UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, DC 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934
Date of Report (Date of earliest event reported): May 22, 2023
Hepion Pharmaceuticals, Inc.
(Exact name of registrant as specified in its charter)
| Delaware | 001-36856 | 46-2783806 | ||
| (State or other jurisdiction of incorporation or organization) |
(Commission File Number) |
IRS Employer Identification No.) |
399
Thornall Street, First Floor
Edison, NJ 08837
(Address of principal executive offices)
Registrant’s telephone number, including area code: (732) 902-4000
(Former name or former address, if changed since last report)
Securities registered pursuant to Section 12(b) of the Act:
| Title of each class: | Trading Symbol(s) | Name of each exchange on which registered: | ||
| Common Stock | HEPA | Nasdaq Capital Market |
Check the appropriate box below if the Form 8-K filing is intended to simultaneously satisfy the filing obligation of the registrant under any of the following provisions:
¨ Written communication pursuant to Rule 425 under the Securities Act (17 CFR 230.425)
¨ Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12)
¨ Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b))
¨ Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c))
Indicate by check mark whether the registrant is an emerging growth company as defined in as defined in Rule 405 of the Securities Act of 1933 (§230.405 of this chapter) or Rule 12b-2 of the Securities Exchange Act of 1934 (§240.12b-2 of this chapter). Emerging growth company ¨
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ¨
| Item 7.01 | Regulation FD Disclosure |
Hepion Pharmaceuticals, Inc. (the “Company”) intends to conduct meetings with third parties in which its corporate slide presentation will be presented. A copy of the presentation materials is attached as Exhibit 99.1 to this Current Report on Form 8-K and is incorporated herein by reference.
The information in this Item 7.01 and the document attached as Exhibit 99.1 is being furnished and shall not be deemed “filed” for purposes of Section 18 of the Securities and Exchange Act of 1934, as amended (the “Exchange Act”), nor otherwise subject to the liabilities of that section, nor incorporated by reference in any filing under the Securities Act of 1933 or the Exchange Act, except as shall be expressly set forth by specific reference in such a filing.
| Item 8.01 | Other Events |
On May 22, 2023, the Company issued a press release announcing positive topline results from its recently completed Phase 2 ALTITUDE-NASH clinical trial. A copy of the press release is furnished as Exhibit 99.2 to this Form 8-K.
| Item 9.01 | Financial Statements and Exhibits |
(d) Exhibits
| 99.1 | Hepion Pharmaceuticals, Inc. Corporate Presentation |
| 99.2 | Press Release of Hepion Pharmaceuticals, Inc. |
| 104 | Cover Page Interactive Data File - the cover page iXBRL tags are embedded within the inline XBRL document. |
| - |
SIGNATURE
Pursuant to the requirements of the Securities Exchange Act of 1934, the Registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
Dated: May 22, 2023
| HEPION PHARMACEUTICALS, INC. | ||
| By: | /s/ Robert Foster | |
| Robert Foster | ||
| Chief Executive Officer | ||
| - |
|
1 1 Rencofilstat (CRV431): A Novel Drug Candidate for NASH, Fibrosis, and HCC May 2023 Creating a Therapeutic Ecosystem NASDAQ:HEPA |
|
2 This presentation may contain forward-looking statements within the meaning of Section 27A of the Securities Act of 1933 and Section 21E of the Securities Exchange Act of 1934. Such forward-looking statements are characterized by future or conditional verbs such as “may,” “will,” “expect,” “intend,” “anticipate,” believe,” “estimate” and “continue” or similar words. You should read statements that contain these words carefully because they discuss future expectations and plans, which contain projections of future results of operations or financial condition or state other forward-looking information. Such statements are only predictions, and our actual results may differ materially