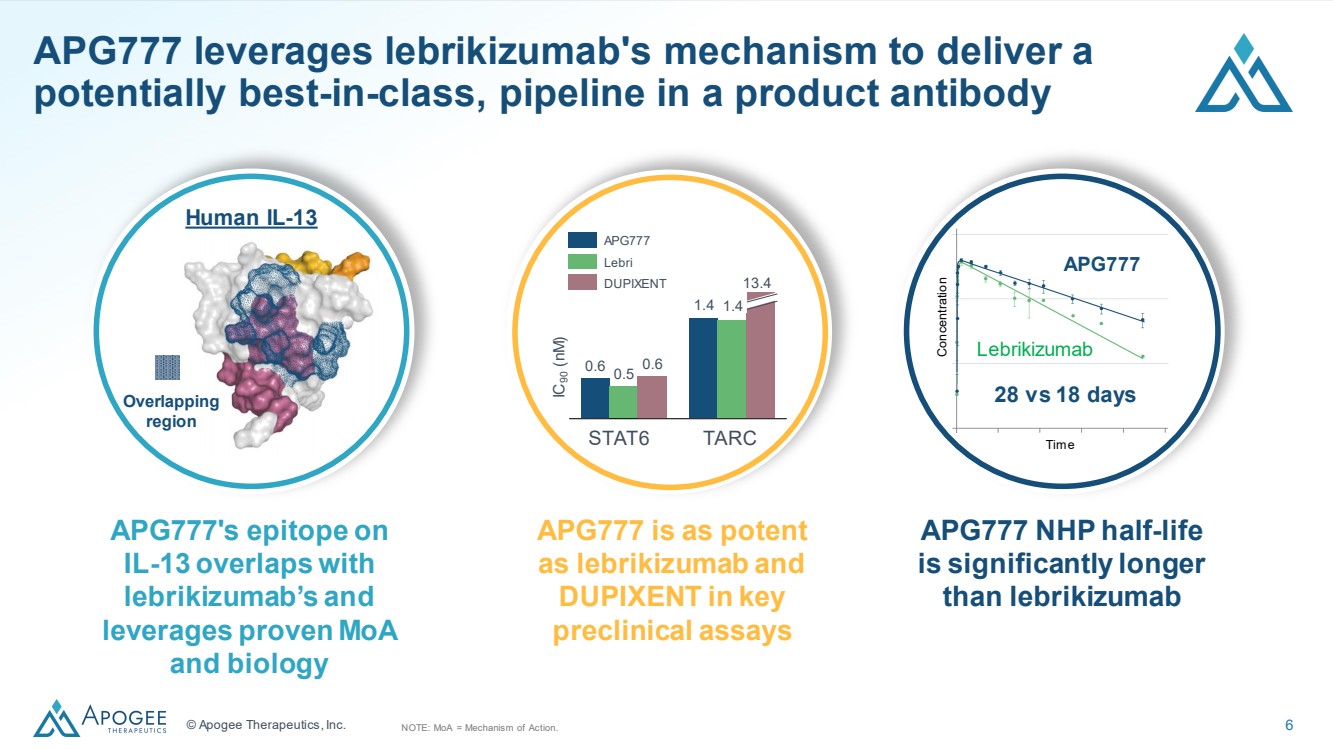
© Apogee Therapeutics, Inc. 6 APG777 leverages lebrikizumab's mechanism to deliver a potentially best-in-class, pipeline in a product antibody 0.6 1.4 0.5 0.6 STAT6 TARC 1.4 13.4 IC90 (nM) APG777 Concentration Lebrikizumab Time 28 vs 18 days APG777 Lebri DUPIXENT Overlapping region Human IL-13 APG777's epitope on IL-13 overlaps with lebrikizumab’s and leverages proven MoA and biology APG777 is as potent as lebrikizumab and DUPIXENT in key preclinical assays APG777 NHP half-life is significantly longer than lebrikizumab NOTE: MoA = Mechanism of Action. |
|
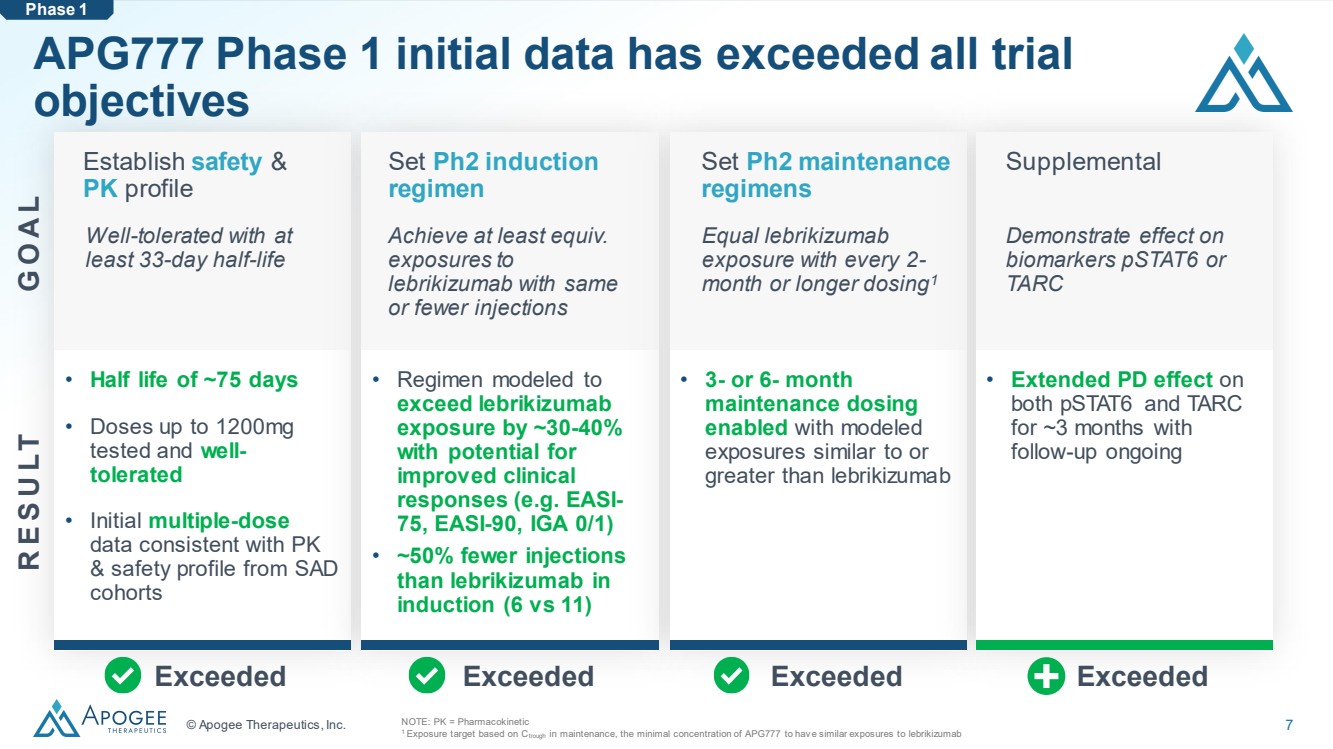
© Apogee Therapeutics, Inc. 7 APG777 Phase 1 initial data has exceeded all trial objectives NOTE: PK = Pharmacokinetic 1 Exposure target based on Ctrough in maintenance, the minimal concentration of APG777 to hav e similar exposures to lebrikizumab Phase 1 Establish safety & PK profile Well-tolerated with at least 33-day half-life Set Ph2 induction regimen Achieve at least equiv. exposures to lebrikizumab with same or fewer injections Set Ph2 maintenance regimens Equal lebrikizumab exposure with every 2- month or longer dosing1 Supplemental Demonstrate effect on biomarkers pSTAT6 or TARC Exceeded Exceeded Exceeded Exceeded • Half life of ~75 days • Doses up to 1200mg tested and well-tolerated • Initial multiple-dose data consistent with PK & safety profile from SAD cohorts • Regimen modeled to exceed lebrikizumab exposure by ~30-40% with potential for improved clinical responses (e.g. EASI-75, EASI-90, IGA 0/1) • ~50% fewer injections than lebrikizumab in induction (6 vs 11) • 3- or 6- month maintenance dosing enabled with modeled exposures similar to or greater than lebrikizumab • Extended PD effect on both pSTAT6 and TARC for ~3 months with follow-up ongoing G O A L R E S U LT |
|
APG777 Phase 1 in Healthy Volunteers |
|
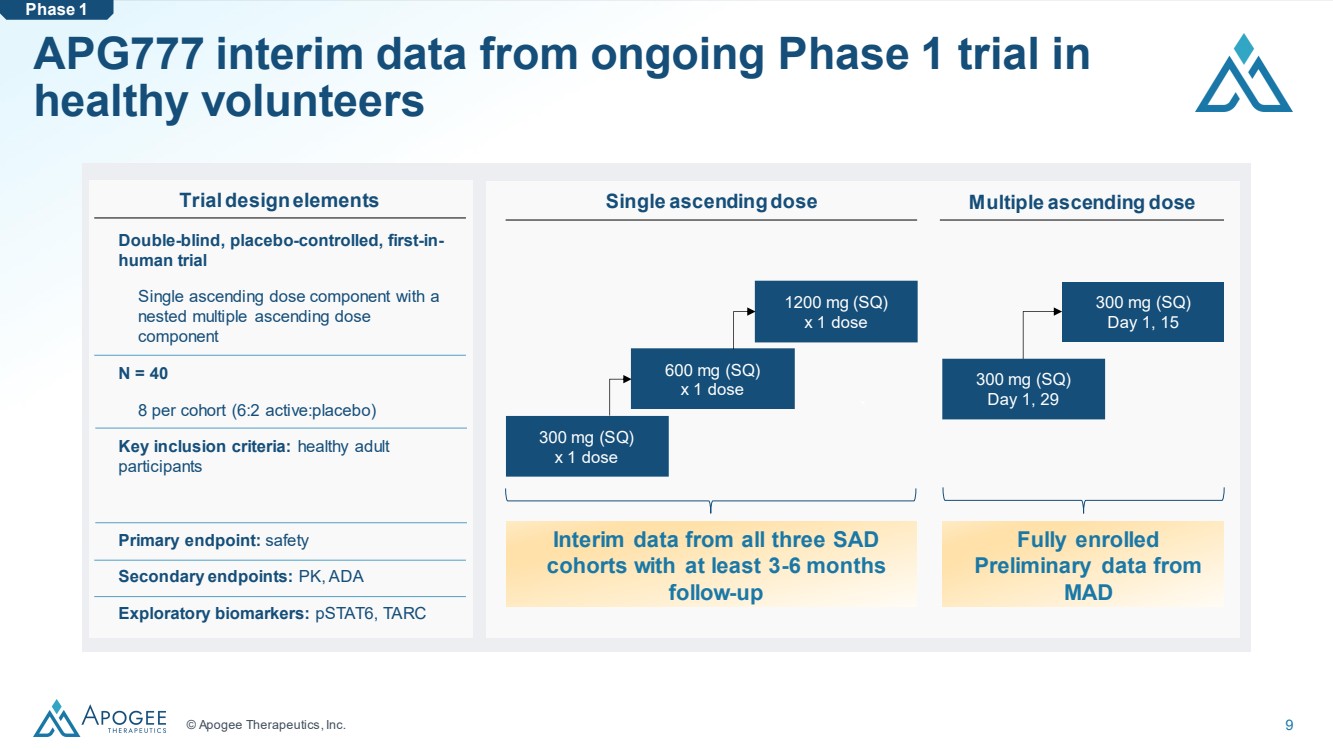
© Apogee Therapeutics, Inc. 9 APG777 interim data from ongoing Phase 1 trial in healthy volunteers ` ` Single ascendingdose Multiple ascending dose Double-blind, placebo-controlled, first-in-human trial Single ascending dose component with a nested multiple ascending dose component N = 40 8 per cohort (6:2 active:placebo) Key inclusion criteria: healthy adult participants Primary endpoint: safety Secondary endpoints: PK, ADA Exploratory biomarkers: pSTAT6, TARC 300 mg (SQ) x 1 dose 600 mg (SQ) x 1 dose 1200 mg (SQ) x 1 dose 300 mg (SQ) Day 1, 15 Trial design elements 300 mg (SQ) Day 1, 29 Interim data from all three SAD cohorts with at least 3-6 months follow-up Fully enrolled Preliminary data from MAD Phase 1 |
|
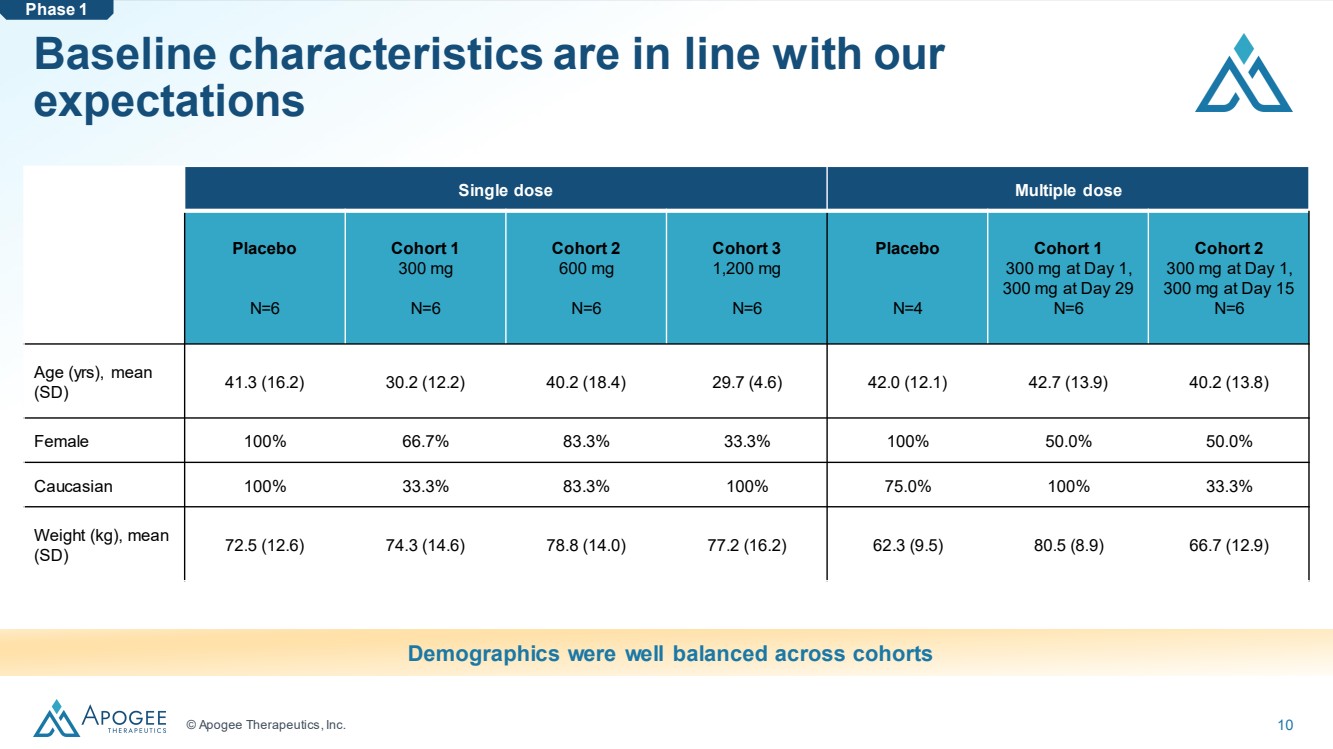
© Apogee Therapeutics, Inc. 10 Baseline characteristics are in line with our expectations Single dose Multiple dose Placebo N=6 Cohort 1 300 mg N=6 Cohort 2 600 mg N=6 Cohort 3 1,200 mg N=6 Placebo N=4 Cohort 1 300 mg at Day 1, 300 mg at Day 29 N=6 Cohort 2 300 mg at Day 1, 300 mg at Day 15 N=6 Age (yrs), mean (SD) 41.3 (16.2) 30.2 (12.2) 40.2 (18.4) 29.7 (4.6) 42.0 (12.1) 42.7 (13.9) 40.2 (13.8) Female 100% 66.7% 83.3% 33.3% 100% 50.0% 50.0% Caucasian 100% 33.3% 83.3% 100% 75.0% 100% 33.3% Weight (kg), mean (SD) 72.5 (12.6) 74.3 (14.6) 78.8 (14.0) 77.2 (16.2) 62.3 (9.5) 80.5 (8.9) 66.7 (12.9) Demographics were well balanced across cohorts Phase 1 |
|
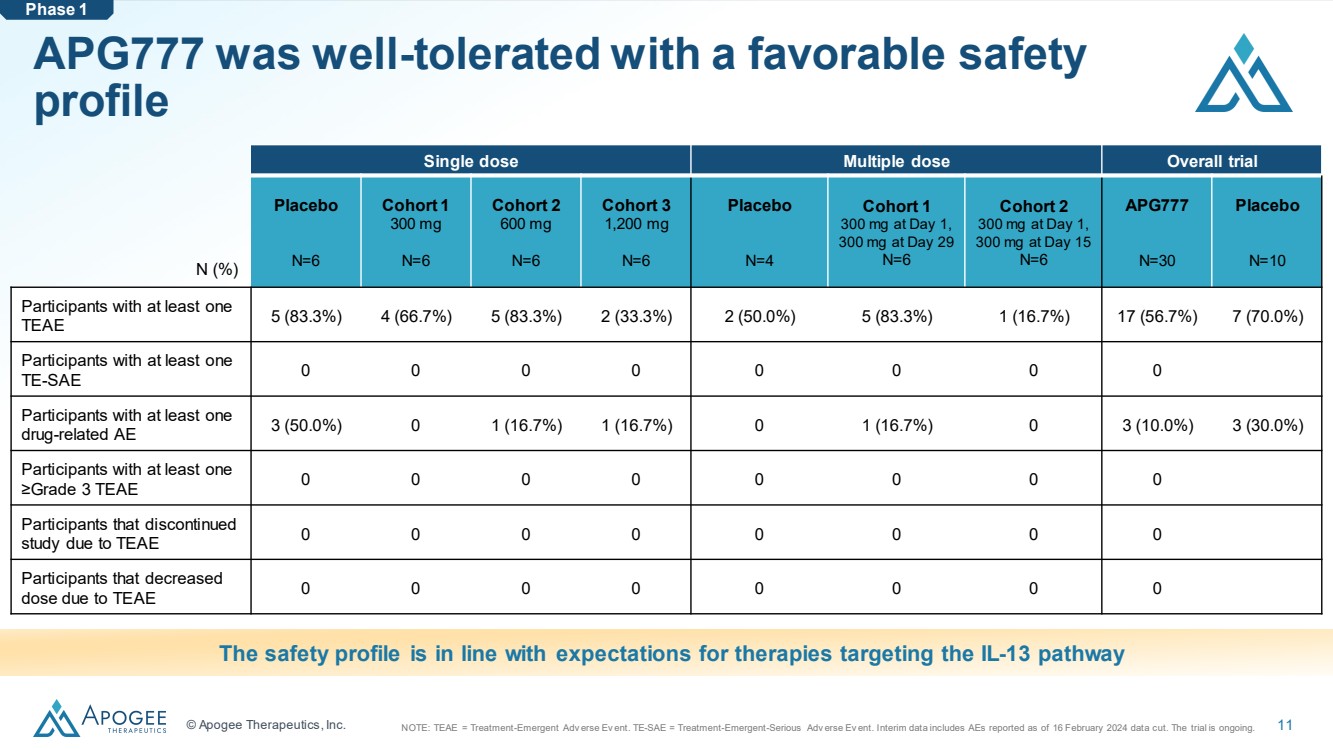
© Apogee Therapeutics, Inc. 11 APG777 was well-tolerated with a favorable safety profile Single dose Multiple dose Overall trial Placebo N=6 Cohort 1 300 mg N=6 Cohort 2 600 mg N=6 Cohort 3 1,200 mg N=6 Placebo N=4 Cohort 1 300 mg at Day 1, 300 mg at Day 29 N=6 Cohort 2 300 mg at Day 1, 300 mg at Day 15 N=6 APG777 N=30 Placebo N=10 Participants with at least one TEAE 5 (83.3%) 4 (66.7%) 5 (83.3%) 2 (33.3%) 2 (50.0%) 5 (83.3%) 1 (16.7%) 17 (56.7%) 7 (70.0%) Participants with at least one TE-SAE 0 0 0 0 0 0 0 0 Participants with at least one drug-related AE 3 (50.0%) 0 1 (16.7%) 1 (16.7%) 0 1 (16.7%) 0 3 (10.0%) 3 (30.0%) Participants with at least one ≥Grade 3 TEAE 0 0 0 0 0 0 0 0 Participants that discontinued study due to TEAE 0 0 0 0 0 0 0 0 Participants that decreased dose due to TEAE 0 0 0 0 0 0 0 0 The safety profile is in line with expectations for therapies targeting the IL-13 pathway N (%) Phase 1 NOTE: TEAE = Treatment-Emergent Adv erse Ev ent. TE-SAE = Treatment-Emergent-Serious Adv erse Ev ent. Interim data includes AEs reported as of 16 February 2024 data cut. The trial is ongoing. |
|
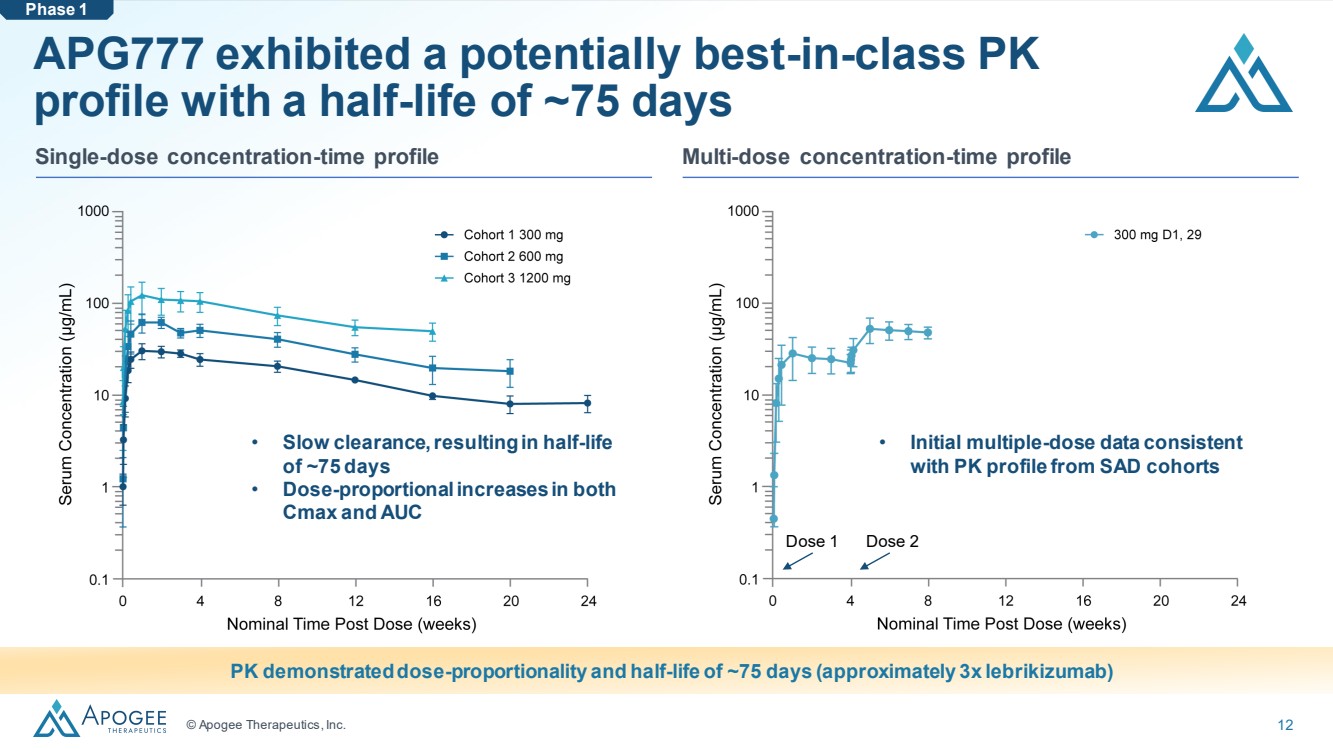
© Apogee Therapeutics, Inc. 12 APG777 exhibited a potentially best-in-class PK profile with a half-life of ~75 days • Slow clearance, resulting in half-life of ~75 days • Dose-proportional increases in both Cmax and AUC PK demonstrated dose-proportionality and half-life of ~75 days (approximately 3x lebrikizumab) • Initial multiple-dose data consistent with PK profile from SAD cohorts Single-dose concentration-time profile Multi-dose concentration-time profile Phase 1 Dose 1 Dose 2 |
|
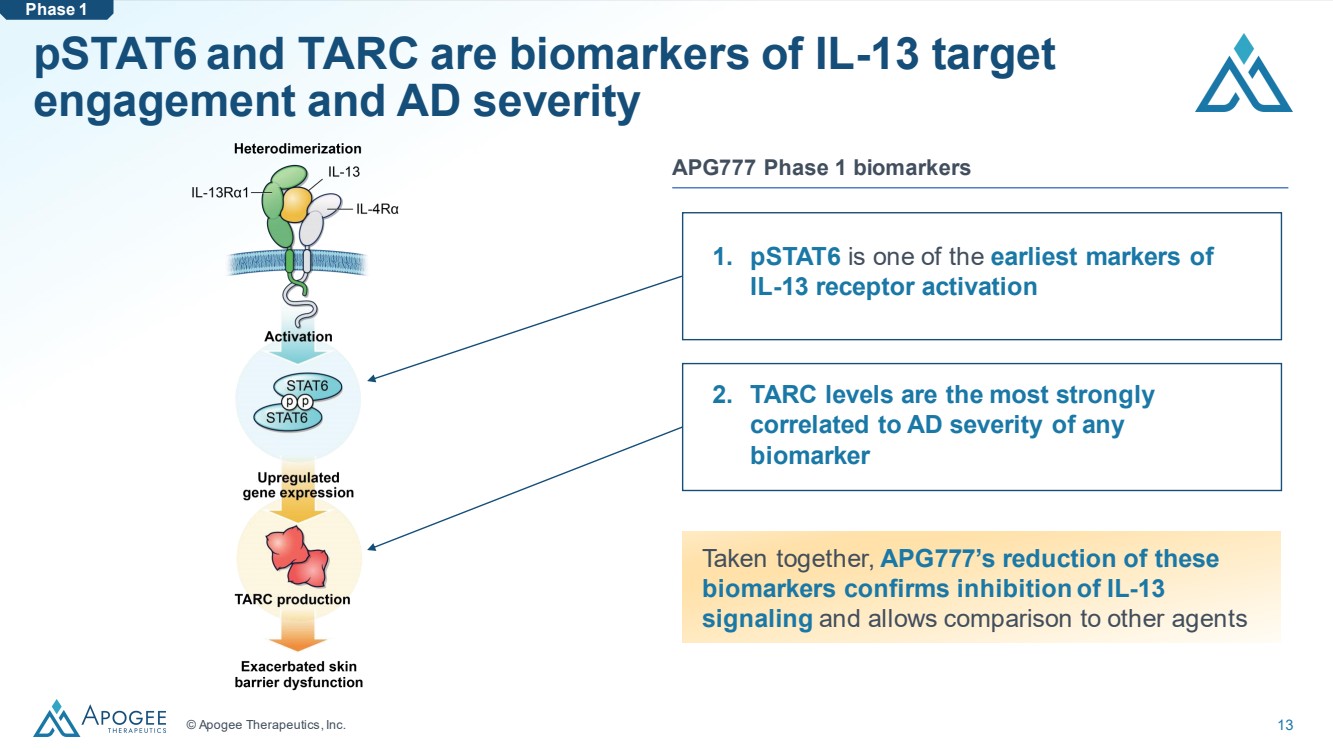
© Apogee Therapeutics, Inc. 13 pSTAT6 and TARC are biomarkers of IL-13 target engagement and AD severity 1. pSTAT6 is one of the earliest markers of IL-13 receptor activation APG777 Phase 1 biomarkers Taken together, APG777’s reduction of these biomarkers confirms inhibition of IL-13 signaling and allows comparison to other agents Phase 1 2. TARC levels are the most strongly correlated to AD severity of any biomarker |
|
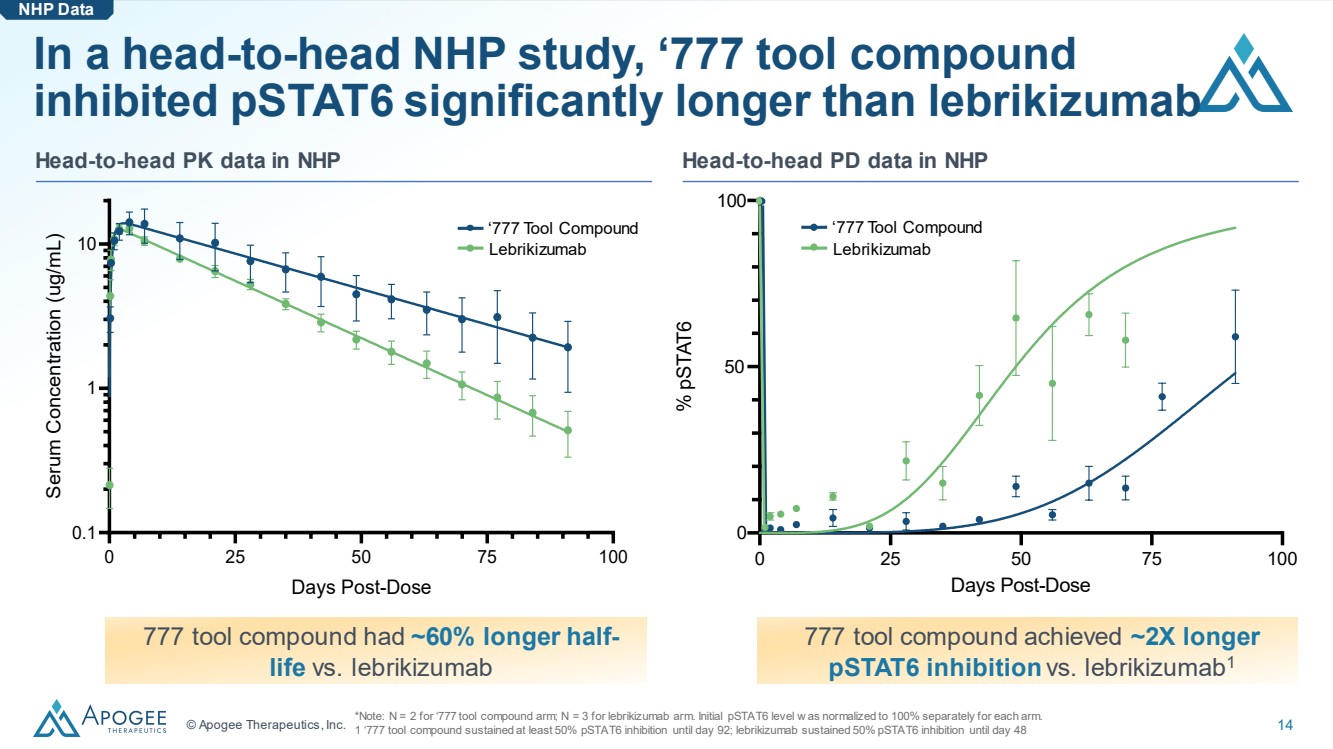
© Apogee Therapeutics, Inc. 14 0 25 50 75 100 50 100 0 Days Post-Dose % pSTAT6 ‘777 Tool Compound Lebrikizumab In a head-to-head NHP study, ‘777 tool compound inhibited pSTAT6 significantly longer than lebrikizumab Head-to-head PK data in NHP Head-to-head PD data in NHP 777 tool compound had ~60% longer half-life vs. lebrikizumab *Note: N = 2 for ‘777 tool compound arm; N = 3 for lebrikizumab arm. Initial pSTAT6 level w as normalized to 100% separately for each arm. 1 ‘777 tool compound sustained at least 50% pSTAT6 inhibition until day 92; lebrikizumab sustained 50% pSTAT6 inhibition until day 48 NHP Data 777 tool compound achieved ~2X longer pSTAT6 inhibition vs. lebrikizumab1 ‘777 Tool Compound Lebrikizumab 0 25 50 75 100 0.1 1 10 Days Post-Dose Serum Concentration (ug/mL) |
|
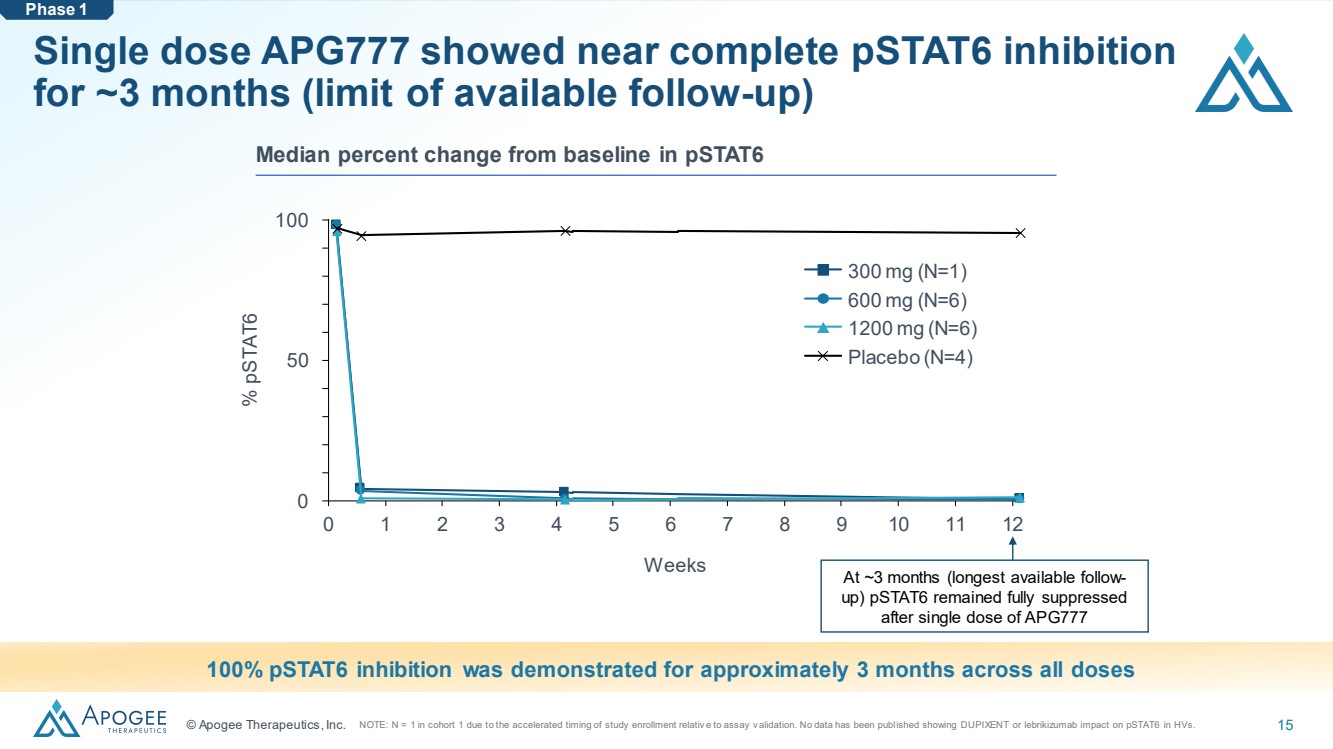
© Apogee Therapeutics, Inc. 15 Single dose APG777 showed near complete pSTAT6 inhibition for ~3 months (limit of available follow-up) 0 1 2 3 4 5 6 7 8 9 10 11 12 0 50 100 Weeks % pSTAT6 300 mg (N=1) 600 mg (N=6) 1200 mg (N=6) Placebo (N=4) 100% pSTAT6 inhibition was demonstrated for approximately 3 months across all doses Median percent change from baseline in pSTAT6 Phase 1 At ~3 months (longest available follow-up) pSTAT6 remained fully suppressed after single dose of APG777 NOTE: N = 1 in cohort 1 due to the accelerated timing of study enrollment relativ e to assay v alidation. No data has been published showing DUPIXENT or lebrikizumab impact on pSTAT6 in HVs. |
|
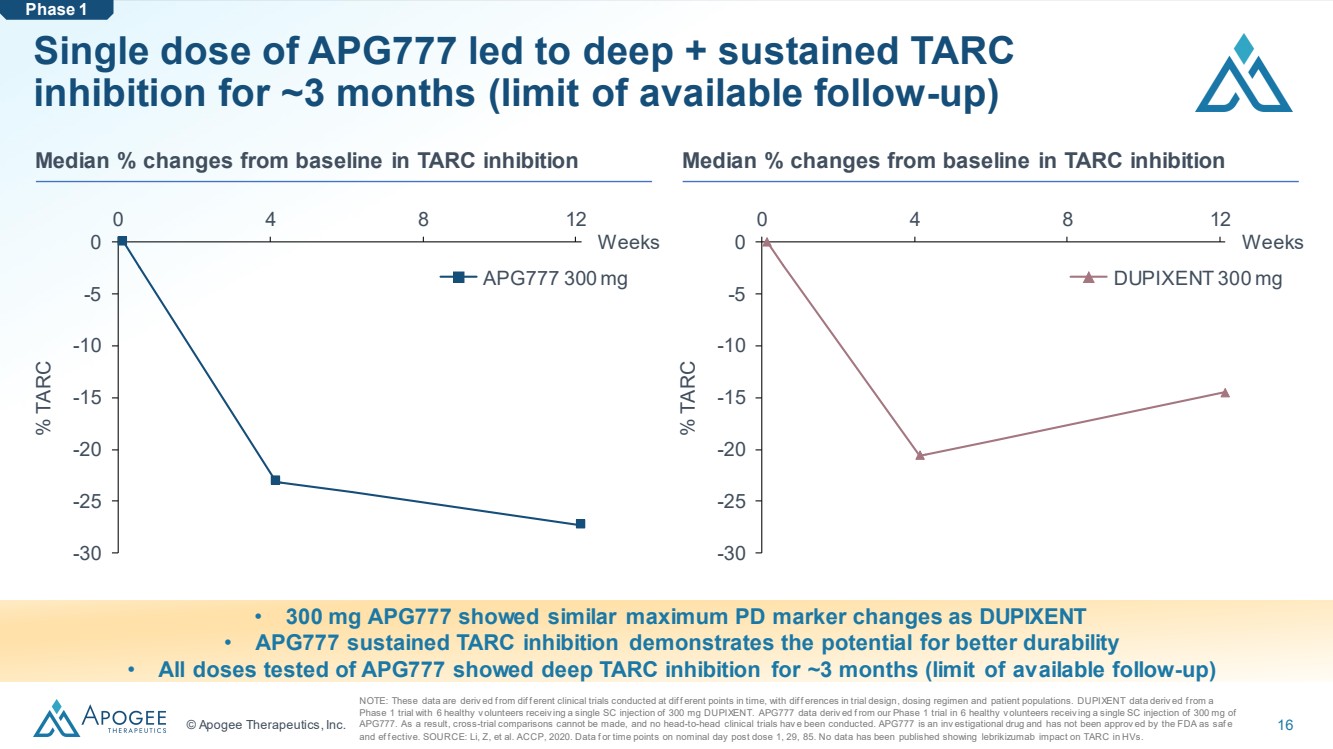
© Apogee Therapeutics, Inc. 16 Single dose of APG777 led to deep + sustained TARC inhibition for ~3 months (limit of available follow-up) • 300 mg APG777 showed similar maximum PD marker changes as DUPIXENT • APG777 sustained TARC inhibition demonstrates the potential for better durability • All doses tested of APG777 showed deep TARC inhibition for ~3 months (limit of available follow-up) -30 -25 -20 -15 -10 -5 0 0 4 8 12 Weeks % TARC APG777 300 mg NOTE: These data are deriv ed f rom dif f erent clinical trials conducted at dif f erent points in time, with dif f erences in trial design, dosing regimen and patient populations. DUPIXENT data deriv ed f rom a Phase 1 trial with 6 healthy v olunteers receiv ing a single SC injection of 300 mg DUPIXENT. APG777 data deriv ed f rom our Phase 1 trial in 6 healthy v olunteers receiv ing a single SC injection of 300 mg of APG777. As a result, cross-trial comparisons cannot be made, and no head-to-head clinical trials hav e been conducted. APG777 is an inv estigational drug and has not been approv ed by the FDA as saf e and ef f ective. SOURCE: Li, Z, et al. ACCP, 2020. Data f or time points on nominal day post dose 1, 29, 85. No data has been published showing lebrikizumab impact on TARC in HVs. Median % changes from baseline in TARC inhibition Median % changes from baseline in TARC inhibition -30 -25 -20 -15 -10 -5 0 0 4 8 12 Weeks % TARC DUPIXENT 300 mg Phase 1 |
|
© Apogee Therapeutics, Inc. 17 APG777 positive PK readout is a key risk-reducing milestone that validates program and pipeline Phase 1 Antibody attributes Clinical profile Equivalent or better potency vs. 1st generation mAbs across relevant pre-clinical assays Epitope overlaps with lebrikizumab epitope Clinically validated IL-13 target PK data supports every 3- to 6-month maintenance dosing: ~75-day half-life Near maximal pathway suppression for ~3 months (limit of current follow up) Well-tolerated with ability to achieve increased exposures in induction for potential improved clinical responses Apogee intends to initiate a Phase 2 in atopic dermatitis in 1H 2024 |
|
APG777 Phase 2 in Atopic Dermatitis |
|
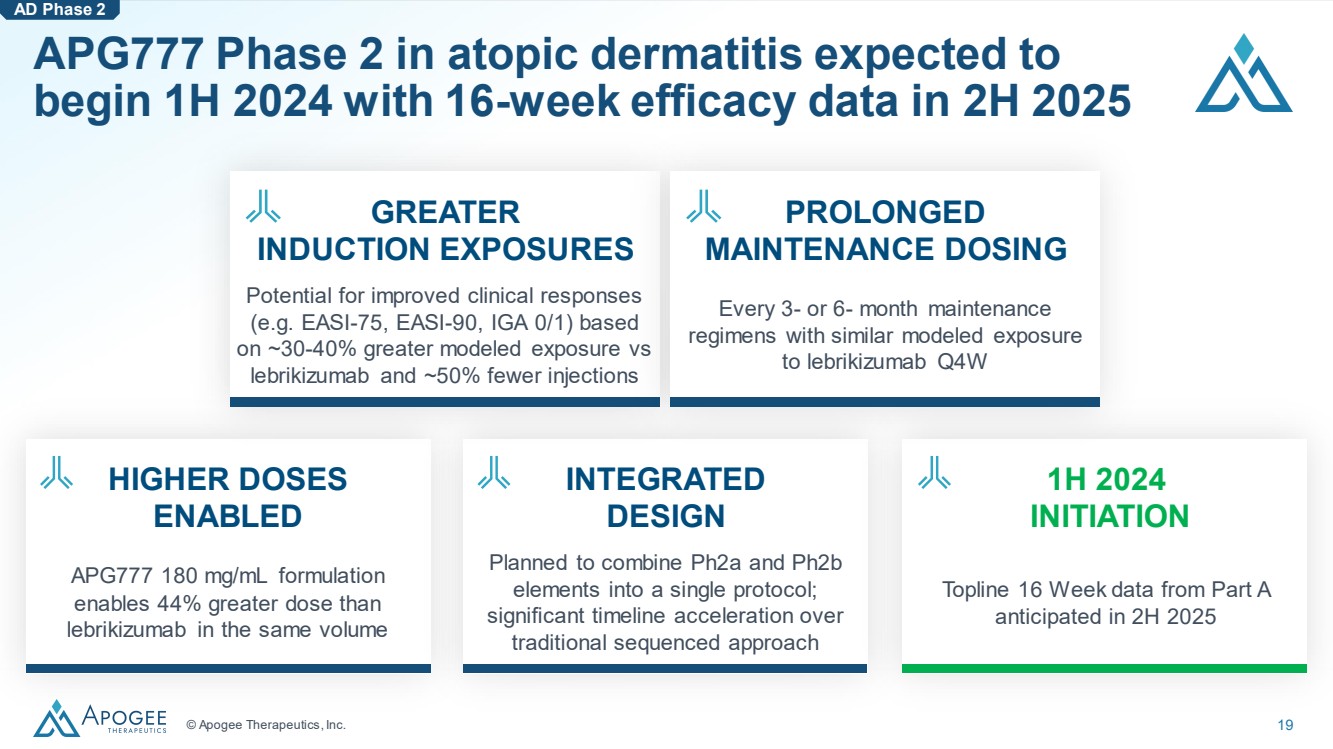
© Apogee Therapeutics, Inc. 19 APG777 Phase 2 in atopic dermatitis expected to begin 1H 2024 with 16-week efficacy data in 2H 2025 AD Phase 2 APG777 180 mg/mL formulation enables 44% greater dose than lebrikizumab in the same volume HIGHER DOSES ENABLED Planned to combine Ph2a and Ph2b elements into a single protocol; significant timeline acceleration over traditional sequenced approach INTEGRATED DESIGN Topline 16 Week data from Part A anticipated in 2H 2025 1H 2024 INITIATION Potential for improved clinical responses (e.g. EASI-75, EASI-90, IGA 0/1) based on ~30-40% greater modeled exposure vs lebrikizumab and ~50% fewer injections GREATER INDUCTION EXPOSURES Every 3- or 6- month maintenance regimens with similar modeled exposure to lebrikizumab Q4W PROLONGED MAINTENANCE DOSING |
|
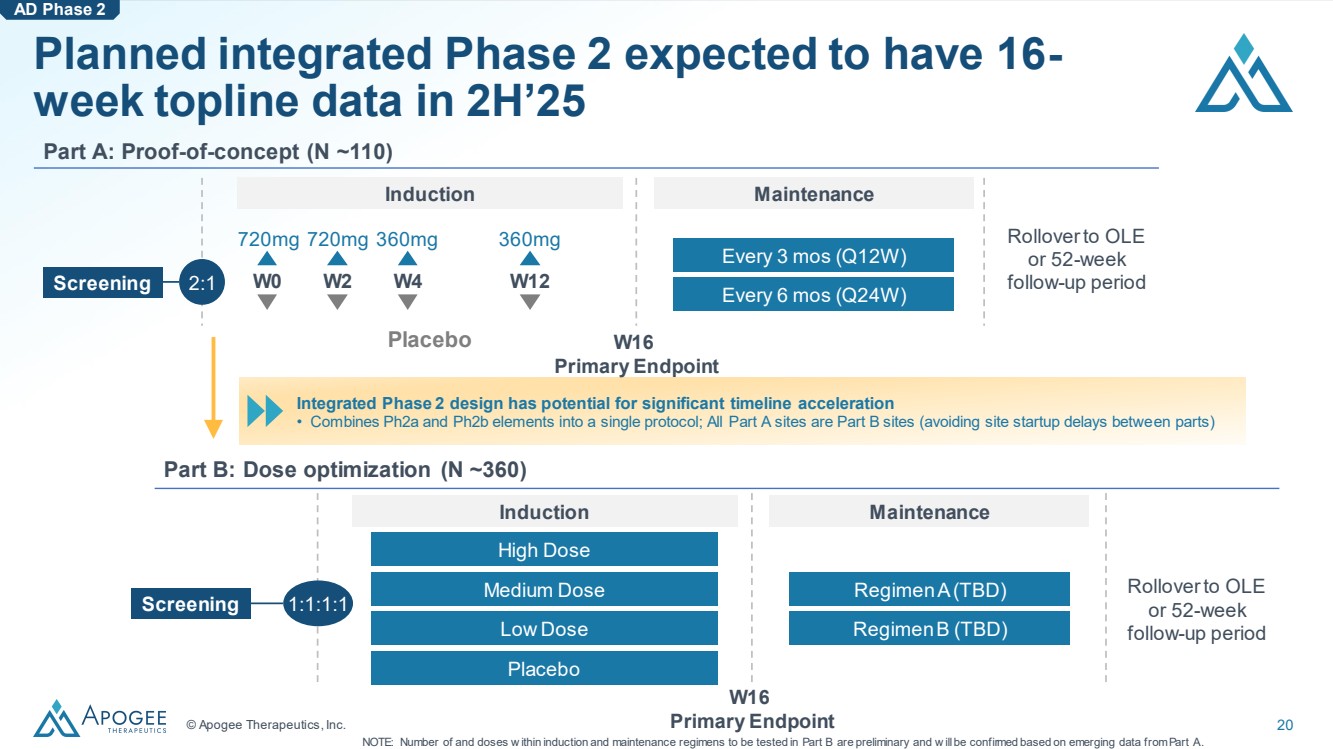
© Apogee Therapeutics, Inc. 20 Integrated Phase 2 design has potential for significant timeline acceleration • Combines Ph2a and Ph2b elements into a single protocol; All Part A sites are Part B sites (avoiding site startup delays between parts) Planned integrated Phase 2 expected to have 16- week topline data in 2H’25 Part A: Proof-of-concept (N ~110) Induction Maintenance Screening 2:1 W0 W2 W4 W12 720mg 720mg 360mg 360mg Every 3 mos (Q12W) Every 6 mos (Q24W) W16 Primary Endpoint NOTE: Number of and doses w ithin induction and maintenance regimens to be tested in Part B are preliminary and w ill be confirmed based on emerging data from Part A. Rollover to OLE or 52-week follow-up period AD Phase 2 Part B: Dose optimization (N ~360) Screening 1:1:1:1 Regimen A (TBD) Rollover to OLE or 52-week follow-up period High Dose Medium Dose Low Dose Placebo Induction Maintenance W16 Primary Endpoint Regimen B (TBD) Placebo |
|
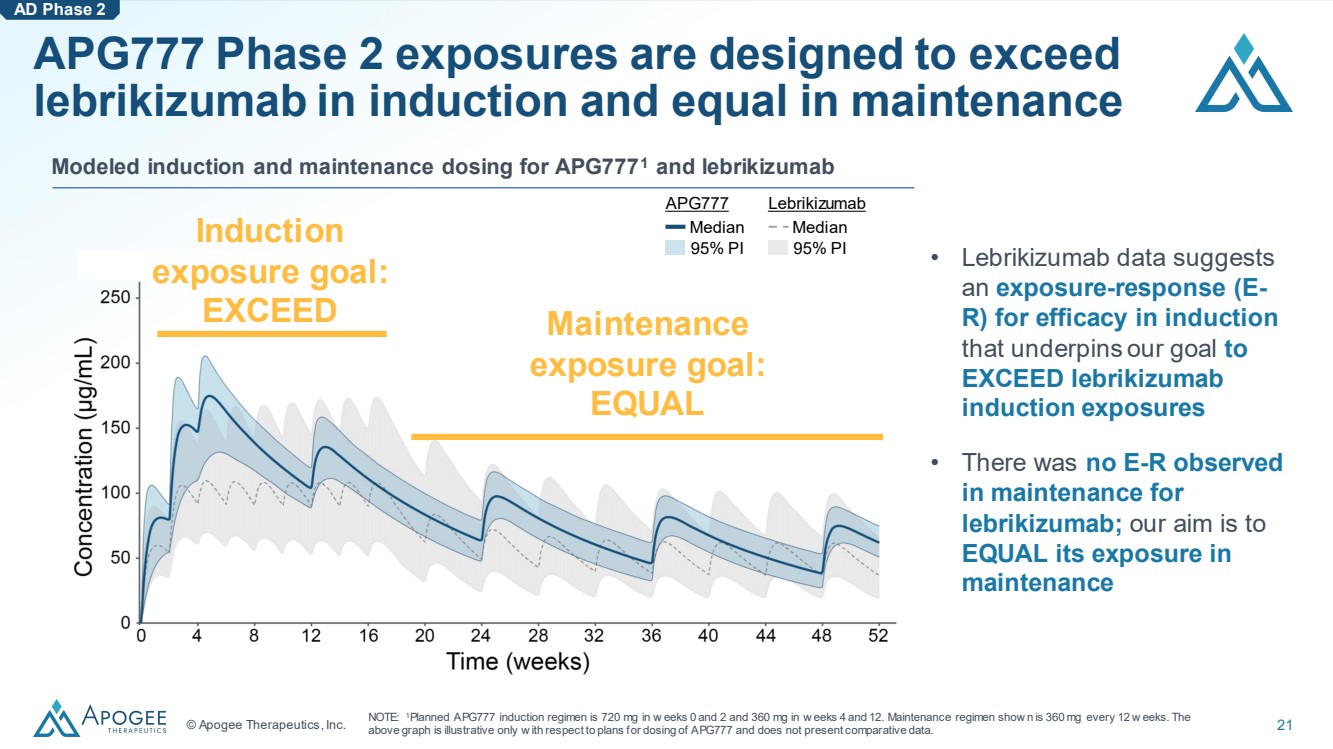
© Apogee Therapeutics, Inc. 21 APG777 Phase 2 exposures are designed to exceed lebrikizumab in induction and equal in maintenance Modeled induction and maintenance dosing for APG7771 and lebrikizumab Induction exposure goal: EXCEED Maintenance exposure goal: EQUAL AD Phase 2 • Lebrikizumab data suggests an exposure-response (E-R) for efficacy in induction that underpins our goal to EXCEED lebrikizumab induction exposures • There was no E-R observed in maintenance for lebrikizumab; our aim is to EQUAL its exposure in maintenance APG777 Median 95% PI Lebrikizumab Median 95% PI NOTE: 1Planned APG777 induction regimen is 720 mg in w eeks 0 and 2 and 360 mg in w eeks 4 and 12. Maintenance regimen show n is 360 mg every 12 w eeks. The above graph is illustrative only w ith respect to plans for dosing of APG777 and does not present comparative data. |