from those anticipated in these forward-looking statements. We believe that it is important to communicate future expectations to investors. However, there may be events in the future that we are not able to accurately predict or control. Factors that may cause such differences include, but are not limited to, those discussed under Risk Factors in our periodic reports filed with the Securities and Exchange Commission, including the uncertainties associated with product development, the risk that products that appeared promising in early clinical trials do not demonstrate safety and efficacy in larger-scale clinical trials, the risk that we will not obtain approval to market our products, risks associated with delays, increased costs and funding shortages caused by the COVID-19 pandemic; the risks associated with dependence upon key personnel and the need for additional financing. We do not assume any obligation to update forward-looking statements as circumstances change. This presentation does not constitute an offer or invitation for the sale or purchase of securities or to engage in any other transaction with Hepion Pharmaceuticals or its affiliates. The information in this presentation is not targeted at the residents of any particular country or jurisdiction and is not intended for distribution to, or use by, any person in any jurisdiction or country where such distribution or use would be contrary to local law or regulation. Statements Forward-Looking |
|
3 Rencofilstat Anti-Fibrotic Drug Candidate • Novel mechanism - cyclophilin inhibition • Once-daily, oral medication – soft gel capsules • Collagen-specific anti-fibrotic • Targets key pathologies including fibrosis, inflammation, cell injury • All clinical trials to date show rencofilstat to be well tolerated – over 425 subjects dosed • Currently undergoing Phase 2 clinical trials Rencofilstat Highlights |
|
4 NASH Fibrotic Liver Disease Leading Indication for Rencofilstat |
|
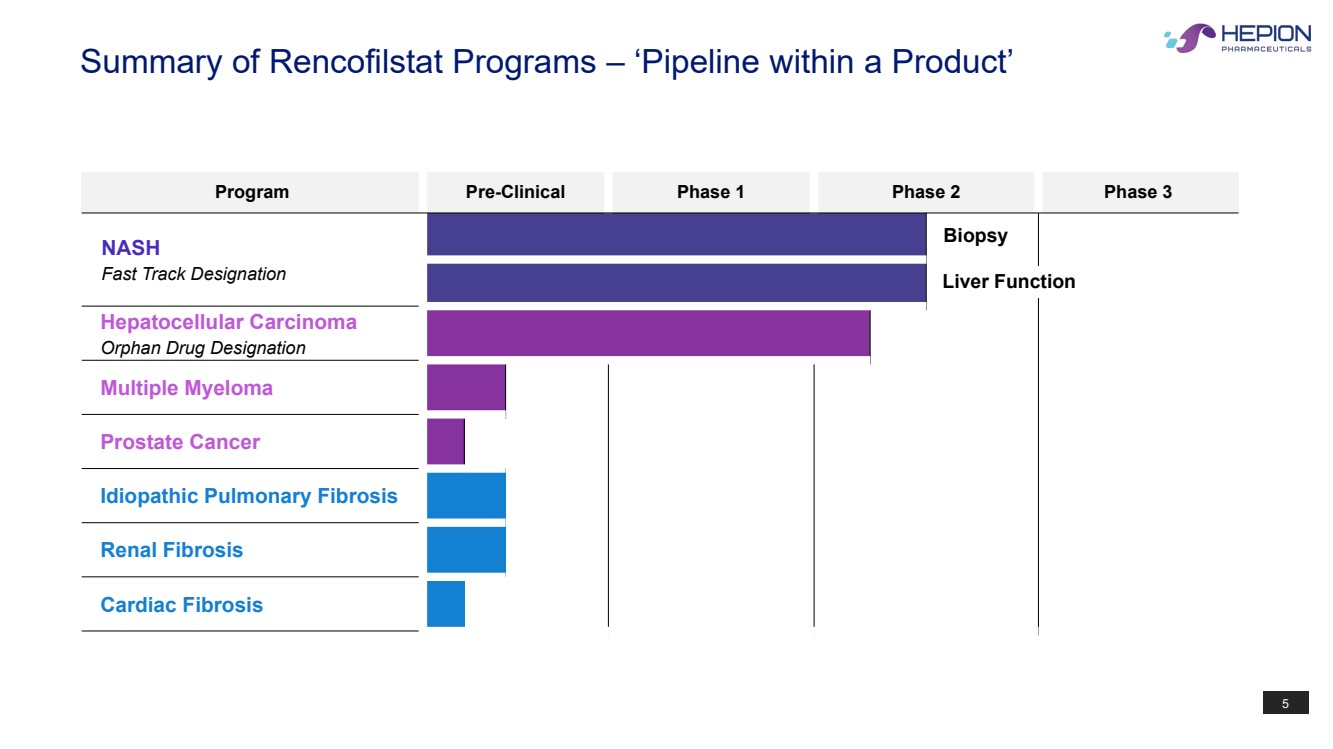
5 Program Pre-Clinical Phase 1 Phase 2 Phase 3 NASH Fast Track Designation Hepatocellular Carcinoma Orphan Drug Designation Multiple Myeloma Prostate Cancer Idiopathic Pulmonary Fibrosis Renal Fibrosis Cardiac Fibrosis Biopsy Summary of Rencofilstat Programs – ‘Pipeline within a Product’ Liver Function |
|
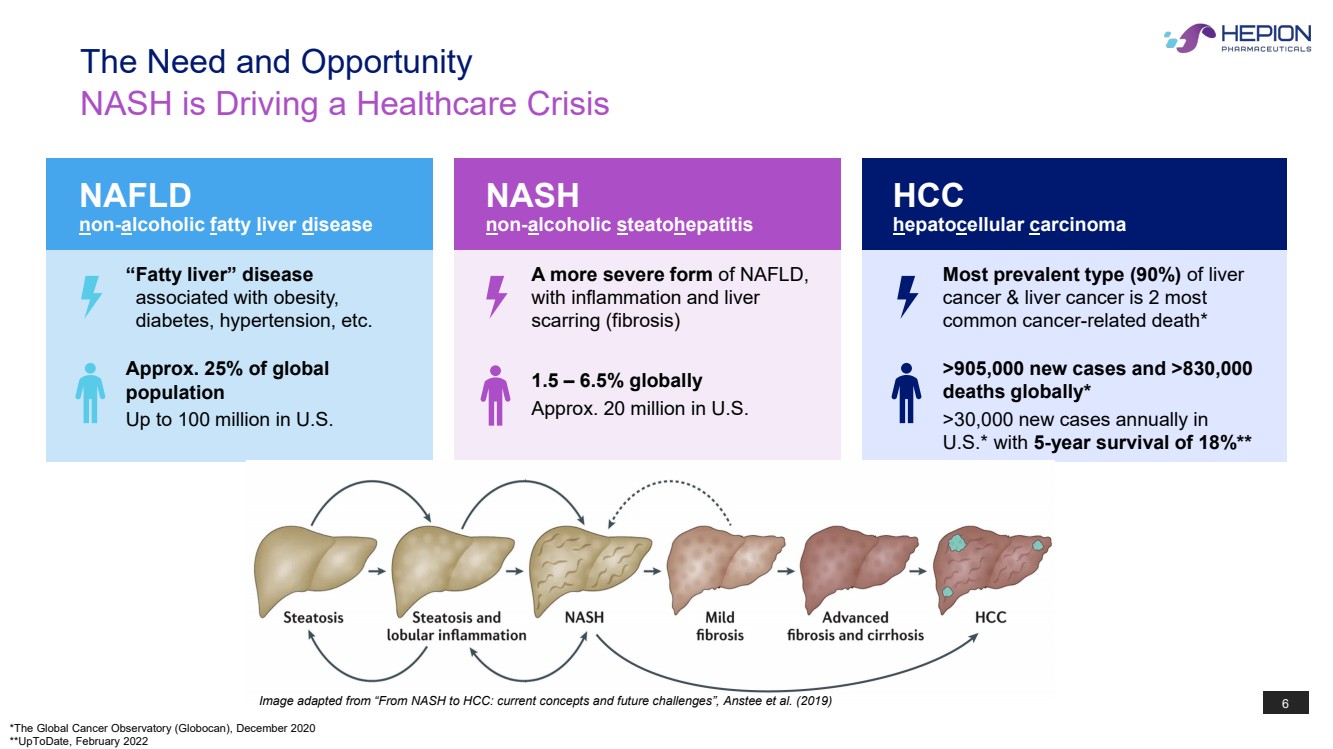
Image adapted from “From NASH to HCC: current concepts and future challenges”, Anstee et al. (2019) 6 NASH is Driving a Healthcare Crisis The Need and Opportunity NAFLD non-alcoholic fatty liver disease Approx. 25% of global population Up to 100 million in U.S. “Fatty liver” disease associated with obesity, diabetes, hypertension, etc. 1.5 – 6.5% globally Approx. 20 million in U.S. A more severe form of NAFLD, with inflammation and liver scarring (fibrosis) NASH non-alcoholic steatohepatitis HCC hepatocellular carcinoma Most prevalent type (90%) of liver cancer & liver cancer is 2 most common cancer-related death* >905,000 new cases and >830,000 deaths globally* >30,000 new cases annually in U.S.* with 5-year survival of 18%** *The Global Cancer Observatory (Globocan), December 2020 **UpToDate, February 2022 |
|
7 Why Develop a Drug for NASH? • No currently approved drugs for the treatment of NASH • Market for NASH is extremely large (estimated as ~20 million adults in U.S. alone) • NAFLD/NASH may be asymptomatic with no convenient diagnostic to identify subjects early in disease progression • Symptoms may only appear when disease has progressed to the point where disease associated fibrosis is well established • Consequences of NASH may be severe (need for liver transplant, cancer, cardiovascular disease, and death) |
|
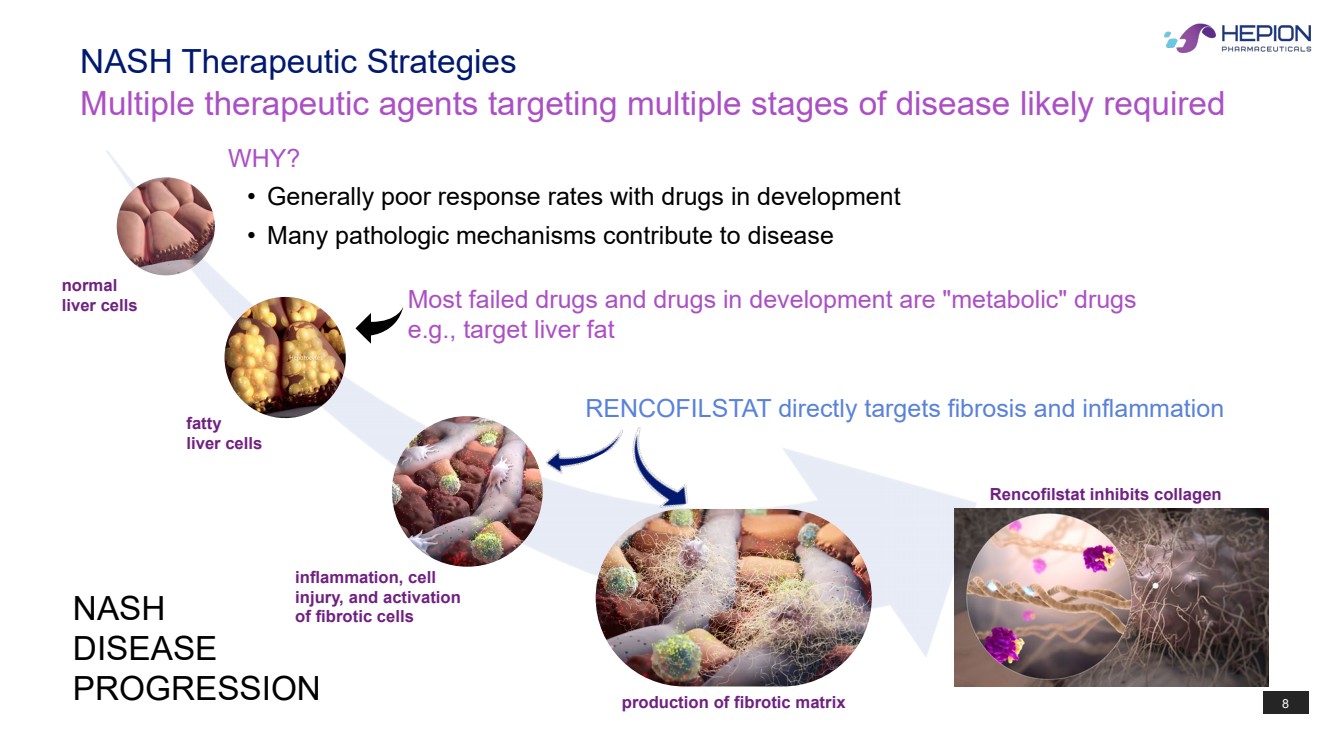
8 NASH DISEASE PROGRESSION normal liver cells fatty liver cells inflammation, cell injury, and activation of fibrotic cells production of fibrotic matrix WHY? • Generally poor response rates with drugs in development • Many pathologic mechanisms contribute to disease Most failed drugs and drugs in development are "metabolic" drugs e.g., target liver fat Rencofilstat inhibits collagen Multiple therapeutic agents targeting multiple stages of disease likely required NASH Therapeutic Strategies RENCOFILSTAT directly targets fibrosis and inflammation |