|
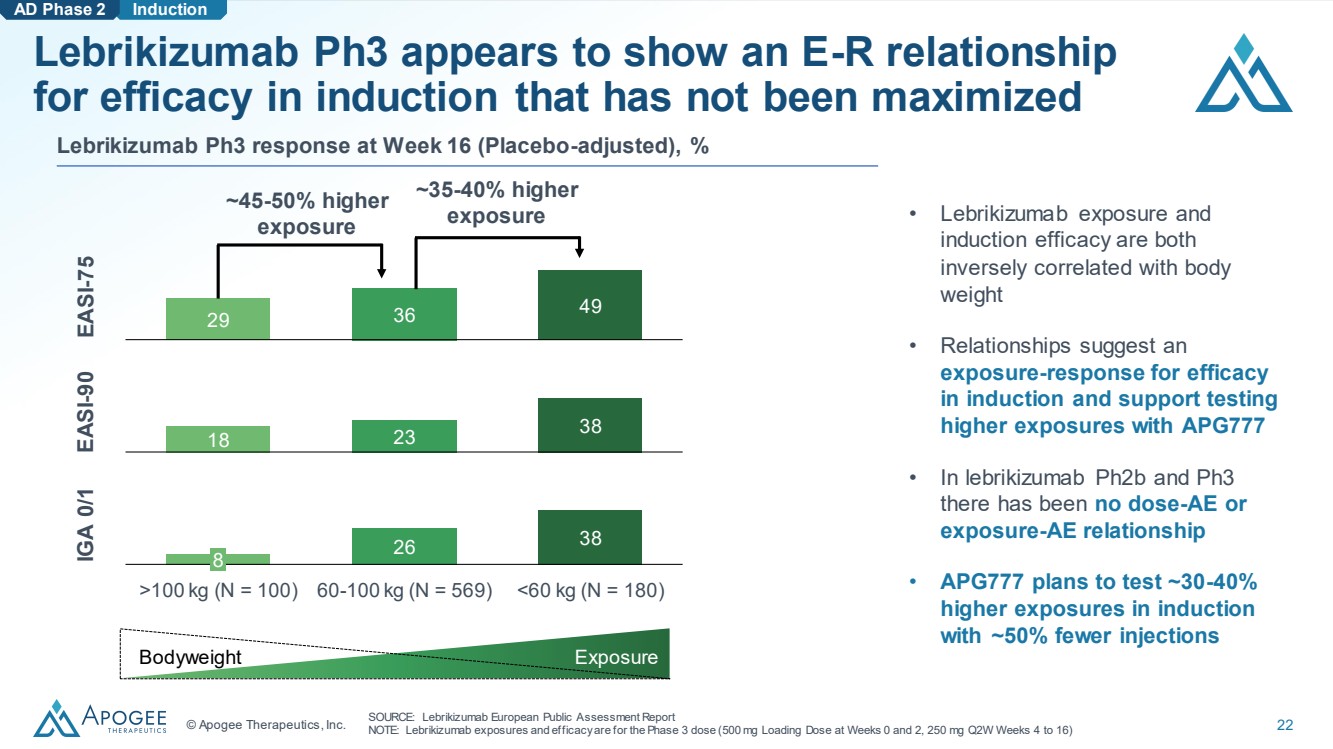
© Apogee Therapeutics, Inc. 22 Exposure Induction Lebrikizumab Ph3 appears to show an E-R relationship for efficacy in induction that has not been maximized SOURCE: Lebrikizumab European Public Assessment Report NOTE: Lebrikizumab exposures and efficacy are for the Phase 3 dose (500 mg Loading Dose at Weeks 0 and 2, 250 mg Q2W Weeks 4 to 16) Lebrikizumab Ph3 response at Week 16 (Placebo-adjusted), % 26 38 8 >100 kg (N = 100) 60-100 kg (N = 569) <60 kg (N = 180) 18 23 38 29 36 49 EASI-75 EASI-90 IGA 0/1 • Lebrikizumab exposure and induction efficacy are both inversely correlated with body weight • Relationships suggest an exposure-response for efficacy in induction and support testing higher exposures with APG777 • In lebrikizumab Ph2b and Ph3 there has been no dose-AE or exposure-AE relationship • APG777 plans to test ~30-40% higher exposures in induction with ~50% fewer injections AD Phase 2 ~35-40% higher exposure ~45-50% higher exposure Bodyweight |
|
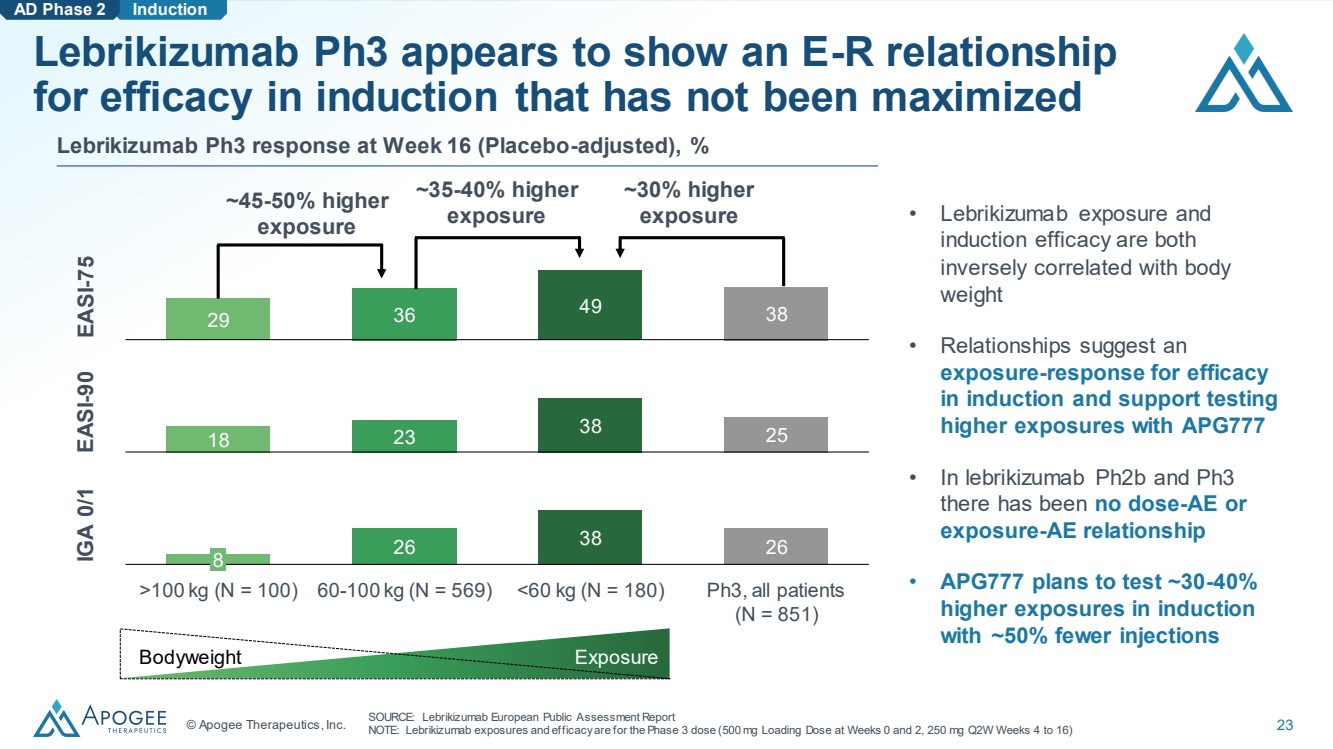
© Apogee Therapeutics, Inc. 23 Exposure Induction Lebrikizumab Ph3 appears to show an E-R relationship for efficacy in induction that has not been maximized SOURCE: Lebrikizumab European Public Assessment Report NOTE: Lebrikizumab exposures and efficacy are for the Phase 3 dose (500 mg Loading Dose at Weeks 0 and 2, 250 mg Q2W Weeks 4 to 16) Lebrikizumab Ph3 response at Week 16 (Placebo-adjusted), % 26 38 26 8 >100 kg (N = 100) 60-100 kg (N = 569) <60 kg (N = 180) Ph3, all patients (N = 851) 18 23 38 25 29 36 49 38 EASI-75 EASI-90 IGA 0/1 ~30% higher exposure • Lebrikizumab exposure and induction efficacy are both inversely correlated with body weight • Relationships suggest an exposure-response for efficacy in induction and support testing higher exposures with APG777 • In lebrikizumab Ph2b and Ph3 there has been no dose-AE or exposure-AE relationship • APG777 plans to test ~30-40% higher exposures in induction with ~50% fewer injections AD Phase 2 ~35-40% higher exposure ~45-50% higher exposure Bodyweight |
|
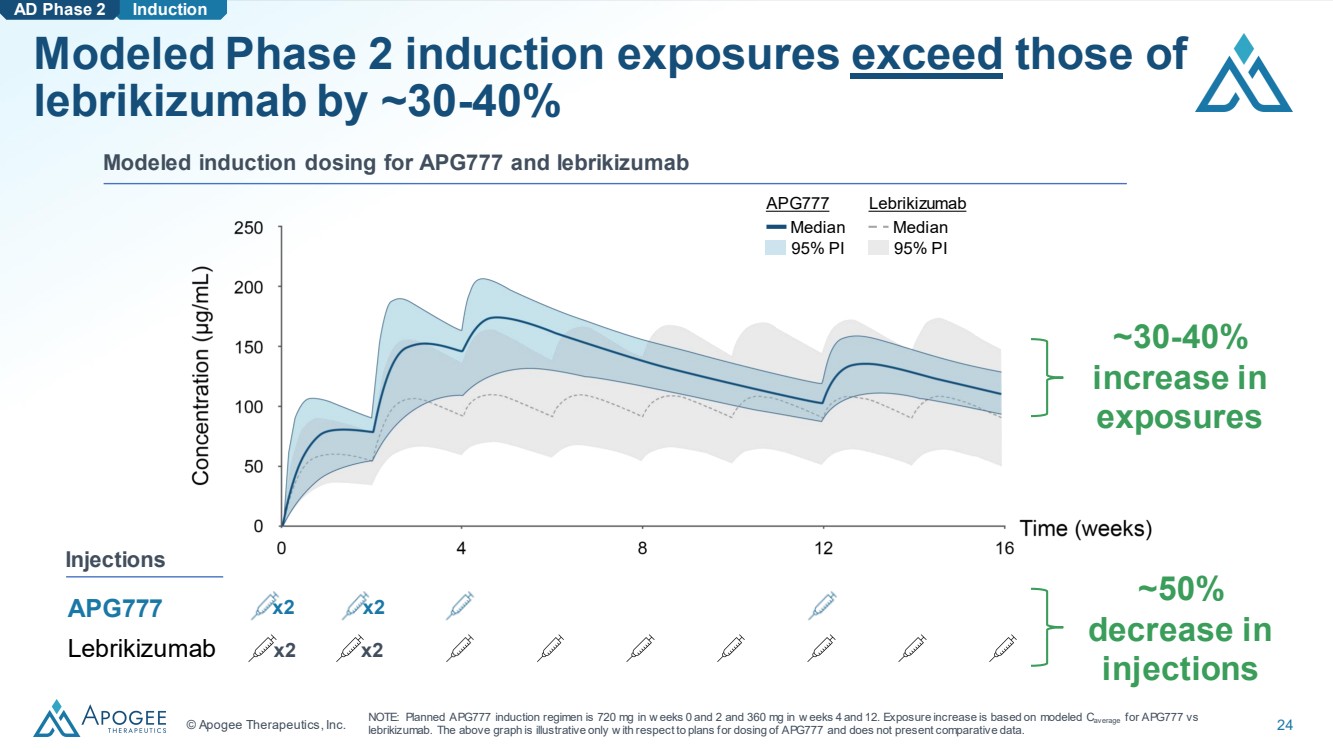
© Apogee Therapeutics, Inc. 24 Modeled induction dosing for APG777 and lebrikizumab Modeled Phase 2 induction exposures exceed those of lebrikizumab by ~30-40% ~30-40% increase in exposures APG777 Lebrikizumab Injections x2 x2 x2 x2 Induction NOTE: Planned APG777 induction regimen is 720 mg in w eeks 0 and 2 and 360 mg in w eeks 4 and 12. Exposure increase is based on modeled Caverage for APG777 vs lebrikizumab. The above graph is illustrative only w ith respect to plans for dosing of APG777 and does not present comparative data. ~50% decrease in injections AD Phase 2 APG777 Median 95% PI Lebrikizumab Median 95% PI |
|
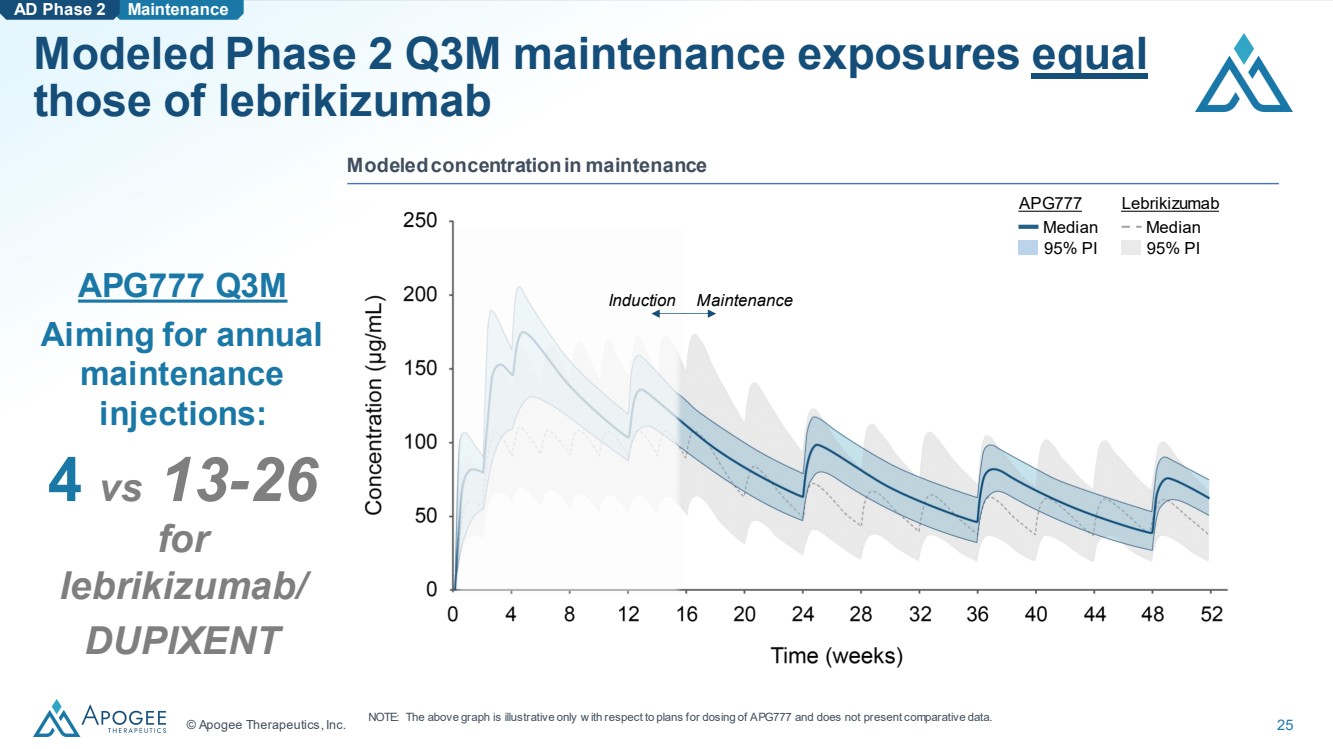
© Apogee Therapeutics, Inc. 25 Modeled Phase 2 Q3M maintenance exposures equal those of lebrikizumab AD Phase 2 Maintenance APG777 Q3M Aiming for annual maintenance injections: 4 vs 13-26 for lebrikizumab/ DUPIXENT Modeled concentration in maintenance Induction Maintenance APG777 Median 95% PI Lebrikizumab Median 95% PI NOTE: The above graph is illustrative only w ith respect to plans for dosing of APG777 and does not present comparative data. |
|
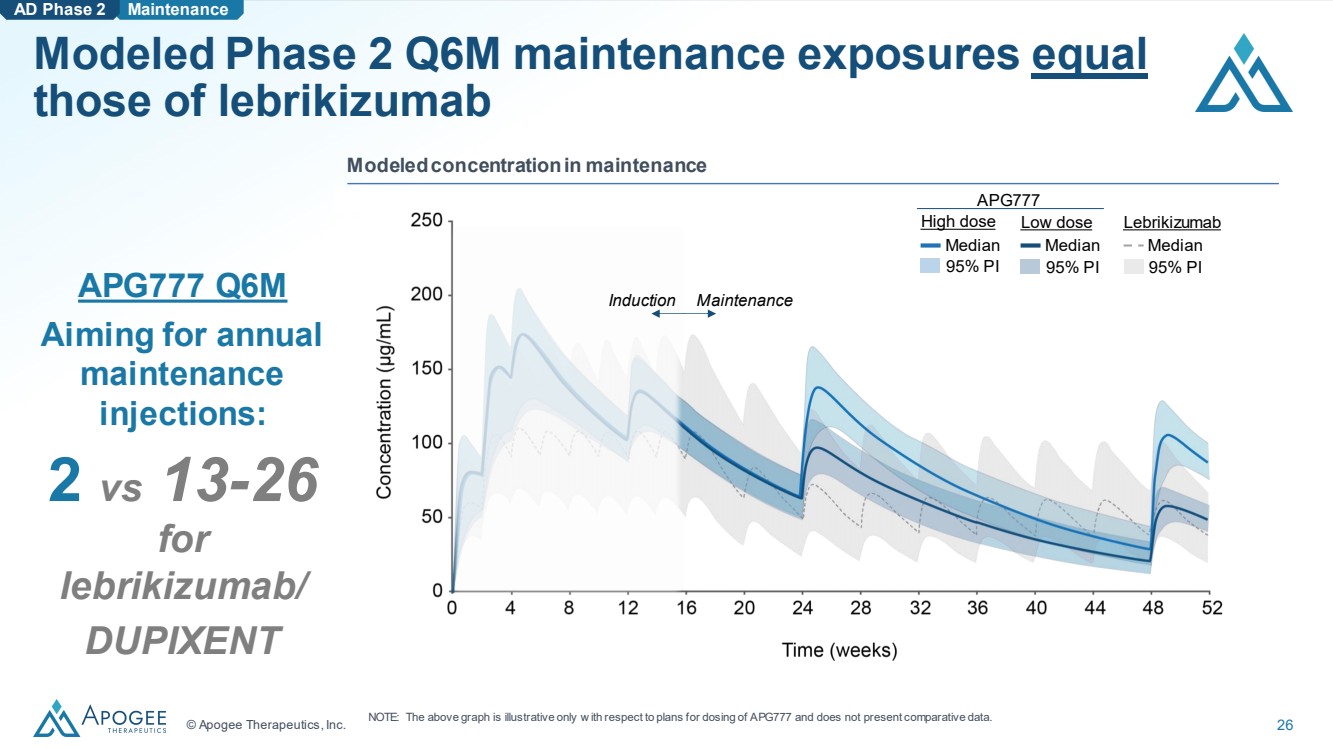
© Apogee Therapeutics, Inc. 26 Modeled Phase 2 Q6M maintenance exposures equal those of lebrikizumab AD Phase 2 Maintenance APG777 Q6M Aiming for annual maintenance injections: 2 vs 13-26 for lebrikizumab/ DUPIXENT Modeled concentration in maintenance Induction Maintenance 95% PI Median Low dose Median 95% PI Lebrikizumab Median 95% PI APG777 High dose NOTE: The above graph is illustrative only w ith respect to plans for dosing of APG777 and does not present comparative data. |
|
Building a Leading I&I Company |
|
© Apogee Therapeutics, Inc. 28 APG777’s best-in-class Phase 1 PK profile shows potential to be a leading product in the expected $50B+ AD market1 Favorable product characteristics and COGS • As few as 2-4 doses per year in maintenance • Expected improved formulation, manufacturability and viscosity Potential for improved clinical responses (e.g. EASI-75, EASI-90, IGA 0/1) based on ~30-40% greater modeled induction exposures than lebrikizumab • Overlapping epitope and equivalent potency as lebrikizumab (KD < 100 pM) 2 • ~30% higher exposure seen in lebrikizumab low bodyweight group resulted in at least 10 PPT better efficacy than overall study population across all key endpoints Extended dosing interval addresses clear unmet need • Potential for every 3- or 6-month dosing to improve patient convenience & compliance Novel IP into mid-2040s Corporate APG777 NOTE: 1$50B projected AD market in 2035, based on projected growth of AD market at a similar rate to psoriasis. 2APG777 has demonstrated equiv alent potency to lebrikizumab in our head-to-head preclinical assay s. SOURCE: Ev aluatePharma. |
|
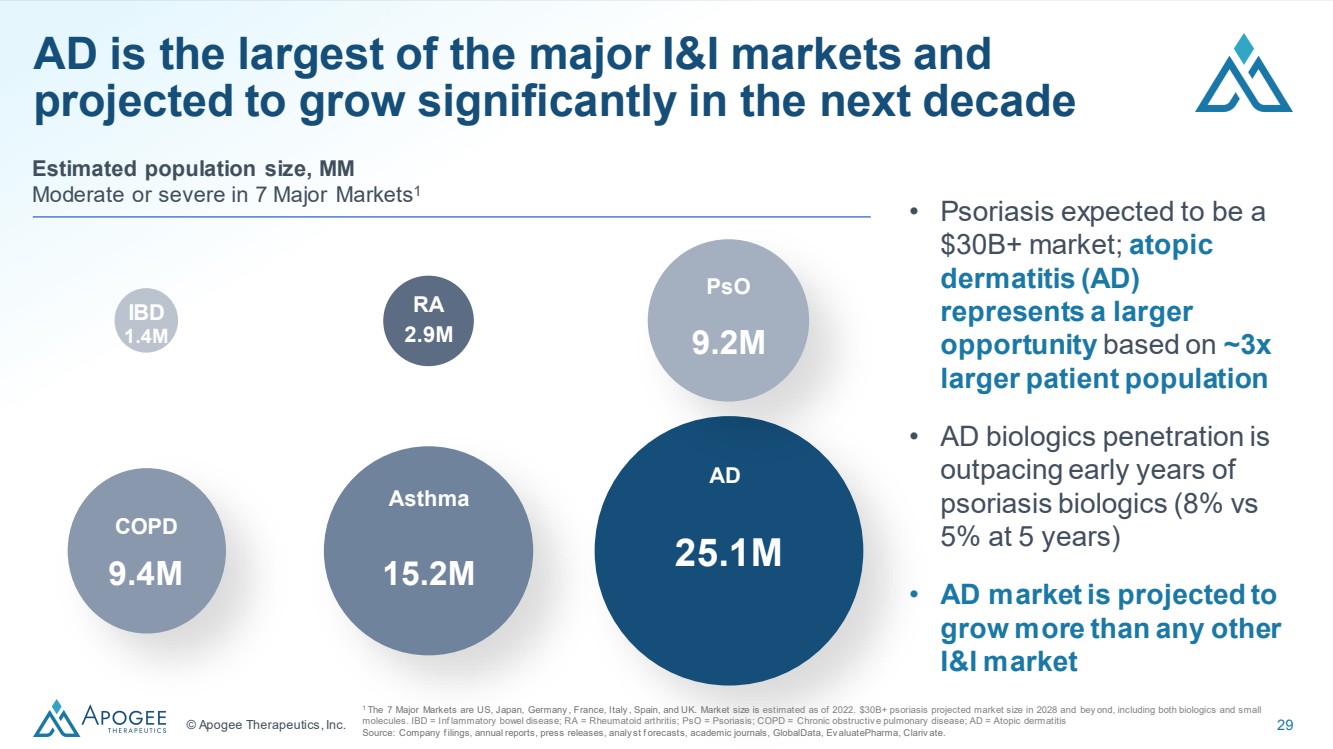
© Apogee Therapeutics, Inc. 29 AD is the largest of the major I&I markets and projected to grow significantly in the next decade Estimated population size, MM Moderate or severe in 7 Major Markets1 25.1M AD 1.4M IBD 2.9M RA 15.2M Asthma 9.4M COPD 9.2M PsO • Psoriasis expected to be a $30B+ market; atopic dermatitis (AD) represents a larger opportunity based on ~3x larger patient population • AD biologics penetration is outpacing early years of psoriasis biologics (8% vs 5% at 5 years) • AD market is projected to grow more than any other I&I market 1 The 7 Major Markets are US, Japan, Germany , France, Italy , Spain, and UK. Market size is estimated as of 2022. $30B+ psoriasis projected market size in 2028 and bey ond, including both biologics and small molecules. IBD = Inf lammatory bowel disease; RA = Rheumatoid arthritis; PsO = Psoriasis; COPD = Chronic obstructiv e pulmonary disease; AD = Atopic dermatitis Source: Company f ilings, annual reports, press releases, analy st f orecasts, academic journals, GlobalData, Ev aluatePharma, Clariv ate. |
|
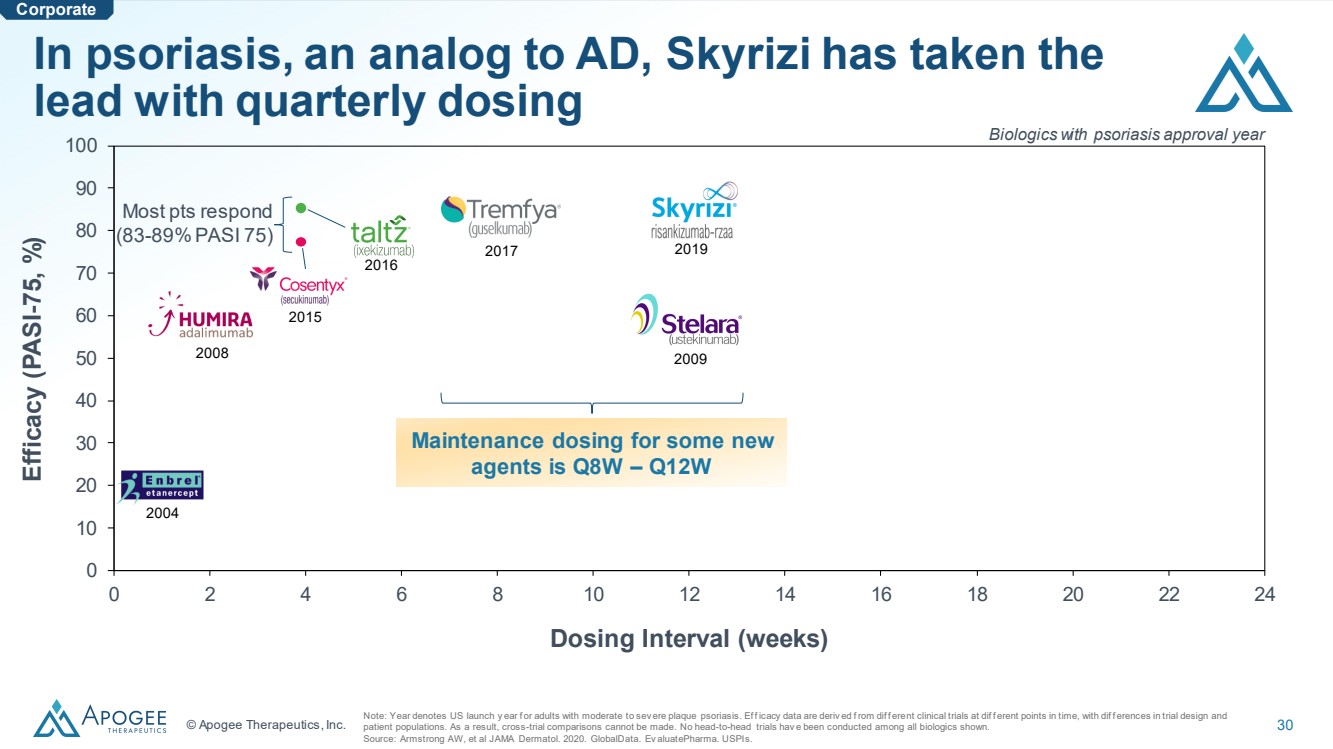
© Apogee Therapeutics, Inc. 30 0 10 20 30 40 50 60 70 80 90 100 0 2 4 6 8 10 12 14 16 18 20 22 24 Dosing Interval (weeks) Efficacy (PASI -75, %) In psoriasis, an analog to AD, Skyrizi has taken the lead with quarterly dosing Note: Year denotes US launch y ear f or adults with moderate to sev ere plaque psoriasis. Ef f icacy data are deriv ed f rom dif f erent clinical trials at dif f erent points in time, with dif f erences in trial design and patient populations. As a result, cross-trial comparisons cannot be made. No head-to-head trials hav e been conducted among all biologics shown. Source: Armstrong AW, et al JAMA Dermatol. 2020. GlobalData. Ev aluatePharma. USPIs. Most pts respond (83-89% PASI 75) 2019 2009 2017 2015 2016 2008 2004 Biologics with psoriasis approval year Maintenance dosing for some new agents is Q8W – Q12W Corporate |
|
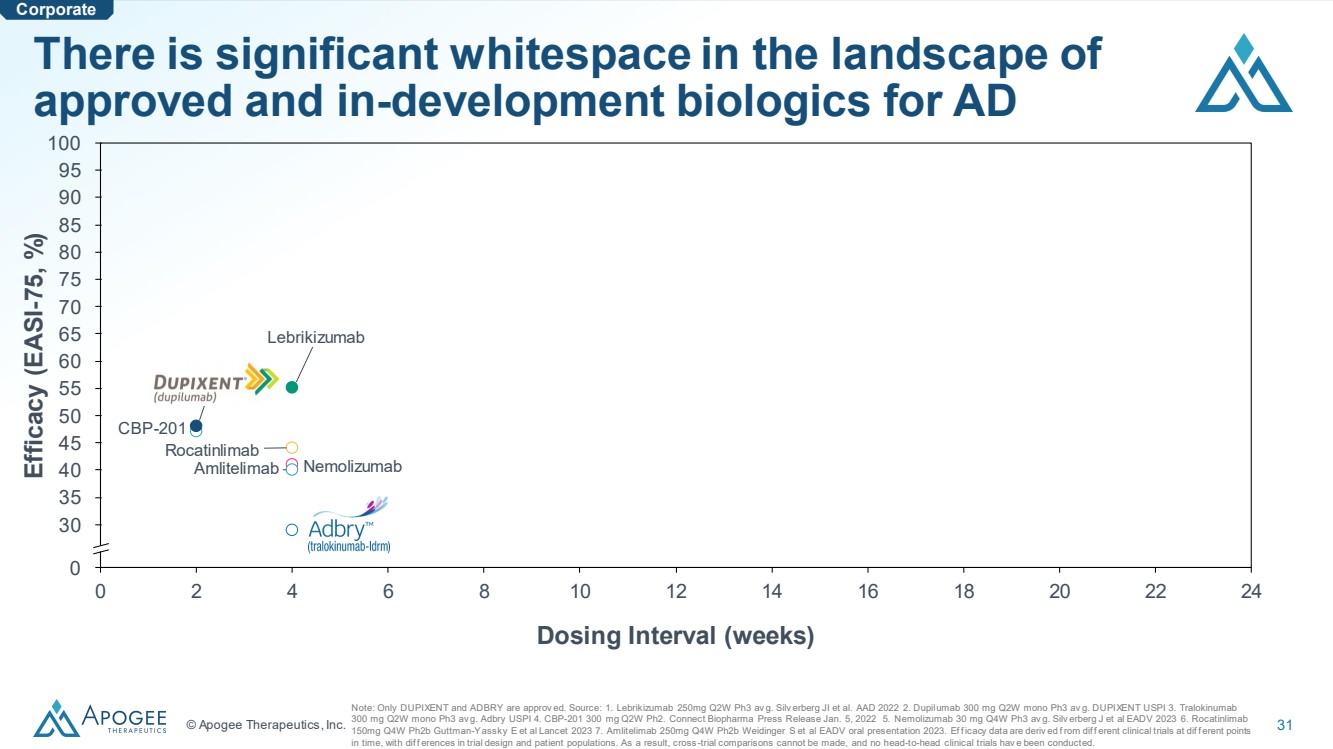
© Apogee Therapeutics, Inc. 31 0 2 4 6 8 10 12 14 16 18 20 22 24 0 30 35 40 45 50 55 60 65 70 75 80 95 90 100 85 Dosing Interval (weeks) Lebrikizumab CBP-201 Nemolizumab Rocatinlimab Amlitelimab Dupilumab Tralokinumab There is significant whitespace in the landscape of approved and in-development biologics for AD Note: Only DUPIXENT and ADBRY are approv ed. Source: 1. Lebrikizumab 250mg Q2W Ph3 av g. Silv erberg JI et al. AAD 2022 2. Dupilumab 300 mg Q2W mono Ph3 av g. DUPIXENT USPI 3. Tralokinumab 300 mg Q2W mono Ph3 av g. Adbry USPI 4. CBP-201 300 mg Q2W Ph2. Connect Biopharma Press Release Jan. 5, 2022 5. Nemolizumab 30 mg Q4W Ph3 av g. Silv erberg J et al EADV 2023 6. Rocatinlimab 150mg Q4W Ph2b Guttman-Yassky E et al Lancet 2023 7. Amlitelimab 250mg Q4W Ph2b Weidinger S et al EADV oral presentation 2023. Ef f icacy data are deriv ed f rom dif f erent clinical trials at dif f erent points in time, with dif f erences in trial design and patient populations. As a result, cross-trial comparisons cannot be made, and no head-to-head clinical trials hav e been conducted. Efficacy (EASI -75, %) Corporate |
|
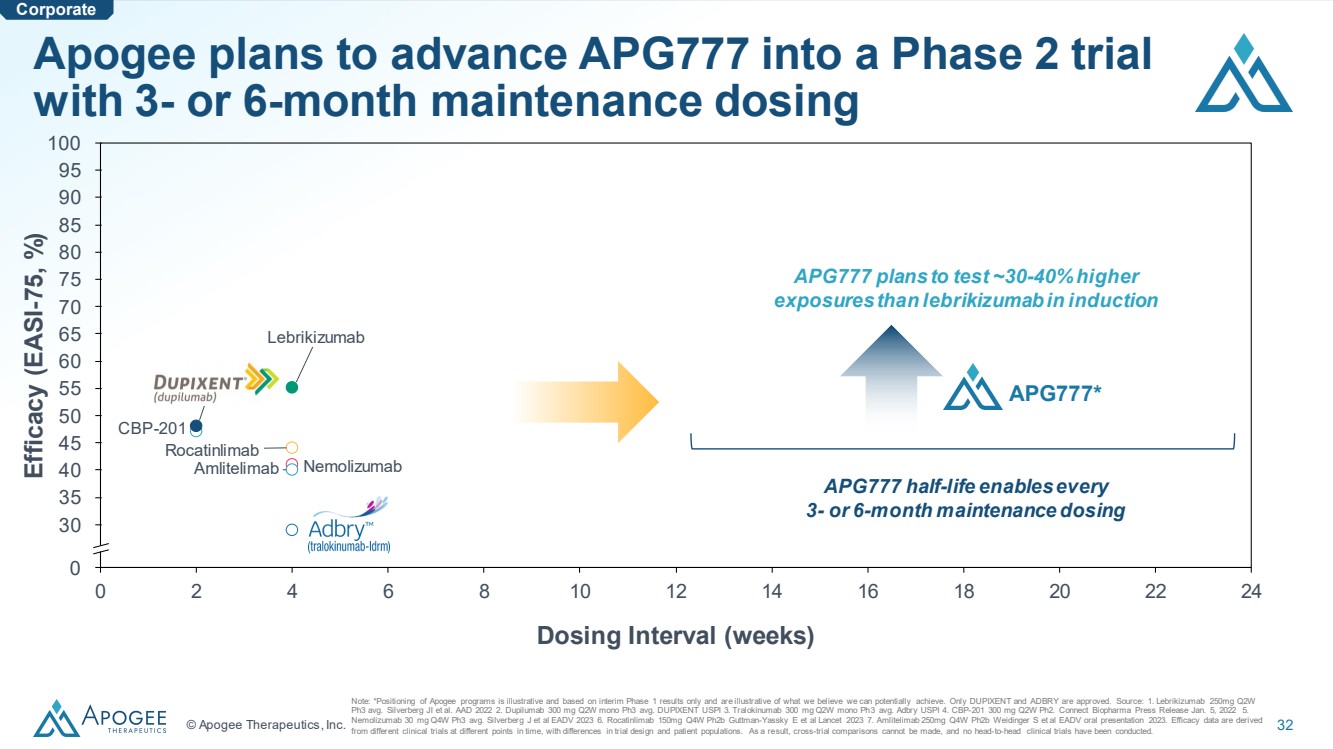
© Apogee Therapeutics, Inc. 32 0 2 4 6 8 10 12 14 16 18 20 22 24 0 30 35 40 45 50 55 60 65 70 75 80 95 90 100 85 Dosing Interval (weeks) Lebrikizumab CBP-201 Nemolizumab Rocatinlimab Amlitelimab Dupilumab Tralokinumab Apogee plans to advance APG777 into a Phase 2 trial with 3- or 6-month maintenance dosing Note: *Positioning of Apogee programs is illustrative and based on interim Phase 1 results only and are illustrative of what we believe we can potentially achieve. Only DUPIXENT and ADBRY are approved. Source: 1. Lebrikizumab 250mg Q2W Ph3 avg. Silverberg JI et al. AAD 2022 2. Dupilumab 300 mg Q2W mono Ph3 avg. DUPIXENT USPI 3. Tralokinumab 300 mg Q2W mono Ph3 avg. Adbry USPI 4. CBP-201 300 mg Q2W Ph2. Connect Biopharma Press Release Jan. 5, 2022 5. Nemolizumab 30 mg Q4W Ph3 avg. Silverberg J et al EADV 2023 6. Rocatinlimab 150mg Q4W Ph2b Guttman-Yassky E et al Lancet 2023 7. Amlitelimab 250mg Q4W Ph2b Weidinger S et al EADV oral presentation 2023. Efficacy data are derived from different clinical trials at different points in time, with differences in trial design and patient populations. As a result, cross-trial comparisons cannot be made, and no head-to-head clinical trials have been conducted. Corporate Efficacy (EASI -75, %) APG777 plans to test ~30-40% higher exposures than lebrikizumab in induction APG777 half-life enables every 3- or 6-month maintenance dosing APG777* |
|
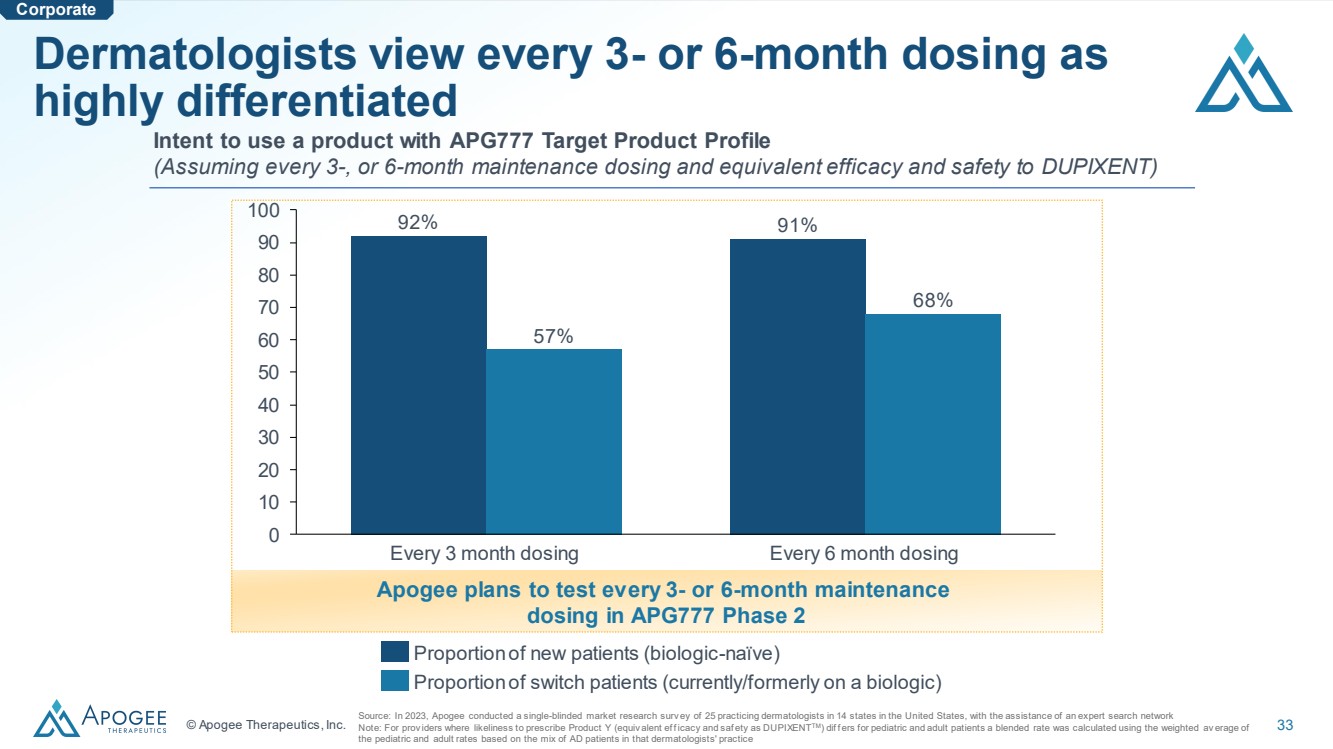
© Apogee Therapeutics, Inc. 33 Dermatologists view every 3- or 6-month dosing as highly differentiated Source: In 2023, Apogee conducted a single-blinded market research surv ey of 25 practicing dermatologists in 14 states in the United States, with the assistance of an expert search network Note: For prov iders where likeliness to prescribe Product Y (equiv alent ef f icacy and saf ety as DUPIXENTTM) dif f ers for pediatric and adult patients a blended rate was calculated using the weighted av erage of the pediatric and adult rates based on the mix of AD patients in that dermatologists' practice 0 10 20 30 40 50 60 70 80 90 100 Every 3 month dosing Every 6 month dosing 92% 57% 91% 68% Proportion of new patients (biologic-naïve) Proportion of switch patients (currently/formerly on a biologic) Intent to use a product with APG777 Target Product Profile (Assuming every 3-, or 6-month maintenance dosing and equivalent efficacy and safety to DUPIXENT) Apogee plans to test every 3- or 6-month maintenance dosing in APG777 Phase 2 Corporate |
|
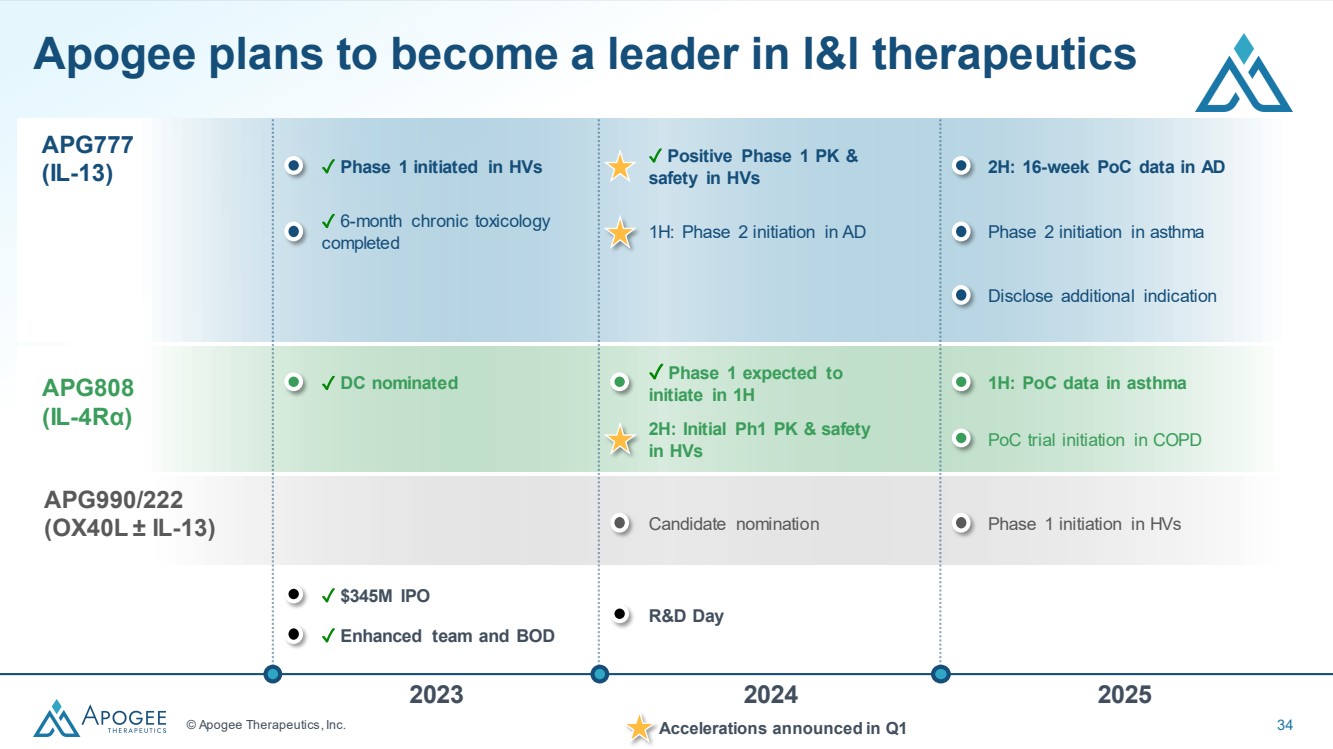
© Apogee Therapeutics, Inc. 34 APG777 (IL-13) ✓ Positive Phase 1 PK & safety in HVs 1H: Phase 2 initiation in AD 2H: 16-week PoC data in AD Phase 2 initiation in asthma Disclose additional indication ✓ Phase 1 initiated in HVs ✓ 6-month chronic toxicology completed Candidate nomination Phase 1 initiation in HVs Apogee plans to become a leader in l&l therapeutics 2023 2024 2025 R&D Day APG990/222 (OX40L ± IL-13) APG808 (IL-4Rα) ✓ Phase 1 expected to initiate in 1H 2H: Initial Ph1 PK & safety in HVs 1H: PoC data in asthma PoC trial initiation in COPD ✓ DC nominated ✓ $345M IPO ✓ Enhanced team and BOD Accelerations announced in Q1 |
|
Q&A Backup |
|
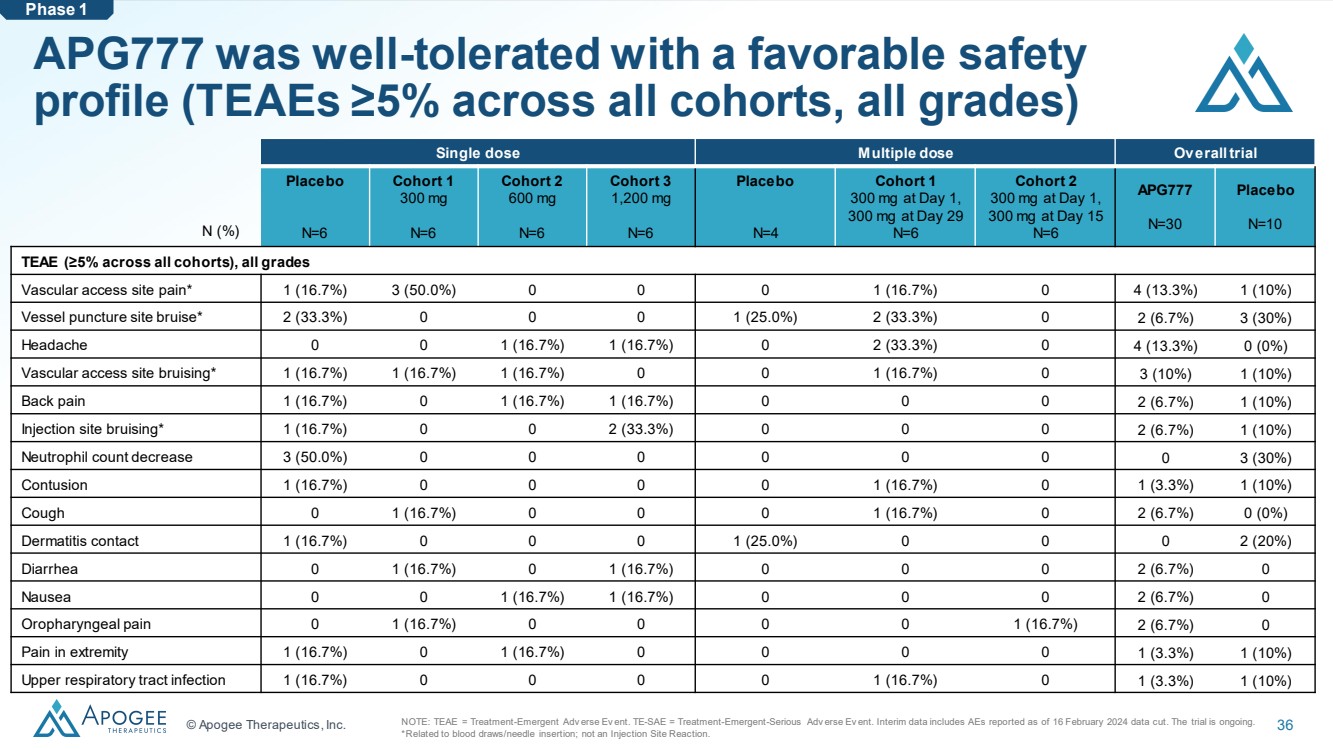