|
9 Rencofilstat Mode of Action |
|
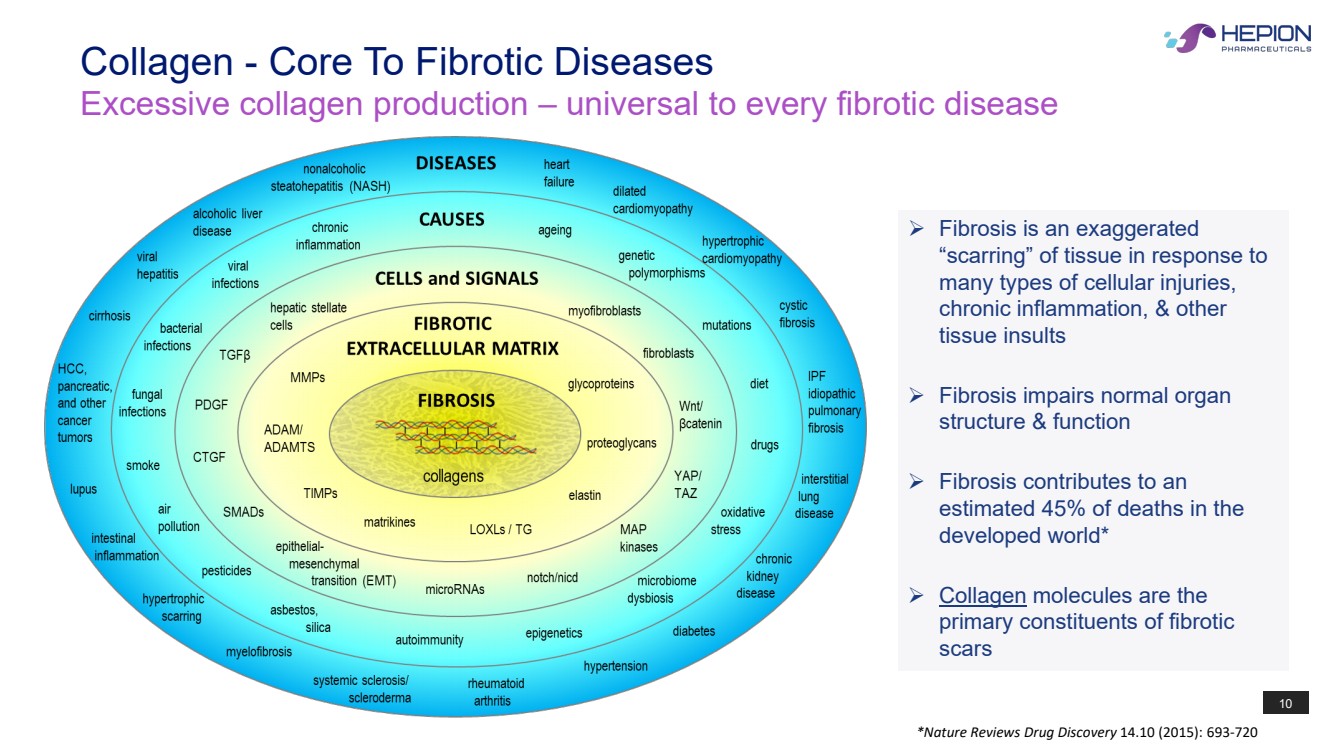
10 Collagen - Core To Fibrotic Diseases Excessive collagen production – universal to every fibrotic disease Fibrosis is an exaggerated “scarring” of tissue in response to many types of cellular injuries, chronic inflammation, & other tissue insults Fibrosis impairs normal organ structure & function Fibrosis contributes to an estimated 45% of deaths in the developed world* Collagen molecules are the primary constituents of fibrotic scars *Nature Reviews Drug Discovery 14.10 (2015): 693-720 |
|
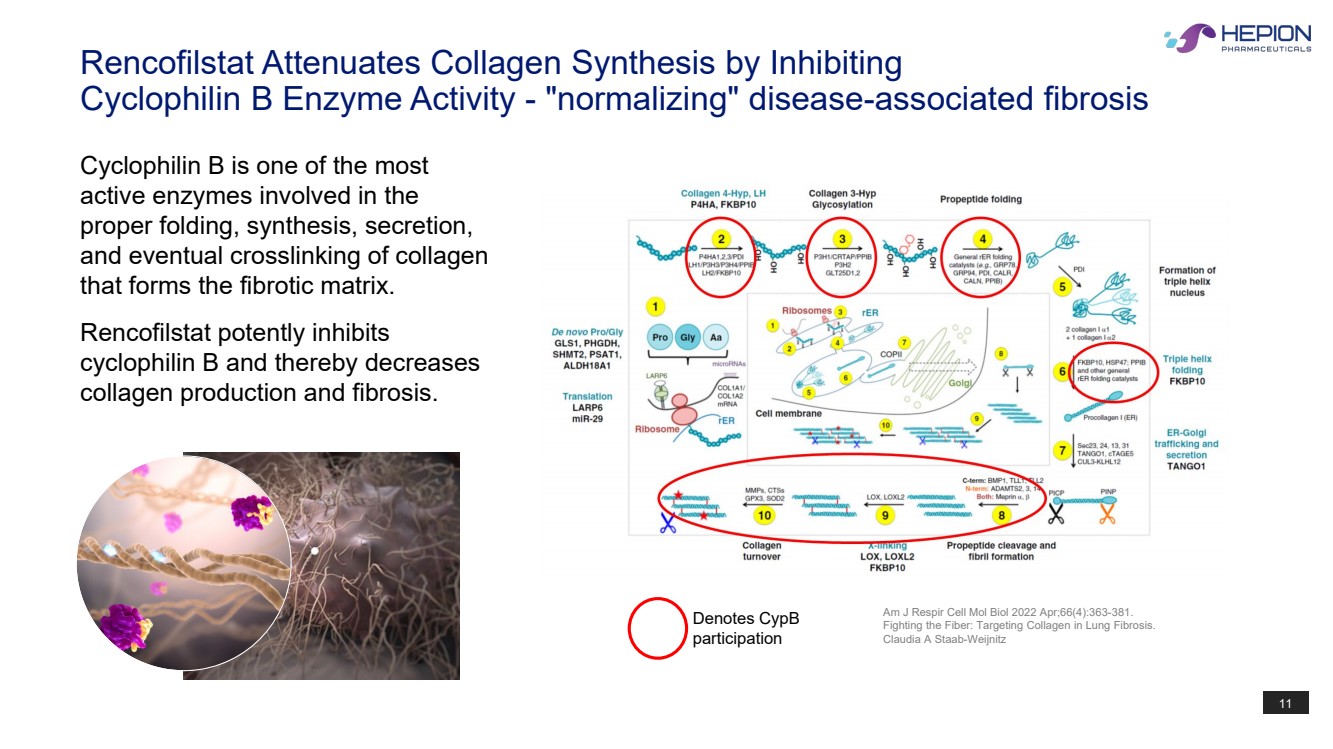
11 Rencofilstat Attenuates Collagen Synthesis by Inhibiting Cyclophilin B Enzyme Activity - "normalizing" disease-associated fibrosis Denotes CypB participation Am J Respir Cell Mol Biol 2022 Apr;66(4):363-381. Fighting the Fiber: Targeting Collagen in Lung Fibrosis. Claudia A Staab-Weijnitz Cyclophilin B is one of the most active enzymes involved in the proper folding, synthesis, secretion, and eventual crosslinking of collagen that forms the fibrotic matrix. Rencofilstat potently inhibits cyclophilin B and thereby decreases collagen production and fibrosis. |
|
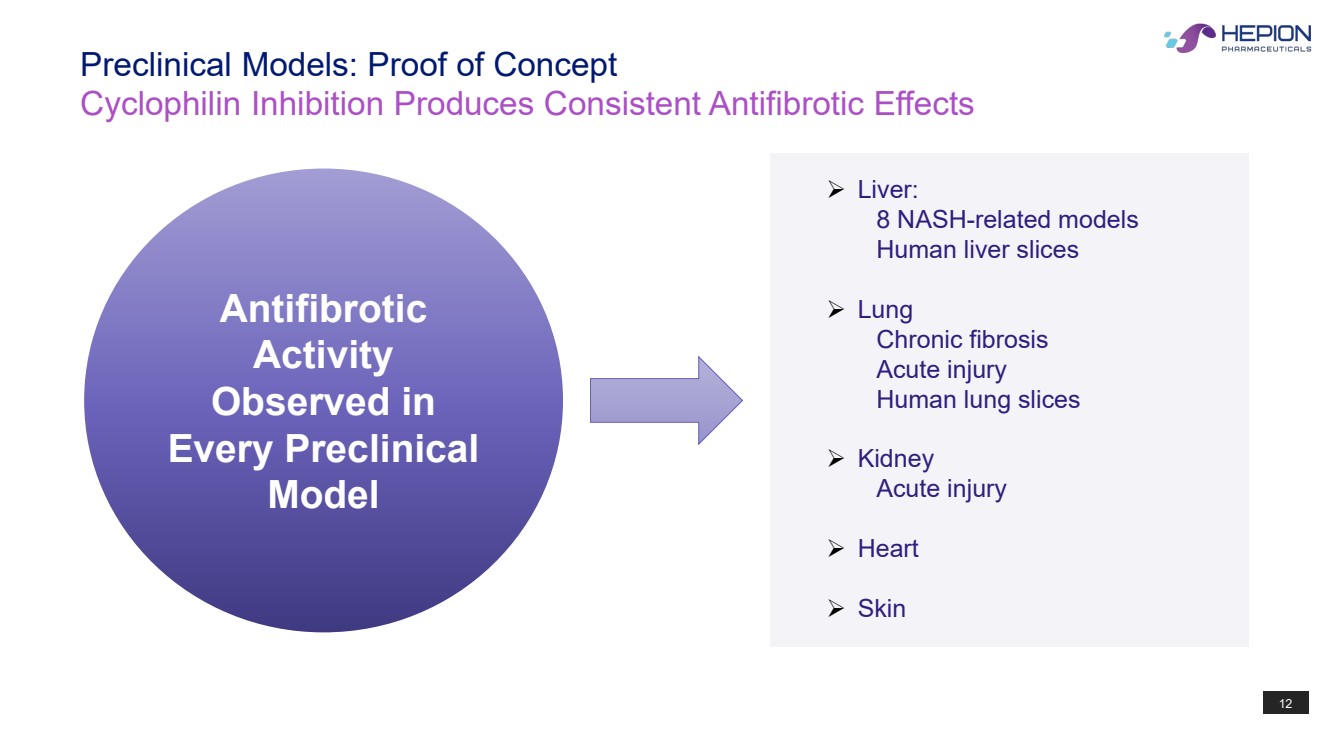
12 Cyclophilin Inhibition Produces Consistent Antifibrotic Effects Preclinical Models: Proof of Concept Liver: 8 NASH-related models Human liver slices Lung Chronic fibrosis Acute injury Human lung slices Kidney Acute injury Heart Skin Antifibrotic Activity Observed in Every Preclinical Model |
|
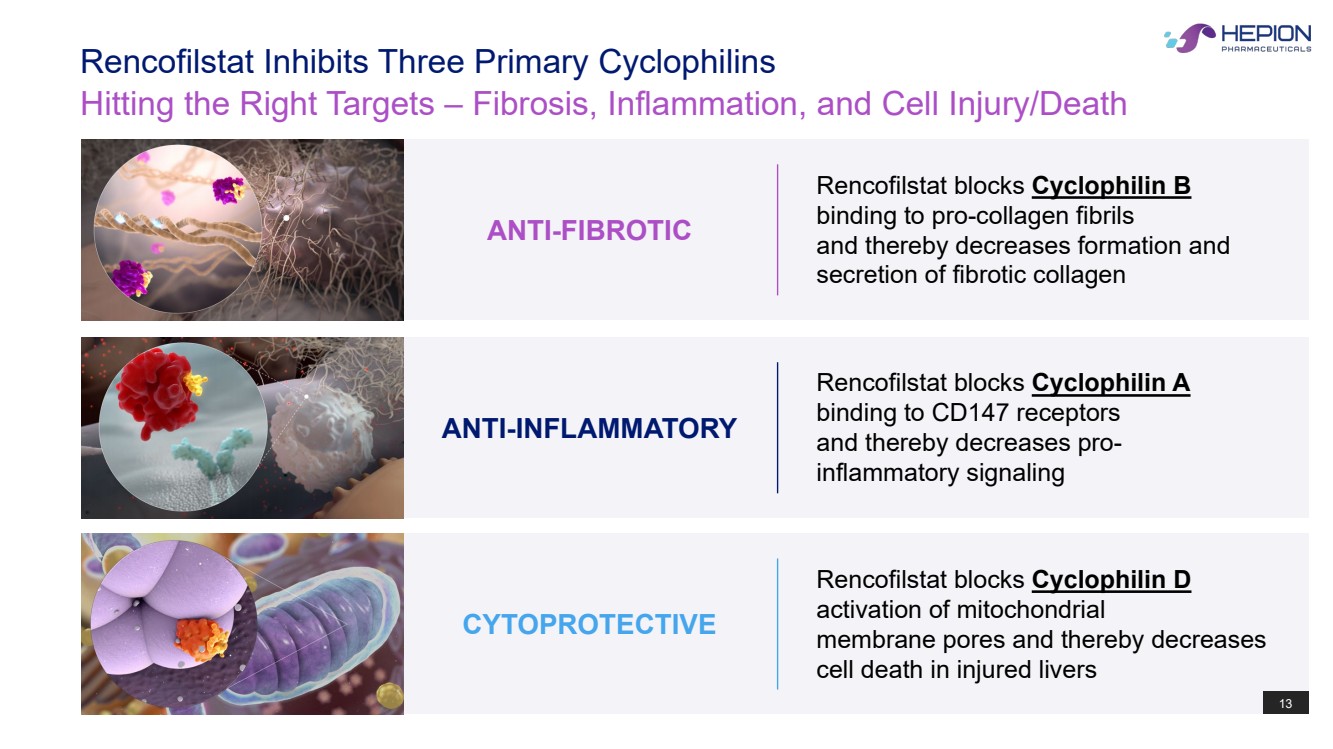
13 Hitting the Right Targets – Fibrosis, Inflammation, and Cell Injury/Death Rencofilstat Inhibits Three Primary Cyclophilins Rencofilstat blocks Cyclophilin D activation of mitochondrial membrane pores and thereby decreases cell death in injured livers CYTOPROTECTIVE 13 Rencofilstat blocks Cyclophilin A binding to CD147 receptors and thereby decreases pro-inflammatory signaling ANTI-INFLAMMATORY Rencofilstat blocks Cyclophilin B binding to pro-collagen fibrils and thereby decreases formation and secretion of fibrotic collagen ANTI-FIBROTIC |
|
14 Overview of Phase 1 Studies (Completed) |
|
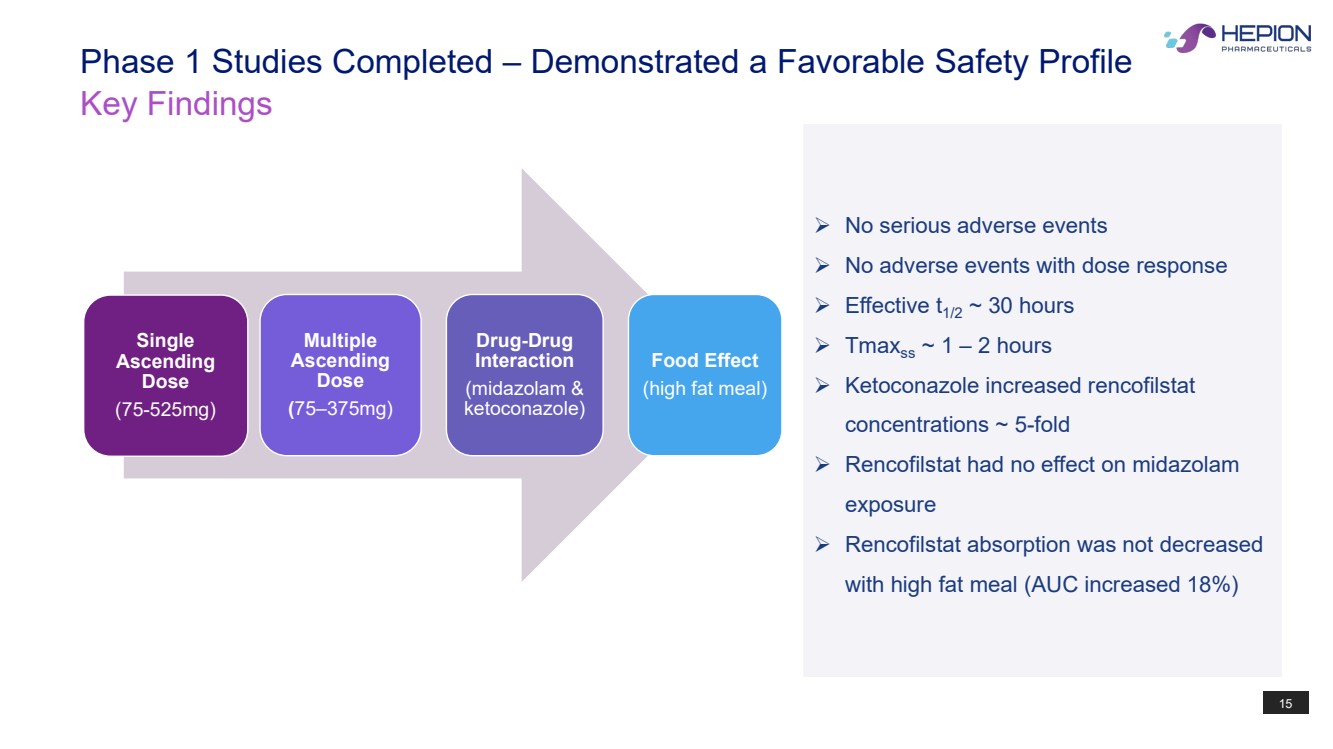
15 Key Findings Phase 1 Studies Completed – Demonstrated a Favorable Safety Profile No serious adverse events No adverse events with dose response Effective t1/2 ~ 30 hours Tmaxss ~ 1 – 2 hours Ketoconazole increased rencofilstat concentrations ~ 5-fold Rencofilstat had no effect on midazolam exposure Rencofilstat absorption was not decreased with high fat meal (AUC increased 18%) Single Ascending Dose (75-525mg) Multiple Ascending Dose (75–375mg) Drug-Drug Interaction (midazolam & ketoconazole) Food Effect (high fat meal) |
|
16 Overview of Phase 2a ‘AMBITION’ NASH Trial (Completed) |
|
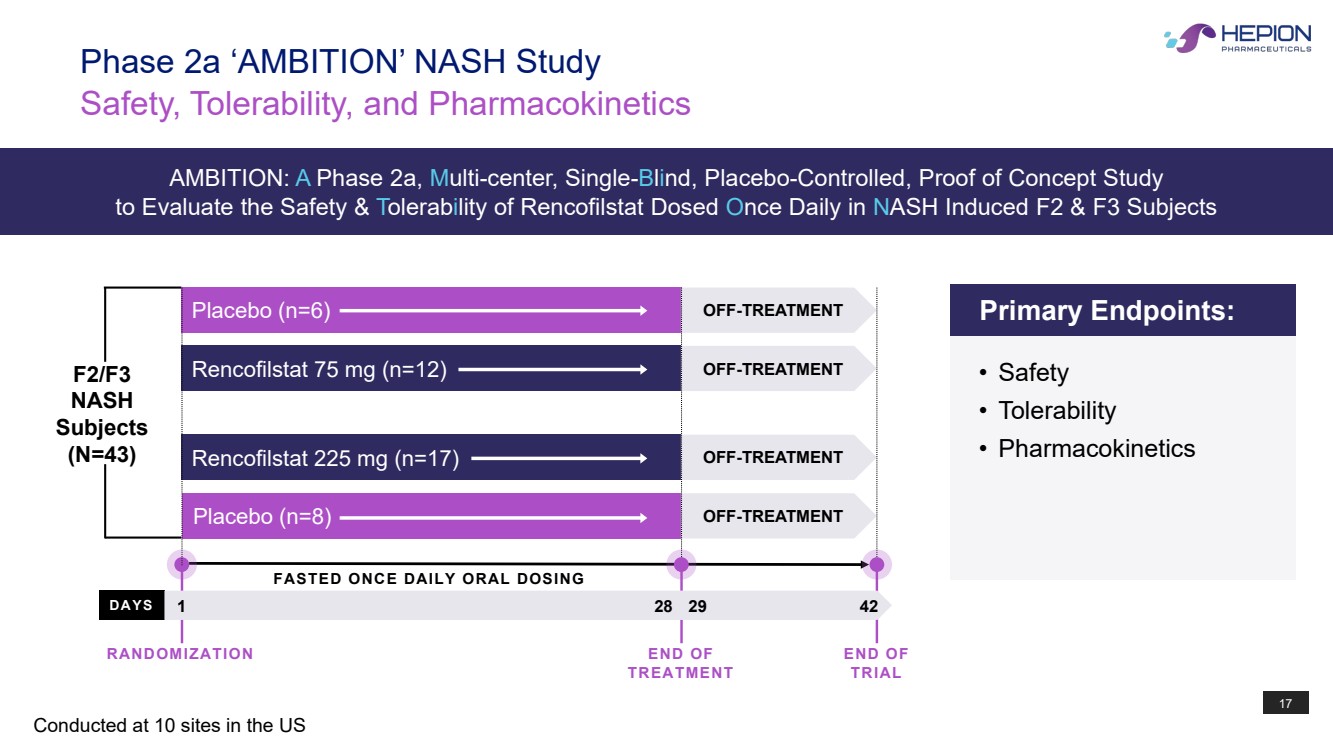
17 F2/F3 NASH Subjects (N=43) Rencofilstat 225 mg (n=17) Placebo (n=8) Placebo (n=6) Rencofilstat 75 mg (n=12) OFF-TREATMENT OFF-TREATMENT OFF-TREATMENT OFF-TREATMENT DAYS FASTED ONCE DAILY ORAL DOSING Safety, Tolerability, and Pharmacokinetics Phase 2a ‘AMBITION’ NASH Study Conducted at 10 sites in the US 1 28 42 Primary Endpoints: • Safety • Tolerability • Pharmacokinetics RANDOMIZATION END OF TREATMENT END OF TRIAL 29 AMBITION: A Phase 2a, Multi-center, Single-Blind, Placebo-Controlled, Proof of Concept Study to Evaluate the Safety & Tolerability of Rencofilstat Dosed Once Daily in NASH Induced F2 & F3 Subjects |
|
18 Rencofilstat demonstrated a favorable safety profile Efficacy signals were observed in only 28 days including: • Reduction in ALT (marker of inflammation & fibrosis) • Reduction in Pro-C3 (marker of fibrosis) • Downregulation of collagen genes • Upregulation of genes associated with liver recovery and favorable lipid dynamics Early evidence of a concentration-effect relationship was observed with both ALT and Pro-C3 Rencofilstat concentrations are not significantly altered by NASH Rencofilstat concentrations expected to be effective in NASH endpoints (ALT and Pro-C3) were achieved All Primary Endpoints Met Phase 2a ‘AMBITION’ NASH Study |