© Apogee Therapeutics, Inc. 36 APG777 was well-tolerated with a favorable safety profile (TEAEs ≥5% across all cohorts, all grades) Single dose Multiple dose Overall trial Placebo N=6 Cohort 1 300 mg N=6 Cohort 2 600 mg N=6 Cohort 3 1,200 mg N=6 Placebo N=4 Cohort 1 300 mg at Day 1, 300 mg at Day 29 N=6 Cohort 2 300 mg at Day 1, 300 mg at Day 15 N=6 APG777 N=30 Placebo N=10 TEAE (≥5% across all cohorts), all grades Vascular access site pain* 1 (16.7%) 3 (50.0%) 0 0 0 1 (16.7%) 0 4 (13.3%) 1 (10%) Vessel puncture site bruise* 2 (33.3%) 0 0 0 1 (25.0%) 2 (33.3%) 0 2 (6.7%) 3 (30%) Headache 0 0 1 (16.7%) 1 (16.7%) 0 2 (33.3%) 0 4 (13.3%) 0 (0%) Vascular access site bruising* 1 (16.7%) 1 (16.7%) 1 (16.7%) 0 0 1 (16.7%) 0 3 (10%) 1 (10%) Back pain 1 (16.7%) 0 1 (16.7%) 1 (16.7%) 0 0 0 2 (6.7%) 1 (10%) Injection site bruising* 1 (16.7%) 0 0 2 (33.3%) 0 0 0 2 (6.7%) 1 (10%) Neutrophil count decrease 3 (50.0%) 0 0 0 0 0 0 0 3 (30%) Contusion 1 (16.7%) 0 0 0 0 1 (16.7%) 0 1 (3.3%) 1 (10%) Cough 0 1 (16.7%) 0 0 0 1 (16.7%) 0 2 (6.7%) 0 (0%) Dermatitis contact 1 (16.7%) 0 0 0 1 (25.0%) 0 0 0 2 (20%) Diarrhea 0 1 (16.7%) 0 1 (16.7%) 0 0 0 2 (6.7%) 0 Nausea 0 0 1 (16.7%) 1 (16.7%) 0 0 0 2 (6.7%) 0 Oropharyngeal pain 0 1 (16.7%) 0 0 0 0 1 (16.7%) 2 (6.7%) 0 Pain in extremity 1 (16.7%) 0 1 (16.7%) 0 0 0 0 1 (3.3%) 1 (10%) Upper respiratory tract infection 1 (16.7%) 0 0 0 0 1 (16.7%) 0 1 (3.3%) 1 (10%) N (%) Phase 1 NOTE: TEAE = Treatment-Emergent Adv erse Ev ent. TE-SAE = Treatment-Emergent-Serious Adv erse Ev ent. Interim data includes AEs reported as of 16 February 2024 data cut. The trial is ongoing. *Related to blood draws/needle insertion; not an Injection Site Reaction. |
|
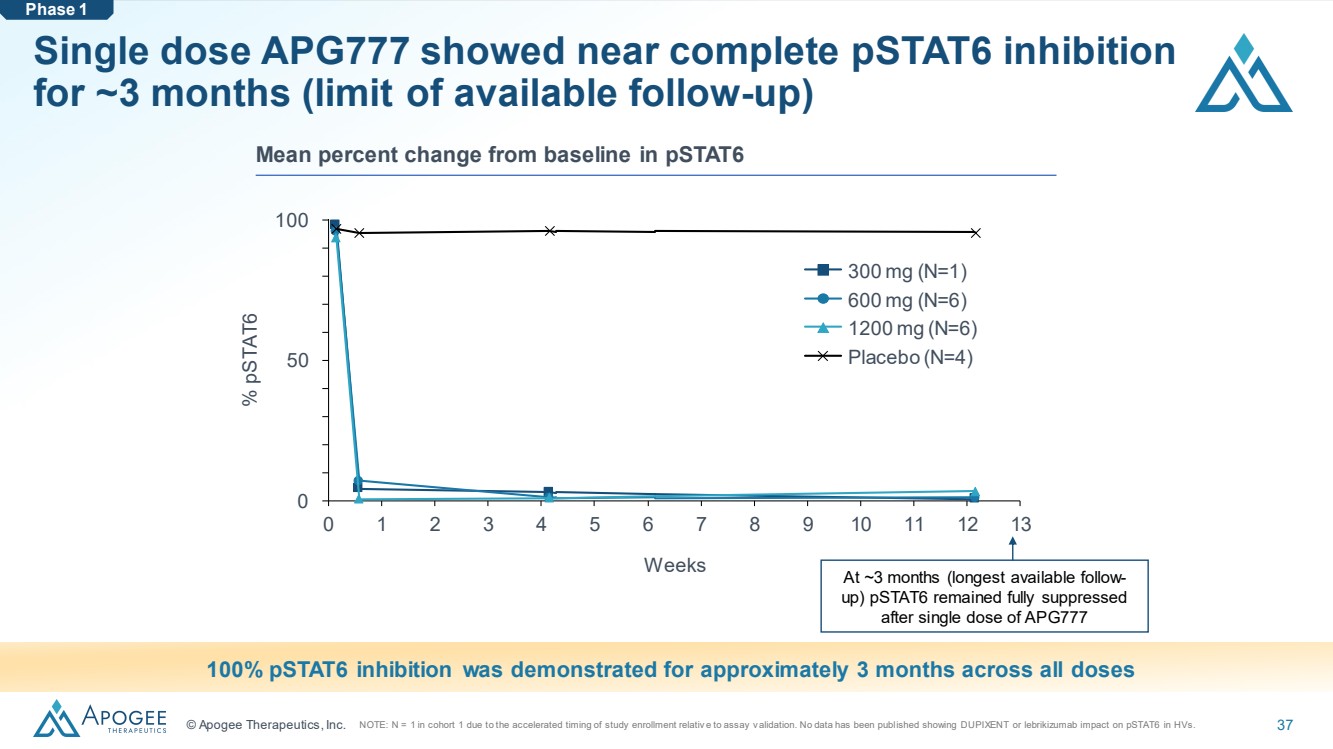
© Apogee Therapeutics, Inc. 37 Single dose APG777 showed near complete pSTAT6 inhibition for ~3 months (limit of available follow-up) 0 1 2 3 4 5 6 7 8 9 10 11 12 13 0 50 100 Weeks % pSTAT6 300 mg (N=1) 600 mg (N=6) 1200 mg (N=6) Placebo (N=4) 100% pSTAT6 inhibition was demonstrated for approximately 3 months across all doses Mean percent change from baseline in pSTAT6 Phase 1 At ~3 months (longest available follow-up) pSTAT6 remained fully suppressed after single dose of APG777 NOTE: N = 1 in cohort 1 due to the accelerated timing of study enrollment relativ e to assay v alidation. No data has been published showing DUPIXENT or lebrikizumab impact on pSTAT6 in HVs. |
|
Company Overview |
|
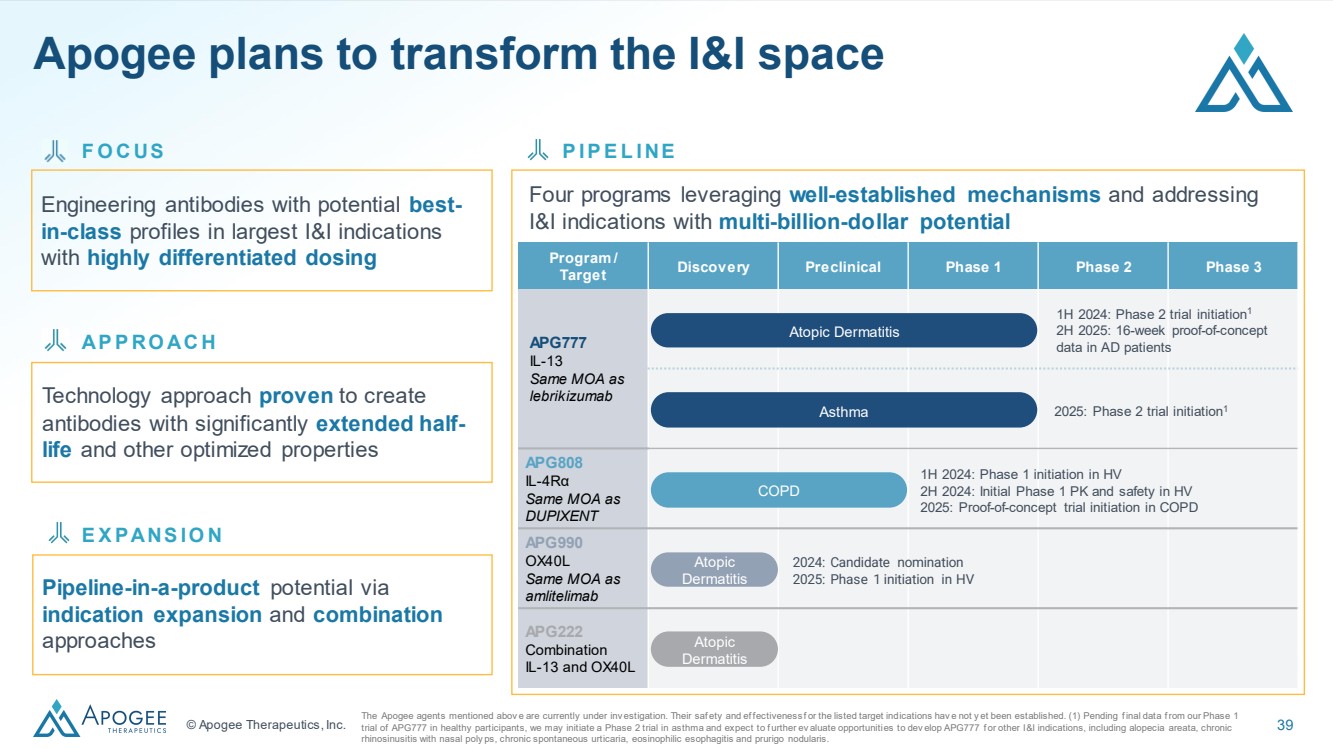
© Apogee Therapeutics, Inc. 39 Engineering antibodies with potential best-in-class profiles in largest I&I indications with highly differentiated dosing Four programs leveraging well-established mechanisms and addressing I&I indications with multi-billion-dollar potential Technology approach proven to create antibodies with significantly extended half-life and other optimized properties P I P E L I NE AP P RO AC H Program / Target Discovery Preclinical Phase 1 Phase 2 Phase 3 APG777 IL-13 Same MOA as lebrikizumab APG808 IL-4Rα Same MOA as DUPIXENT APG990 OX40L Same MOA as amlitelimab APG222 Combination IL-13 and OX40L Atopic Dermatitis Atopic Dermatitis 1H 2024: Phase 2 trial initiation1 2H 2025: 16-week proof-of-concept data in AD patients COPD 1H 2024: Phase 1 initiation in HV 2H 2024: Initial Phase 1 PK and safety in HV 2025: Proof-of-concept trial initiation in COPD Atopic Dermatitis 2024: Candidate nomination 2025: Phase 1 initiation in HV Asthma 2025: Phase 2 trial initiation1 The Apogee agents mentioned abov e are currently under inv estigation. Their saf ety and ef fectiveness f or the listed target indications hav e not y et been established. (1) Pending f inal data f rom our Phase 1 trial of APG777 in healthy participants, we may initiate a Phase 2 trial in asthma and expect to f urther ev aluate opportunities to dev elop APG777 f or other I&I indications, including alopecia areata, chronic rhinosinusitis with nasal poly ps, chronic spontaneous urticaria, eosinophilic esophagitis and prurigo nodularis. F O C US Pipeline-in-a-product potential via indication expansion and combination approaches E X PANS I O N Apogee plans to transform the I&I space |
|
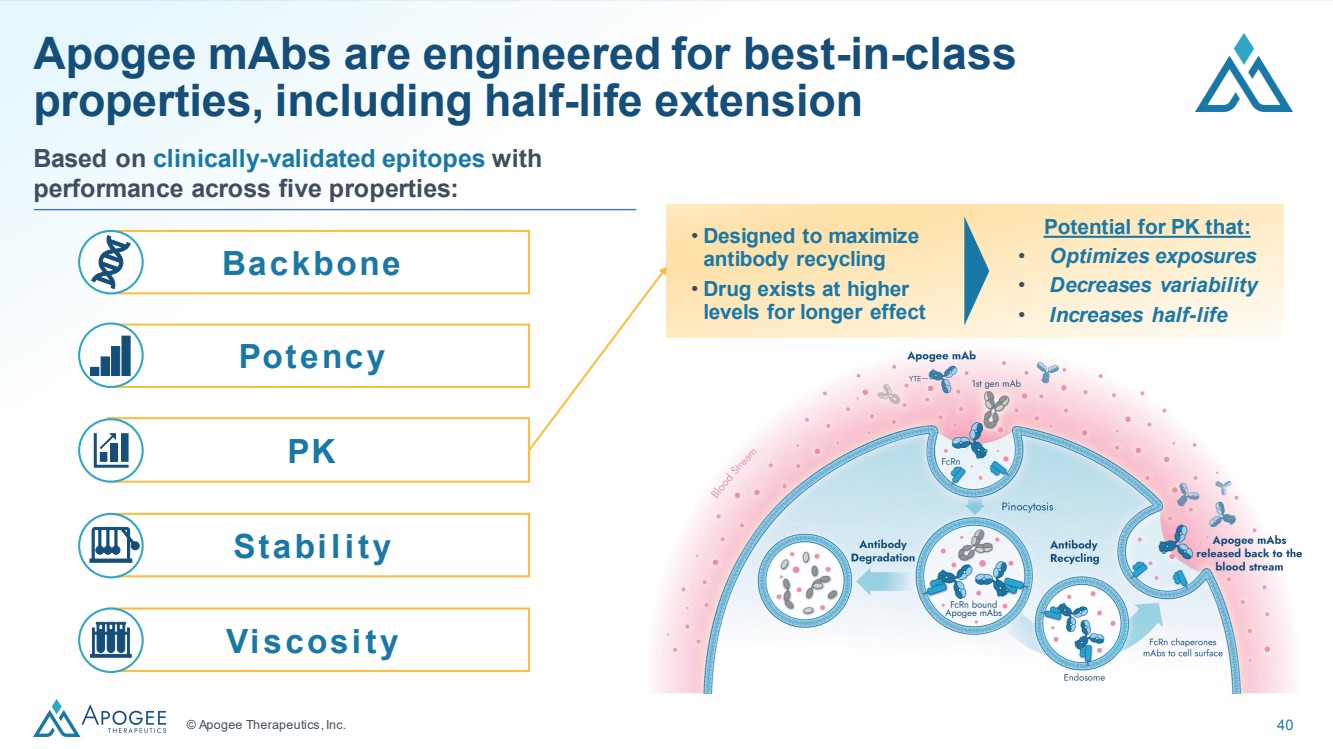
© Apogee Therapeutics, Inc. 40 Apogee mAbs are engineered for best-in-class properties, including half-life extension Potential for PK that: • Optimizes exposures • Decreases variability • Increases half-life • Designed to maximize antibody recycling • Drug exists at higher levels for longer effect Potency Viscosity PK Stability Backbone Based on clinically-validated epitopes with performance across five properties: |
|
APG777 |
|
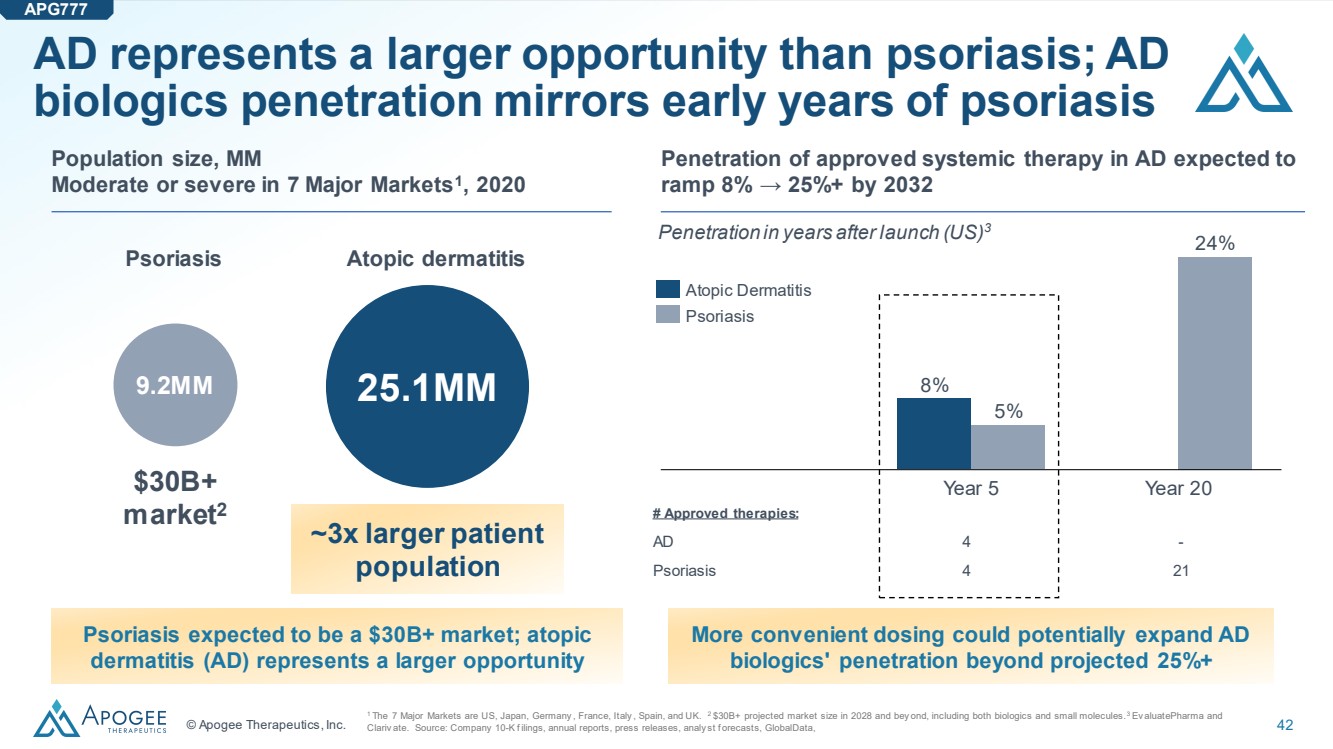
© Apogee Therapeutics, Inc. 42 AD represents a larger opportunity than psoriasis; AD biologics penetration mirrors early years of psoriasis 1 The 7 Major Markets are US, Japan, Germany , France, Italy , Spain, and UK. 2 $30B+ projected market size in 2028 and bey ond, including both biologics and small molecules. 3 Ev aluatePharma and Clariv ate. Source: Company 10-K f ilings, annual reports, press releases, analy st f orecasts, GlobalData, 9.2MM 25.1MM Population size, MM Moderate or severe in 7 Major Markets1 , 2020 Psoriasis Atopic dermatitis $30B+ market2 ~3x larger patient population Psoriasis expected to be a $30B+ market; atopic dermatitis (AD) represents a larger opportunity Year 5 Year 20 8% 5% 24% Atopic Dermatitis Psoriasis # Approved therapies: AD 4 - Psoriasis 4 21 Penetration in years after launch (US)3 Penetration of approved systemic therapy in AD expected to ramp 8% → 25%+ by 2032 More convenient dosing could potentially expand AD biologics' penetration beyond projected 25%+ APG777 |
|
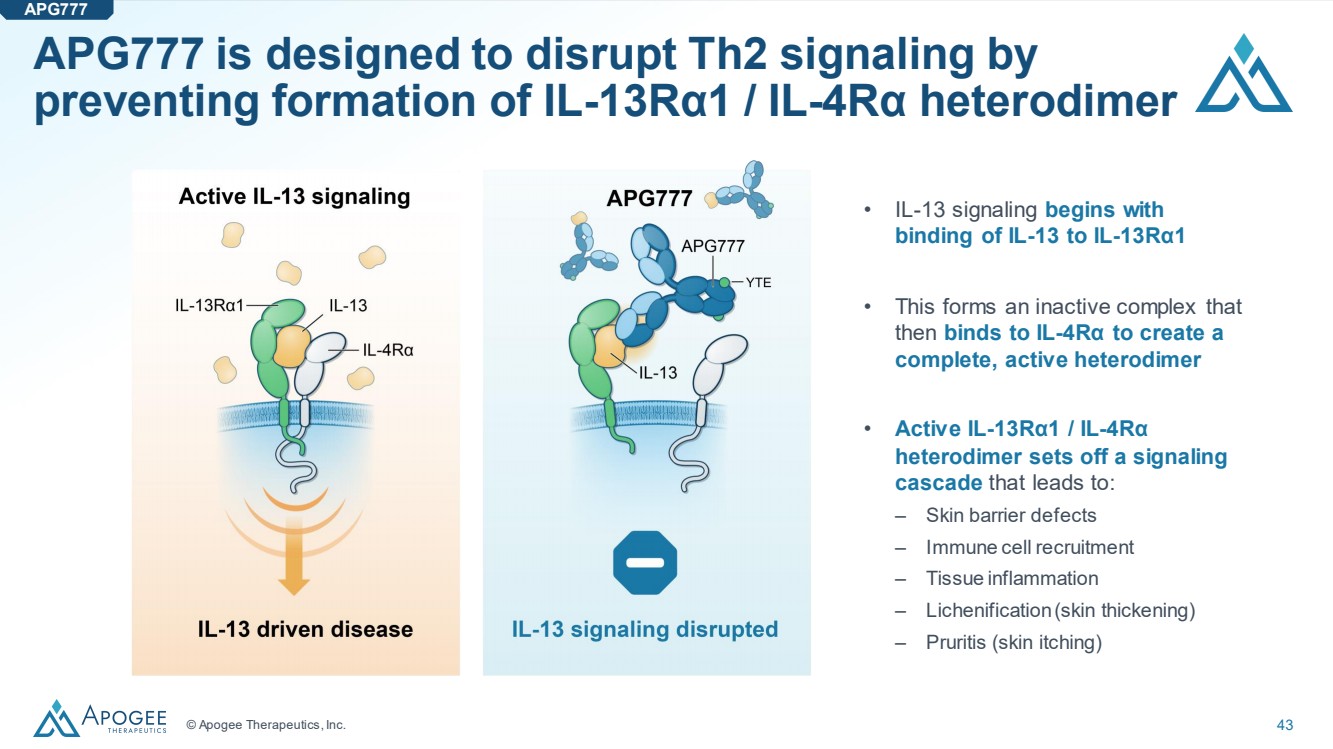
© Apogee Therapeutics, Inc. 43 APG777 is designed to disrupt Th2 signaling by preventing formation of IL-13Rα1 / IL-4Rα heterodimer • IL-13 signaling begins with binding of IL-13 to IL-13Rα1 • This forms an inactive complex that then binds to IL-4Rα to create a complete, active heterodimer • Active IL-13Rα1 / IL-4Rα heterodimer sets off a signaling cascade that leads to: ‒ Skin barrier defects ‒ Immune cell recruitment ‒ Tissue inflammation ‒ Lichenification(skin thickening) ‒ Pruritis (skin itching) APG777 |
|
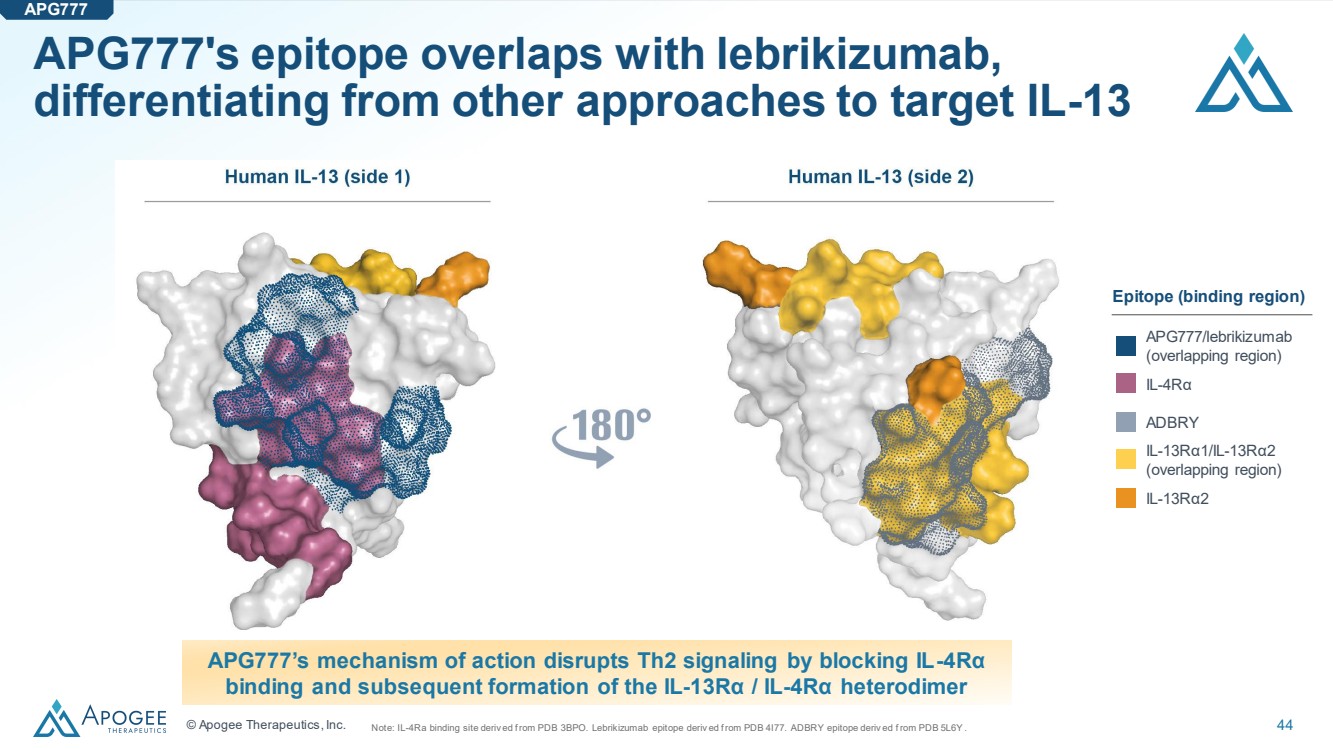
© Apogee Therapeutics, Inc. 44 APG777's epitope overlaps with lebrikizumab, differentiating from other approaches to target IL-13 Note: IL-4Ra binding site deriv ed f rom PDB 3BPO. Lebrikizumab epitope deriv ed f rom PDB 4I77. ADBRY epitope deriv ed f rom PDB 5L6Y . APG777’s mechanism of action disrupts Th2 signaling by blocking IL-4Rα binding and subsequent formation of the IL-13Rα / IL-4Rα heterodimer APG777/lebrikizumab (overlapping region) IL-4Rα ADBRY IL-13Rα1/IL-13Rα2 (overlapping region) IL-13Rα2 Epitope (binding region) APG777 |
|
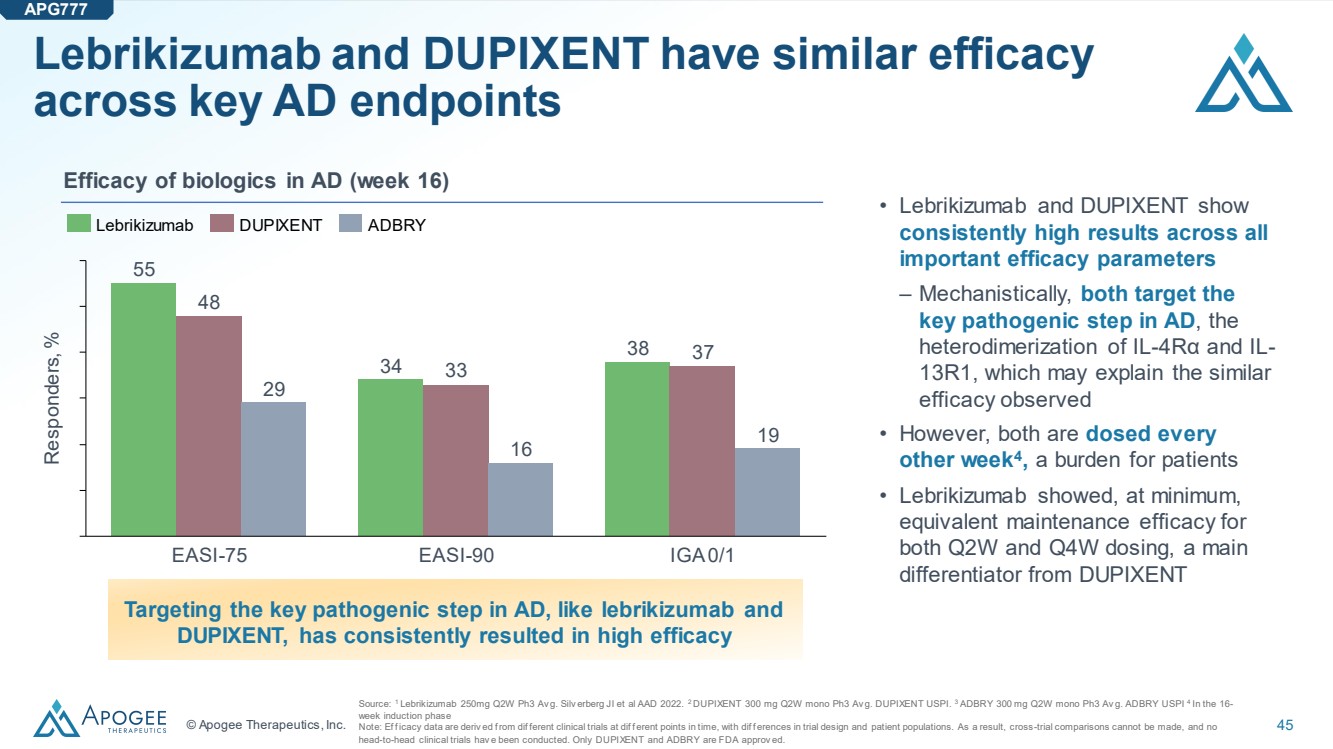
© Apogee Therapeutics, Inc. 45 Lebrikizumab and DUPIXENT have similar efficacy across key AD endpoints Source: 1 Lebrikizumab 250mg Q2W Ph3 Av g. Silv erberg JI et al AAD 2022. 2 DUPIXENT 300 mg Q2W mono Ph3 Av g. DUPIXENT USPI. 3 ADBRY 300 mg Q2W mono Ph3 Av g. ADBRY USPI 4 In the 16- week induction phase Note: Ef f icacy data are deriv ed f rom dif ferent clinical trials at dif f erent points in time, with dif f erences in trial design and patient populations. As a result, cross-trial comparisons cannot be made, and no head-to-head clinical trials hav e been conducted. Only DUPIXENT and ADBRY are FDA approv ed. Efficacy of biologics in AD (week 16) • Lebrikizumab and DUPIXENT show consistently high results across all important efficacy parameters – Mechanistically, both target the key pathogenic step in AD, the heterodimerization of IL-4Rα and IL-13R1, which may explain the similar efficacy observed • However, both are dosed every other week4 , a burden for patients • Lebrikizumab showed, at minimum, equivalent maintenance efficacy for both Q2W and Q4W dosing, a main differentiator from DUPIXENT Targeting the key pathogenic step in AD, like lebrikizumab and DUPIXENT, has consistently resulted in high efficacy APG777 55 34 38 48 33 37 29 16 19 Responders, % EASI-75 EASI-90 IGA 0/1 Lebrikizumab DUPIXENT ADBRY |
|
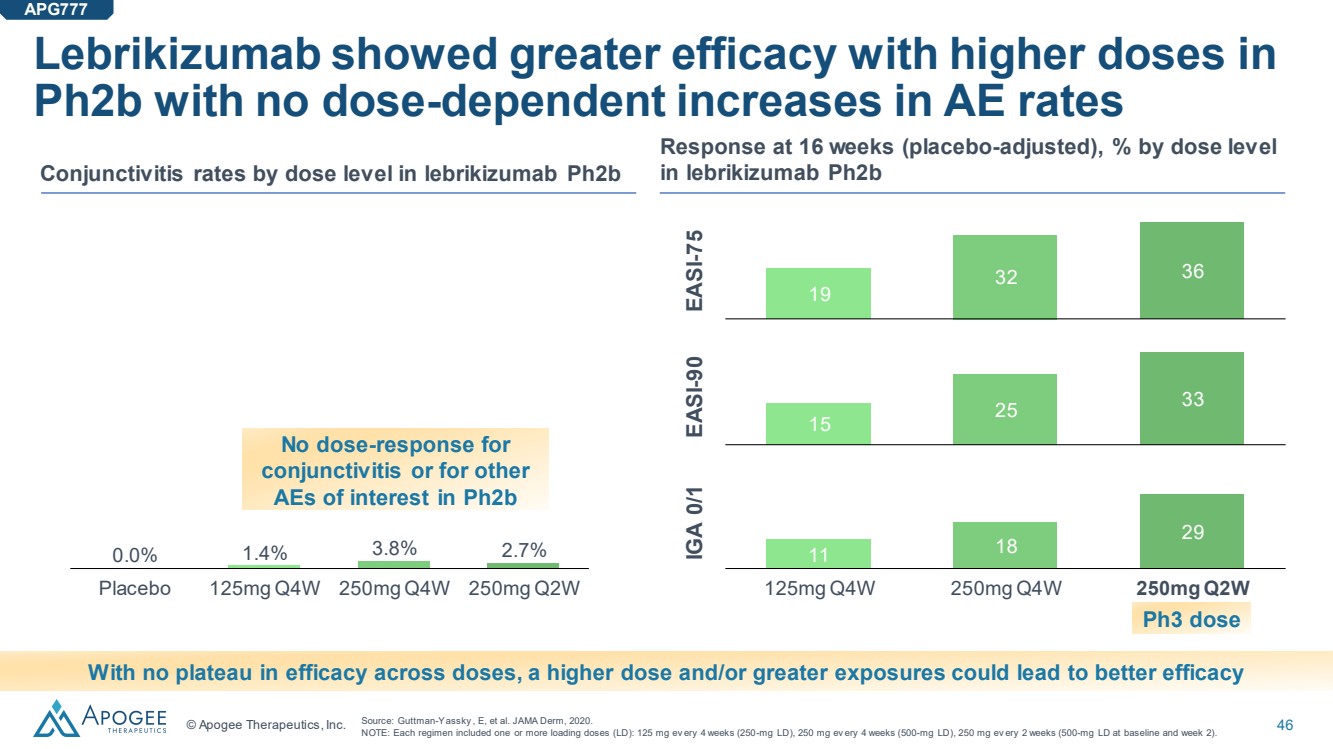
© Apogee Therapeutics, Inc. 46 Lebrikizumab showed greater efficacy with higher doses in Ph2b with no dose-dependent increases in AE rates Placebo 125mg Q4W 250mg Q4W 250mg Q2W 0.0% 1.4% 3.8% 2.7% Conjunctivitis rates by dose level in lebrikizumab Ph2b Response at 16 weeks (placebo-adjusted), % by dose level in lebrikizumab Ph2b With no plateau in efficacy across doses, a higher dose and/or greater exposures could lead to better efficacy Source: Guttman-Yassky , E, et al. JAMA Derm, 2020. NOTE: Each regimen included one or more loading doses (LD): 125 mg ev ery 4 weeks (250-mg LD), 250 mg ev ery 4 weeks (500-mg LD), 250 mg ev ery 2 weeks (500-mg LD at baseline and week 2). No dose-response for conjunctivitis or for other AEs of interest in Ph2b APG777 11 18 29 125mg Q4W 250mg Q4W 250mg Q2W EASI-75 EASI-90 IGA 0/1 15 25 33 19 32 36 Ph3 dose |
|
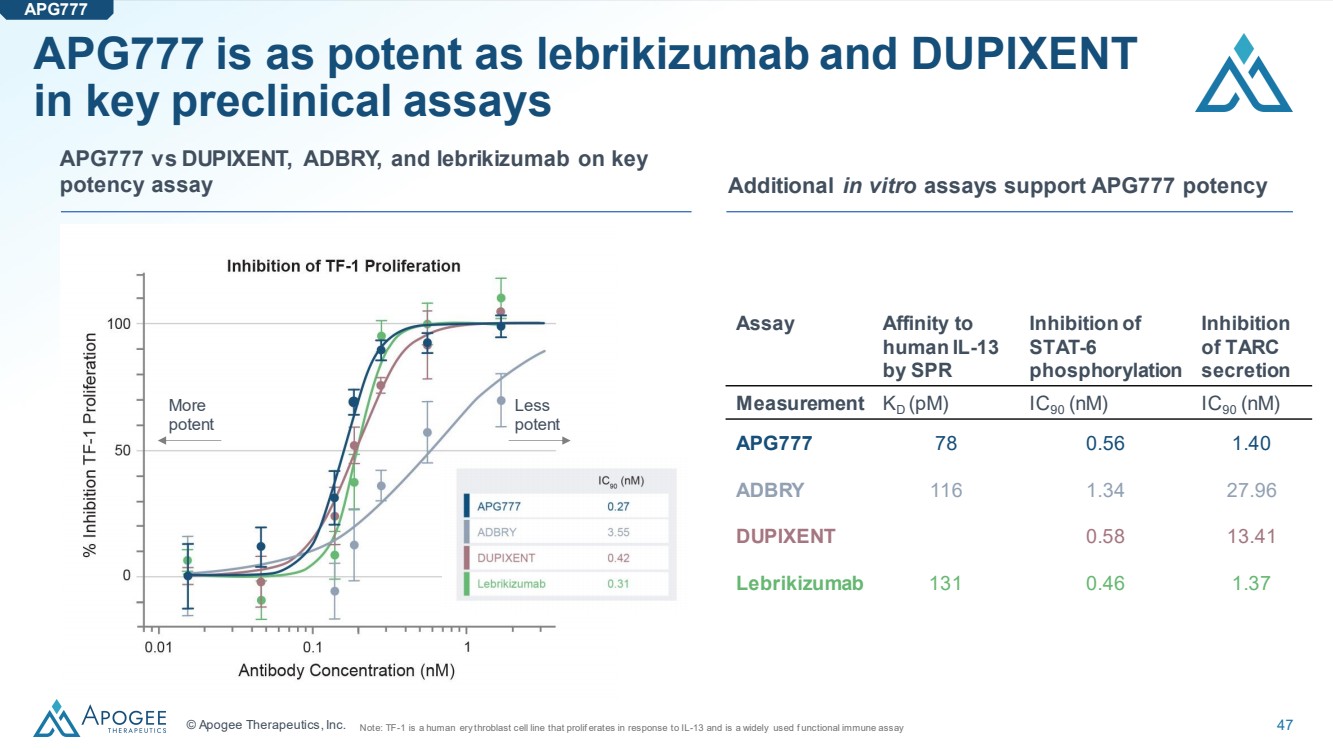
© Apogee Therapeutics, Inc. 47 APG777 is as potent as lebrikizumab and DUPIXENT in key preclinical assays More potent Less potent Assay Affinity to human IL-13 by SPR Inhibition of STAT-6 phosphorylation Inhibition of TARC secretion Measurement KD (pM) IC90 (nM) IC90 (nM) APG777 78 0.56 1.40 ADBRY 116 1.34 27.96 DUPIXENT 0.58 13.41 Lebrikizumab 131 0.46 1.37 Note: TF-1 is a human ery throblast cell line that prolif erates in response to IL-13 and is a widely used f unctional immune assay Additional in vitro assays support APG777 potency APG777 vs DUPIXENT, ADBRY, and lebrikizumab on key potency assay APG777 |
|
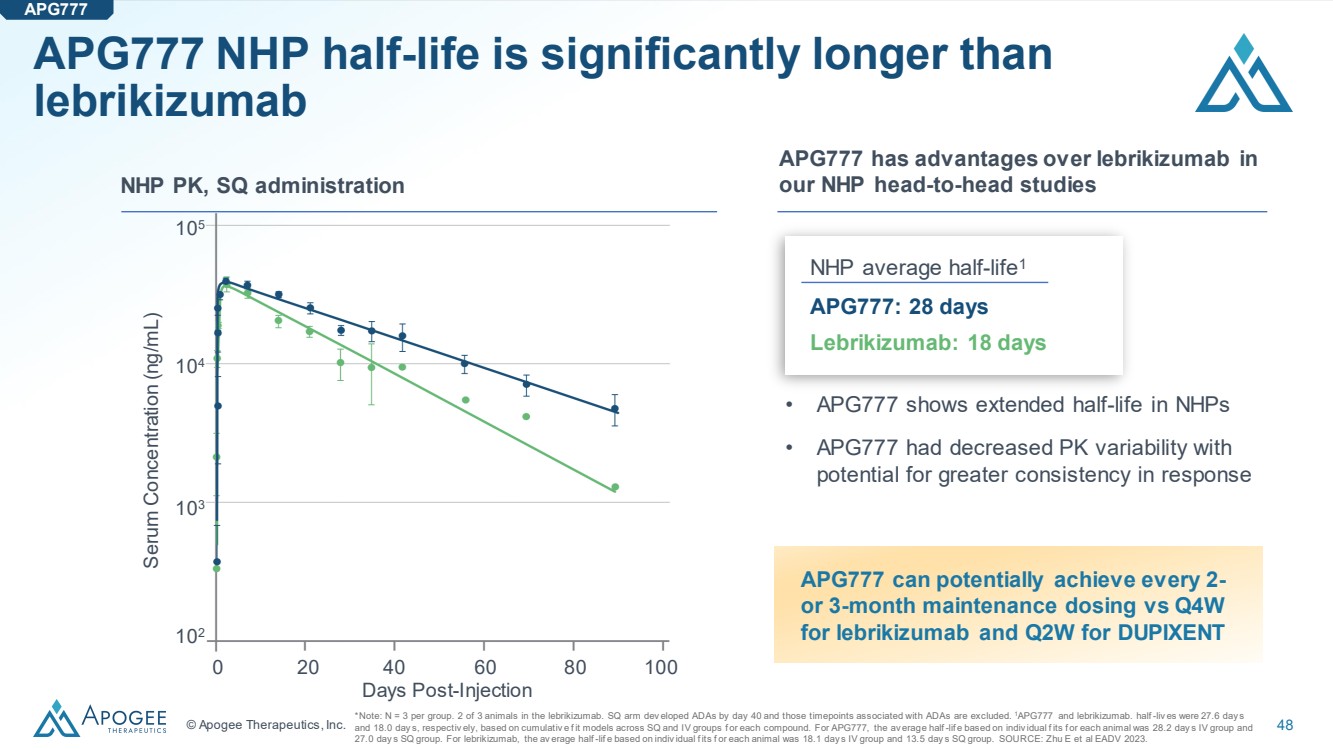
© Apogee Therapeutics, Inc. 48 APG777 NHP half-life is significantly longer than lebrikizumab *Note: N = 3 per group. 2 of 3 animals in the lebrikizumab. SQ arm dev eloped ADAs by day 40 and those timepoints associated with ADAs are excluded. 1APG777 and lebrikizumab. half -liv es were 27.6 day s and 18.0 day s, respectiv ely, based on cumulativ e f it models across SQ and IV groups f or each compound. For APG777, the av erage half -lif e based on indiv idual f its f or each animal was 28.2 day s IV group and 27.0 day s SQ group. For lebrikizumab, the av erage half -lif e based on indiv idual f its f or each animal was 18.1 day s IV group and 13.5 day s SQ group. SOURCE: Zhu E et al EADV 2023. Days Post-Injection 0 20 40 60 80 100 Serum Concentration (ng/mL) 102 103 104 105 APG777 has advantages over lebrikizumab in NHP PK, SQ administration our NHP head-to-head studies NHP average half-life1 APG777: 28 days Lebrikizumab: 18 days • APG777 shows extended half-life in NHPs • APG777 had decreased PK variability with potential for greater consistency in response APG777 APG777 can potentially achieve every 2- or 3-month maintenance dosing vs Q4W for lebrikizumab and Q2W for DUPIXENT |
|
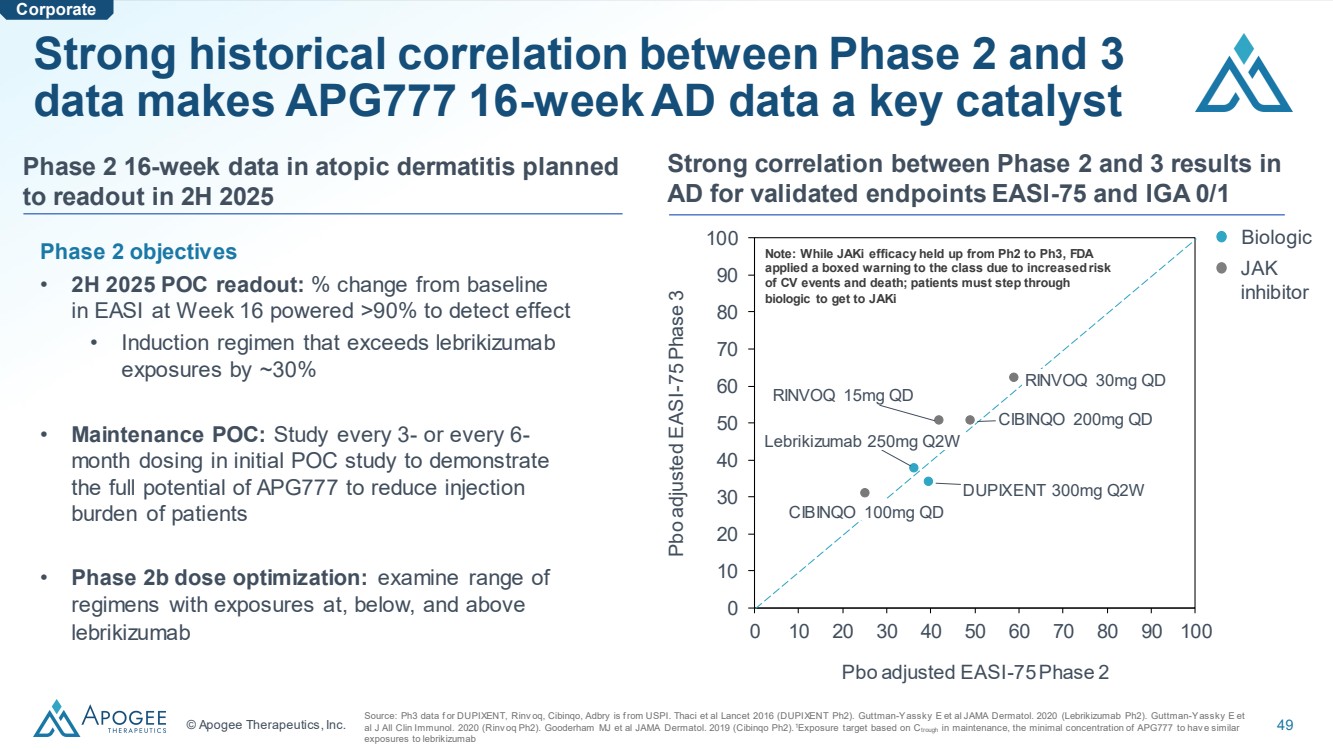
© Apogee Therapeutics, Inc. 49 Strong correlation between Phase 2 and 3 results in AD for validated endpoints EASI-75 and IGA 0/1 Strong historical correlation between Phase 2 and 3 data makes APG777 16-week AD data a key catalyst Source: Ph3 data f or DUPIXENT, Rinv oq, Cibinqo, Adbry is f rom USPI. Thaci et al Lancet 2016 (DUPIXENT Ph2). Guttman-Yassky E et al JAMA Dermatol. 2020 (Lebrikizumab Ph2). Guttman-Yassky E et al J All Clin Immunol. 2020 (Rinv oq Ph2). Gooderham MJ et al JAMA Dermatol. 2019 (Cibinqo Ph2).1Exposure target based on Ctrough in maintenance, the minimal concentration of APG777 to hav e similar exposures to lebrikizumab 0 10 20 30 40 50 60 70 80 90 100 0 10 20 30 40 50 60 70 80 90 100 Pbo adjusted EASI-75 Phase 2 Pbo adjusted EASI-75 Phase 3 DUPIXENT 300mg Q2W Lebrikizumab 250mg Q2W RINVOQ 15mg QD RINVOQ 30mg QD CIBINQO 100mg QD CIBINQO 200mg QD Biologic Note: While JAKi efficacy held up from Ph2 to Ph3, FDA applied a boxed warning to the class due to increased risk of CV events and death; patients must step through biologic to get to JAKi JAK inhibitor Phase 2 objectives • 2H 2025 POC readout: % change from baseline in EASI at Week 16 powered >90% to detect effect • Induction regimen that exceeds lebrikizumab exposures by ~30% • Maintenance POC: Study every 3- or every 6- month dosing in initial POC study to demonstrate the full potential of APG777 to reduce injection burden of patients • Phase 2b dose optimization: examine range of regimens with exposures at, below, and above lebrikizumab Phase 2 16-week data in atopic dermatitis planned to readout in 2H 2025 Corporate |