|
19 Hepion’s Proprietary Artificial Intelligence |
|
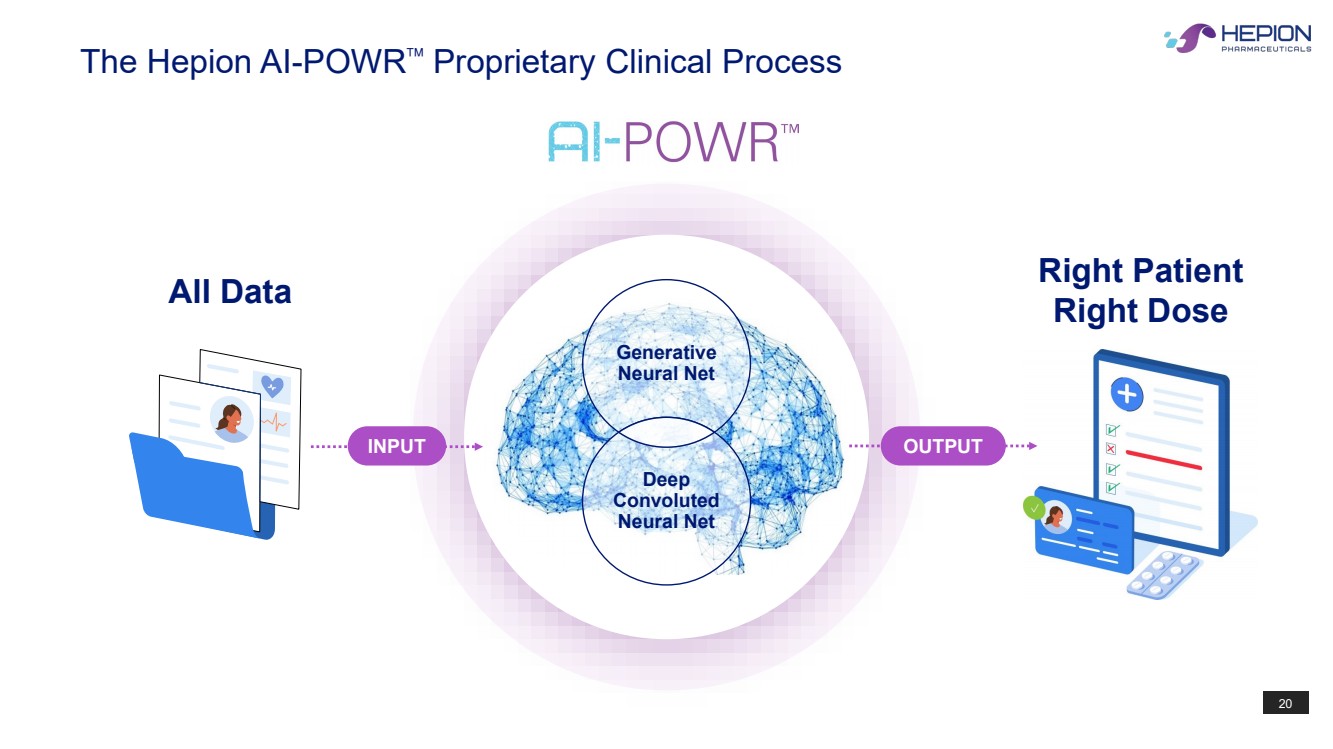
20 Right Patient Right Dose The Hepion AI-POWR Proprietary Clinical Process All Data Generative Neural Net Deep Convoluted Neural Net INPUT OUTPUT |
|
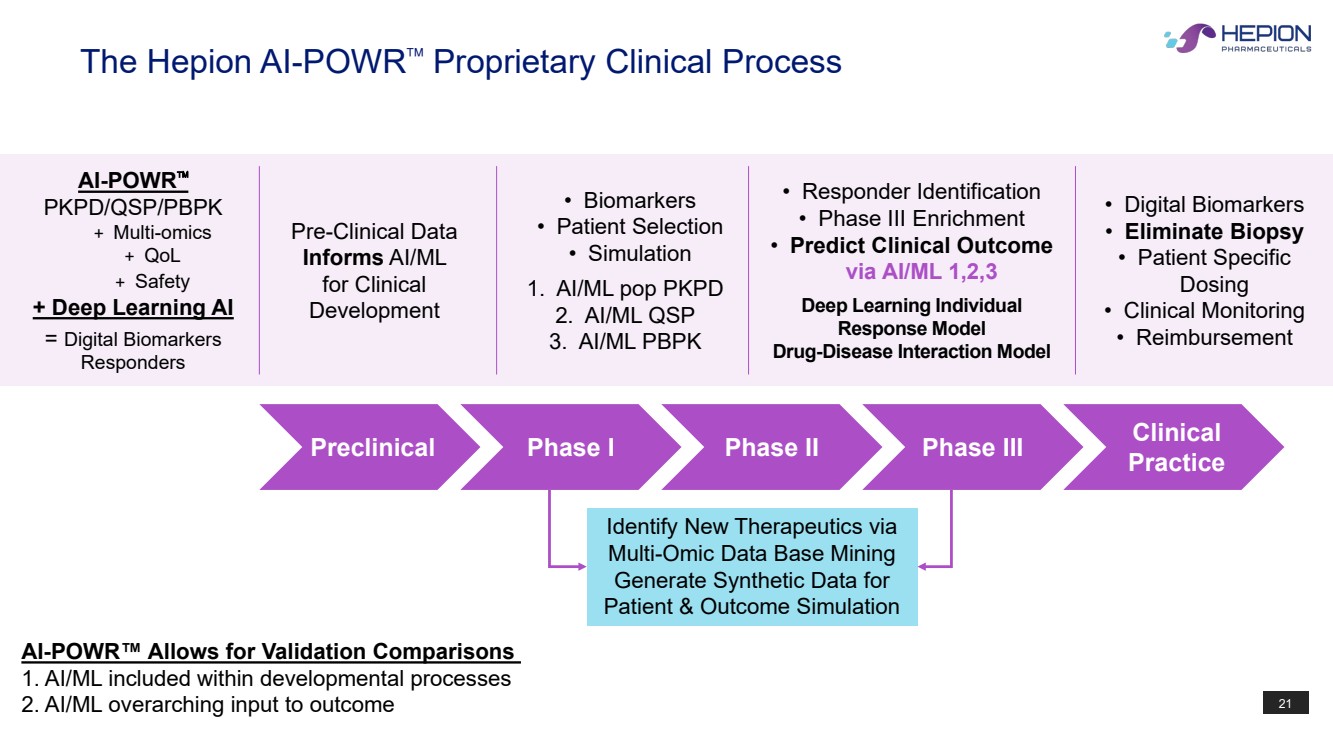
21 The Hepion AI-POWR Proprietary Clinical Process Pre-Clinical Data Informs AI/ML for Clinical Development • Biomarkers • Patient Selection • Simulation 1. AI/ML pop PKPD 2. AI/ML QSP 3. AI/ML PBPK AI-POWR PKPD/QSP/PBPK + Multi-omics + QoL + Safety + Deep Learning AI = Digital Biomarkers Responders • Responder Identification • Phase III Enrichment • Predict Clinical Outcome via AI/ML 1,2,3 Deep Learning Individual Response Model Drug-Disease Interaction Model • Digital Biomarkers • Eliminate Biopsy • Patient Specific Dosing • Clinical Monitoring • Reimbursement Identify New Therapeutics via Multi-Omic Data Base Mining Generate Synthetic Data for Patient & Outcome Simulation AI-POWR™ Allows for Validation Comparisons 1. AI/ML included within developmental processes 2. AI/ML overarching input to outcome Preclinical Phase I Phase II Phase III Clinical Practice |
|
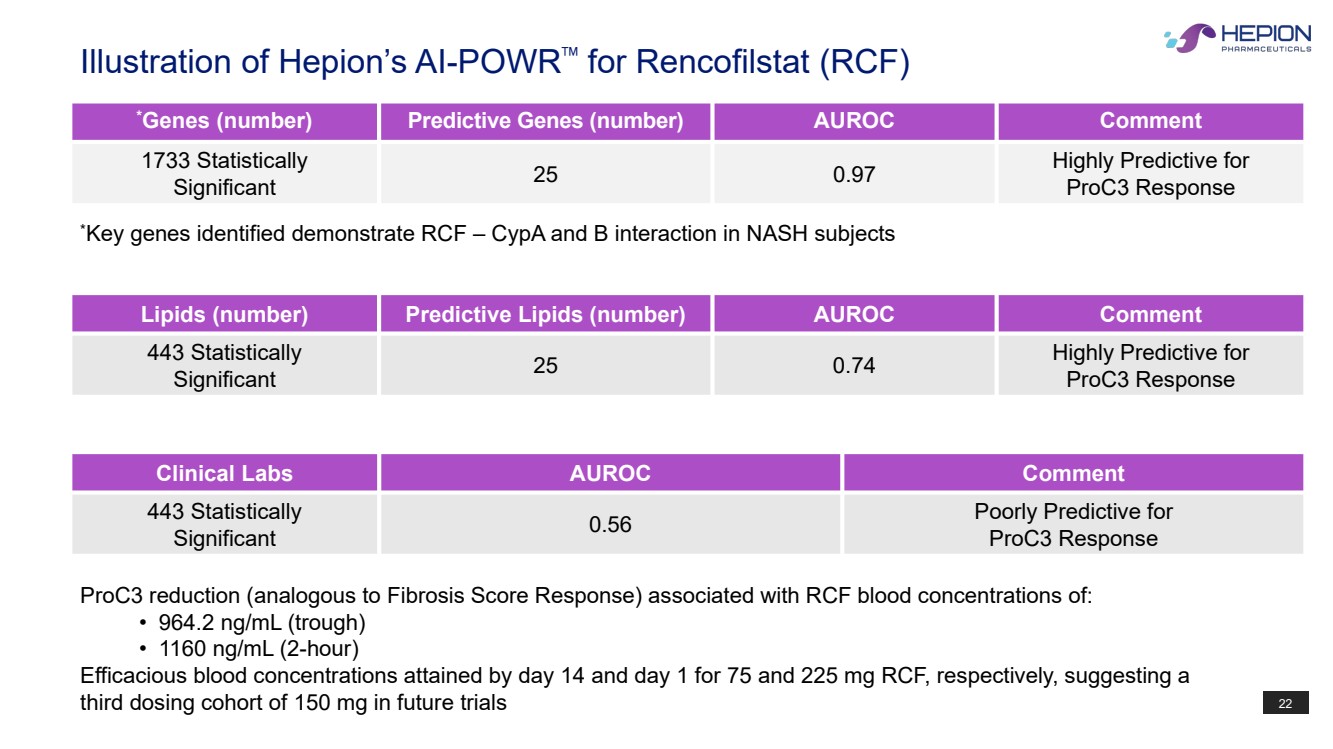
22 Illustration of Hepion’s AI-POWR™ for Rencofilstat (RCF) * Genes (number) Predictive Genes (number) AUROC Comment 1733 Statistically Significant 25 0.97 Highly Predictive for ProC3 Response Lipids (number) Predictive Lipids (number) AUROC Comment 443 Statistically Significant 25 0.74 Highly Predictive for ProC3 Response Clinical Labs AUROC Comment 443 Statistically Significant 0.56 Poorly Predictive for ProC3 Response * Key genes identified demonstrate RCF – CypA and B interaction in NASH subjects ProC3 reduction (analogous to Fibrosis Score Response) associated with RCF blood concentrations of: • 964.2 ng/mL (trough) • 1160 ng/mL (2-hour) Efficacious blood concentrations attained by day 14 and day 1 for 75 and 225 mg RCF, respectively, suggesting a third dosing cohort of 150 mg in future trials |
|
23 Phase 2 ‘ALTITUDE-NASH’ Trial (Clinically Complete) |
|
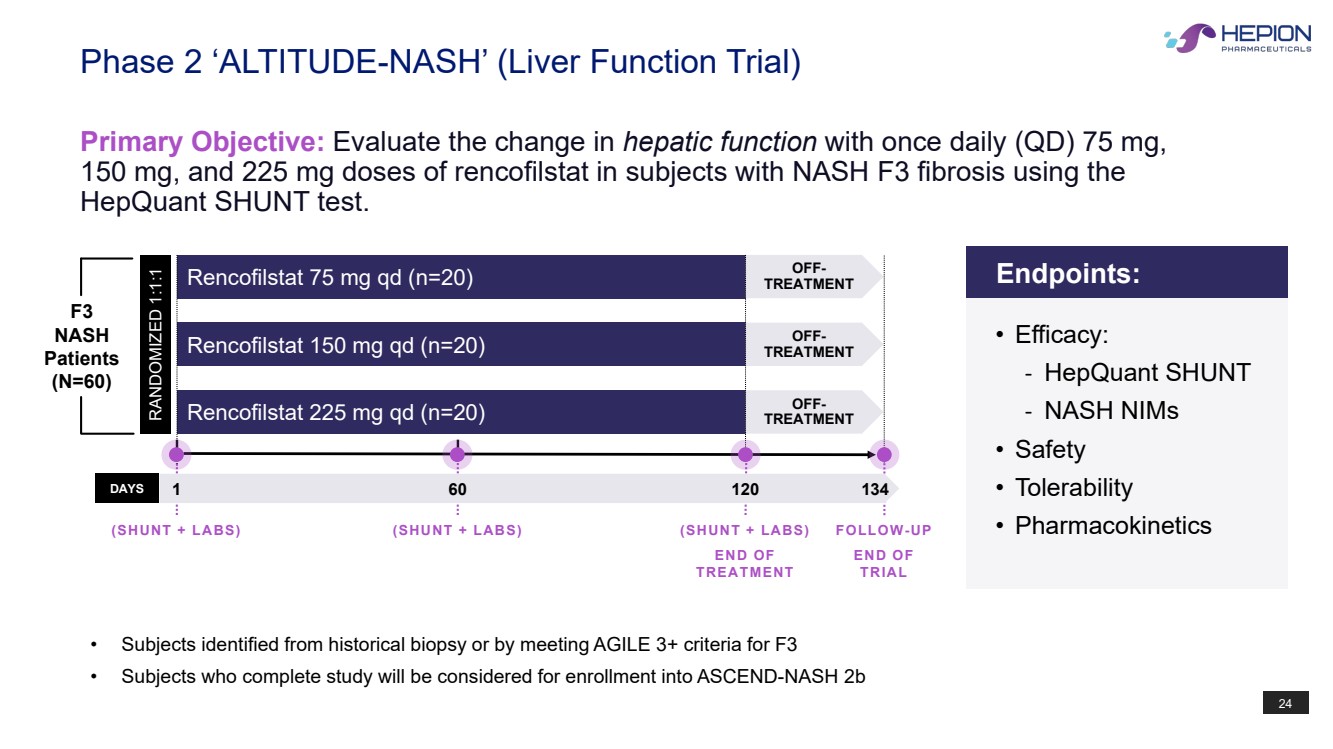
24 • Subjects identified from historical biopsy or by meeting AGILE 3+ criteria for F3 • Subjects who complete study will be considered for enrollment into ASCEND-NASH 2b Phase 2 ‘ALTITUDE-NASH’ (Liver Function Trial) Primary Objective: Evaluate the change in hepatic function with once daily (QD) 75 mg, 150 mg, and 225 mg doses of rencofilstat in subjects with NASH F3 fibrosis using the HepQuant SHUNT test. Rencofilstat 225 mg qd (n=20) Rencofilstat 75 mg qd (n=20) Rencofilstat 150 mg qd (n=20) RANDOMIZED 1:1:1 OFF-TREATMENT OFF-TREATMENT OFF-TREATMENT DAYS 1 120 134 (SHUNT + LABS) END OF TREATMENT FOLLOW-UP END OF TRIAL (SHUNT + LABS) F3 NASH Patients (N=60) 60 (SHUNT + LABS) Endpoints: • Efficacy: - HepQuant SHUNT - NASH NIMs • Safety • Tolerability • Pharmacokinetics |
|
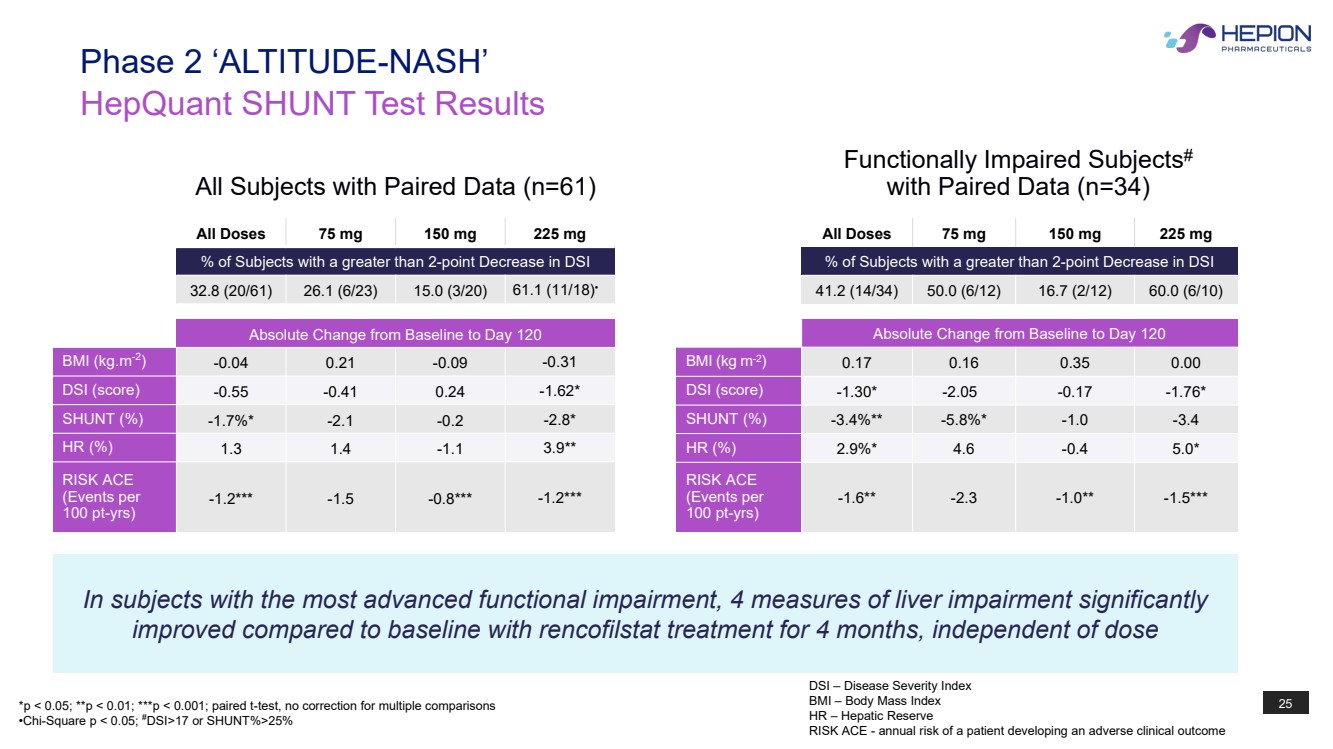
25 HepQuant SHUNT Test Results Phase 2 ‘ALTITUDE-NASH’ All Doses 75 mg 150 mg 225 mg % of Subjects with a greater than 2-point Decrease in DSI 32.8 (20/61) 26.1 (6/23) 15.0 (3/20) 61.1 (11/18)• Absolute Change from Baseline to Day 120 BMI (kg.m-2 ) -0.04 0.21 -0.09 -0.31 DSI (score) -0.55 -0.41 0.24 -1.62* SHUNT (%) -1.7%* -2.1 -0.2 -2.8* HR (%) 1.3 1.4 -1.1 3.9** RISK ACE (Events per 100 pt-yrs) -1.2*** -1.5 -0.8*** -1.2*** All Doses 75 mg 150 mg 225 mg % of Subjects with a greater than 2-point Decrease in DSI 41.2 (14/34) 50.0 (6/12) 16.7 (2/12) 60.0 (6/10) Absolute Change from Baseline to Day 120 BMI (kg m-2) 0.17 0.16 0.35 0.00 DSI (score) -1.30* -2.05 -0.17 -1.76* SHUNT (%) -3.4%** -5.8%* -1.0 -3.4 HR (%) 2.9%* 4.6 -0.4 5.0* RISK ACE (Events per 100 pt-yrs) -1.6** -2.3 -1.0** -1.5*** In subjects with the most advanced functional impairment, 4 measures of liver impairment significantly improved compared to baseline with rencofilstat treatment for 4 months, independent of dose *p < 0.05; **p < 0.01; ***p < 0.001; paired t-test, no correction for multiple comparisons •Chi-Square p < 0.05; # DSI>17 or SHUNT%>25% All Subjects with Paired Data (n=61) Functionally Impaired Subjects# with Paired Data (n=34) DSI – Disease Severity Index BMI – Body Mass Index HR – Hepatic Reserve RISK ACE - annual risk of a patient developing an adverse clinical outcome |