|
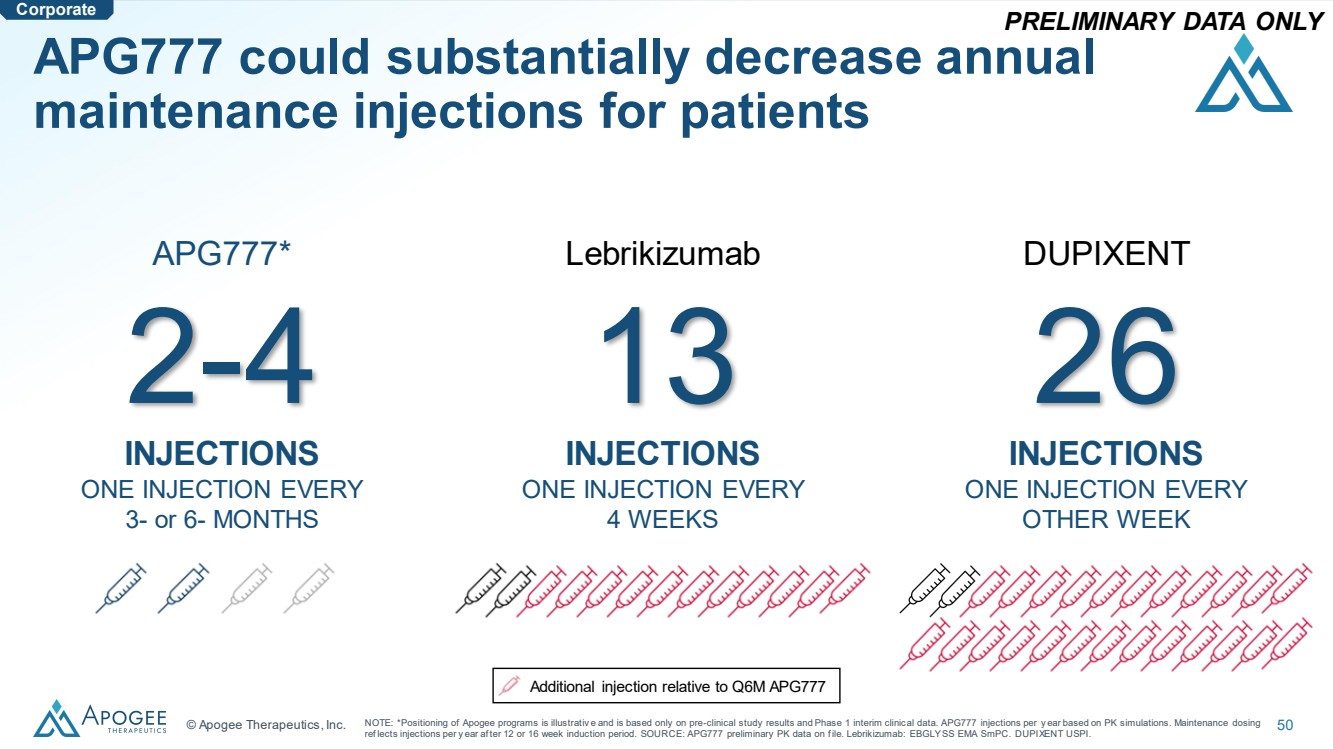
© Apogee Therapeutics, Inc. 50 APG777 could substantially decrease annual maintenance injections for patients Lebrikizumab 13 INJECTIONS ONE INJECTION EVERY 4 WEEKS DUPIXENT 26 INJECTIONS ONE INJECTION EVERY OTHER WEEK APG777* 2-4 INJECTIONS ONE INJECTION EVERY 3- or 6- MONTHS NOTE: *Positioning of Apogee programs is illustrativ e and is based only on pre-clinical study results and Phase 1 interim clinical data. APG777 injections per y ear based on PK simulations. Maintenance dosing ref lects injections per y ear af ter 12 or 16 week induction period. SOURCE: APG777 preliminary PK data on f ile. Lebrikizumab: EBGLYSS EMA SmPC. DUPIXENT USPI. PRELIMINARY DATA ONLY Additional injection relative to Q6M APG777 Corporate |
|
APG808 |
|
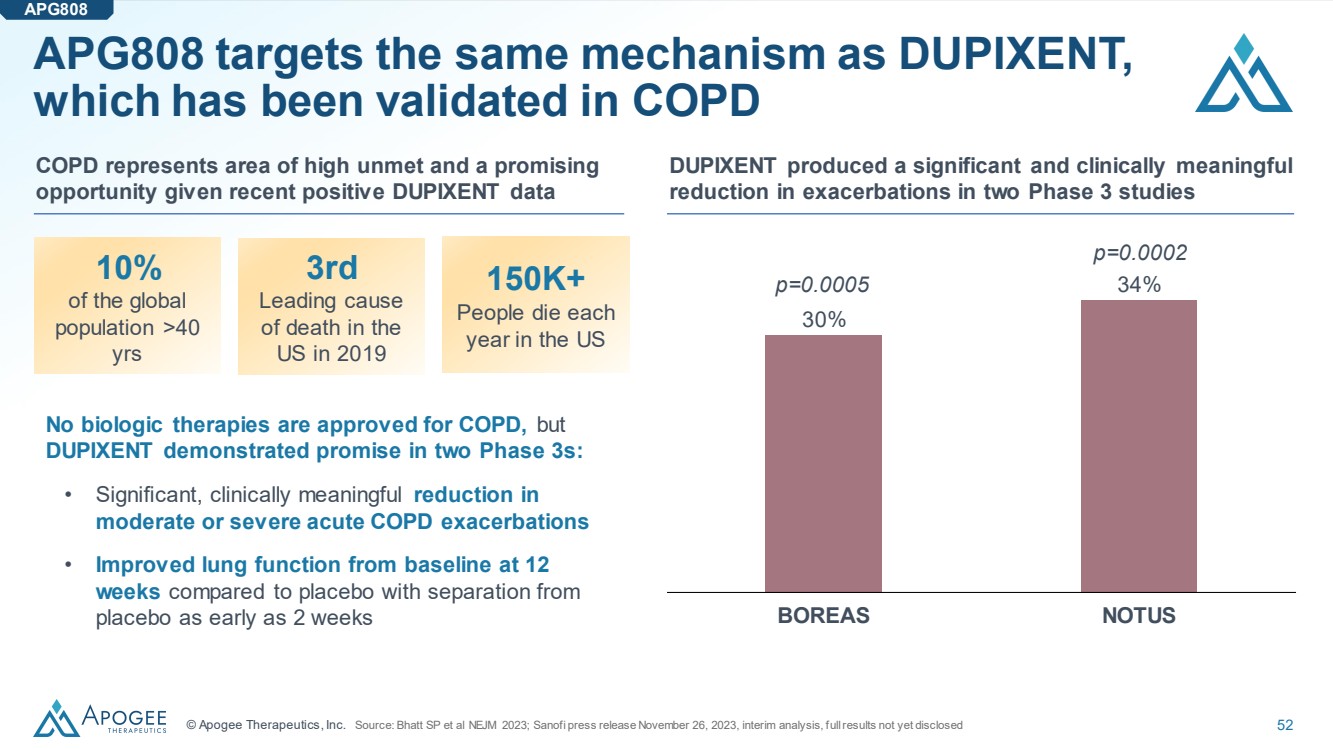
© Apogee Therapeutics, Inc. 52 APG808 targets the same mechanism as DUPIXENT, which has been validated in COPD COPD represents area of high unmet and a promising opportunity given recent positive DUPIXENT data 10% of the global population >40 yrs 3rd Leading cause of death in the US in 2019 150K+ People die each year in the US No biologic therapies are approved for COPD, but DUPIXENT demonstrated promise in two Phase 3s: • Significant, clinically meaningful reduction in moderate or severe acute COPD exacerbations • Improved lung function from baseline at 12 weeks compared to placebo with separation from placebo as early as 2 weeks APG808 DUPIXENT produced a significant and clinically meaningful reduction in exacerbations in two Phase 3 studies 30% 34% BOREAS NOTUS p=0.0002 p=0.0005 Source: Bhatt SP et al NEJM 2023; Sanofi press release November 26, 2023, interim analysis, full results not yet disclosed |
|
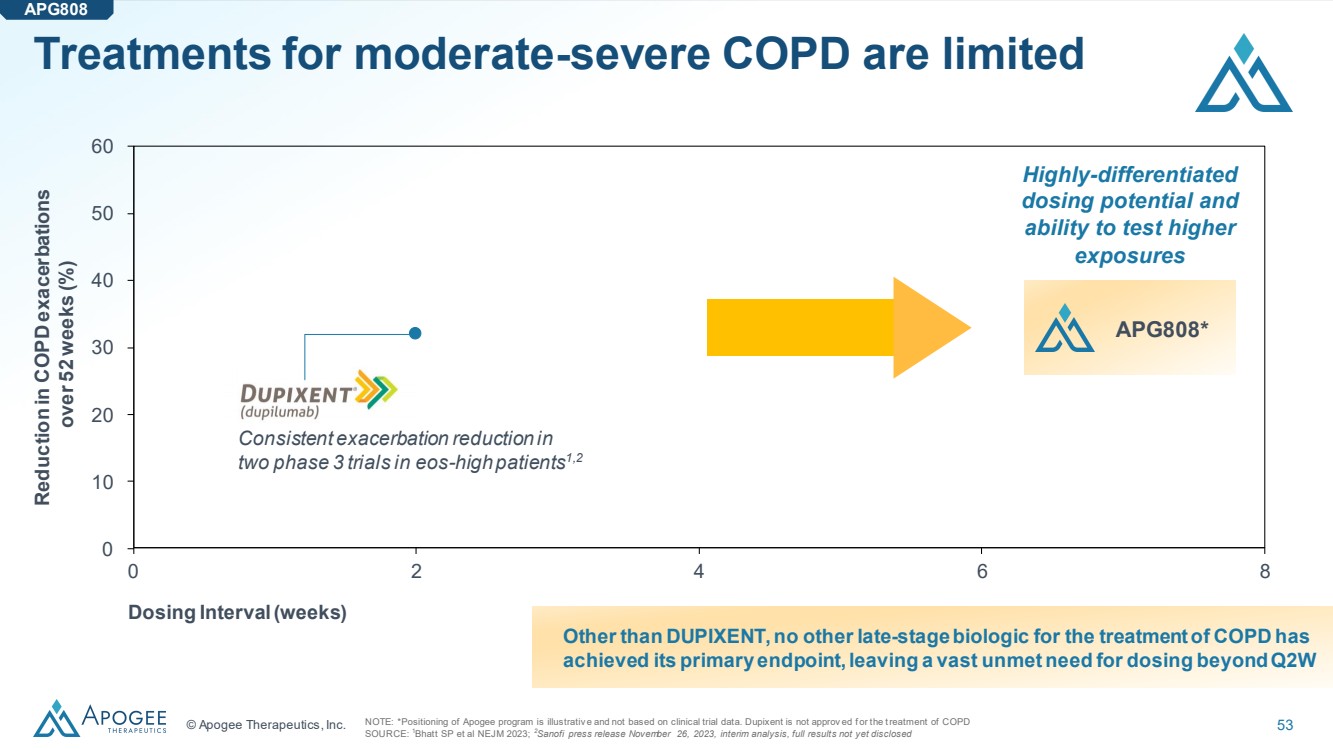
© Apogee Therapeutics, Inc. 53 Treatments for moderate-severe COPD are limited NOTE: *Positioning of Apogee program is illustrativ e and not based on clinical trial data. Dupixent is not approv ed f or the treatment of COPD SOURCE: 1Bhatt SP et al NEJM 2023; 2Sanofi press release November 26, 2023, interim analysis, full results not yet disclosed Other than DUPIXENT, no other late-stage biologic for the treatment of COPD has achieved its primary endpoint, leaving a vast unmet need for dosing beyond Q2W 0 2 4 6 8 30 40 20 50 10 60 0 Reduction in COPD exacerbations over 52 weeks (%) Dosing Interval(weeks) Highly-differentiated dosing potential and ability to test higher exposures APG808* Consistent exacerbation reduction in two phase 3 trials in eos-high patients1,2 APG808 |
|
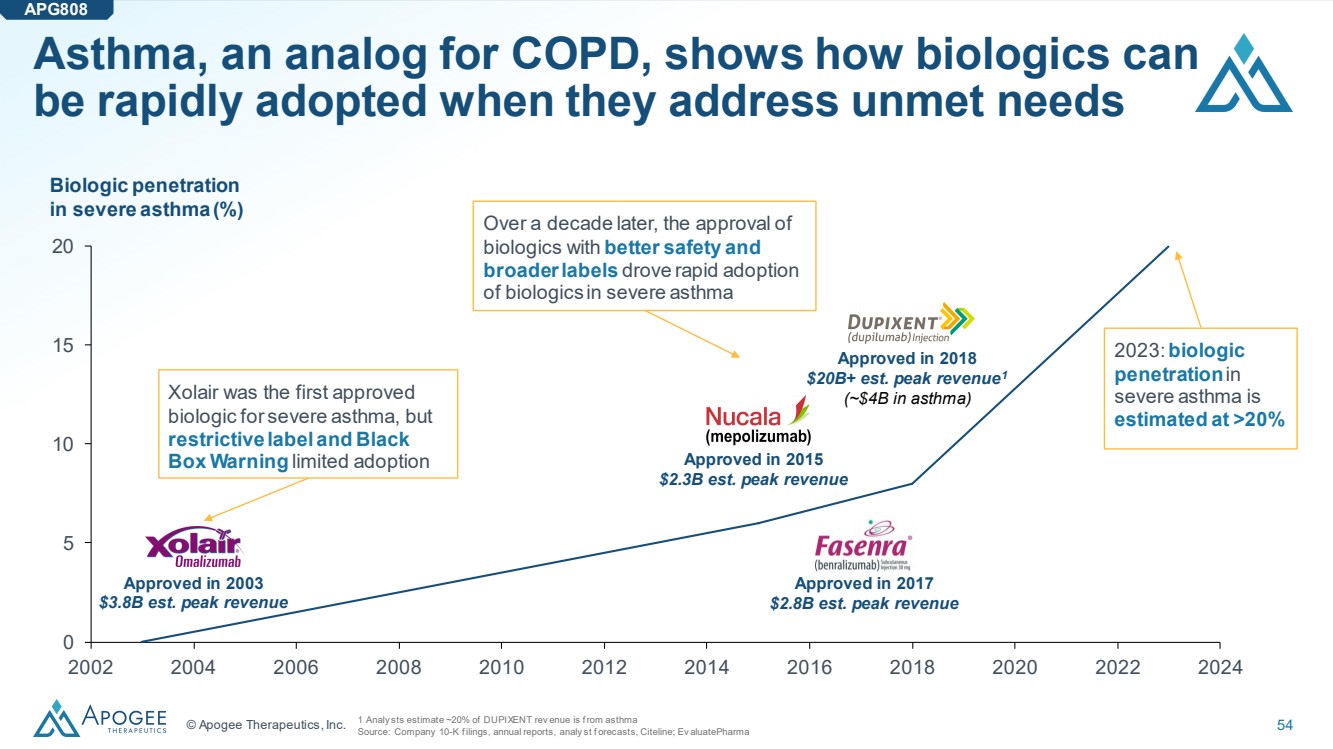
© Apogee Therapeutics, Inc. 54 Asthma, an analog for COPD, shows how biologics can be rapidly adopted when they address unmet needs 0 5 10 15 20 2002 2004 2006 2008 2010 2012 2014 2016 2018 2020 2022 2024 Biologic penetration in severe asthma (%) Approved in 2018 $20B+ est. peak revenue1 Xolair was the first approved (~$4B in asthma) biologic for severe asthma, but restrictive label and Black Box Warning limited adoption Over a decade later, the approval of biologics with better safety and broader labels drove rapid adoption of biologics in severe asthma 2023: biologic penetration in severe asthma is estimated at >20% 1 Analy sts estimate ~20% of DUPIXENT rev enue is f rom asthma Source: Company 10-K f ilings, annual reports, analy st f orecasts, Citeline; Ev aluatePharma APG808 Approved in 2017 $2.8B est. peak revenue Approved in 2015 $2.3B est. peak revenue Approved in 2003 $3.8B est. peak revenue |
|
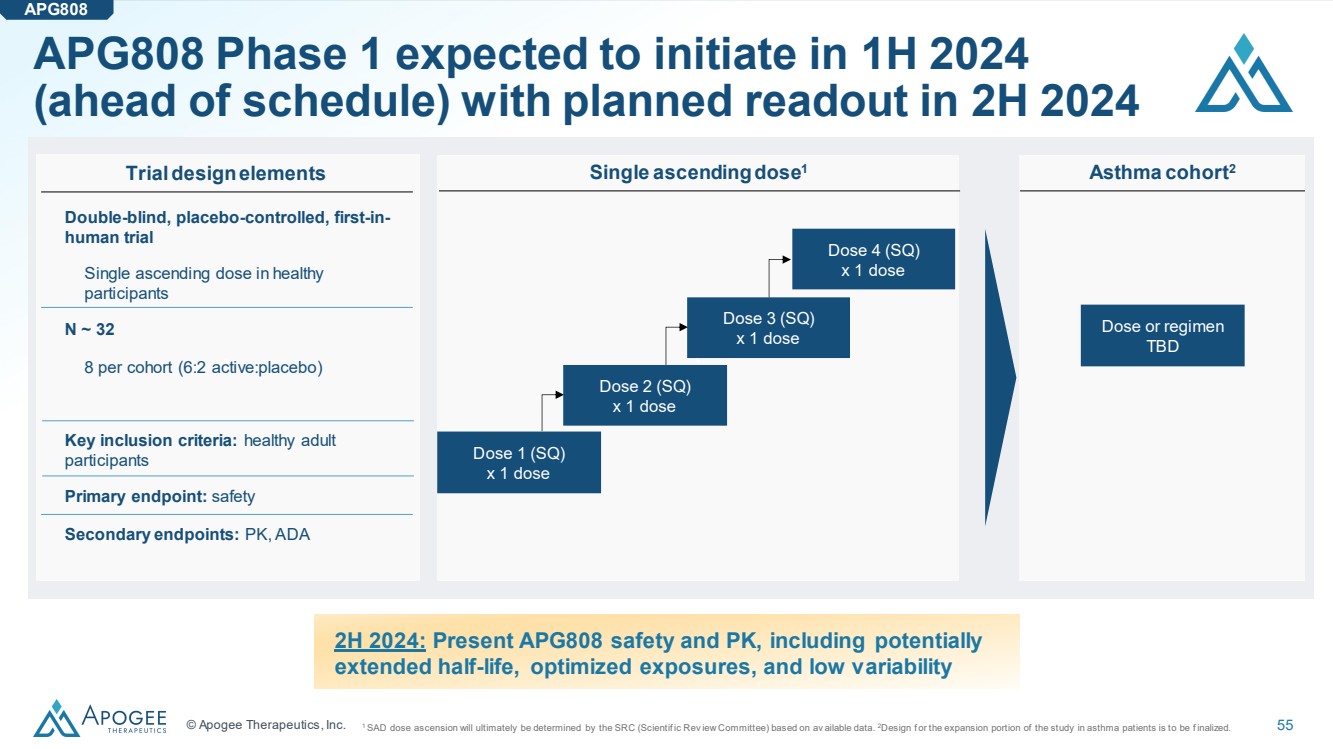
© Apogee Therapeutics, Inc. 55 APG808 Phase 1 expected to initiate in 1H 2024 (ahead of schedule) with planned readout in 2H 2024 1 SAD dose ascension will ultimately be determined by the SRC (Scientif ic Rev iew Committee) based on av ailable data. 2Design f or the expansion portion of the study in asthma patients is to be f inalized. 2H 2024: Present APG808 safety and PK, including potentially extended half-life, optimized exposures, and low variability APG808 ` ` Single ascendingdose1 Double-blind, placebo-controlled, first-in-human trial Single ascending dose in healthy participants N ~ 32 8 per cohort (6:2 active:placebo) Key inclusion criteria: healthy adult participants Primary endpoint: safety Secondary endpoints: PK, ADA Dose 1 (SQ) x 1 dose Dose 2 (SQ) x 1 dose Dose 3 (SQ) x 1 dose Trial design elements Dose 4 (SQ) x 1 dose ` Asthma cohort2 Dose or regimen TBD |
|
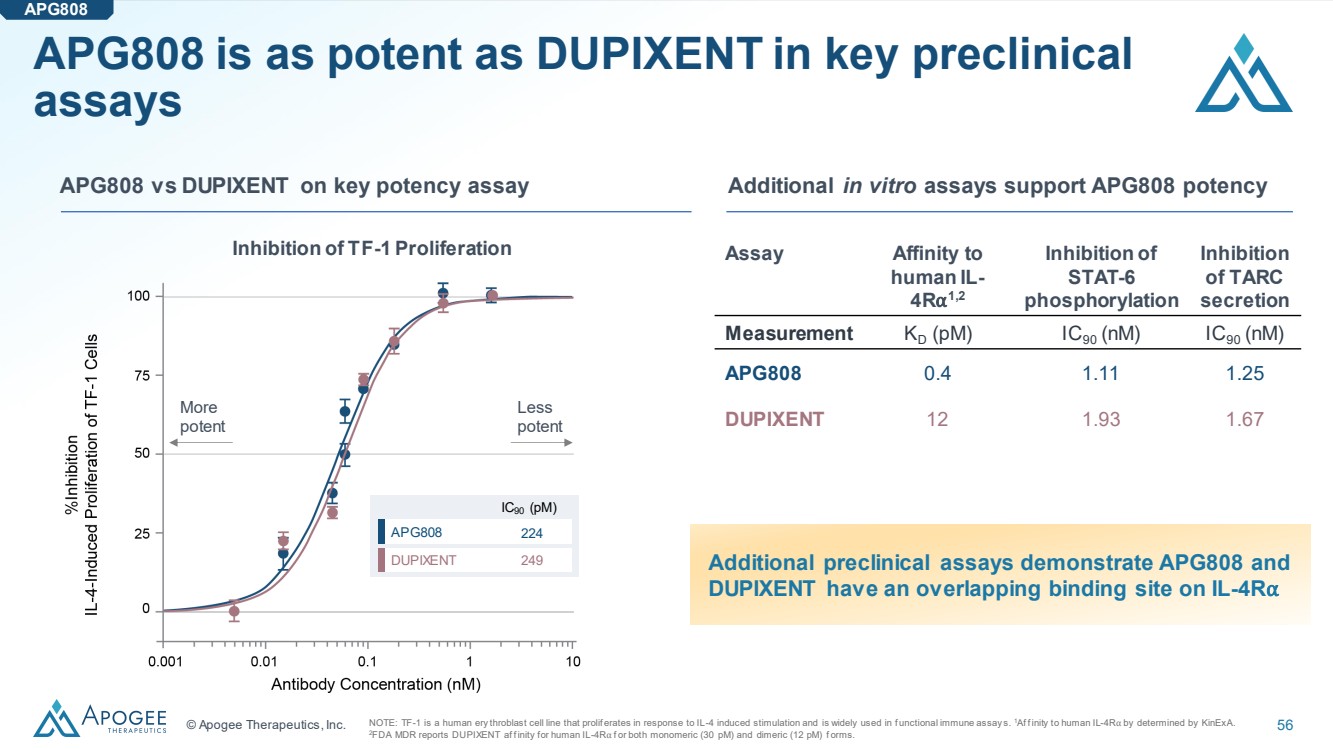
© Apogee Therapeutics, Inc. 56 APG808 is as potent as DUPIXENT in key preclinical assays APG808 APG808 vs DUPIXENT on key potency assay Additional in vitro assays support APG808 potency Assay Affinity to human IL-4R⍺ 1,2 Inhibition of STAT-6 phosphorylation Inhibition of TARC secretion Measurement KD (pM) IC90 (nM) IC90 (nM) APG808 0.4 1.11 1.25 DUPIXENT 12 1.93 1.67 NOTE: TF-1 is a human ery throblast cell line that prolif erates in response to IL-4 induced stimulation and is widely used in f unctional immune assay s. 1Af f inity to human IL-4R⍺ by determined by KinExA. 2FDA MDR reports DUPIXENT af f inity for human IL-4R⍺ f or both monomeric (30 pM) and dimeric (12 pM) f orms. More potent Less potent IC90 (pM) APG808 DUPIXENT 224 249 Inhibition of TF-1 Proliferation Additional preclinical assays demonstrate APG808 and DUPIXENT have an overlapping binding site on IL-4R⍺ |
|
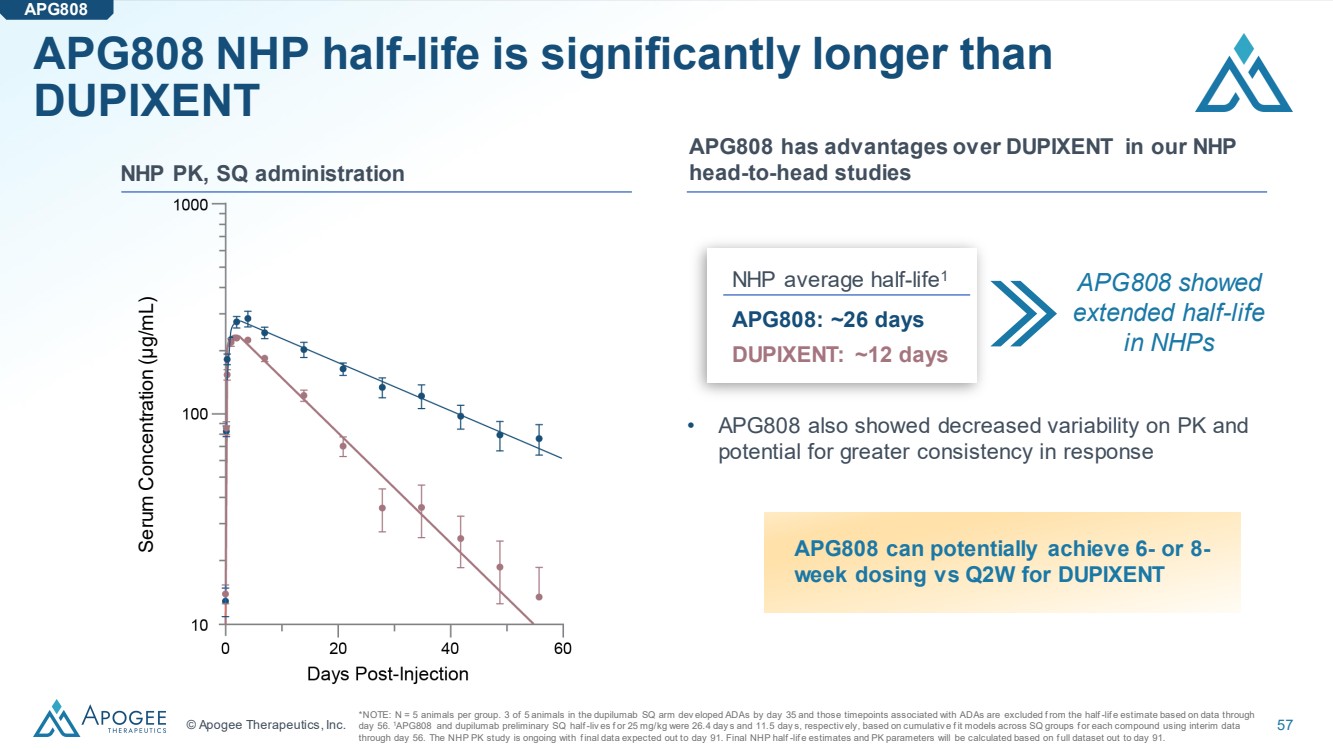
© Apogee Therapeutics, Inc. 57 APG808 NHP half-life is significantly longer than DUPIXENT APG808 APG808 has advantages over DUPIXENT in our NHP NHP PK, SQ administration head-to-head studies NHP average half-life1 APG808: ~26 days DUPIXENT: ~12 days APG808 showed extended half-life in NHPs *NOTE: N = 5 animals per group. 3 of 5 animals in the dupilumab SQ arm dev eloped ADAs by day 35 and those timepoints associated with ADAs are excluded f rom the half -lif e estimate based on data through day 56. 1APG808 and dupilumab preliminary SQ half -liv es f or 25 mg/kg were 26.4 day s and 11.5 day s, respectiv ely, based on cumulativ e f it models across SQ groups f or each compound using interim data through day 56. The NHP PK study is ongoing with f inal data expected out to day 91. Final NHP half -lif e estimates and PK parameters will be calculated based on f ull dataset out to day 91. Serum Concentration (µg/mL) APG808 can potentially achieve 6- or 8- week dosing vs Q2W for DUPIXENT • APG808 also showed decreased variability on PK and potential for greater consistency in response |
|
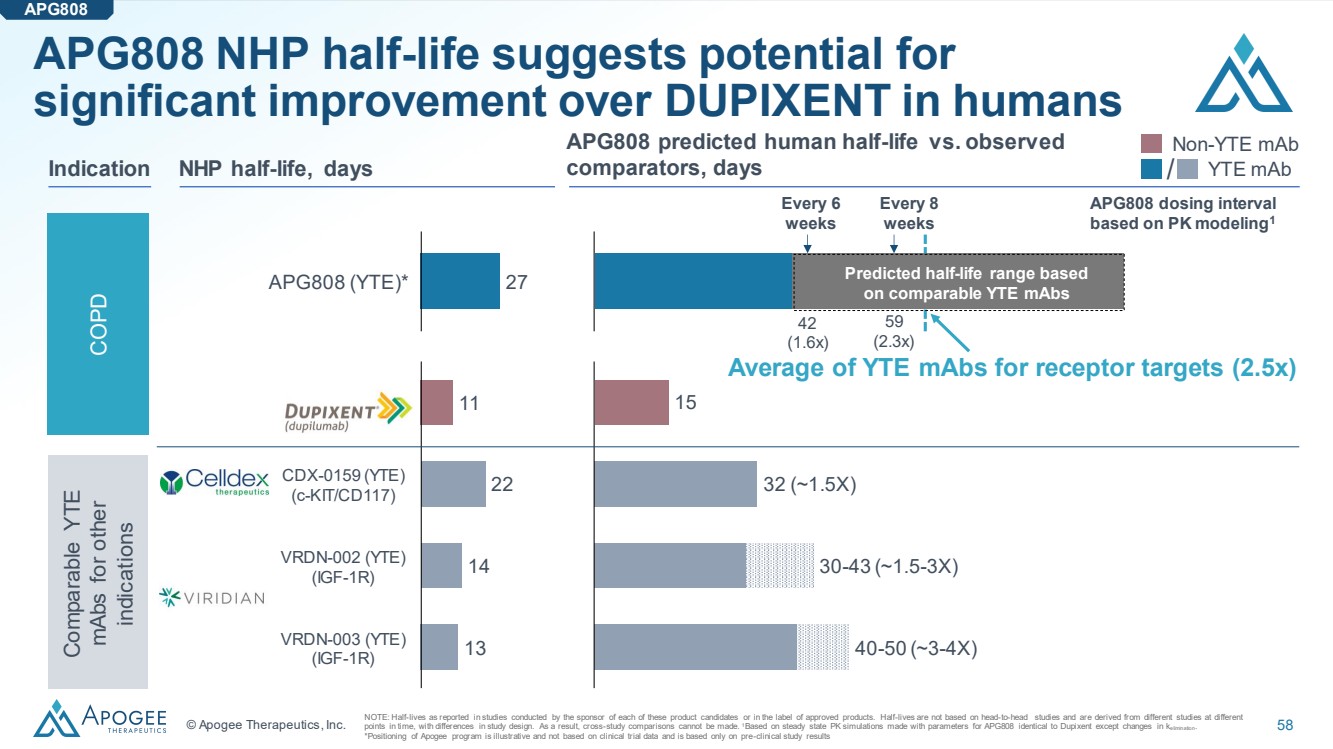
© Apogee Therapeutics, Inc. 58 APG808 (YTE)* 27 APG808 predicted human half-life vs. observed NHP half-life, days comparators, days 22 14 13 Dupixent CDX-0159 (YTE) (c-KIT/CD117) VRDN-002 (YTE) (IGF-1R) VRDN-003 (YTE) (IGF-1R) 11 15 32 (~1.5X) 30-43 (~1.5-3X) 40-50 (~3-4X) Non-YTE mAb Indication / YTE mAb COPD Comparable YTE mAbs for other indications APG808 NHP half-life suggests potential for significant improvement over DUPIXENT in humans APG808 NOTE: Half-lives as reported in studies conducted by the sponsor of each of these product candidates or in the label of approved products. Half-lives are not based on head-to-head studies and are derived from different studies at different points in time, with differences in study design. As a result, cross-study comparisons cannot be made. 1Based on steady state PK simulations made with parameters for APG808 identical to Dupixent except changes in kelimination. *Positioning of Apogee program is illustrative and not based on clinical trial data and is based only on pre-clinical study results Predicted half-life range based on comparable YTE mAbs Every 8 weeks Every 6 weeks APG808 dosing interval based on PK modeling1 42 (1.6x) 59 (2.3x) Average of YTE mAbs for receptor targets (2.5x) |
|
APG990/APG222 |
|
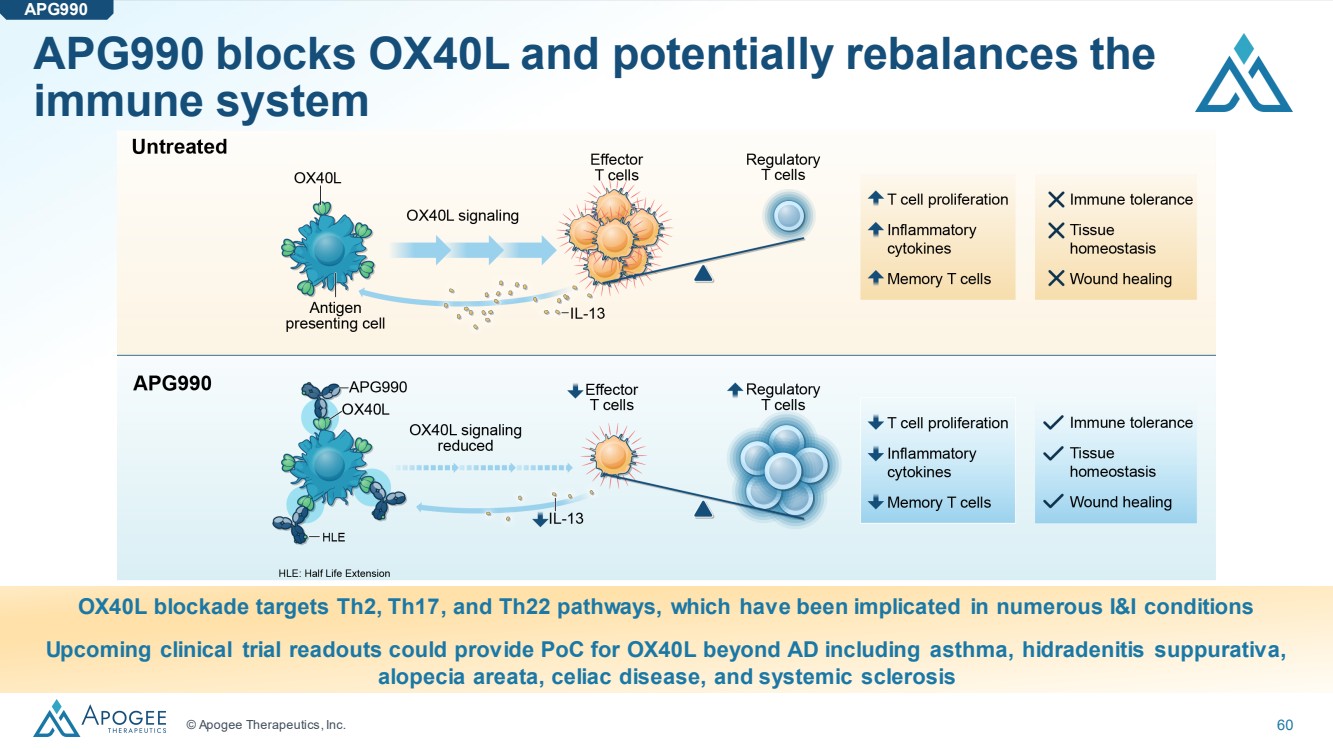
© Apogee Therapeutics, Inc. 60 APG990 blocks OX40L and potentially rebalances the immune system OX40L blockade targets Th2, Th17, and Th22 pathways, which have been implicated in numerous I&I conditions Upcoming clinical trial readouts could provide PoC for OX40L beyond AD including asthma, hidradenitis suppurativa, alopecia areata, celiac disease, and systemic sclerosis APG990 |
|
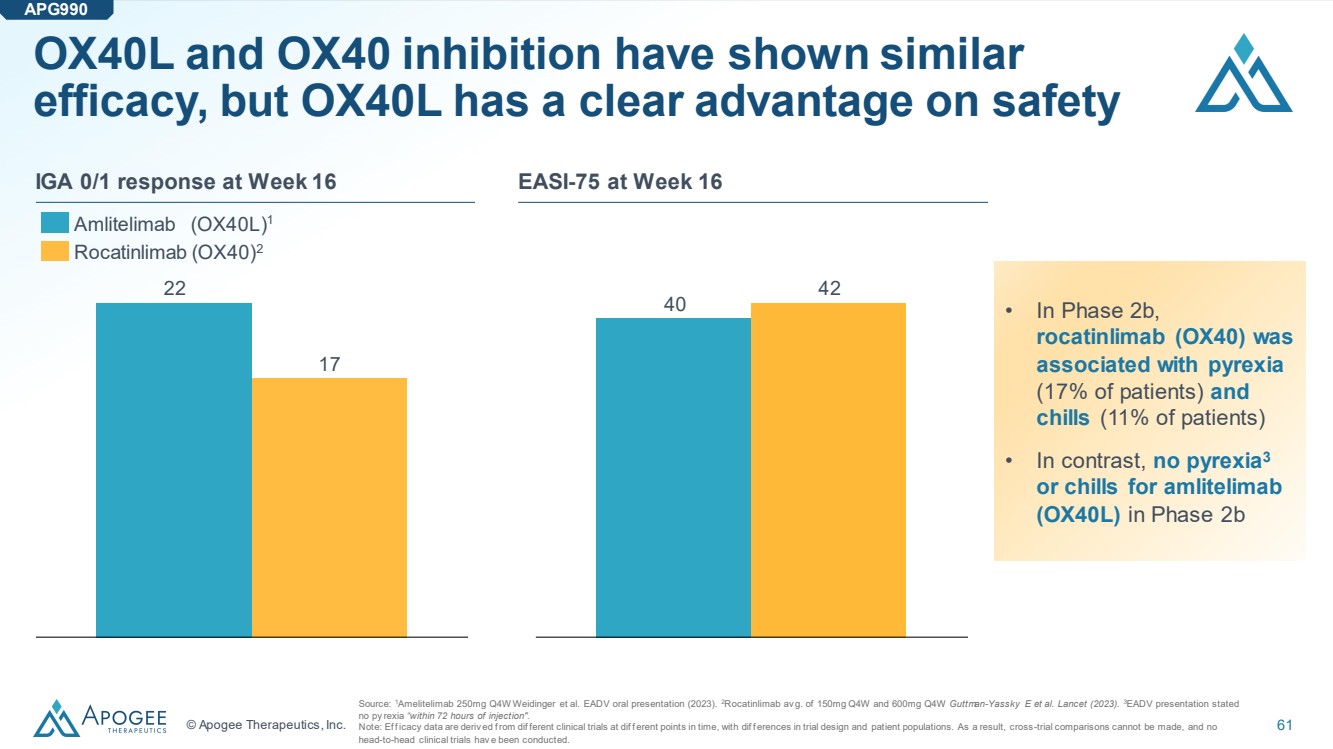
© Apogee Therapeutics, Inc. 61 OX40L and OX40 inhibition have shown similar efficacy, but OX40L has a clear advantage on safety 22 17 IGA 0/1 response at Week 16 Amlitelimab (OX40L)1 Rocatinlimab (OX40)2 40 42 EASI-75 at Week 16 APG990 • In Phase 2b, rocatinlimab (OX40) was associated with pyrexia (17% of patients) and chills (11% of patients) • In contrast, no pyrexia3 or chills for amlitelimab (OX40L) in Phase 2b Source: 1Amelitelimab 250mg Q4W Weidinger et al. EADV oral presentation (2023). 2Rocatinlimab av g. of 150mg Q4W and 600mg Q4W Guttman-Yassky E et al. Lancet (2023). 3EADV presentation stated no py rexia “within 72 hours of injection". Note: Ef f icacy data are deriv ed f rom dif ferent clinical trials at dif f erent points in time, with dif f erences in trial design and patient populations. As a result, cross-trial comparisons cannot be made, and no head-to-head clinical trials hav e been conducted. |
|
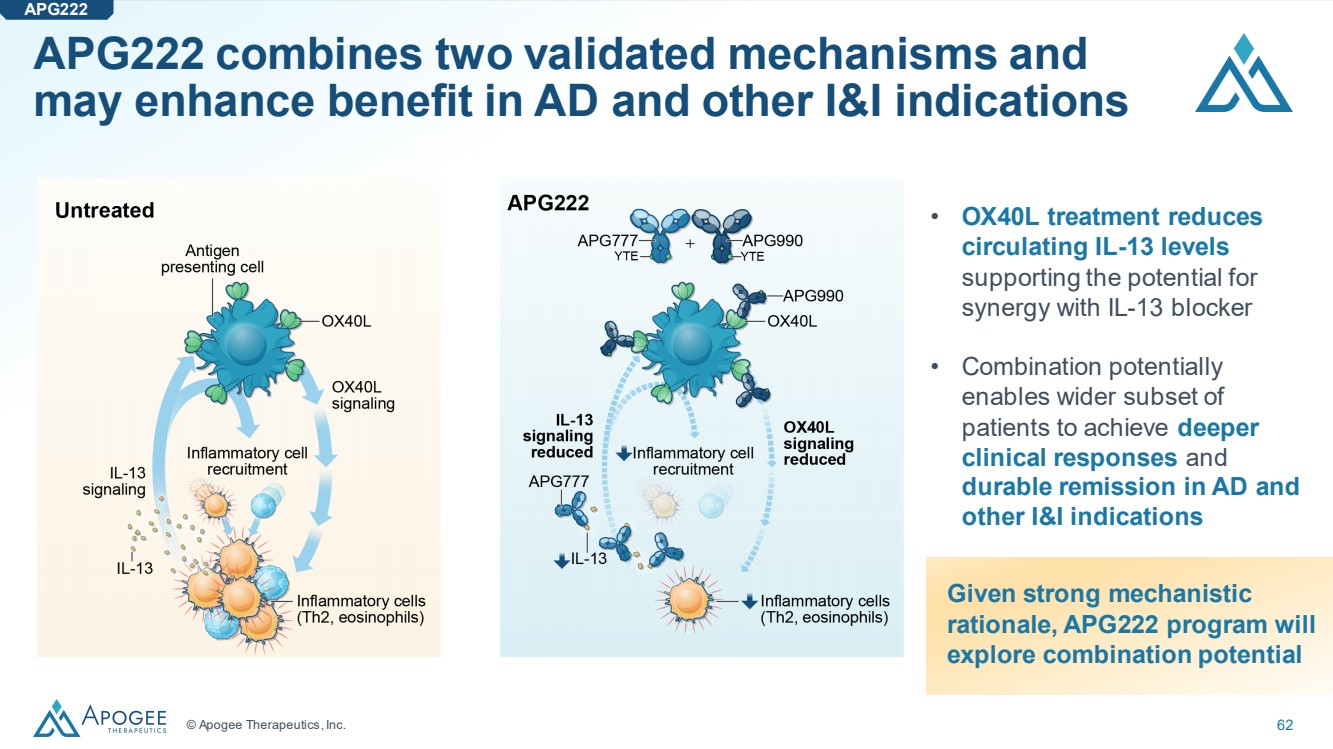
© Apogee Therapeutics, Inc. 62 • OX40L treatment reduces circulating IL-13 levels supporting the potential for synergy with IL-13 blocker • Combination potentially enables wider subset of patients to achieve deeper clinical responses and durable remission in AD and other I&I indications Given strong mechanistic rationale, APG222 program will explore combination potential APG222 combines two validated mechanisms and may enhance benefit in AD and other I&I indications APG222 |
|
Corporate |
|
© Apogee Therapeutics, Inc. 64 Michael Henderson, MD Chief Executive Officer, Director Carl Dambkowski, MD Chief Medical Officer Jane Pritchett Henderson Chief Financial Officer Rebecca Dabora, PhD Chief Technical Officer Matt Batters, JD General Counsel Wendy Aspden-Curran SVP of Clinical Operations Drew Badger, PhD SVP of Regulatory Affairs & Toxicology Dan Mulreany SVP of Business Development & Strategy Kristine Nograles, MD, MSc SVP of Clinical Development Corporate Experienced team with proven history of clinical development and commercial execution |
|
© Apogee Therapeutics, Inc. 65 Michael Henderson, MD CEO, Apogee Therapeutics BJ Jones CCO, NewAmsterdam Pharma Mark McKenna Chairman Peter Harwin Managing Member, Fairmount Jennifer Fox CFO & CBO, Zenas BioPharma Andrew Gottesdiener, MD Venrock Tomas Kiselak Managing Member, Fairmount Nimish Shah Venrock Corporate Board of Directors with industry-leading development, commercial and management expertise |
|
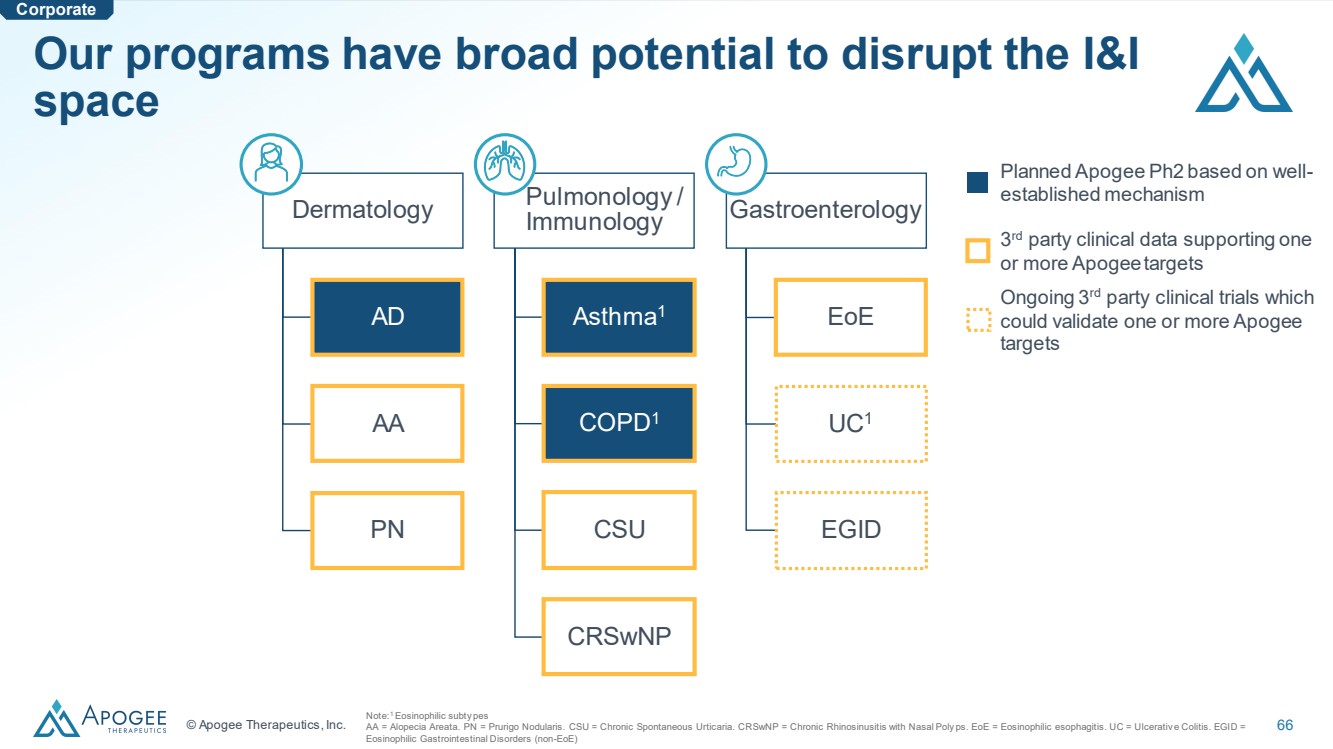
© Apogee Therapeutics, Inc. 66 Dermatology AD AA PN Pulmonology / Immunology Asthma1 COPD1 CSU CRSwNP Gastroenterology EoE UC1 EGID Planned Apogee Ph2 based on well-established mechanism 3 rd party clinical data supporting one or more Apogee targets Ongoing 3rd party clinical trials which could validate one or more Apogee targets Note:1 Eosinophilic subty pes AA = Alopecia Areata. PN = Prurigo Nodularis. CSU = Chronic Spontaneous Urticaria. CRSwNP = Chronic Rhinosinusitis with Nasal Poly ps. EoE = Eosinophilic esophagitis. UC = Ulcerativ e Colitis. EGID = Eosinophilic Gastrointestinal Disorders (non-EoE) Corporate Our programs have broad potential to disrupt the I&I space |
|
Apogee /ˈapəjē/ noun The highest point in the development of something; a climax or culmination |