|
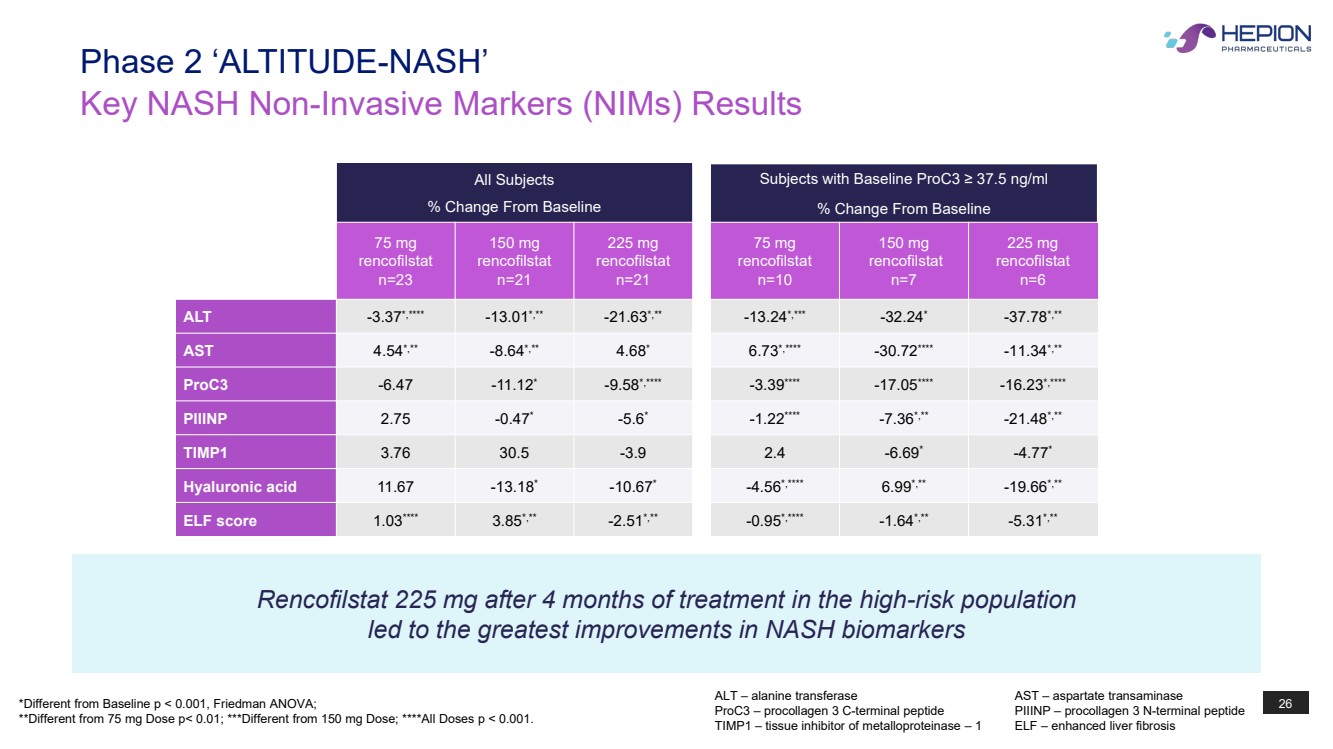
26 All Subjects % Change From Baseline Subjects with Baseline ProC3 ≥ 37.5 ng/ml % Change From Baseline 75 mg rencofilstat n=23 150 mg rencofilstat n=21 225 mg rencofilstat n=21 75 mg rencofilstat n=10 150 mg rencofilstat n=7 225 mg rencofilstat n=6 ALT -3.37*,**** -13.01*,** -21.63*,** -13.24*,*** -32.24* -37.78*,** AST 4.54*,** -8.64*,** 4.68* 6.73*,**** -30.72**** -11.34*,** ProC3 -6.47 -11.12* -9.58*,**** -3.39**** -17.05**** -16.23*,**** PIIINP 2.75 -0.47* -5.6* -1.22**** -7.36*,** -21.48*,** TIMP1 3.76 30.5 -3.9 2.4 -6.69* -4.77* Hyaluronic acid 11.67 -13.18* -10.67* -4.56*,**** 6.99*,** -19.66*,** ELF score 1.03**** 3.85*,** -2.51*,** -0.95*,**** -1.64*,** -5.31*,** Key NASH Non-Invasive Markers (NIMs) Results Phase 2 ‘ALTITUDE-NASH’ Rencofilstat 225 mg after 4 months of treatment in the high-risk population led to the greatest improvements in NASH biomarkers *Different from Baseline p < 0.001, Friedman ANOVA; **Different from 75 mg Dose p< 0.01; ***Different from 150 mg Dose; ****All Doses p < 0.001. ALT – alanine transferase AST – aspartate transaminase ProC3 – procollagen 3 C-terminal peptide PIIINP – procollagen 3 N-terminal peptide TIMP1 – tissue inhibitor of metalloproteinase – 1 ELF – enhanced liver fibrosis |
|
27 Phase 2b ‘ASCEND-NASH’ Trial (Enrolling) |
|
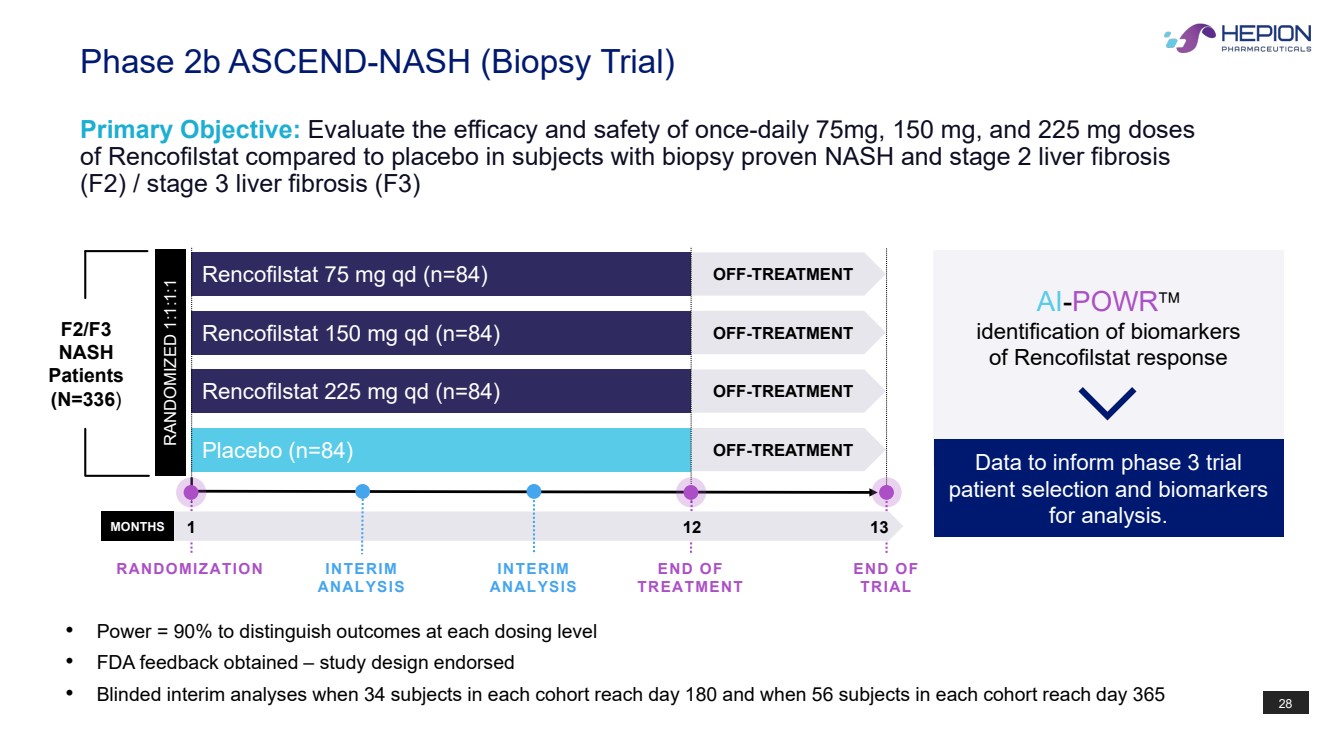
28 Phase 2b ASCEND-NASH (Biopsy Trial) Primary Objective: Evaluate the efficacy and safety of once-daily 75mg, 150 mg, and 225 mg doses of Rencofilstat compared to placebo in subjects with biopsy proven NASH and stage 2 liver fibrosis (F2) / stage 3 liver fibrosis (F3) Rencofilstat 225 mg qd (n=84) Placebo (n=84) Rencofilstat 75 mg qd (n=84) Rencofilstat 150 mg qd (n=84) RANDOMIZED 1:1:1:1 OFF-TREATMENT OFF-TREATMENT OFF-TREATMENT OFF-TREATMENT MONTHS 1 12 13 END OF TREATMENT END OF TRIAL INTERIM ANALYSIS INTERIM ANALYSIS RANDOMIZATION Data to inform phase 3 trial patient selection and biomarkers for analysis. AI-POWR identification of biomarkers of Rencofilstat response F2/F3 NASH Patients (N=336) • Power = 90% to distinguish outcomes at each dosing level • FDA feedback obtained – study design endorsed • Blinded interim analyses when 34 subjects in each cohort reach day 180 and when 56 subjects in each cohort reach day 365 |
|
29 Phase 2b ASCEND-NASH Primary Efficacy Endpoint: Superiority of rencofilstat compared to placebo on liver histology at month 12 relative to the screening biopsy, by assessing the proportion of subjects with improvement in fibrosis by at least 1 stage (NASH CRN system) OR NASH resolution without worsening of fibrosis Secondary Efficacy Endpoints: Superiority of rencofilstat compared to placebo on histology at month 12 relative to screening by assessing the proportion of subjects with improvement in fibrosis by: • At least 1 stage regardless of effect on NASH • At least 2 stages regardless of effect on NASH • At least 2 stages AND no worsening of NASH. |
|
30 Phase 2a HCC Trial (Pending) |
|
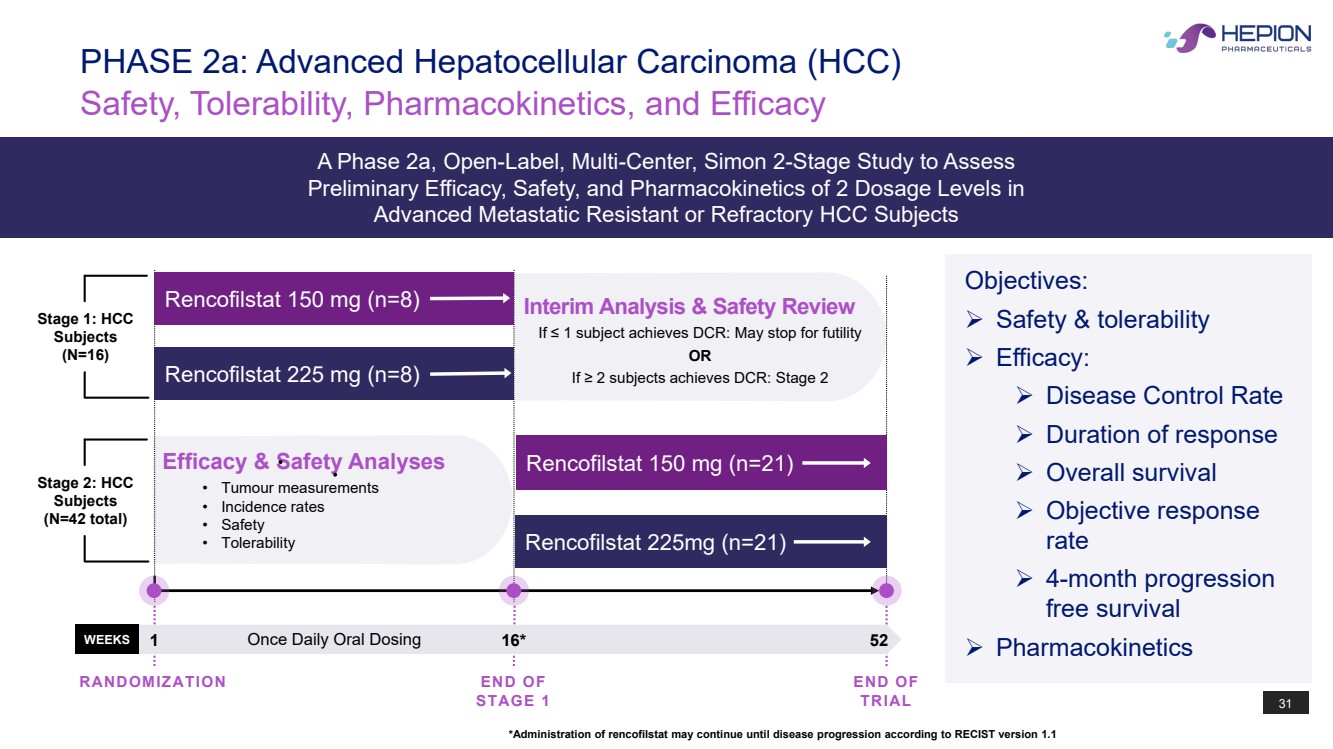
31 Objectives: Safety & tolerability Efficacy: Disease Control Rate Duration of response Overall survival Objective response rate 4-month progression free survival Pharmacokinetics Safety, Tolerability, Pharmacokinetics, and Efficacy PHASE 2a: Advanced Hepatocellular Carcinoma (HCC) A Phase 2a, Open-Label, Multi-Center, Simon 2-Stage Study to Assess Preliminary Efficacy, Safety, and Pharmacokinetics of 2 Dosage Levels in Advanced Metastatic Resistant or Refractory HCC Subjects *Administration of rencofilstat may continue until disease progression according to RECIST version 1.1 WEEKS 1 16* 52 END OF STAGE 1 END OF TRIAL RANDOMIZATION Once Daily Oral Dosing Efficacy & Safety Analyses • Tumour measurements • Incidence rates • Safety • Tolerability Rencofilstat 150 mg (n=21) Rencofilstat 225mg (n=21) Stage 2: HCC Subjects (N=42 total) Interim Analysis & Safety Review If ≤ 1 subject achieves DCR: May stop for futility OR If ≥ 2 subjects achieves DCR: Stage 2 Rencofilstat 150 mg (n=8) Rencofilstat 225 mg (n=8) Stage 1: HCC Subjects (N=16) |
|
32 Intellectual Property |
|
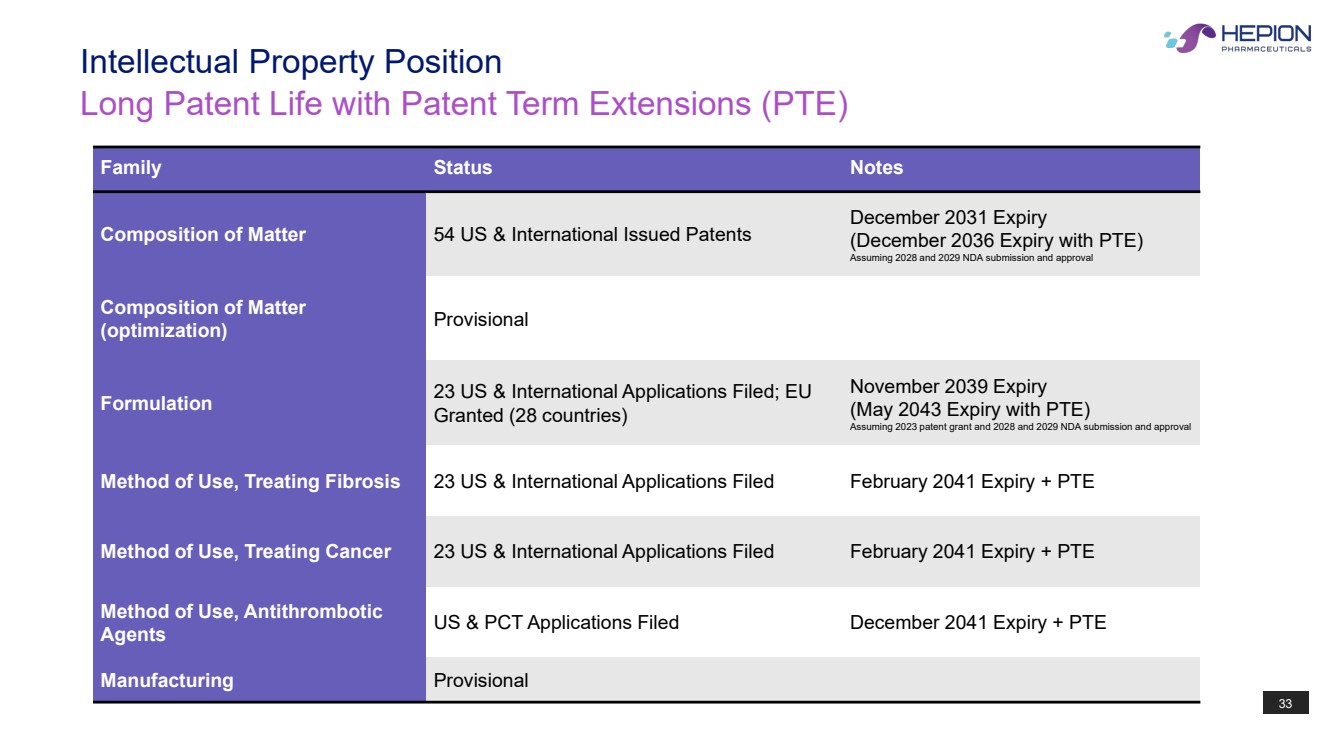
33 Long Patent Life with Patent Term Extensions (PTE) Intellectual Property Position Family Status Notes Composition of Matter 54 US & International Issued Patents December 2031 Expiry (December 2036 Expiry with PTE) Assuming 2028 and 2029 NDA submission and approval Composition of Matter (optimization) Provisional Formulation 23 US & International Applications Filed; EU Granted (28 countries) November 2039 Expiry (May 2043 Expiry with PTE) Assuming 2023 patent grant and 2028 and 2029 NDA submission and approval Method of Use, Treating Fibrosis 23 US & International Applications Filed February 2041 Expiry + PTE Method of Use, Treating Cancer 23 US & International Applications Filed February 2041 Expiry + PTE Method of Use, Antithrombotic Agents US & PCT Applications Filed December 2041 Expiry + PTE Manufacturing Provisional |
|
34 Summary |
|
35 $43.0 M Cash as of 03/31/23 Financials Two Tackling Fibrotic Diseases Value Drivers • Rencofilstat, once-daily oral, targeting key drivers of pathology, tested in over 425 subjects • Two Phase 2 NASH trials: • ALTITUDE-NASH – Clinically Complete • ASCEND-NASH Phase 2b – Recruiting • Upcoming Phase 2 for HCC • Developing companion A.I. for clinical development and commercialization strategy • Core scientific team discovered and developed voclosporin (currently marketed) • Robust IP 3.8 M Common Shares Outstanding 35 |
|
36 Patrick Mayo, PhD SVP, Clinical Pharmacology and Analytics Joined Isotechnika (Aurinia) in 2002 and joined HEPA in 2019. Robert Foster, PharmD, PhD CEO Founded Isotechnika (Aurinia) in 1993, and served mostly as CEO & Chairman, until 2014. Joined HEPA in 2016 as CSO and became CEO in 2018. John Cavan, MBA CFO Formerly of Pine Hill, Stemline, Aegerion, AlgoRx, Alpharma, Sony, American Express and International Specialty Products, joined HEPA in 2016. Todd Hobbs, MD CMO Formerly Chief Medical Officer of Novo Nordisk, joined HEPA in 2021. Launa Aspeslet, PhD COO Formerly COO of Isotechnika (Aurinia) from 1996- 2013. Was CEO of an oncology CRO from 2013 until joining HEPA in 2022. Daren Ure, PhD CSO Joined Isotechnika (Aurinia) in 2003 and joined HEPA in 2016. Daniel Trepanier, PhD SVP, Drug Development Joined Isotechnika (Aurinia) in 1997 and joined HEPA in 2016. Core R&D team has collectively > 120 yrs of experience with cyclophilin inhibition drug development, most notably voclosporin (Lupkynis®) for lupus nephritis while at Isotechnika (Aurinia, NASDAQ:AUPH) Experienced Team |
|
CONTACT US Hepion Pharmaceuticals Inc. 399 Thornall Street, First Floor Edison, New Jersey, USA, 08837 Email: info@hepionpharma.com Phone: 732-902-4000 www.hepionpharma.com |
Exhibit 99.2
Hepion Pharmaceuticals’ Phase 2 ‘ALTITUDE-NASH’ Trial Achieves Primary and Secondary Endpoints, Including Improvement in Liver Function and Multiple NASH Biomarkers
- Improvements in physiologic liver function and key NASH biomarkers including ALT, ProC3, PIIINP and ELF -
- Results reinforce rencofilstat’s direct antifibrotic mode of action; increases confidence for reductions in fibrosis in ongoing Phase 2b ‘ASCEND-NASH’ paired biopsy trial -
EDISON, N.J., May 22, 2023 - Hepion Pharmaceuticals, Inc. (NASDAQ:HEPA), a clinical stage biopharmaceutical company focused on artificial Intelligence (“AI”)-assisted therapeutic drug development for the treatment of non-alcoholic steatohepatitis (“NASH”), fibrotic diseases, hepatocellular carcinoma (“HCC”), and other chronic diseases, today announced positive topline results from its recently completed Phase 2 ALTITUDE-NASH clinical trial.
ALTITUDE-NASH met its primary endpoint by demonstrating improved physiologic liver function and was well tolerated after four months of treatment in subjects with stage 3 or greater fibrosis based on the AGILE 3+ criteria. Several additional secondary endpoints were also met, including reductions in the liver injury biomarkers, alanine and aspartate transaminases (“ALT” and “AST”); and multiple fibrosis-associated biomarkers, including ProC3 (procollagen 3 C-terminal peptide), PIIINP (procollagen 3 N-terminal peptide), TIMP1 (tissue inhibitor of metalloproteinase-1), hyaluronic acid, and enhanced liver fibrosis (“ELF”) scores (composite of PIIINP, TIMP1, and hyaluronic acid). These observations build on similar findings from a shorter Phase 2a trial and reinforce rencofilstat’s direct antifibrotic mode of action and increases the confidence for reductions in fibrosis in Hepion’s ongoing Phase 2b ASCEND-NASH paired biopsy trial.
“We are thrilled that the ALTITUDE-NASH trial met both its primary efficacy and safety endpoints, in particular with the 225 mg rencofilstat dose showing the greatest benefit to liver function and multiple NASH-associated biomarkers,” said Todd Hobbs, MD, Hepion’s Chief Medical Officer. “This trial was designed to inform us on how well rencofilstat improves hepatic function in those with significant impairment and risk for complications from their advanced NASH. Further, it provided an opportunity to evaluate data generated from different doses of rencofilstat. I am very pleased with the research team and the ALTITUDE-NASH sites that quickly recruited this study. Our improved understanding of which subjects best respond to rencofilstat can be immediately applied to increase the likelihood of success of our larger and longer ASCEND-NASH paired biopsy trial.”
Primary Endpoint: Four Measures of Liver Impairment Significantly Improved Compared to Baseline with Four Months Rencofilstat 225 mg Treatment
The HepQuant SHUNT Test was used in this study under an FDA-issued Investigational Device Exemption (IDE). The SHUNT Test is a minimally invasive test that tracks changes in the degree of liver function impairment and was used to determine four key measures: HepQuant DSI™ (Disease Severity Index) score, which primarily reflects hepatocyte function; SHUNT, which reflects the impact of micro-architectural changes, such as fibrosis on blood flow through the liver; HepQuant HR™ (Hepatic Reserve); and RISK ACE, which reflects the annual risk of a patient developing an adverse clinical outcome (Table 1). Rencofilstat met the primary endpoint and lowered mean DSI score in all doses, with rencofilstat 225 mg treatment over 4 months resulting in statistically significant decreases in DSI (mean Δ = -1.62 units; p<0.05), SHUNT% (mean Δ = -2.8%; p<0.05), HR% (mean Δ = 3.9%; p<0.01), and RISK ACE (mean Δ = -1.2 events per 100 patient-years; p<0.001) compared to baseline; and 61% of subjects in the 225 mg rencofilstat arm had a DSI improvement of >2.0 points (p<0.05). In HepQuant’s research, improvements from baseline, especially for high DSI scores that decrease by 2.0 points or more, are associated with clinically significant reductions in risk for liver related complications, including esophageal varices and encephalopathy.
Table 1: HepQuant Test Results in All Subjects with Paired Data (n=61)
| All Doses | 75 mg | 150 mg | 225 mg | |
| % of Subjects with a 2-point or Greater Decrease in DSI | ||||
| 32.8 (20/61) | 26.1 (6/23) | 15.0 (3/20) | 61.1 (11/18)§ | |
| Mean Difference from Baseline to Day 120 | ||||
| BMI (kg.m-2) | -0.04 | 0.21 | -0.09 | -0.31 |
| DSI (score) | -0.55 | -0.41 | 0.24 | -1.62* |
| SHUNT (%) | -1.7* | -2.1 | -0.2 | -2.8* |
| HR (%) | 1.3 | 1.4 | -1.1 | 3.9** |
| RISK ACE (Events per 100 patient-years) | -1.2*** | -1.5 | -0.8*** | -1.2*** |
*p < 0.05; **p < 0.01; ***p < 0.001; paired t-test, no correction for multiple comparisons
§Chi-Square p < 0.05
In subjects with the most advanced functional impairment, four measures of liver impairment significantly improved compared to baseline with rencofilstat treatment for 4 months, independent of dose.
To address the potential of rencofilstat for patients with the most advanced functional impairment and greatest risk of disease progression, an analysis was conducted on the 34 subjects with DSI>17 or SHUNT%>25 as research indicates these subjects are at high risk for hepatic complications (Table 2). In this subgroup, independent of rencofilstat dose, statistically significant decreases at Day 120 compared to baseline were again observed for DSI score (mean Δ = -1.30 units; p<0.05), SHUNT% (mean Δ = -3.4%; p<0.01), HR% (mean Δ = 2.9%; p<0.05), and RISK ACE (mean Δ = -1.6 events per 100 patient-years; p<0.01). The large reduction in SHUNT% suggests alleviation of micro-architectural defects as anticipated from an antifibrotic agent and suggests that rencofilstat may be most effective in patients with more severe liver impairment.
Table 2: HepQuant Test Results in Functionally Impaired Subjects with Paired Data (n=34)
| All Doses | 75 mg | 150 mg | 225 mg | |
| % of Subjects with a 2-point or Greater Decrease in DSI | ||||
| 41.2 (14/34) | 50.0 (6/12) | 16.7 (2/12) | 60.0 (6/10) | |
| Absolute Change from Baseline to Day 120 | ||||
| BMI (kg m-2) | 0.17 | 0.16 | 0.35 | 0.00 |
| DSI (score) | -1.30* | -2.05 | -0.17 | -1.76* |
| SHUNT (%) | -3.4** | -5.8* | -1.0 | -3.4 |
| HR (%) | 2.9* | 4.6 | -0.4 | 5.0* |
| RISK ACE& (Events per 100 patient-years) | -1.6** | -2.3 | -1.0** | -1.5*** |
*p < 0.05; **p < 0.01; ***p < 0.001; paired t-test, no correction for multiple comparisons
Secondary Endpoints: Fibrosis- and Injury-Associated Biomarkers Improved with all Doses of Rencofilstat, with the Greatest Reductions Observed with the 225 mg Arm
Multiple biomarkers related to fibrosis were improved following four months of treatment with rencofilstat: ProC3, PIIINP, TIMP1, and hyaluronic acid. ELF scores were similarly improved by rencofilstat. Robust reductions in ALT and AST were also observed with all doses of rencofilstat, with the greatest reductions seen in the 225 mg rencofilstat dosing arm. Incremental dose-response patterns were observed for most of the biomarkers, and in all cases the largest reductions from baseline for each of the biomarkers occurred in the 225 mg rencofilstat group (Table 3).
Table 3: Percent Change from Baseline in Key NASH Biomarkers After Four Months Treatment with Rencofilstat
| All Subjects: Safety Population | 75
mg rencofilstat n=23 |
150
mg rencofilstat n=21 |
225
mg rencofilstat n=21 |
| %Change | %Change | %Change | |
| ALT | -3.37*,**** | -13.01*,** | -21.63*,** |
| AST | 4.54*,** | -8.64*,** | 4.68* |
| ProC3 | -6.47 | -11.12* | -9.58*,**** |
| PIIINP | 2.75 | -0.47* | -5.6* |
| TIMP1 | 3.76 | 30.5 | -3.9 |
| Hyaluronic acid | 11.67 | -13.18* | -10.67* |
| ELF score | 1.03* | 3.85*,** | -2.51*,** |
*Different from Baseline p < 0.001, Friedman ANOVA, **Different from 75 mg Dose p< 0.01,
***Different from 150 mg Dose, ****All Doses p < 0.001.
Rencofilstat 225 mg in high-risk population led to the greatest improvements in NASH biomarkers.
Additional analyses were performed on the approximate one-third of subjects with elevated baseline ProC3, which assesses the formation of type III collagen and indicates both severity and activity of disease. Because Pro-C3 is a measure of collagen cleavage during active fibrinogenesis, subjects with high ProC3 levels represent a NASH population with more active disease, therefore representing an important target population for many NASH drug candidates. In ALTITUDE-NASH, the greatest magnitude of effects was observed with 225 mg rencofilstat (Table 4), and most frequent dose-dependencies were observed in subjects with baseline ProC3>37.5 ng/ml (Roche, Elecsys). Rencofilstat 225 mg, and often the 150 mg dose, led to greater improvements than with 75 mg rencofilstat for all the NASH biomarkers in this high-risk population as well as in the entire study population.
Table 4: Percent Change From Baseline in NASH Biomarkers in Subjects with ProC3 ≥ 37.5 ng/ml
| 75
mg rencofilstat n=10 |
150
mg rencofilstat n=7 |
225
mg rencofilstat n=6 |
|
| %Change | %Change | %Change | |
| ALT | -13.24*,*** | -32.24* | -37.78*,** |
| AST | 6.73*,**** | -30.72**** | -11.34*,** |
| ProC3 | -3.39**** | -17.05**** | -16.23*,**** |
| PIIINP | -1.22**** | -7.36*,** | -21.48*,** |
| TIMP1 | 2.4 | -6.69* | -4.77* |
| Hyaluronic acid | -4.56*,**** | 6.99*,** | -19.66*,** |
| ELF score | -0.95*,**** | -1.64*,** | -5.31*,** |
*Different from Baseline p < 0.001, Friedman ANOVA, **Different from 75 mg Dose p< 0.01,
***Different from 150 mg Dose, ****All Doses p < 0.001.
Primary Safety and Tolerability Endpoints Met with No Serious Adverse Events Attributed to Rencofilstat
Of the 70 subjects enrolled in the study, 67 completed all study procedures including 120 days oral dosing of rencofilstat with a 14-day routine safety follow up period. Rencofilstat was well tolerated, with no trends in adverse events or safety signals identified. There were no deaths or hepatic decompensation events recorded in the trial, and a total of five serious adverse events (SAEs) occurred with four unrelated to study drug (COVID-19, headache, fibula fracture, COPD) and a single SAE (biliary acute pancreatitis) classified as possibly related to study drug in a subject diagnosed with a pancreatic stone as the likely source for the pancreatitis. Other safety labs, EKGs, and physical exams did not reveal any safety signals or concerns over the course of the study.
Study Design and Objectives
ALTITUDE-NASH was designed as a Phase 2, multi-center, randomized, open label study. F3 NASH subjects were identified by having a baseline AGILE 3+ screening score of ≥0.53 or historical biopsy obtained within the preceding 6 months. The AGILE 3+ score is calculated using FibroScan fibrosis score, laboratory values (AST, ALT, platelets), and clinical parameters (age, sex, diabetes status). Subjects were randomized to one of three rencofilstat treatment groups receiving either 75 mg, 150 mg, or 225 mg soft gelatin capsules once daily for a period of 4 months. The HepQuant Shunt test was administered at baseline, Day 60, and Day 120 of treatment in addition to serum analyses for safety and efficacy markers at each study visit. End-of-study liver biopsies or other measures of structural extracellular matrix changes were not collected due to the relatively short duration of treatment. The objectives were to: investigate liver function and safety; confirm the positive results observed in the 28-day Phase 2a AMBITION clinical trial; and collect additional data to support Hepion’s AI-based precision medicine program (AI-POWR™) which will be used to optimize future studies and patient outcomes. This trial also serves as a bridge to Hepion’s current 12-month Phase 2b ASCEND-NASH liver biopsy-based trial.
The HepQuant SHUNT procedure was chosen as the primary endpoint in ALTITUDE-NASH based on its ability to quantify the severity of hepatic dysfunction and portal-systemic shunting. Currently under review by the U.S. Food and Drug Administration (“FDA”), the procedure measures clearance by the liver of administered doses of an isotopically labeled bile salt, cholate, which reflects an important physiologic function of the liver. The test is minimally invasive and is able to sensitively track changes in the degree of liver function impairment. This contrasts with liver biopsy results, which are obtained through a more invasive procedure and only documents liver pathology, not liver function. Further, according to Gregory T. Everson, MD, HepQuant’s Founder and Chief Executive Officer, “The results from HepQuant’s testing platform provide compelling evidence that those patients at the highest risk of complications are the ones that responded most consistently and robustly to treatment with rencofilstat.”
Stephen Harrison, MD, Chairman and Co-Founder of Summit Clinical Research and Chair of Hepion’s Scientific Advisory Board commented, “Use of the AGILE 3+ in screening allowed us to identify an advanced NASH population in ALTITUDE-NASH at a high risk for complications associated with the disease. Improvements in numerous NASH biomarkers in concert across this population not only affirms the positive results in this four-month study but also increases my confidence in positive outcomes in the larger and longer Phase 2b ASCEND-NASH biopsy trial which is currently recruiting well”.
Patrick Mayo, PhD, Hepion’s Senior Vice President, Clinical Pharmacology & Analytics added, “ALTITUDE-NASH represents a veritable data bonanza, providing us information on patient responsiveness to rencofilstat in a very advanced NASH population that will further enhance our AI-POWR™ platform, which should allow us to predict rencofilstat-responders a priori. This not only enhances and de-risks future studies, including potential Phase 3 trials, but will ultimately allow clinicians to provide rencofilstat to patients who they know will respond. Determining which patient is best-suited to receive rencofilstat could ultimately provide guidance to our eventual commercial strategy.”
Conference Call Details
Hepion is pleased to invite all interested parties to participate in a conference call at 8:30 a.m. ET today, during which the ALTITUDE-NASH topline results will be discussed. To participate in this conference call, please dial (800) 715-9871 (U.S.) or (646) 307-1963 (international), conference ID 9439742, approximately 10 minutes prior to the start time. The call will also be broadcast live and archived on the Company's website at www.hepionpharma.com under "Events" in the Investors section.
About Hepion Pharmaceuticals
The Company's lead drug candidate, rencofilstat, is a potent inhibitor of cyclophilins, which are involved in many disease processes. Rencofilstat has been shown to reduce liver fibrosis and hepatocellular carcinoma tumor burden in experimental disease models and is currently in Phase 2 clinical development for the treatment of NASH. In November 2021, the U.S. Food and Drug Administration (“FDA”) granted Fast Track designation for rencofilstat for the treatment of NASH. That was followed in June 2022 by the FDA’s granting of Orphan Drug designation to rencofilstat for the treatment of HCC.
Hepion has created a proprietary AI platform, called AI-POWR™, which stands for Artificial Intelligence - Precision Medicine; Omics (including genomics, proteomics, metabolomics, transcriptomics, and lipidomics); World database access; and Response and clinical outcomes. Hepion intends to use AI-POWR™ to help identify which NASH patients will best respond to rencofilstat, potentially shortening development timelines and increasing the observable differences between placebo and treatment groups. In addition to using AI-POWR™ to drive its ongoing NASH clinical development program, Hepion intends to use the platform to identify additional potential indications for rencofilstat to expand the company's footprint in the cyclophilin inhibition therapeutic space.
Forward-Looking Statements
Certain statements in this press release are forward-looking within the meaning of the Private Securities Litigation Reform Act of 1995. These statements may be identified by the use of forward-looking words such as “anticipate,” “believe,” “forecast,” “estimated,” and “intend,” among others. These forward-looking statements are based on Hepion Pharmaceuticals’ current expectations and actual results could differ materially. There are a number of factors that could cause actual events to differ materially from those indicated by such forward-looking statements. These factors include, but are not limited to, substantial competition; our ability to continue as a going concern; our need for additional financing; uncertainties of patent protection and litigation; risks associated with delays, increased costs and funding shortages caused by the COVID-19 pandemic; uncertainties with respect to lengthy and expensive clinical trials, that results of earlier studies and trials may not be predictive of future trial results; uncertainties of government or third party payer reimbursement; limited sales and marketing efforts and dependence upon third parties; and risks related to failure to obtain FDA clearances or approvals and noncompliance with FDA regulations. As with any drug candidates under development, there are significant risks in the development, regulatory approval, and commercialization of new products. There are no guarantees that future clinical trials discussed in this press release will be completed or successful, or that any product will receive regulatory approval for any indication or prove to be commercially successful. Hepion Pharmaceuticals does not undertake an obligation to update or revise any forward-looking statement. Investors should read the risk factors set forth in Hepion Pharmaceuticals’ Form 10-K for the year ended December 31, 2022, and other periodic reports filed with the Securities and Exchange Commission.
For further information, please contact:
Stephen Kilmer
Hepion Pharmaceuticals Investor Relations
Direct: (646) 274-3580
skilmer@hepionpharma.com